
Abstract
Keywords
Introduction
The Advisory Committee on Immunization Practices (ACIP) recommends routine use of HPV vaccination for females and males between ages 11 and 12 years and catch-up HPV vaccination for all persons through age 26 years. 1 Yet, HPV vaccination is well below Healthy People 2030s goal of 80% completion rate for adolescents. 2 The rates for adolescents 13–17 who are up-to-date on the recommended HPV vaccine doses were 54% nationally and 52% in New Jersey for females; and 49% nationally and 46% in New Jersey for males.3,4 Moreover, site-based studies in New Jersey found lower rates of HPV vaccine uptake among adolescents younger adolescents (11–12 years) and those seen by non-pediatric HCPs.5-7 Several studies have shown that healthcare provider (HCP) recommendation of the HPV vaccine is associated with increased uptake8-12 as well with fewer parental refusals and delays for the HPV vaccine. 13 Despite the critical role of HCPs in improving HPV vaccine uptake, the proportion of HCPs who report discussing the HPV vaccine with parents of adolescents in the target adolescent age groups ranges between 35% and 48%.14-16 It is worthwhile to note that studies have defined HCPs differently by including physicians, nurse practitioners (NPs), physician assistants (PAs), or combinations of these groups.
The HCPs’ knowledge, attitudes, and beliefs about HPV, the vaccine, and HPV vaccine recommendations can affect their recommendation behaviors 17 and the quality/strength of recommendation. 18 Barriers to recommendations include HCPs’ lack of HPV and vaccine knowledge, negative beliefs about vaccine safety and efficacy, discomfort discussing sexuality, and low self-confidence to address parents’ concerns.15,19,20 Higher rates of parental refusals and deferrals have been associated with providers anticipating an uncomfortable conversation with parents, not strongly recommending the vaccine, and/or differentially recommending vaccination based on patient and parent factors.21,22 For example, instead of following age-based recommendations, some HCPs defer the discussion when they perceive patients to be low risk or too young or parents to be hesitant.23,24
Differences in recommendation behaviors, strength of recommendation, and vaccination uptake have been noted by provider specialty. Pediatricians are more likely to make strong recommendations using a presumptive approach compared to family physicians. 25 Barriers to vaccine recommendation have also been identified across type of provider. Although confidence in safety and efficacy of the vaccine is similar across different types of providers, physicians have reported more perceived barriers than PAs or NPs. 26 In addition, practice-related factors that influence provider knowledge, recommendations, and uptake include participation in Vaccines for Children (VFC) and clinical decision support and reminders.27,28 Thus, it is important to understand contextual factors about practice settings as they relate to HCPs’ knowledge about HPV vaccine and vaccination guidelines.
In conclusion, existing literature has focused the communication behaviors of HCPs (i.e., recommendation behaviors and the quality/strength of recommendation) and their impact on the HPV vaccine uptake. However, little is known about the specific factors that influence HCPs’ recommendations of HPV vaccination. More specifically, existing literature has focused predominantly on HCPs’ characteristics, with little attention on the impact of practice characteristics on HCPs’ recommendations of HPV vaccination. Further, given the rising demand for primary care practitioners, 28 existing studies are lacking in their sampling approaches that are representative of the primary care workforce diversity, particularly the different types of professions and specialties. This study contributes to the existing literature by addressing both HCP and practice characteristic and by being inclusive of both physicians and NPs as well as providers working in both pediatric and non-pediatric specialties. More importantly, this study focuses on New Jersey, in which HPV vaccine uptake is lower than national levels.3,4 Therefore, the purpose of this study was to examine factors associated with HCPs’ recommendation of HPV vaccination for younger and older adolescents. The factors examined in this study included both HCP and practice characteristics.
Methods
This is a cross-sectional study, using an anonymous, web-based survey of 390 HCPs in New Jersey. Eligible providers included being a physician or NP and working pediatrics, women’s health or OB/GYN, and family medicine or family health. We recruited HCPs through email announcements sent to Vaccines for Children (VFC) Program participants, members of the New Jersey Chapter of the American Academy of Pediatrics, and members of the Advanced Practice Nurses of New Jersey. In addition, flyers about the study were distributed at local pediatric, family medicine, women’s health, and immunization meetings. Survey responses were collected from January to December 2018. All study participants were offered the option of receiving a US$20 gift card incentive for completing the survey; and 80% indicated their interest in receiving the incentive, which was mailed to an address of their choice. This study was reviewed and approved by Rutgers University, Institutional Review Board. Study participants were provided informed consent on the first page of the online survey and were asked to click a button on the web-based survey to indicate their agreement to participate in the study, which was required for participants to take part in the study.
Survey Instrument
The 60-item survey assessed HCPs’ knowledge, beliefs (perceived effectiveness and concerns), and perceived barriers and facilitators. Survey items were adapted from published measures in this area of research.15,20,29-31 Furthermore, we have conducted qualitative interviews with 8 HCPs in pediatric, women’s health, and family medicine to review the survey items and identify missing areas. These interviews resulted in adding items around perceived concerns, barriers, and facilitators.
Study Outcome
The main outcome, HCPs’ HPV vaccine recommendation, was assessed using the following question: “In the past 12 months, how often did you recommend the HPV vaccine to your patients?” for younger (11–13 years old) and older (14–17 years old) adolescents. This comparison most closely reflects recommendation practices based on national guidelines. 32 Response options included qualitative descriptors and quantitative estimates on the following scale: “never” (0%), “rarely” (1–25%), “sometimes” (26–50%), “often” (51–75%), or “always” (>75%). We created a binary outcome measure to indicate those who reported “always” recommending the HPV vaccine (>75% of the time) for the analyses compared to those who responded in the other four categories. This approach for measuring HCPs’ recommendation has frequently been used in similar studies.15,27,33
Study Predictors
The survey included 6 items on knowledge about the vaccine scored on a 3-point scale (1 = not familiar to 3 = very familiar), 3 items on perceived vaccine effectiveness and 7 items on concerns about the vaccine scored on a 4-point scale (1 = strongly disagree to 4 = strongly agree), 10 items on perceived barriers for recommending HPV vaccination scored on a 3-point scale (1 = never to 3 = always), and 7 items on perceived facilitators for recommending HPV vaccination scored on a 4-point scale (1 = strongly disagree to 4 = strongly agree). Perceived concerns items addressed HPV vaccine safety, long-term effects, drug companies’ motivations, and sexual health behavior consequences. Perceived barriers included system-related barriers (5 items) on issues with ordering, stocking, or administering the HPV vaccine and barriers communicating with parents about the vaccine (5 items). The facilitators included whether their colleagues recommend the HPV vaccine, the use of vaccination quality indicators in staff meeting discussions, involvement in immunization or cancer prevention coalitions, and awareness of national and professional organizations recommendations on HPV vaccination. Survey items on knowledge, beliefs, and perceived barriers and facilitators have demonstrated adequate validity and reliability in previous studies.15,30,31 In this study, the Cronbach alpha reliability coefficients were .868 for knowledge items, .838 for perceived vaccine effectiveness items, .920 for perceived concerns items, .821 perceived barriers items, and .709 for perceived facilitators items. In addition, the survey included items about the HCPs’ demographics characteristics (i.e., gender, profession, and specialty) as well as practice characteristics (i.e., proportions of race/ethnicity, adolescents, public/private insurance, and VFC recipients).
Data Analysis
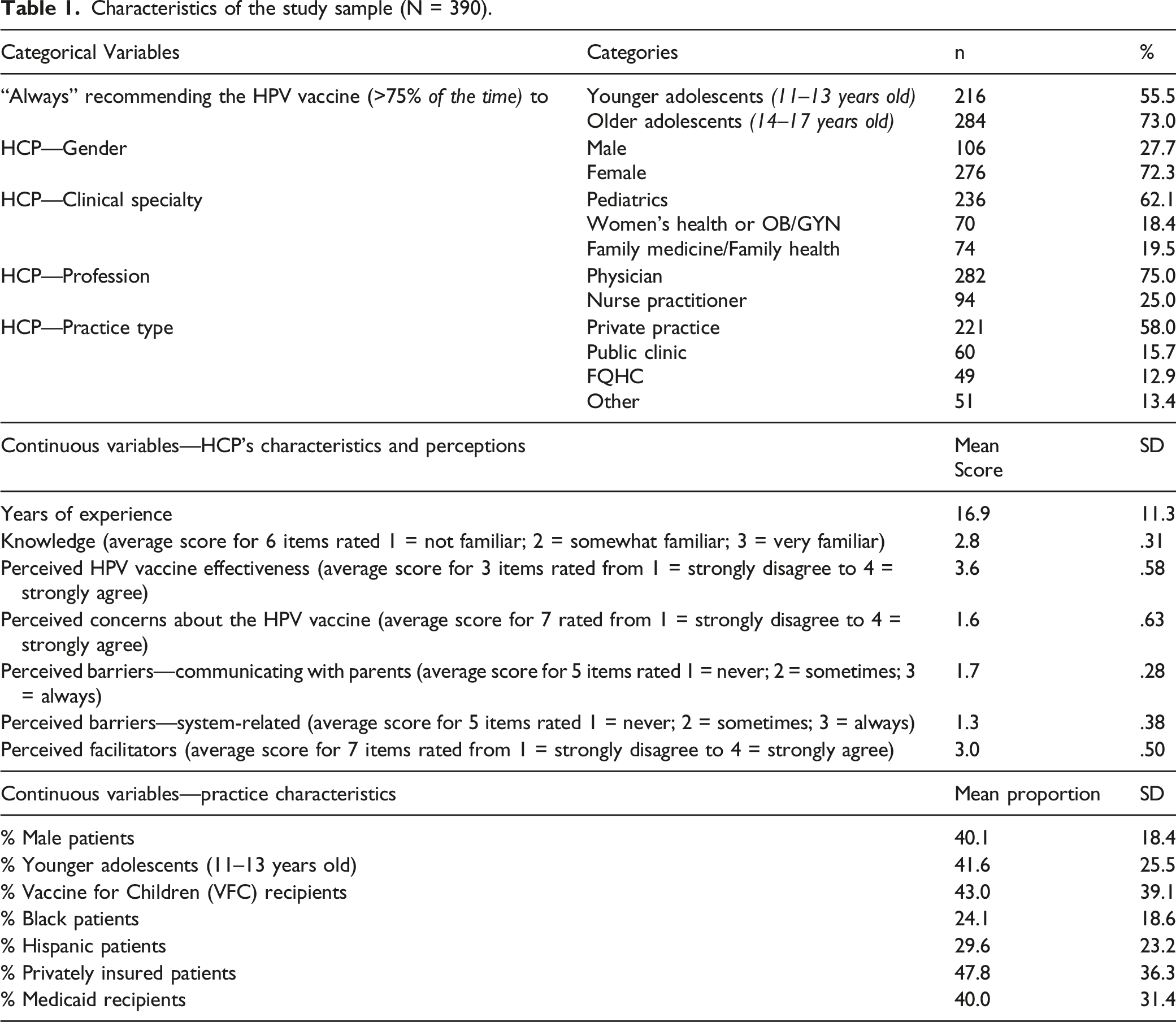
Characteristics of the study sample (N = 390).
Logistic regression analysis of HCP’s recommendation of HPV vaccination.
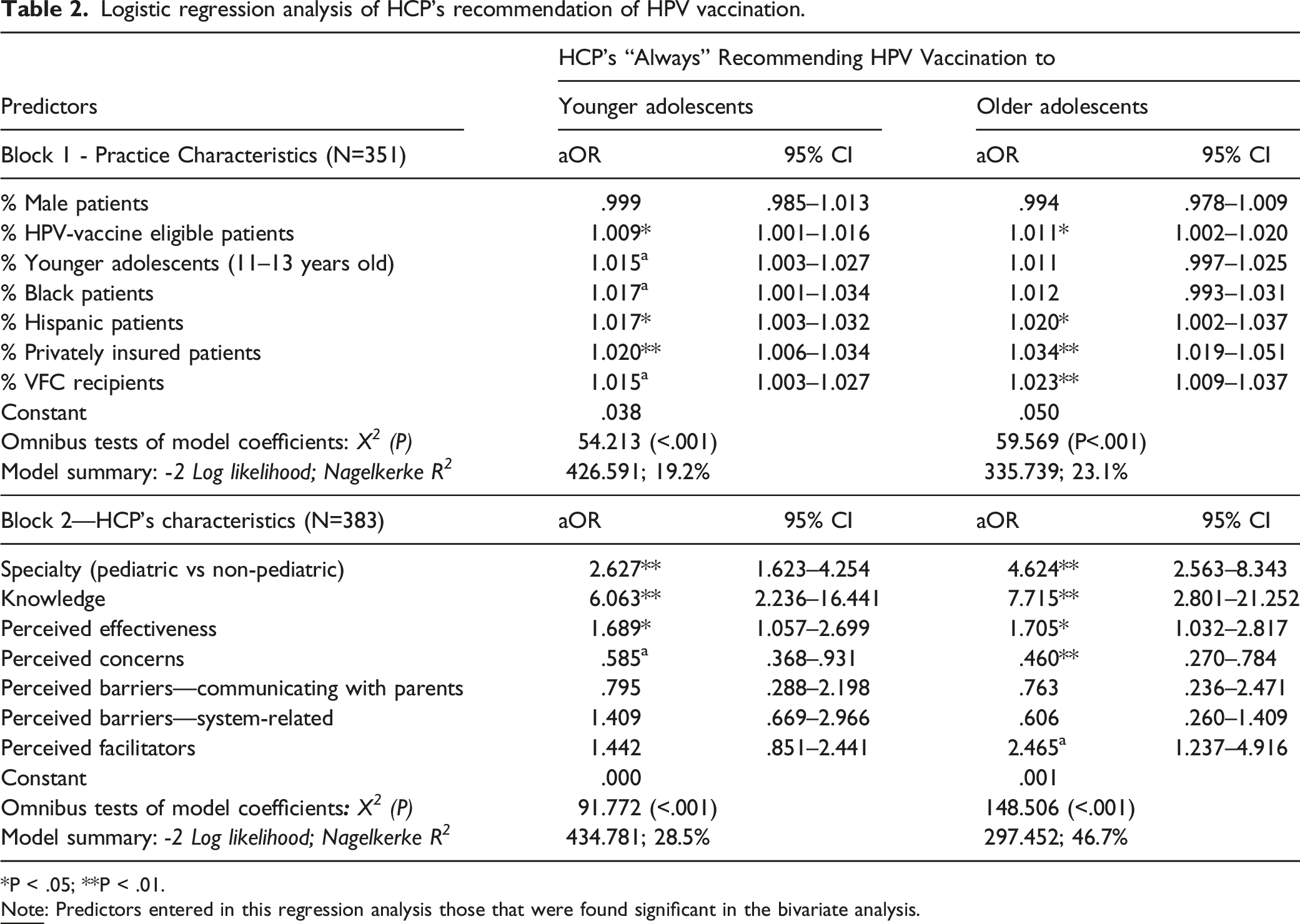
P < .05; **P < .01.
Logistic regression analysis of the surviving predictors for HCP’s recommendation of HPV vaccination, using backward stepwise Wald method.
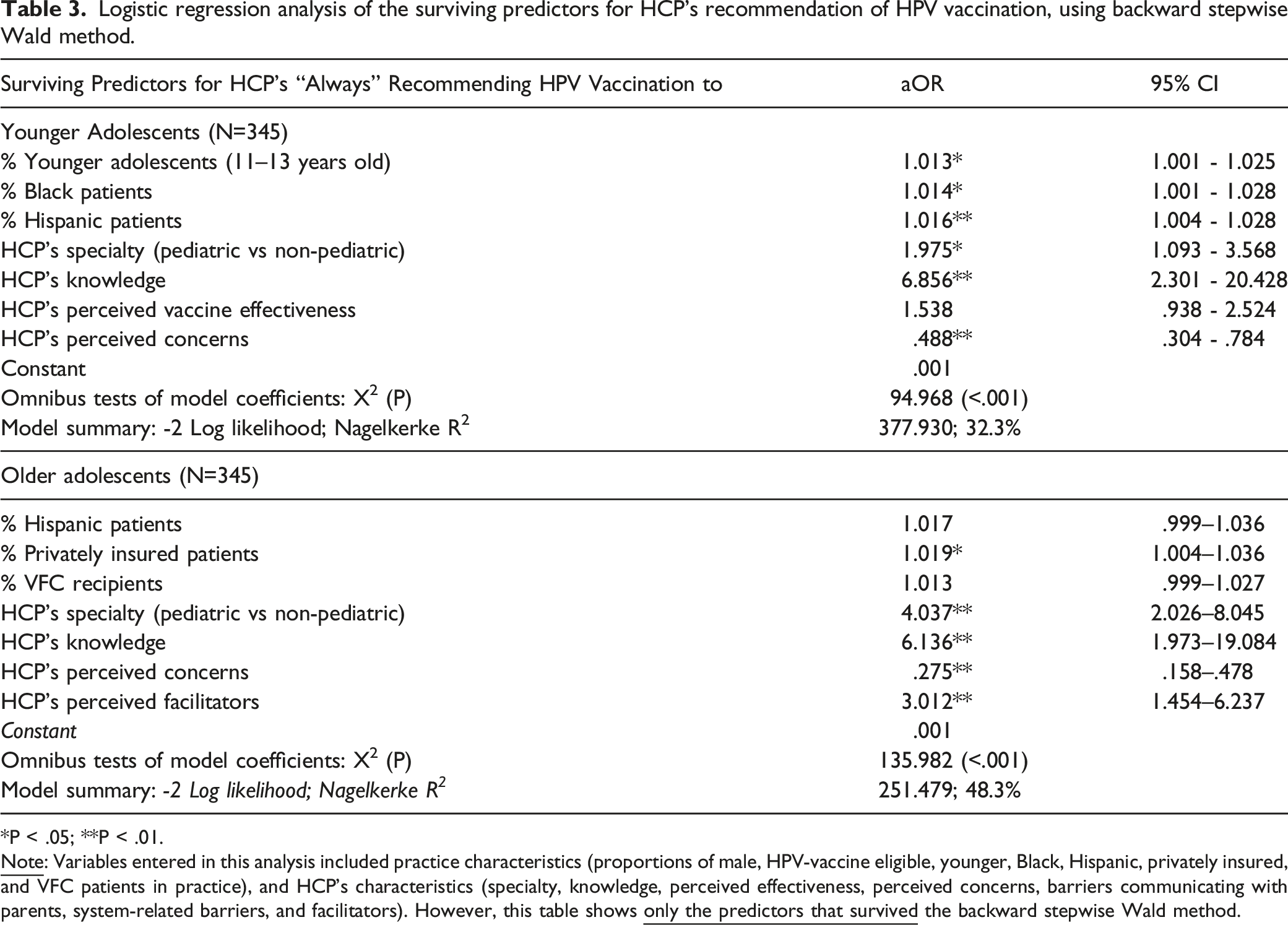
P < .05; **P < .01.
Results
Sample Characteristics
We recruited 390 HCPs, including physicians (75%) and NPs (25%) who worked in the areas of pediatrics (62%), women’s health or OB/GYN (18%), and family medicine/health (20%) (Table 1). Fifty-eight percent worked in private practice and their practices had, on average, 40% male, 42% younger adolescents (11–13 years old), 43% VFC recipients, 24% Black, 30% Hispanic, 48% with private insurance, and 40% Medicaid recipients. The rates of “always” recommending the HPV vaccine (>75% of the time) were 56% for younger adolescents (11–13 years old) and 73% for older adolescents 14–17 years old.
Predictors of HCP Recommendation of HPV Vaccination for Younger Adolescents
Regarding practice characteristics (Table 2), HCP “always” recommending the HPV vaccine to younger adolescents (11–13 years old) was significantly associated with practices that reported higher proportions of HPV-vaccine eligible patients, younger adolescents (11–13 years old), Black and Hispanic patients, patients with private insurance, and VFC recipients in the HCP’s practice (X2 = 54.213; P < .001). These variables predicted 19% of the variance in HCP’s recommendation of the HPV vaccine for younger adolescents. Regarding provider characteristics (Table 2), HCP “always” recommending the HPV vaccine to younger adolescents was significantly associated with HCP’s pediatric specialty, higher levels of knowledge and perceived effectiveness of the vaccine, and lower levels of concern about the vaccine (X2 = 120.722; P < .001). These variables predicted 29% of the variance in HCP’s recommendation of the HPV vaccine for younger adolescents.
Using a backward stepwise Wald method for both practice and provider characteristics (Table 3), HCP recommendation of HPV vaccination for younger adolescents was significantly associated with proportions of younger adolescents (11–13 years old), Black and Hispanic patients, and HCP’s specialty, knowledge, and perceived concerns about the HPV vaccine (X2 = 94.968; P < .001). Variables in this analysis explained 32% of the variability in HCP’s recommendation of HPV vaccination for younger adolescents. Focusing on the strongest predictors, the adjusted odds of HCP recommendation of HPV vaccination for younger adolescents are nearly 2 times higher among pediatric than non-pediatric providers (aOR: 1.975; 95% CI: 1.093–3.568), 7 times higher with increased HCP’s knowledge scores (aOR: 6.876; 95% CI: 2.301–20.428), and 51% lower with increased scores for HCP’s perceived concerns about the vaccine (aOR: .488; 95% CI: .304–.784). In the backward stepwise approach, predictors that did not survive the analysis because they were not statistically significant included the proportions of male, privately insured, and VFC patients; and the HCP’s perceived barriers (both communicating with parents and system-related barriers) and facilitators for recommending HPV vaccination.
Predictors of HCP Recommendation of HPV Vaccination for Older Adolescents
Regarding practice characteristics (Table 2), HCP “always” recommending the HPV vaccine to older adolescents (14-17 years old) was significantly associated with practices that reported higher proportions of HPV-vaccine eligible patients, Hispanic patients, patients with private insurance, and VFC recipients in the HCP’s practice (X2 = 59.569; P < .001). These variables predicted 23% of the variance in HCP’s recommendation of the HPV vaccine for older adolescents. Regarding provider characteristics (Table 2), HCP “always” recommending the HPV vaccine to older adolescents was significantly associated with HCP’s pediatric specialty, higher levels of knowledge about and perceived effectiveness of the vaccine, lower levels of concern about the vaccine, and higher levels of facilitators (X2 = 120.722; P < .001). These variables predicted 47% of the variance in HCP’s recommendation of the HPV vaccine for older adolescents.
Using a backward stepwise Wald method for both practice and provider characteristics (Table 3), HCP recommendation of HPV vaccination for older adolescents was significantly associated with the proportion of privately insurance patients and with HCP’s specialty, knowledge, perceived concerns about the HPV vaccine, and facilitators (X2 = 135.982; P < .001). Variables in this analysis predicted 48% of the variability in HCP’s recommendation of HPV vaccination for older adolescents. Focusing on the strongest predictors, the adjusted odds of HCP recommendation of HPV vaccination for older adolescents are 4 times higher among pediatric than non-pediatric providers (aOR: 4.037; 95% CI: 2.026–8.045), 6 times higher with increased HCP’s knowledge scores (aOR: 6.136; 95% CI: 1.973–19.084), 73% lower with increased HCP’s score for perceived concerns about the vaccine (aOR: .275; 95% CI: .158–.478), and 3 times higher with increased HCP’s scores for facilitators (aOR: 3.012; 95% CI: 1.454–6.237). In the backward stepwise approach, predictors that did not survive the analysis because they were not statistically significant include the proportions of male, younger, and Black patients; and the HCP’s perceived vaccine effectiveness and their perceived barriers (both communicating with parents and system-related barriers).
Discussion
In this survey of HCPs, both physicians and NPs, we found that the rates of “always” recommending HPV vaccination were 56% for younger adolescents and 73% for older adolescents; and different psychosocial factors and practice characteristics were significantly associated with recommendations by adolescent age. The HCPs’ pediatric specialty and HPV vaccination knowledge were key drivers in recommendations for both young and old adolescents. Although HCP perceived barriers in communicating with parents were not significantly associated with recommendations in either age group, perceived concerns score was negatively associated with recommendations.
We found a greater proportion of HCPs always recommended the vaccine for older (aged 14–17 years) compared to younger (aged 11–13 years) adolescents. The rate for younger adolescents (56%) is slightly higher than rates reported in other studies for 2011–2014, which ranged between 35% and 48%.14-16 However, they are much lower than rates reported in more recent literature, which ranged between 74% and 99%.24,36 This is consistent with higher vaccination rates among teenagers than younger adolescents 37 as well as studies showing that providers make stronger recommendations for older adolescents 18 and receive less resistance compared to younger adolescents. 24 Furthermore, we found that HCP knowledge of the HPV vaccine significantly increased the odds of recommending the vaccine for adolescents of all ages. This is consistent with other researcher that documented how HCPs’ low HPV knowledge corresponded with low recommendation and that when professional society/colleagues’ norms were accepted, vaccination was higher. 11 Our findings support continued efforts to educate providers on HPV vaccination recommended age groups (particularly younger adolescents), especially delivery of strong recommendations, which has been emphasized in recent years through research and professional training on communication to improve the quality of recommendations. 38 However, in a systematic review, Rodriguez and colleagues 37 found that provider-targeted education interventions alone were insufficient to change vaccination outcomes.
Our study also found that some HCPs had concerns about the vaccine which was associated with lower odds of recommendations for younger and older adolescents. The perceived concerns in this study included HPV vaccine safety and long-term effects, the vaccine being pushed by drug companies to make money or “experimenting” on children, as well as concerns about the vaccine discouraging routine gynecologic examinations/Pap tests, increasing sexual promiscuity, and decreasing condom use. The lower odds of recommending HPV vaccination may also be due to provider’s low perceived risk of HPV among their patients in general, hesitancy to recommend too many vaccines in a single visit or concerns about sexual behaviors. 17 Others have documented that physicians were more likely to report patients being too young and getting too many shots as potential parental barriers compared to NPs or PAs. 25 Provider vaccine confidence has also been linked to perceived parental hesitancy, which can influence recommendations. 22 The findings of our study contributes to existing literature by identifying the effect of the HCPs’ beliefs about the HPV vaccine on their recommendation practices and the need to integrate strategies addressing those beliefs in provider-targeted interventions to increase confidence in the vaccine. In addition, more research is needed to understand the factors to contribute to varying levels of HCPs’ beliefs about the vaccine.
Further, we found that the facilitators were significant for older adolescent recommendations. The HCPs’ facilitators included in this study were whether colleagues recommend the HPV vaccine, involvement in immunization or cancer prevention coalitions, and awareness of national and professional organizations recommendations on HPV vaccination. Facilitator strategies, such as the use of quality improvement incentives, can improve HCPs’ recommendation of HPV vaccination as well as increase the vaccine uptake. 39 However, we did not find a significant association between facilitators and HCPs’ recommendation of the HPV vaccine among younger adolescents. The effect of facilitators could be overshadowed by the HCPs’ perceived concerns about vaccinating younger adolescents or their anticipation of resistance from parents of younger adolescents. This suggests the need for further examination of this relationship as well as exploring the effect of additional facilitators and clinic/health system-level interventions in increasing vaccination, particularly among younger adolescents.
We found that HCP specializing in pediatrics had higher odds of recommending the vaccine for both younger and older adolescents. Similarly, Kempe and colleagues 24 reported pediatricians being more likely to make strong recommendations and use a presumptive approach compared to family physicians, and that family physicians report more refusals/deferrals than pediatricians across all patient age levels. Pediatric providers have been and continue to be the drivers behind the efforts to promote HPV vaccination. 26 Regarding provider type, we did not observe significant differences in rates of recommending the vaccine by HCP type, and our sample included 25% NPs. This is consistent with the findings of Finney Rutten and collegues 12 and inconsistent with the findings of McRee and colleagues 27 who found lower rates of recommending HPV vaccination among NPs compared to physicians. Educational interventions have shown no differences in communication self-efficacy by specialty (pediatric or family medicine) or training (MD/DO or PA/family NP or RN), though PAs and family NPs were more engaged in course content. 40 Our findings as well as findings from others studies suggest vaccination promotion and training interventions should include a variety of HCP types and specialties involved in vaccination, including non-pediatric and non-physician providers.
In addition to HCPs’ characteristics, practice characteristics that were significantly associated with HCPs’ recommendation of HPV vaccination in our study were practice proportions of patients related to race/ethnicity, insurance status, and VFC participation. We found that HCPs who reported higher proportions of Black and Hispanic patients in their practice had also reported higher rates of recommending HPV vaccination for younger adolescents, which is consistent with other research. 15 Regarding insurance status, we found that HCPs who reported higher proportions of privately insured patients in their practice had also reported higher rates of recommending HPV vaccination for only older adolescents. This is partially consistent with the findings of Vadaparampila and colleges 15 who found not significant association with recommendation for younger adolescents; however, they did not investigate recommendation for older adolescents. Regarding VFC participation, we found that HCPs who reported higher proportions of VFC recipients in their practice had also reported higher rates of recommending HPV vaccination for older adolescents. This is consistent with the findings of other research. 15 This can be explained by lower reports of system-related barriers among HCP’s who participate in VFC programs, such as less vaccine stocking and reimbursement issues. 41
The study has several strengths, particularly the use of a relatively large and diverse sample that included both physicians and NPs, of different clinical specialties and clinical settings. A limitation of this study is its cross-sectional design, which hinders any conclusions of causation. Nevertheless, the associations uncovered in this study lay the ground for future research to utilize other research designs aimed at exploring and testing causations. In addition, due to the sensitive nature of HCPs reporting on their own professional practices, there is a possible risk that their responses were affected by social desirability (e.g., HCPs overstating their rates of recommending the HPV vaccine). Such risk was minimized in this study by using an online data collection and maintaining anonymity by not asking for names or any other identifiers. Lastly, even though our sample included a group of provider types and specialties, oversampling of specific subgroups, such as NPs and women’s health specialties, could have allowed for comparisons across provider groups. Notwithstanding these limitations, the study findings provide several implications for clinical practice as well as future research.
Study Implications
The study findings provide several implications for practice and research. Interventions targeting HCPs are critically needed to focus on improving their knowledge about the HPV vaccine, reduce their concerns about HPV vaccination, and increase the facilitators for recommending the HPV vaccine. The findings clearly demonstrate that pediatric HCP have taken on the overwhelming portion in the effort to improve HPV vaccination. As such, there is a critical need to educate non-pediatric providers who provide services to adolescents and young adults about the HPV vaccine. Such interventions should address knowledge needs among HCPs regarding the HPV vaccine indications, side effects, and national recommendations regarding age, gender, dosing intervals, and catchup doses. Furthermore, intervention strategies need to address HCPs’ concerns about the HPV vaccine such as the safety of the vaccine as well as perceptions that HPV vaccine is being pushed by drug companies to make money. Lastly, studies are needed to evaluate the impact of intervention strategies focused on facilitators on the recommendation practices among HCPs. This includes raising awareness about the CDC - ACIP as well as professional organizations recommendations regarding HPV vaccination. This also includes the need to examine the effect of clinical practice strategies such as the use of regular staff meetings about vaccination quality indicators, peer influence, and participating in coalitions and/or advocacy groups for immunization/vaccination. Health care provider (HCP) recommendation of the HPV vaccine increases the vaccine’s uptake8-12 and reduces parental refusal/delay of the vaccine.
13
Yet, the proportion of HCPs who report discussing the HPV vaccine with parents of adolescents in various studies ranges between 35% and 48%.14-16 The rates that providers reported in this study for recommending the HPV vaccine were 56% and 73% for younger and older adolescents. For both age groups, these rates were higher in practices that had more Hispanic patients and among providers who worked in pediatrics and had higher levels of knowledge and lower levels of concerns about the HPV vaccine. The rates for older adolescents were also higher in practices with more VFC and privately insured patients and among providers who reported more facilitators for recommending the vaccine. Interventions are needed to target pediatric and non-pediatric providers and practices with lower rates of Hispanic patients and VFC recipients. In addition, interventions targeting HCPs are needed to improve their knowledge and address their concerns about the HPV vaccine (e.g., vaccine safety and perceptions about motives of drug companies). Lastly, studies are needed to evaluate the impact of interventions using various types of facilitators on HCPs’ recommendation of HPV vaccination.So What?
What is already known on this topic?
What does this article add?
What are the implications for health promotion practice or research?
Footnotes
Author Contributions
Rula Btoush is the principal investigator for this study, responsible to designing the study, supervising recruitment and data collection activities, conducting the data analysis, and preparing the manuscript. Racquel Kohler’s role in this work included assisting with the data analysis, interpreting the study findings, and preparing the manuscript. Dennis Carmody’s role included assisting with designing the study, the data analysis decisions, and preparing the manuscript. Shawna Hudson’s role included assisting with designing the study, interpreting the study findings, and preparing the manuscript. Jennifer Tsui’s role included assisting with designing the study, interpreting the study findings, and preparing the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by the Rutgers Cancer Institute of New Jersey (P30CA072720) – Cancer Prevention and Control (CPC) Pilot Award Program, New Brunswick, NJ and by the National Center for Advancing Translational Sciences UL1TR003017 at the National Institutes of Health.
Ethical Approval and Approval Number
Rutgers University, Health Sciences IRB - Newark (Pro20160000177).