
Abstract
Purpose
Lifestyle modification programs have been shown to effectively treat chronic disease. The Coronary Health Improvement Program has been delivered by both paid professional and unpaid volunteer facilitators. This study compared participant outcomes of each mode in the United States.
Design
Pre-/post-analysis of CHIP interventions delivered between 1999 and 2012.
Setting
Professional-delivered programs in Rockford Illinois 1999-2004 and volunteer-delivered programs across North America 2005-2012.
Subjects
Adults ≥21 years (professional programs N = 3158 34.3% men, mean age = 54.0 ± 11.4 years; volunteer programs N = 7115 33.4% men, mean age = 57.4 ± 13.0 years).
Measures
Body mass index, blood pressure (systolic and diastolic), blood lipid profile (total cholesterol, high-density lipoprotein, triglycerides, low-density lipoprotein), and fasting plasma glucose.
Analysis
Analysis of Covariance, with adjustment for age, gender, BMI change and baseline biometric and effect sizes.
Results
The professional-delivered programs achieved significantly greater reductions in BMI (.4%, P < .001) and HDL (1.9%, P < .001) and the volunteer-delivered programs achieved greater reductions in SBP (1.4%, P < .001), DBP (1.1%, P < .001), TC (1.4%, P = .004), LDL (2.3%, P < .001), TG (4.0%, P = .006), and FPG (2.7%, P < .001). However, the effect size differences between the groups were minimal (Cohen’s d .1-.2).
Conclusions
Lifestyle modification programs have been shown to effectively treat chronic disease. The Complete Health Improvement Program (CHIP) lifestyle intervention has been delivered by both paid professional and unpaid volunteer facilitators. This study compared selected chronic disease biometric outcomes of participants in each mode in the United States. It found volunteer-delivered programs do not appear to be any less effective than programs delivered by paid professionals, which is noteworthy as volunteers may provide important social capital in the combat of chronic disease.
Keywords
Introduction
Chronic diseases are the leading causes of death and disability in the western world, with more than half of all deaths each year attributed to heart disease, stroke, diabetes, and cancer.1,2 These diseases place a large burden on families and communities through increased morbidity, with a subsequent major fiscal burden. The direct (medical) and indirect (productivity) costs of cardiovascular disease alone are projected to increase from $450 billion in 2010 to more than $1 trillion by 2030. 3
Lifestyle modification programs have been shown to be effective in the treatment of chronic disease. 4 One such program is the Coronary Health Improvement Program (CHIP), a community-based lifestyle modification program developed in the United States in 1986 to target cardiovascular disease. As studies showed this intervention addresses other chronic diseases such as type 2 diabetes mellitus, it was renamed in 2012 the Complete Health Improvement Program, thereby retaining the acronym CHIP. CHIP has demonstrated significant reductions in selected chronic disease risk factors among large cohorts from several countries, including the United States, Australia/New Zealand, and Canada.5-10 CHIP includes a strong educative component to change the participants’ attitudes toward healthy living, group support to help foster social norms that promote healthy lifestyle, and regular health risk assessments to increase the participants’ health related self-efficacy and perceived control.
CHIP has been demonstrated to achieve meaningful reductions in selected risk factors, including body mass index (BMI), blood pressure (BP), total cholesterol (TC), low-density lipoprotein (LDL), triglycerides (TG), and fasting plasma glucose (FPG) among large cohorts from several countries.5-10 Furthermore, the reduction in risk factors and self-reported adherence to the health behaviors promoted in the intervention have been found to occur over the long-term, indicating that CHIP is a useful intervention for enabling behavior change.11,12
The CHIP lifestyle intervention has been delivered by professional and unpaid volunteers in various workplaces, community, and medical settings.5-10 While lifestyle modification programs can be delivered by both paid professional or unpaid volunteer facilitators, there is a common perception that lifestyle modification programs delivered by trained, experienced, healthcare professionals have greater effectiveness than those delivered by volunteers. 13 Volunteers, in most cases, do not have the same training or experience as trained healthcare professionals and because remuneration cannot be used as an inducement it can be more difficult to motivate and control volunteers. However, the costs associated with paid professionals can greatly inflate the cost of delivering the lifestyle modification programs, which can result in these programs being out of the reach of a significant proportion of the population.
Whilst the outcomes following CHIP programs delivered by professionals and unpaid volunteers have been reported in the literature, a detailed analysis of the differential responsiveness to professional and volunteer facilitators has not been performed. This study compared the outcomes of individuals participating in the CHIP lifestyle intervention delivered by paid professional versus volunteer facilitators in the United States.
Methods
Participants
The professional-delivered CHIP intervention was delivered to 3158 participants who were largely college educated with higher income ($>50,000/year), who had self-selected to participate in the program between 1999 and 2004 in Rockford, Illinois. Eligibility criteria for this study were ≥21 years; able to engage in walking exercises; and able to pay the program fee ($290-$395 professional-delivered program and $200 volunteer-delivered program), with some participants provided a needs-based subsidy and others receiving some employer subsidy. The cost charged for the professional-delivered program covered hiring an impressive auditorium and payment of keynote speakers to create a professional environment for employees of the Swedish American Health System. On the other hand, the intention of the volunteer-delivered programs was to provide the same program to the wider community by securing a venue at low cost or free and trained facilitators who donated their time. Exclusion criteria were ≤3 months post bypass surgery; undergoing treatment for cancer; and/or affected by a substance use disorder.14,15
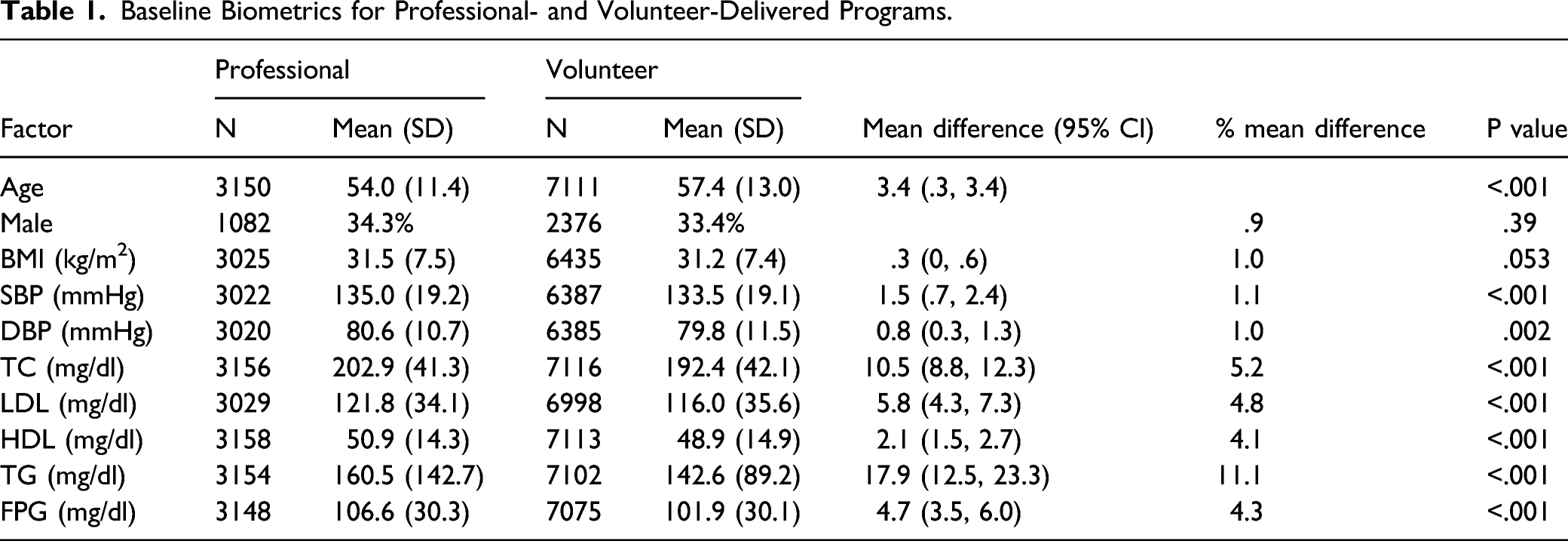
Baseline Biometrics for Professional- and Volunteer-Delivered Programs.
Facilitator Information
The professional-delivered programs were coordinated by the Swedish American Health System in Rockford Illinois. The facilitators were required to attend a two-day training workshop to acquire an overview of the program and the screening procedure. Program facilitators were predominantly physicians, nurses, dietitians, or corporate health promotion professionals. 18
The volunteer-delivered CHIP programs were conducted by unpaid volunteer facilitators—sourced primarily through the Seventh-day Adventist Church—who had an interest in positively influencing the health of their local community. There were no educational requirements or selection criteria for the volunteer facilitators. However, all volunteers were required to undergo two days of training to learn about the CHIP intervention and develop group facilitation skills. The training of both professional and volunteer facilitators followed the procedure outlined in the Facilitator Manual, which instructed both facilitator types to deliver the CHIP intervention using a standardized curriculum package (described below). Facilitators were also trained to administer and interpret the standardized Health Risk Assessment tool (HRA). As such, the role of both the professional and volunteer facilitators was to organize the meetings and facilitate discussion, not provide individual input into educating and instructing participants in lifestyle intervention.
Description of CHIP
The CHIP intervention sessions were structured around a model of learn, experience, and reflect. 19 The intervention in both streams involved 16 two-hour group sessions, delivered four days a week, over 30 days. All educational, instructional and discussion material for both groups came from the same curriculum package. The educational component involved viewing a pre-recorded lecture on the session’s health topic. A textbook was also provided to the participants to consolidate and reference the material presented in the video. Further, the participants were provided with a workbook that encouraged self-reflection and guided discussion. The use of the supplied resources in the curriculum package resulted in the program being delivery consistently by all the facilitators.
Participants in both streams were educated on the etiology of chronic disease and the benefits of positive lifestyle choices, with particular attention given to encouraging and supporting the consumption of a low-fat (<15% of calories from fat), plant-based ad libitum diet. In addition, the program advocated that participants engage daily in 30 minutes of moderate physical activity (walking) and practice stress management techniques (life balance, sleep, and rest). Behavior change programs that include these components have been shown to be effective at reducing chronic disease by Ornish et al. 4 In addition, sessions relating to behavior change (i.e., overcoming barriers to change, developing emotional intelligence, self-monitoring, goal setting, and problem solving) were also included. For more information about the CHIP intervention, refer to the review article by Morton et al. 19
The participants were deemed to have completed the initial 30 days of the program if they attended 13 of the 16 sessions and underwent both pre- and post-assessments. Before participating in the CHIP intervention (baseline) and again at its conclusion (post-intervention), the participants’ height, weight, SBP, and DBP were taken and fasting (8-hour) blood samples were collected. These measures were originally collected as the program focused on reducing selected CVD risk factors, but due to ease of collection, the fidelity of data collection remained to the present day. The same scales and sphygmomanometer were used for measuring blood pressure at baseline and again at 30-days and was measured by a health professional. The blood samples were collected by trained phlebotomists and analyzed by local pathology laboratories for TC, LDL, HDL, TG, and FPG levels. A standardized HRA was used to record biometric data and also collect information on the participant. Demographic information of age, gender, marital status, education and household income were collected for the professional-delivered groups, while only age, gender, and marital status were collected for the volunteer-delivered groups at baseline. Participant names and identifying information were removed prior to analysis.
Statistical Analysis
The data were analyzed using SPSS™ Statistics (version 21) between June and November 2018. Differences in age and baseline biometric measures between participants in the two program streams were compared using independent t-tests. Chi-square was used to assess differences in the gender balance of the groups. Findings were reported as mean ± SD as the data was deemed to approximate normality because of the large sample size. 20 For difference in changes from baseline to 30 days in professional versus volunteer-delivered programs, Analysis of Covariance (ANCOVA), with adjustment for age, gender, BMI change, and baseline biometric, was used for each biometric. The confidence intervals for the mean were adjusted by applying a Bonferroni correction. The data was explored for interaction effect between age and group type, and gender and group type. If a significant interaction was found the difference in outcomes between the groups was explored for each age group or gender using t-tests. A P value of less than .05 was considered significant.
Results
There was no significant difference (P = .39) in the gender balance between the participants in professional-delivered program (n = 3158), 34% men, 66% women) compared to the volunteer-delivered programs (n = 7115, 33% men, 67% women). The participants in the volunteer-delivered programs (57.4 ± 13.0 years) were marginally older than participants in the professional-delivered programs (54.0 ± 11.4 years) (P < .001).
At baseline, the differences in baseline biometric measures between professional- and volunteer-delivered groups, although statistically significant, were minimal (Table 1).
Comparison of Differences in Change in Selected Biometrics for Professional- and Volunteer-Delivered Groups Post-Intervention.
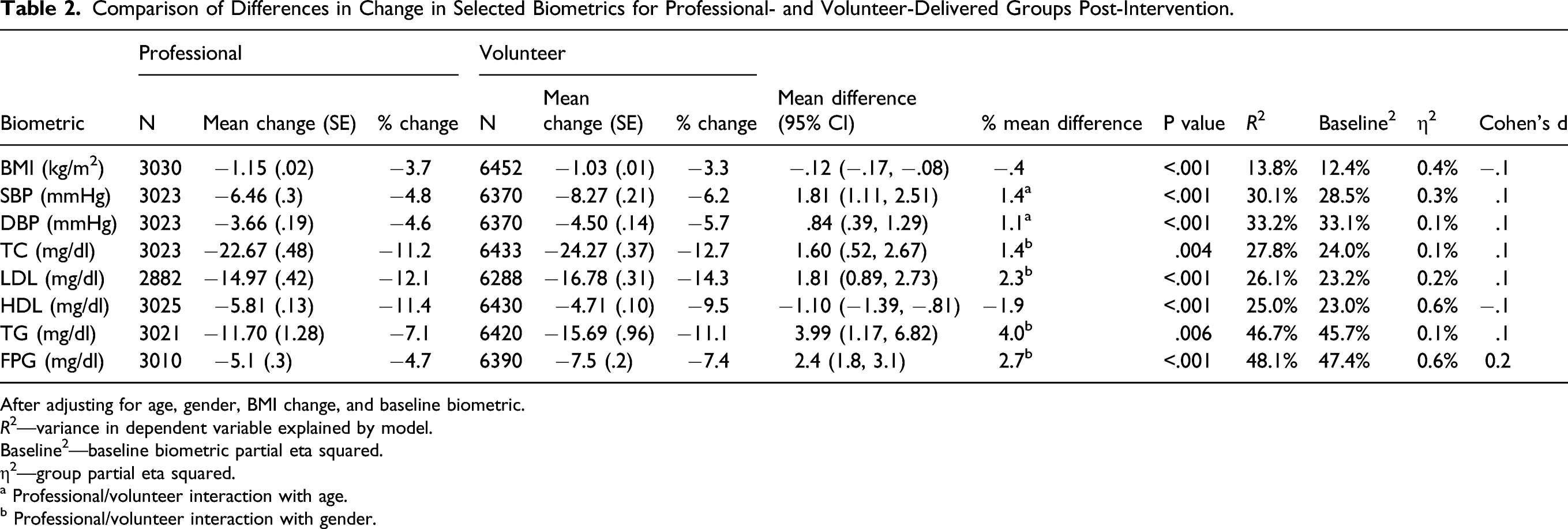
After adjusting for age, gender, BMI change, and baseline biometric.
R2—variance in dependent variable explained by model.
Baseline2—baseline biometric partial eta squared.
η2—group partial eta squared.
a Professional/volunteer interaction with age.
b Professional/volunteer interaction with gender.
Comparison of Differences in Change in Blood Pressure by Age Group for Professional- and Volunteer-Delivered Groups Post-Intervention.
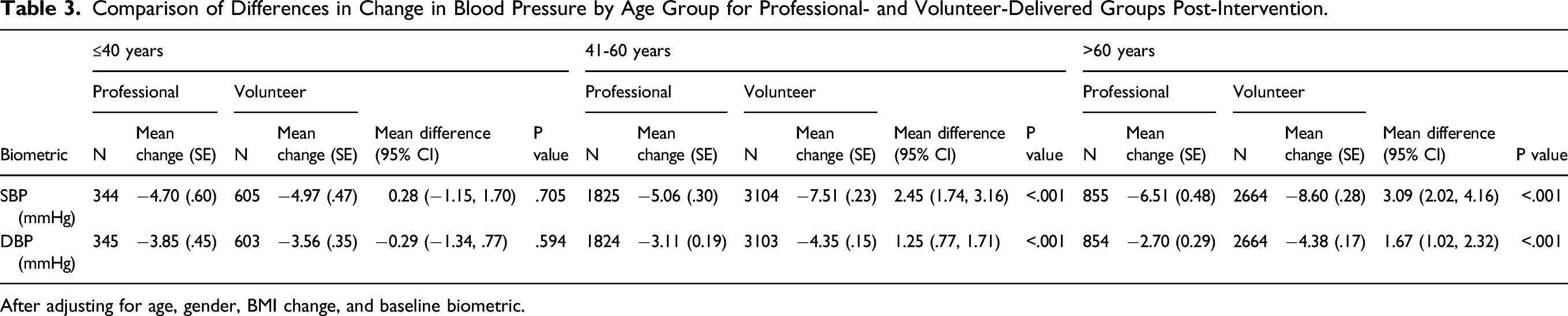
After adjusting for age, gender, BMI change, and baseline biometric.
Comparison of Differences in Change in Blood Biometrics by Gender for Professional- and Volunteer-Delivered Groups Post-Intervention.
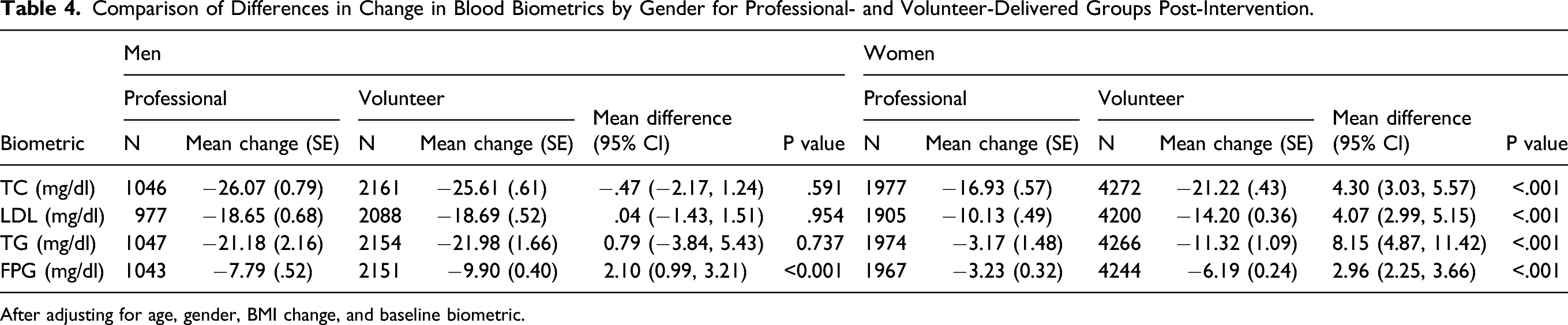
After adjusting for age, gender, BMI change, and baseline biometric.
Loss to follow-up was comparable in both program types with 93% of participants in the professional-delivered program and 94% in the volunteer-delivered programs meeting the criteria for completion (attending 13 of 16 sessions).
Discussion
As stated in the introduction, there is a common misperception that lifestyle modification programs that are delivered by trained, experienced healthcare professionals have greater effectiveness in program delivery and improving health outcomes than those delivered by volunteers. 13 This study indicates that if the program is well-structured and provides facilitators with comprehensive training video-based programs may be a powerful resource for effecting change in health metrics, regardless of whether they are delivered in clinical or community settings by health professional or volunteers.
Notwithstanding limitations on training and a lack of remuneration as a motivator, evidence suggests that adequately resourced volunteers can be effectively utilized in the delivery of community programs. Volunteers from “Faith in Action” groups were successfully used to safely deliver the Strong for Life program to elderly frail people. 21 Furthermore, people with diabetes benefited from the community-based peer-delivered Diabetes Self-Management Program with lasting effects up to 12 months. 22 Delivery of health promotion programs by volunteers allows for wider program dissemination than is possible using only professional leaders. 23 In addition, a Diabetes Prevention Program structured and adapted to the real-world showed significant and sustained clinical weight reduction in people at high risk for diabetes. 24 Moreover, a recent systematic review showed community health volunteers could help improve access to and use of essential health services in low–middle-income countries as well as, and sometimes better than, health workers. 25 However, volunteers were found to be less well equipped in diagnosis and counseling. The function of the volunteers in the present study was no different to that of professional facilitators in that they organized the meetings and facilitated discussions around a standardized set of items and questions predeveloped for the workbook. In this program, costs were lowered by using lay staff, without sacrificing effectiveness.
The use of volunteer facilitator’s means that lifestyle interventions can be delivered at a significantly reduced cost when compared with professional-delivered programs. 26 Additionally, is has been observed that for a community (or worksite) program to be successful, at least one person must champion the program. 27 Volunteers, who are members of the local community (or worksite), already have relationships with individuals in these settings which can be utilized to encourage members to be proactive about their health and make necessary life changes. 28 This means that they are often better placed than paid professionals to champion a program, as a passionate volunteer can incite their peers to action. 28 In addition, friendship and social networks, which are tapped into by peer volunteers, have been shown to be a useful contributor to positive health behavior. 29
We recently reported that CHIP effectively reduced chronic disease risk factors among both genders, but particularly men, with the largest reductions occurring in individuals at greatest risk. 30 Whilst we discussed various physiological or behavioral factors that could explain the differences, including differences in adiposity and hormones, dietary intake, commitment, and social support, we also discussed how men are more inclined to commit to a program if the benefits outweigh the costs. 31 Indeed, once men have made a decision, they are more likely to complete a program that is prescriptive 32 and achieve their goals, 33 particularly if advised by a health professional. 34 On the other hand, women are inclined to commit to interventions for social reasons (trust, interaction, and obligations to significant others). 31 These reasons may elucidate the findings in this study that women in the volunteer-delivered programs achieve greater reductions than men, while men achieve greater reductions overall in both programs.
Volunteering has also been shown to have significant benefits for those who volunteer. 35 A study of older volunteers reported that they felt they were “a great deal better off” for having volunteered and that the benefits of volunteering were also felt by their families. 36 Volunteering in peer educational programs has been found to be a positive and rewarding experience. 37 The motivations for volunteering in university student peer health educators ranged from altruistic motives such as wanting to help others to self-efficacy beliefs, and the need to satisfy personal health goals. 38 Indeed, volunteers of programs targeting drug and sexual behavior have reported making positive lifestyle changes as a result of the information they learned while volunteering. 26
While the ability to utilize volunteers depends on the availability and commitment of the volunteers, the utilization of volunteers maximizes the use of social and human capital. If a significant initial investment is made in social and human capital, other forms of capital, such as financial, physical, and natural, are not always necessary. 39 As volunteer-delivered interventions appear to be as effective as professional-delivered programs, the utilization of voluntary facilitators can dramatically increase the scope of these interventions while keeping costs to a minimum.
A seemingly adverse outcome of the CHIP intervention is the reduction in HDL among participants in both professional- and volunteer-delivered program, which has also been observed in other lifestyle interventions that promote a plant-based eating pattern. 4 However, this reduction in HDL is not considered detrimental to the risk of chronic disease when a whole foods plant-based diet is adopted, as discussed by Kent et al. 40
As the direct (medical) and indirect (productivity) costs of chronic disease are projected to increase, for example, for cardiovascular disease from $450 billion in 2010 to more than $1 trillion (with great impact on corporate medical care costs) by 2030, 41 the reach of evidence-based chronic disease education programs must be expanded. Volunteers may be part of the solution as they can present these programs in a variety of venues and less expensive program types. This is expected to have appealing benefits to the worksite and to insurance companies. Shurney et al (2012) showed a saving in total healthcare costs (medical and prescription drug) of almost $100,000 over 6 months for a workplace-based CHIP program delivered to 21 participants. In this study, the return of investment for this period was 2.1:1. 42
Limitations
This study has shown that the CHIP intervention when delivered by volunteer facilitators achieved comparable results to that of professional-delivered programs. However, a significant limitation of this study is that as data on programs facilitated by professionals and volunteers came from two non-overlapping time periods, implementation of programs may have varied thereby potentially compromising implementation fidelity. The authors do not believe this to be the case due to the standardized structured and nature of the program, with the same content presented in pre-recorded videos, the same data collection processes and the comprehensive training of facilitators. Notably, studies of the CHIP intervention from countries outside the United States show similar outcomes. 43
Another limitation was that demographic information on the professional and volunteer facilitators was not collected. Whilst participant data on age, gender, marital status, education, and household income was collected in professional-delivered programs, education and household income was not collected in the volunteer-delivered program, nor was ethnicity collected in either program. Furthermore, while data on professional-delivered programs came from programs in Rockford Illinois, those that for volunteer-delivered programs came from across the United States. Together, any differences in demographic data could potentially confound outcomes as this may have impacted the extent of participant engagement with the program. The authors do not believe potential differences in either situation would have affected outcomes due to the structured nature of the program, as well as similar outcomes from CHIP interventions conducted in countries outside the United States. Moreover, as volunteer facilitators were mainly sourced from the Seventh-day Adventist Church, which has a strong interest in the promotion of health and well-being, they may have been more highly motivated to ensure the success of the program, thereby confounding the study outcomes. Future studies should collect information on the ethnicity/race, income, education, and religiosity of facilitators and participants.
A further limitation is the unequal sample size of the professional- and volunteer-delivered program. As the volunteer-delivered group was more than twice as large as the professional-delivered group, homogeneity of variance becomes important. However, as stated by the Central Limit Theorem, when samples are large, they approximate a normal distribution. In this study, both the professional- and volunteer-delivered programs are very large and so the issue of unequal sample size becomes negligible.
In the absence of a control group, the extent to which regression to the mean explains the observed improvements in the volunteer-delivered programs cannot be determined. Consistent with regression to the mean is that the individuals with the most extreme baseline measures tended to experience the greatest improvements and hence inclination toward the norm. However, given the large size of the sample and that in some of the outcomes measured the high-risk classifications moved 1.5 to 2 standard deviations, regression to the mean likely only explains a small component of the observed results. Nevertheless, some professional-delivered studies of CHIP have demonstrated the effectiveness of the intervention using a randomized control design and the magnitude of change observed in volunteer-delivered groups is similar to the treatment groups of these studies.40,41
Future Research
As lifestyle interventions, such as CHIP, continue to expand globally, more research needs to be undertaken to establish how to best meet the different needs of male and female participants of all ages. Future research should explore the gender and age-specific physiological and/or behavioral factors that contribute to responsiveness to lifestyle change to assist in the development of more effective lifestyle interventions for all participants. The use of mixed-method triangulation research designs would likely provide rich insights and renewed understandings of participant and facilitator perception, satisfaction and lived experience of lifestyle intervention programs. In addition, future research should identify facilitator personality styles—average, self-centered, role model, and reserved 44 —as this may explain current participant program engagement and therefore long-term impact of the program.
Lifestyle modification programs have been shown to be effective in the treatment of chronic disease. However, programs delivered by professional facilitators, though more costly, are believed to be more efficacious than those delivered by volunteers. This article provides further evidence that volunteers, that is, individuals who donate their time, can be just as effective as paid health professionals in the delivery of CHIP interventions for reducing selected chronic disease risk factors. Lifestyle interventions that are well-structured and provide volunteer facilitators with comprehensive training can dramatically increase the reach to more individuals with chronic disease, while keeping costs to a minimum. Future research should focus on the use of different facilitator types and their long-term impact on participants.So What?
Implications for Health Promotion Practitioners and Researchers
What Is Already Known on This Topic?
What Does This Article Add?
What Are the Implications for Health Promotion Practice or Research?
Footnotes
Author Contributions
Lillian M. Kent: conceptualization, data analysis, and writing—original draft, review, and editing.
Paul M. Rankin: conceptualization, investigation, and writing—review and editing.
Darren P. Morton: methodology and writing—review and editing.
Rebekah M. Rankin: investigation, data analysis, and writing—review and editing.
Roger L. Greenlaw: conceptualization, data acquisition, curation, writing—review and editing—and supervision.
Heine S. Englert: conceptualization, investigation, and writing—review and editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors for the research, authorship, and/or publication of this article.
Human subject approval statement
Ethics consent was obtained from Avondale College of Higher Education Ethics Committee (IRB) (approval number 20:10:07).
Consent to participate
Written informed consent to participate was obtained from the participants.