
Abstract
Purpose
To identify mammography screening prevalence and predictors in Asian American women, focusing on the potential disparities in race and its influence on screening behaviors.
Design
A secondary analysis utilized the California Health Interview Survey (CHIS) 2015–2016.
Setting
California, U.S.
Sample
Cisgender women who were non-Hispanic (NH) White, Chinese, Filipino, Vietnamese, Japanese, Korean, or “other Asian”, aged 40 or above (unweighted N=13 451).
Measures
Socioeconomics, chronic health conditions, and preventive care utilization were mesuared as potential risk factors, where up-to-date mammography screening as the outcome variable.
Analysis
Multivariable adjusted logistic regressions were generalized to identify the up-to-date mammography screening behaviors in relation to potential factors, stratified by race and ethnicity.
Results
The prevalence for up-to-date mammography screening in NH-White and Asian American women were 68.06% and 65.97%, respectively. In NH-White women, receiving an up-to-date mammogram was associated with age, birthplace, smoking status, diabetes, hypertension, health insurance coverage, and a preventive care visit in the past 12 months, whereas only age and a preventive care visit were significant predictors in Asian women.
Conclusions
The findings indicate that utilization disparities exist in mammogram in relation to socioeconomics, chronic health conditions, preventive care utilization, when comparing between race and ethnicity. Asian American women with borderline hypertension and no preventive care visits may require more public health outreach and cancer education.
Keywords
Purpose
Asian Americans, referring to individuals having origins in the Far East, Southeast Asia, or the Indian subcontinent, 1 are among the fastest-growing racial groups in the U.S. and continue to face disparities in healthcare compared to other Americans, especially in the realm of cancer screening. 2 In this study, we used Asian Americans as an umbrella term for Asians and Asian Americans who lived in the U.S. The Centers for Disease Control and Prevention (CDC) reported that, in 2017, cancer has been the leading cause of death among Asian American men and women, compared to their non-Hispanic (NH)-White counterparts. 3 The main cancer disparities could be explained by the low screening rate associated with the differences in demographics (education level, employment status, health insurance, and preventive care utilization), acculturation (language barriers and cultural beliefs), and immigration status.4-6 In regards to breast cancer, one of the most common cancer types in the U.S., Asian American women lagged behind NH-White American women in mammography utilization and follow-up visits.7,8- This could lead to potential delays in the early breast cancer detection and causing more latestage diagnosis and subsequently worse survival outcomes.
Asian American women who were foreign-born face unique challenges compared to their native-born counterparts, such as linguistic isolation from a lack of interpreters and native language public health materials, and reliance on traditional remedies rather than evidence-based medicine. 9 In an earlier study by Kandula et al using data from the 2001 California Health Interview Survey, Asian immigrants’ perceptions of cancer risks and screening benefits for asymptomatic conditions may differ from individuals who were born in the U.S. 10 For example, 21.1% of foreign-born Asian Americans did not have age-appropriate mammograms due to feeling asymptomatic compared to only 6.5% in NH-White and 6.3% in US-born Asian American counterparts, respectively. Though not statistically significant, only 6.4% of foreign-born Asian Americans reported pain/embarrassment as a reason for not pursuing mammograms, whereas this number reached up to 9.2% in NH-White and 13.2% in US-born Asian Americans. 10 More interestingly, 67.4% of US-born Asian Americans stated no specific reason or other reasons for not pursuing mammograms vs. 48.7% in those who were foreign-born. Not having a doctor or lack of insurance did not appear to be a significant reason for not having mammograms.
Since 2000, the Asian population in the U.S. has grown 72%, from 11.9 million to 20.4 million in 2015. 11 Thus, it is of critical importance for preventive health professionals to better understand the mechanisms of screening disparities in Asian Americans. Although Asian Americans have historically been perceived to be healthier in comparison to the general population in the U.S., many scholars postulated that Asian Americans might have health disparities that are often masked when health data is aggregated at the national level.12,13
Therefore, in the present study, we aim to identify mammography screening disparities by race between NH-White and Asian American Women using the 2015–2016 California Health Interview Survey (CHIS), focusing on the potential of ethnicity differences and its influence on screening behaviors within Asian American women subgroups. The findings from the present study will enable us to create more ethnic-specific and culturally comprehensive intervention strategies that are critical to address these public health issues in the future.
Methods
Sample
A cross-sectional, population-based, random digit dial telephone-based (landline or cell phone) survey data from the 2015–2016 CHIS was used to identify health statuses of California’s non-institutionalized population with major racial and ethnic groups. 14 One adult per household was selected randomly to be interviewed. Our study used publicly available de-identified CHIS 2015–2016 data, and no data usage agreement was required. The details of the study methods could be found elsewhere. 14 There were 2 primary reasons to use the CHIS dataset: (1) it includes the largest sample of Asian American subgroups in the U.S. and (2) it provides detailed information on extensive health-related factors. This study involves 6 subgroups of Asian American women, including Chinese, Japanese, Korean, Filipino, South Asian (SA), and Vietnamese Americans. The adult response rate after screening the household was 47.2% in 2015 and 44.6% in 2016. 15 The final data are weighted to account for study design, while adjusting for non-response and the absence of non-telephone households.
The CHIS surveyed 3 age groups: there are children (0–11 years), adolescents (12–17 years), and adults (18 years and older). Our study subsample included only the 13 451 cisgender women (unweighted sample size) aged 40 or above, with self-identification of NH-White, Chinese, Filipino, Vietnamese, Japanese, Korean, or “other Asian”.
Measures
Independent variables consisted of socioeconomic factors, chronic health conditions/health behaviors, and preventive care utilization.
Socioeconomic factors included various variables: race (we only included the data for NH-White and Asian American populations), Asian ethnicity (Chinese, Filipino, Vietnamese, Japanese, Korean, and “other” Asian), age (a regrouped variable: 40–49, 50–74, and 75 or above), educational attainment (a regrouped variable: less than high school (<HS), high school graduate, and college or above), poverty level (0%–99% federal poverty level (FPL), 100%–199% FPL, and 200%–299% FPL), marital status (a regrouped variable: married, divorced/separated/widowed, and single), birthplace (U.S.-born or foreign-born), and language use at home (a regrouped variable: English, Chinese, Korean, other one language (eg, Spanish and Vietnamese), and 2 or more languages).
Chronic health conditions/health behaviors included 3 single items: smoking status (current smoker, not current smoker), diabetes (no, yes/borderline), hypertension (no, yes/borderline).
Preventive care utilization was captured by 2 items, including the current health insurance coverage (no, yes), and whether or not had a preventive care visit in the past 12 months (no, yes).
For the outcome variable, we followed the biennial screening mammography recommendation from The United States Preventive Services Task Force (USPSTF) for women aged 50 to 74 years. Also, the original data about mammogram collected in CHIS data followed the USPSTF that “During the past 2 years, have you had a mammogram?” The responses were “yes” or “no”.
Analysis
First, descriptive characteristics were presented in population estimates between NH-White and Asian American women, as well as by ethnicity within Asian American women subgroups. To investigate differences associated with demographic characteristics (socioeconomic factors, chronic health conditions/health behaviors, and preventive care utilization) by race and ethnicity, bivariate analyses were conducted using chi-square tests (or Fisher’s exact).
Next, a weighted multivariable logistic regression of up-to-date mammography screening with its correlates was conducted among NH-White and Asian American women adjusting for education, poverty, and marital status. The final test was repeated in only Asian American women. All analyses were conducted using survey weights and clustering by sampling unit from CHIS. 16 Two-tailed P values less than .05 were considered statistically significant. The results are presented as odds ratios (ORs) and 95% confidence intervals (CI). All analyses were conducted by using Stata 16 (StataCorp LP, College Station, TX).
Results
Demographic Characteristics
Weighted Descriptive Characteristics among non-Hispanic White and Asian American Women Aged 40 or above, CHIS 2015–2016.
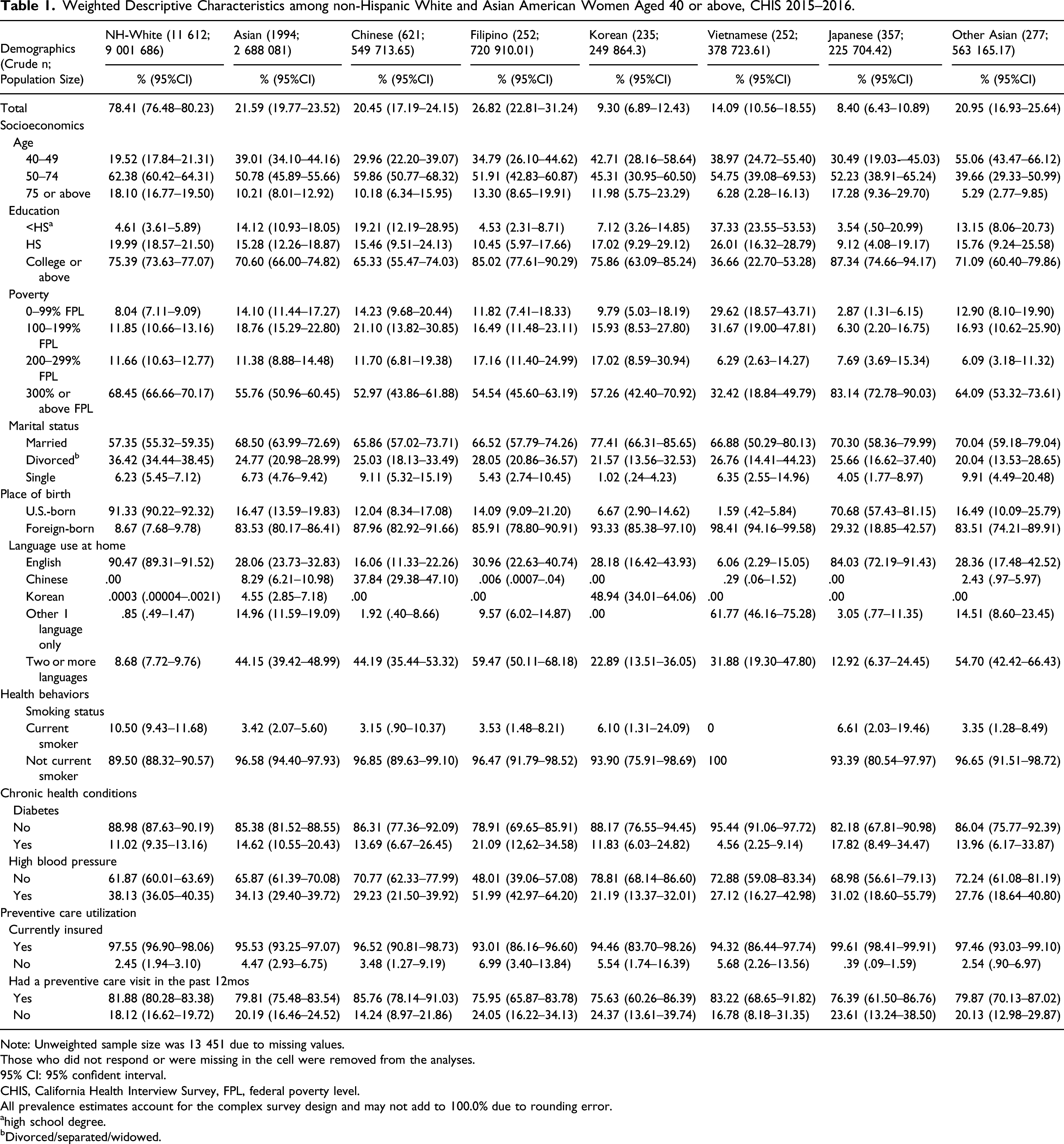
Note: Unweighted sample size was 13 451 due to missing values.
Those who did not respond or were missing in the cell were removed from the analyses.
95% CI: 95% confident interval.
CHIS, California Health Interview Survey, FPL, federal poverty level.
All prevalence estimates account for the complex survey design and may not add to 100.0% due to rounding error.
ahigh school degree.
bDivorced/separated/widowed.
In regard to demographic characteristics among Asian American women (unweighted N = 1994): 20.45% of the sample were Chinese (95% CI = [17.19, 24.15]), 26.82% were Filipino (95% CI = [22.81, 31.24]), 9.30% were Korean (95% CI = [6.89, 12.43]), 14.09% were Vietnamese (95% CI = [10.56, 18.55]), 8.40% were Japanese (95% CI = [6.43, 10.89]), and 20.95% were “other Asians” (95% CI = [16.93, 25.64]). There were significant differences across demographic characteristics except for marital status, diabetes, health insurance coverage, and a preventive care visit by Asian subgroups. Compared to Chinese women, Japanese women tended to be older (75 or above), highly educated, financially advanced, U.S.-born, and diabetic. Meanwhile, Japanese women were less likely to use preventive care in the past 12 months. Vietnamese women were younger, less educated (<HS), financially disadvantaged, foreign-born, and less likely to have diabetes compared to their Chinese peers. Korean women were more likely to be younger, educated, foreign-born, current smokers, and less likely to use preventive care in the past 12 months. Filipino women were more likely to be educated and have hypertension or borderline hypertension. They were less likely to be insured and use preventive care in the past 12 months. Chinese women had the highest rate of having a preventive care visit (85.76%; 95%CI = [78.14, 91.03]) in the past 12 months, and Japanese women had the lowest rate (76.39%; 95%CI = [61.50, 86.76]), although the discrepancy was not significant at .05. There are significant differences in smoking between Asian subgroups. Korean and Japanese women had the highest smoking rates (6.10% and 6.61%, respectively), whereas Vietnamese had the lowest rate (0%). Almost 52% of Filipino women had high blood pressure, whereas only 21.19% in their Korean peers (P < .01).
Breast Cancer Screening
Bivariate Logistic Regression Analysis of Mammography by Race and its Correlates among U.S. Women Aged 40 and above (Weighted), CHIS 2015–2016.
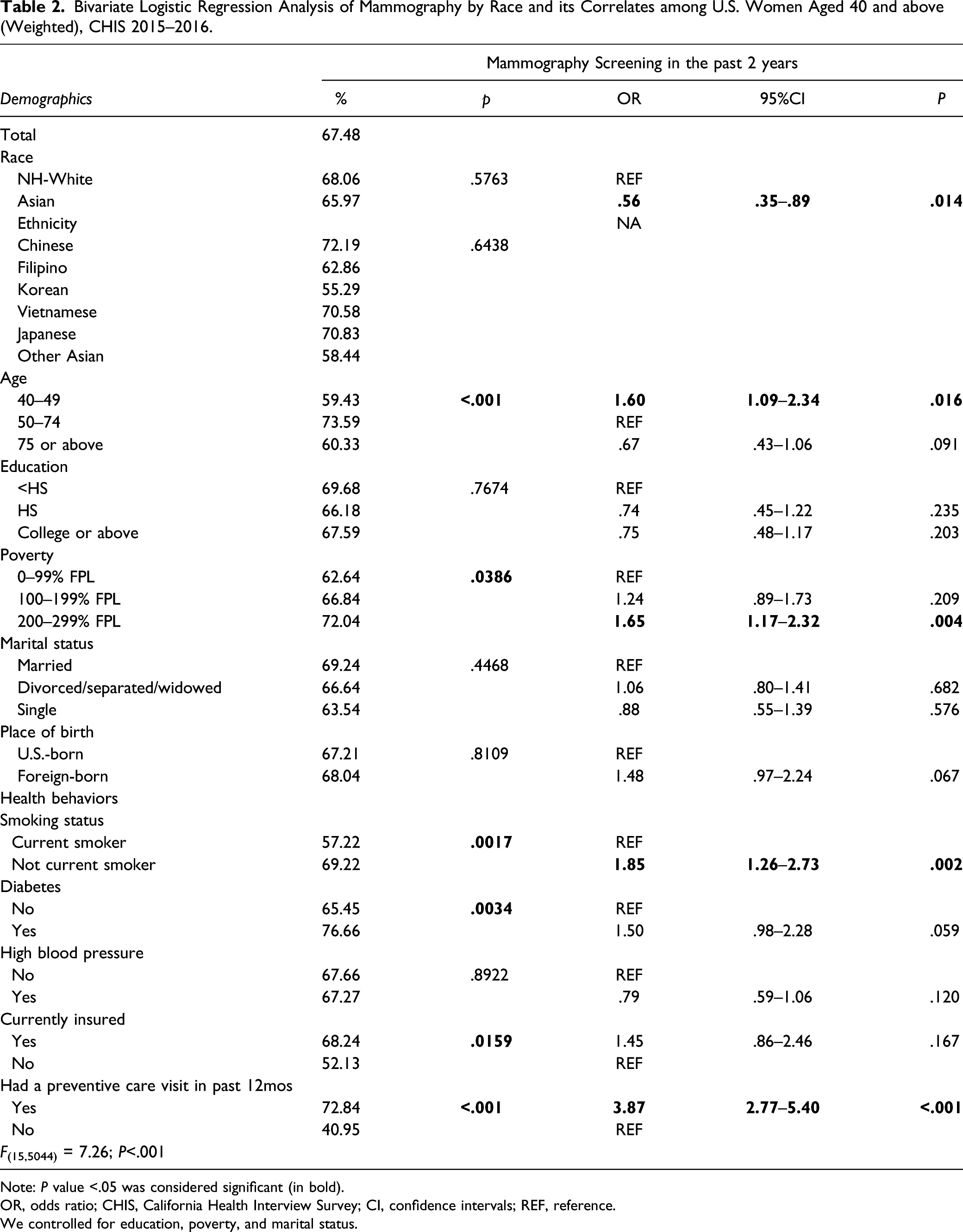
Note: P value <.05 was considered significant (in bold).
OR, odds ratio; CHIS, California Health Interview Survey; CI, confidence intervals; REF, reference.
We controlled for education, poverty, and marital status.
Logistic Regression
A weighted, bivariate logistic regression analysis of receiving an up-to-date mammogram was conducted among U.S. women aged 40–74 (Table 2; F(15, 5044) = 7.26, P < .01). Age, race, birthplace, smoking status, diabetes, hypertension, and preventive care utilization were significant factors. Being aged 40–49 (odds ratio (OR) = 1.60, 95% CI = [1.09, 2.34], P = .02), economically advanced (OR = 1.65, 95% CI = [1.17, 2.32], P < .01), not a current smoker (OR = 1.85, 95% CI = [1.26, 2.73], P < .01), and having a preventive care visit (OR = 3.87, 95% CI = [2.77, 5.40], P < .01) were significantly associated with greater odds of receiving mammogram. Contrarily, being Asian American (OR = .56, 95% CI = [.35, .89], P = .01) was significantly associated with lower odds of receiving mammogram. Though not statistically significant, having diabetes was associated with a potential 50% increased odds of receiving mammogram (OR = 1.50, 95%CI = [.98, 2.28], P = .06).
Weighted Logistic Regression of Mammography and its Correlates among U.S. Women Aged 40 and Above, Stratified by Race, CHIS 2015–2016.
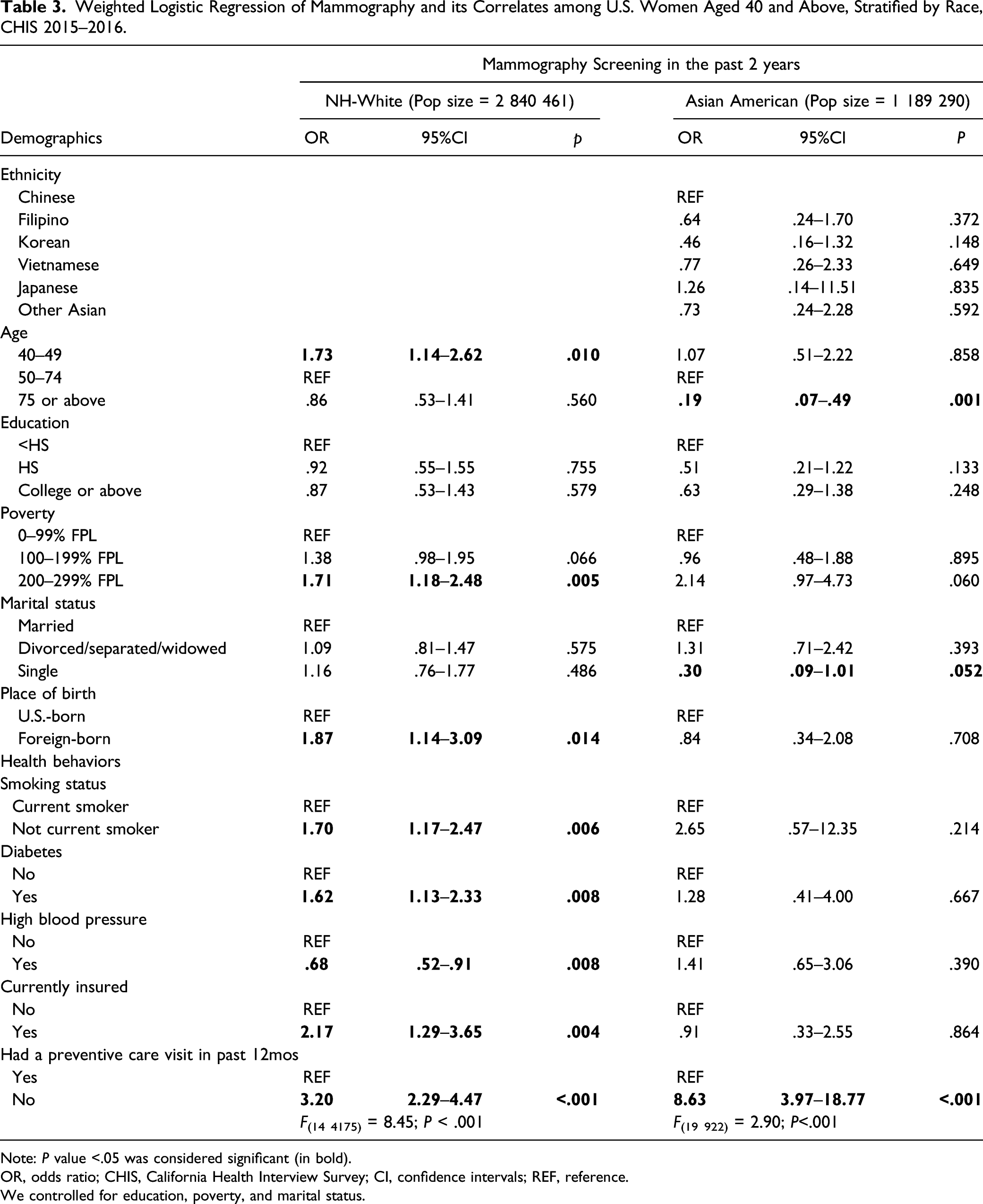
Note: P value <.05 was considered significant (in bold).
OR, odds ratio; CHIS, California Health Interview Survey; CI, confidence intervals; REF, reference.
We controlled for education, poverty, and marital status.
Within Asian American women, a weighted, adjusted logistic regression analysis (F(19, 922) = 2.90, P < .01; Table 3) showed age and preventive care utilization were significant factors. Having a preventive care visit (aOR = 8.63, 95% CI = [3.97, 18.77], P < .01) was significantly associated with greater odds of receiving an up-to-date mammogram.
Discussion
The present study overcomes previous studies’ limitations by having a large non-probability sample of Asian subgroups in a state level. Our findings are in line with previous studies that there were significant differences in demographics and clinical aspects in receiving an up-to-date mammogram between NH-White and Asian American women.5,8,10 We additionally found varying factors that influence the uptake of mammography among NH-White and Asian American women. For NH-White women, being younger (<50 years old), foreign-born, financially advanced, insured, non-current smoker, diabetics, and having a preventive care visit in the past 12 months were associated with increased odds of having an up-to-date mammogram. Among Asian American women, older age (>75 years) was linked to decreased odds of having a mammogram, where having a preventive care visit was associated with increased odds of having a mammogram.
The above findings in our study between NH-White and Asian American women suggest that factors affecting racial disparities in receiving a mammogram are different and multidimensional, while race might serve as a proxy for multiple disparities prevalent in the cancer care contunuum. 17 The lack of a preventive health visit appears to be the main barrier for Asian American women in receiving a mammogram, whereas among NH-White women, multiple demographical and behavioral health factors all influence their mammogram uptake. Those findings support a tailored approach rather than a “one-size-fits-all” strategy when advocating breast cancer screening among eligible women.
Previous studies revealed the differences in breast cancer screening rates might be attributable to socioeconomic and cultural factors as well as issues in health literacy within Asian subgroups.18–22 In our study, the diverse socioeconomic features, smoking status, comorbid conditions, and preventive care usage by Asian subgroups have been highlighted. Japanese women were more likely to be financially secure, U.S.-born, English-speaking at home, and current smokers. Filipino women were more likely to have diabetes and high blood pressure.
Though the discrepancy was not statistically significant, our study showed that Koreans had the lowest rates of recent screening (past 2 years), whereas Chinese had the highest rate. This finding was partially convergent to previous studies that Korean American women were at the lower end of screening rates across many cancer diagnoses.20-22 Lee et al. suggested that Korean American women were less likely to have access to healthcare, less knowledge in cancer prevention, lower perceived self-efficacy, fewer benefits and less spousal support that could help them receive mammogram screening which may partially explain the findings for Asian American women. 20 In Chinese American women, a cross-sectional survey suggested that the lack of healthcare providers recommending a mammogram was significantly associated with lower odds of receiving mammogram screening. 23 Our findings showed that 79.81% of Asian American women reported having had a preventive care visit in the past 12 months, ranging from 85.76% in Vietnamese to 75.63% in Koreans. Such findings indicated that Korean women in the US should be offered culturally competent and language-sensitive services aimed at boosting preventive care utilization.
In consistent with prior studies, our findings showed that socioeconomics (foreign-born), chronic health conditions/health behaviors (smoking status, diabetes, and hypertension), and preventive care visits (insurance and preventive care visits) attenuate the effect of ethnicity on mammography screening within NH-White women but not Asian American women.10,22,24 The discrepancies could be due to several reasons. First, although the odds of having mammogram did not differ significantly in our study, we did observe the differences by demographic characteristics as well as health behaviors in subgroups among Asian American women. For example, the vast majority of Japanese American women had a college degree or above compared to that in only approximately one-third of Vietnamese American women. In addition, Filipino American women had the highest prevalence of self-reported diabetes and hypertension compared to other Asian subgroups. Thus, our neutral findings could be due to residual confounders, small sample sizes of certain ethnic subgroups, and recall bias (from self-reported health behaviors).
Finally, our results also suggest that younger NH-White women (aged <50) were more likely to receive a mammogram than those aged 50–74 years old, whereas there was no difference between those aged 50–74 vs. 75 years or above. In contrast, Asian American women who were younger did not appear to have increased odds of receiving a mammogram, however, those greater than 75 years old were significantly less likely to have mammogram screening. The USPSTF recommends women aged 50–74 years to have biennial screening mammography (Grade B recommendation) and concludes that there is insufficient evidence to assess the benefits and harms of screening mammogram in women aged ≥75 years as this population was excluded from randomized control trials. 25 In addition, the USPSTF also sets forth Grade C recommendations for those aged 40–49 years among which screening mammography should be individualized based on personal risks. 26 The distinct age findings between NH-White and Asian American women could be explained by several reasons. Though Caucasian women were found to have a higher risk of developing breast cancer than Asian women which could be due to genetic, dietary, behavioral, and environmental factors, 27 the findings that younger NH-White women were more likely to have mammogram than those in the recommended age range may indicate the possibility of over-screening in this population. Other possible explanations include differences in perceptions of stigma, cost, navigation services, and language barriers among Asian American women.
Previous studies indicated that culturally specific interventions might increase the Asian American communities’ screening rate and cancer registries. For instance, the Asian American Network for Cancer Awareness, Research, and Training has demonstrated that using Asian inclusive language and respecting cultural norms can assist in incorporating more Asian Americans in clinical trials which can translate to better outcomes in this group. 12 Within some Asian subcultures, a lack of participation in self‐care and not questioning health care providers as they are viewed as authorities have been identified. 28 It is unknown how broadly these issues impact members of the Asian Americans or other immigrant populations but should be assessed and addressed to expand cancer health literacy and participation in screening. Brega et al. reported quality improvement measures that can improve organizational literacy and other positive healthcare interventions, like immunizations and behavior changes, which should be promoted. 29
A few limitations of our study need to be highlighted. First, this analysis used cross-sectional data and therefore neither temporality nor causality can be conducted. Moreover, potential factors, such as language proficiency, acculturation, health literacy, and information, were not available in the open-access data. Future research should include these variables to identify their roles in cancer screening disparities across racial groups using a longitudinal study design. All data were self-reported and not validated using medical records, which may have undermined the validity of mammogram prevalence estimates and related behaviors due to social desirability or recall bias. Thus, future research that uses validated measures for cancer screening is needed to generate unbiased estimates of screening eligibility and utilization. Primary data collection should measure and examine the effects of racism in everyday and/or in a healthcare setting, which could help identify the impact of racism towards Asian Americans in health disparities. Lastly, the data came from state-level data; thus, the generalizability of the results may be limited.
Overall, the disparities in breast cancer screening between NH-White and Asian American women in the U.S. is related to a combination of clinical, socioeconomic, and cultural variables. Our study purposed that having more routine preventive care visits could potentially increase the odds of receiving an up-to-date mammogram among Asian American women, with an effect size larger than that in NH-White women. Future studies should examine racism and acculturation, including organizational health literacy, linguistic behavior and support, and health-related educational information access with a longitudinal study design to close the gap between races and enthnicities in breast cancer screening in the future. The mammogram screening disparities between NH-White and Asian American women exist. There is inadequate evidence to identify various predictors of screening disparities by race and ethnicity. Our findings indicate that utilization disparities exist in screening mammography in relation to socioeconomics, chronic health conditions, preventive care utilization, and race. NH-White women receiving an up-to-date mammogram was associated with age, birthplace, smoking status, diabetes, hypertension, health insurance coverage, and a preventive care visit in the past 12 months, whereas only age and a preventive care visit were significant predictors in Asian women. The exhibition of disparity in breast cancer screening among Asian American women in the U.S. is a combination of clinical, socio-economical, and cultural status. To include more eligible Asian American women in breast cancer screening, we should focus on training in organizational health literacy, linguistic support, and modification of educational information targeting underserved Asian women for more up-to-date preventive care visits and breast cancer screening.So What?
What Is Already Known on This Topic?
What Does This Article Add?
What Are the Implications for Health Promotion Practice or Research?
Footnotes
Acknowledgments
The data is publicly available from the California Health Interview Survey.
Authors’ Contributions
HX contributed to develop study concepts, conduct data analysis, interpret the results, and draft the manuscript. YL contributed to develop study concepts and draft the manuscript. NT and QW contributed to draft the manuscript. All authors approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.