
Abstract
Purpose
Pandemic-related isolation may exacerbate loneliness among rural adults; we sought to characterize loneliness and associated factors among rural adults during the COVID-19 pandemic.
Design
Cross-sectional observational study.
Setting
Remotely delivered self-management education (SME) workshops, rural upstate New York, May-December 2020.
Subjects
Rural SME workshop enrollees, aged 18+, n = 229
Measures
De Jong Gierveld 6-Item Loneliness Scale, sociodemographics, workshop type (chronic disease, chronic pain, diabetes), delivery mode (videoconference, phone, self-study); data collected via workshop process measures and enrollment surveys.
Analysis
Multivariable linear regression.
Results
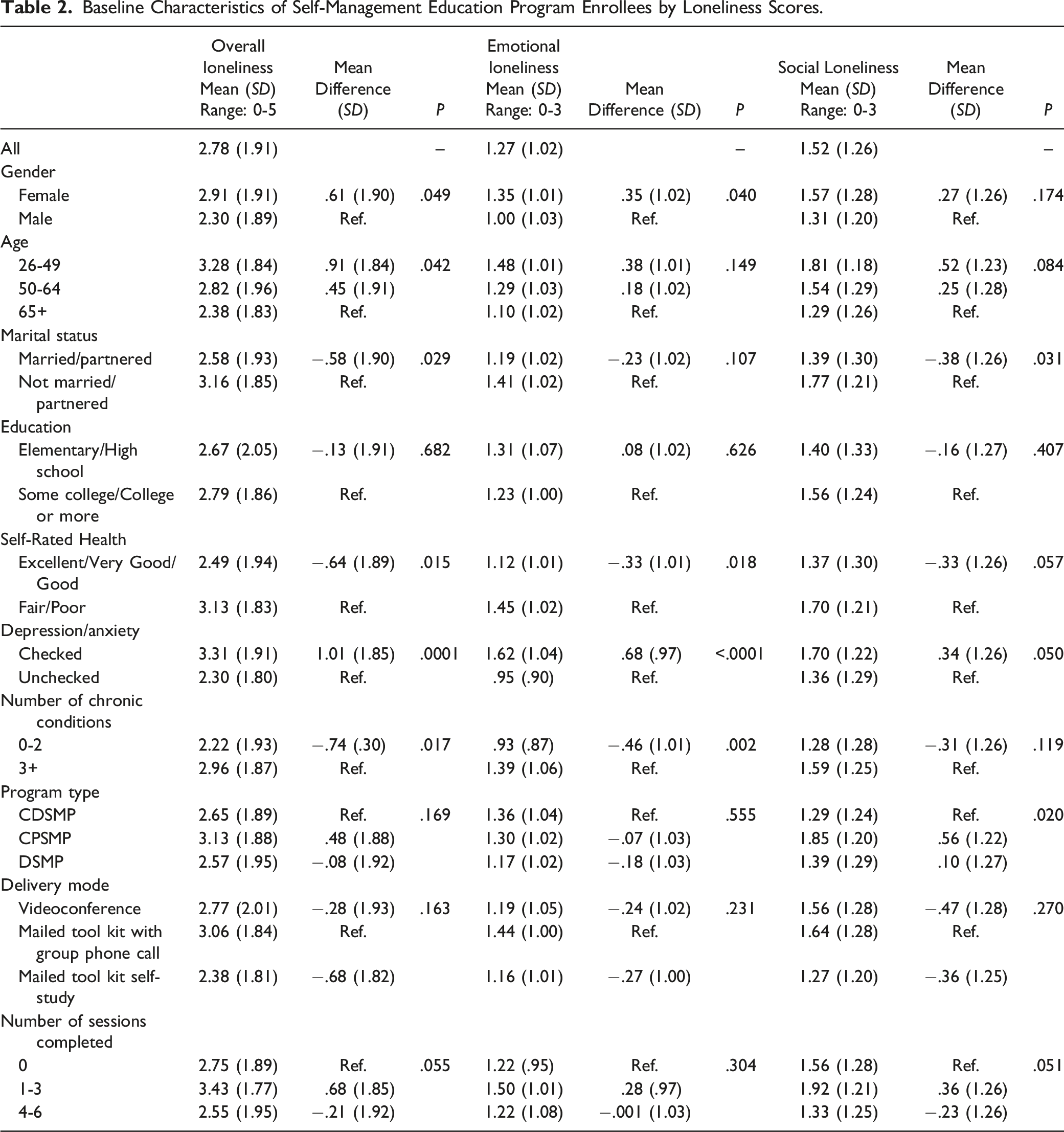
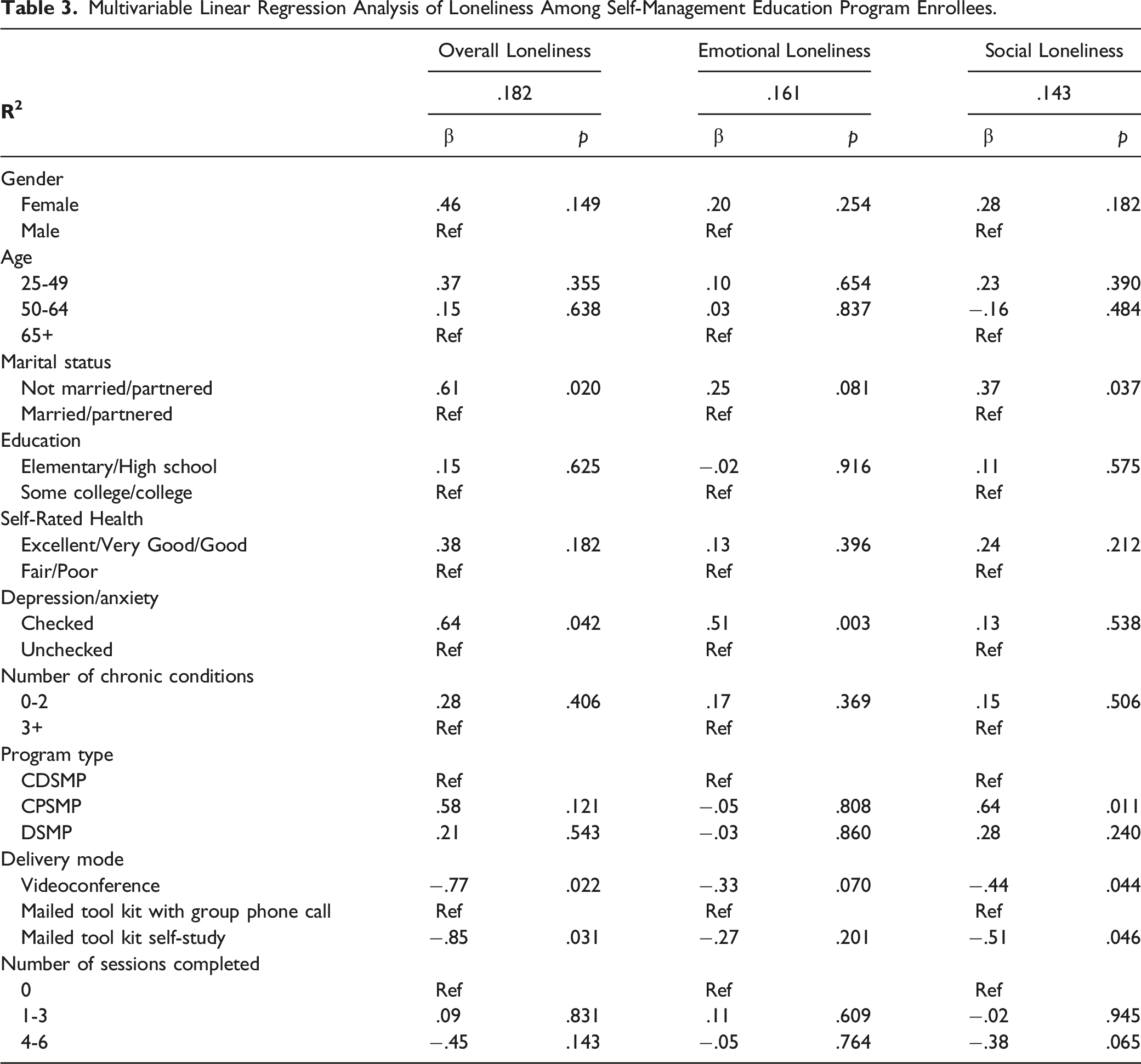
Mean overall, emotional and social loneliness scores were 2.78 (SD = 1.91), 1.27 (SD = 1.02), and 1.52 (SD = 1.26). Being not married/partnered (β = .61) and self-reported depression/anxiety (β = .64) were associated with higher overall scores, and selection of videoconference (β = −.77) and self-study (β =-.85) modes with lower scores. Self-reported depression/anxiety (β = .51) was associated with increased emotional loneliness. Being not married/not partnered (β = .37) and selection of chronic pain workshops (β = .64) was were associated with increased social loneliness. Selection of videoconference (β = −.44) and self-study (β = −.51) delivery modes were protective of social loneliness.
Conclusion
In addition to marital status and depression/anxiety, experiencing chronic pain and selecting phone-based workshops were associated with higher degrees of loneliness among rural adults during the pandemic. The latter may be partly explained by insufficient internet access. Health educators should be prepared to address loneliness in rural areas during the pandemic.
Keywords
Purpose
Rural adults experience higher rates of loneliness than their non-rural counterparts 1 They also experience high rates of chronic disease even after accounting for the older population in rural areas 2 Recent research has demonstrated that social isolation—whether perceived or actual—is as large of a risk factor for mortality as obesity or smoking. 3 The COVID-19 pandemic has brought the issue of social isolation to the forefront with both popular media and the scientific literature documenting the detrimental effects of social isolation on health and well-being.4-8
Loneliness has been defined as a distressed feeling when one’s social relationships are perceived to be inadequate 9 and has been conceptualized as a multidimensional phenomenon. The 2 most commonly cited dimensions are emotional loneliness and social loneliness. Emotional loneliness is the perceived absence of a close attachment figure (eg romantic partner). Social loneliness is the perceived absence of a social network, including friendships, and the lack of feeling as if one belongs. 10
The related concept of social isolation has been used to describe the objective lack of social contact or relationships. Social isolation is typically measured by factors such as living alone, size of the social network and frequency of social contacts. 3 While social isolation is related to loneliness, the concept is distinct. 11
During the COVID-19 pandemic, factors associated with loneliness include age, presence of 2 or more physical health conditions, presence of 2 or more mental health disorders, being male, living alone, lower education level, being a person of color, and presence of anxiety4,8,12 The relationship between these factors can vary depending on which aspect of loneliness is being measured. For instance, being older is protective against emotional loneliness, but a risk factor for social loneliness. 4
It is also known that rural older adults are particularly at risk not only for exposure to the SARS-CoV-2 virus, but also for increased social isolation and loneliness. While rural adults generally have stronger social networks than their urban counterparts, they face higher levels of loneliness. 13 Henning-Smith et al hypothesized that this could be due to lack of access to both transportation and reliable internet connectivity. Between March 2020 and June 2020 when people were forced to stay at home, rural Americans were more likely to lack the resources to connect virtually with their networks, thus exacerbating both social isolation and loneliness. 13 Despite the recent literature on loneliness during COVID, it remains unclear how emotional and social aspects of loneliness have been experienced by rural populations during the pandemic.
The Living Well Program offers self-management education programs for adults in its rural catchment area in central upstate NY. The programs include the Chronic Disease Self-Management Program (CDSMP), Chronic Pain Self-Management Program (CPSMP) and the Diabetes Self-Management Program (DSMP). All 3 programs were developed by the Self-Management Resource Center (SMRC) and were originally designed to be 6-week in-person workshops. As part of its evaluation of the implementation of SMPs in a rural setting, Living Well administers participant surveys at enrollment (baseline) and immediately after the workshop series. When the COVID-19 pandemic precluded in-person workshops, 3 alternative delivery modes were offered: (1) a mailed toolkit (self-study), (2) a mailed tool kit with weekly small group phone calls, and (3) a weekly 2-hour videoconference (Zoom). At that time, we added questions on loneliness to enrollee surveys to better understand the prevalence of loneliness during the pandemic among program enrollees and factors associated with different dimensions of loneliness.
The purpose of this analysis was to characterize loneliness and associated factors among rural adults enrolling in self-management education programs offered during the COVID-19 pandemic. The report is meant to be a first step in identifying who is most impacted by each dimension of loneliness in a rural, chronically ill population.
Methods
Design, Sample, Measures, Intervention, Analysis
Living Well serves 6 rural counties in central upstate New York. Individuals are recruited to enroll in the workshops through a variety of means including targeted social media advertisements, electronic communications sent through the patient portal of the electronic health record (EHR), and general print media disseminated throughout the community. Participants may sign up for the program and delivery mode of their choosing on the healthcare system’s website or by contacting the Living Well office. In addition, when a provider refers a patient to the program via the EHR, the Living Well team contacts the patient to enroll them in the program. To be eligible to participate in a workshop, an individual must be an adult (age 18 and older) and have a chronic disease (CDSMP), diabetes (DSMP) or chronic pain (CPSMP), or be a caregiver for someone who is eligible.
This analysis includes all adults who completed an enrollment survey for the purpose of enrolling in a Living Well workshop from May-December 2020. Surveys were administered electronically via a REDCap14,15 survey link or were mailed with a prepaid return envelope. Surveys were administered at enrollment and following the sixth class.
Measurements
The 6-item De Jong Gierveld Loneliness Scale assesses loneliness with higher scores indicating higher degrees of loneliness. It has been shown to be a reliable and valid measure of loneliness among adults (Cronbach’s α = .70-.76; correlation with 11-item De Jong Gierveld Loneliness Scale = .93-.95). 16 For each item (eg, “I miss having people around me”), respondents indicate “yes”, “no”, or “more or less”. Three items are reverse-coded. Response choices indicating neutrality or more loneliness are scored as 1; response choices indicating less loneliness are scored as 0. The overall scale includes 2 3-item subscales which assess emotional loneliness (ie, missing intimate relationships) and social loneliness (ie, missing one’s social network). Overall scores range from 0-6; subscale scores range from 0-3. Scores were calculated for the entire scale and the 2 subscales (emotional and social loneliness). Based on previously published conventions, overall loneliness scores were also dichotomized into categories of not lonely (scores of 0-1) and lonely (scores of 2-6). 17
The surveys also collected information on age, gender, education, marital status, self-reported depression/anxiety, self-rated health, and self-reported number of chronic conditions. Program information, including self-management program type (chronic disease, chronic pain, diabetes), program delivery mode (mailed toolkit self-study, mailed toolkit with group phone call, videoconference), and number of sessions attended (0 = no-show, 1-3 = non-completer, 4-6 = completer) were recorded for all participants.
Statistical Methods
We calculated mean loneliness scores and standard deviations for overall, emotional, and social loneliness and tested differences in means by enrollee characteristics using t-tests for dichotomous variables and analysis of variance (ANOVA) for categorical variables with 3 or more levels. We used multivariable linear regression to identify independent predictors of loneliness. All analyses were conducted in SAS version 9.4, with a P-value less than .05 considered statistically significant.
The plan for evaluation of the self-management education programs was reviewed by the Mary Imogene Bassett Hospital Institutional Review Board and was determined to have met the federal criteria for exemption as an evaluation of an existing practice.
Results
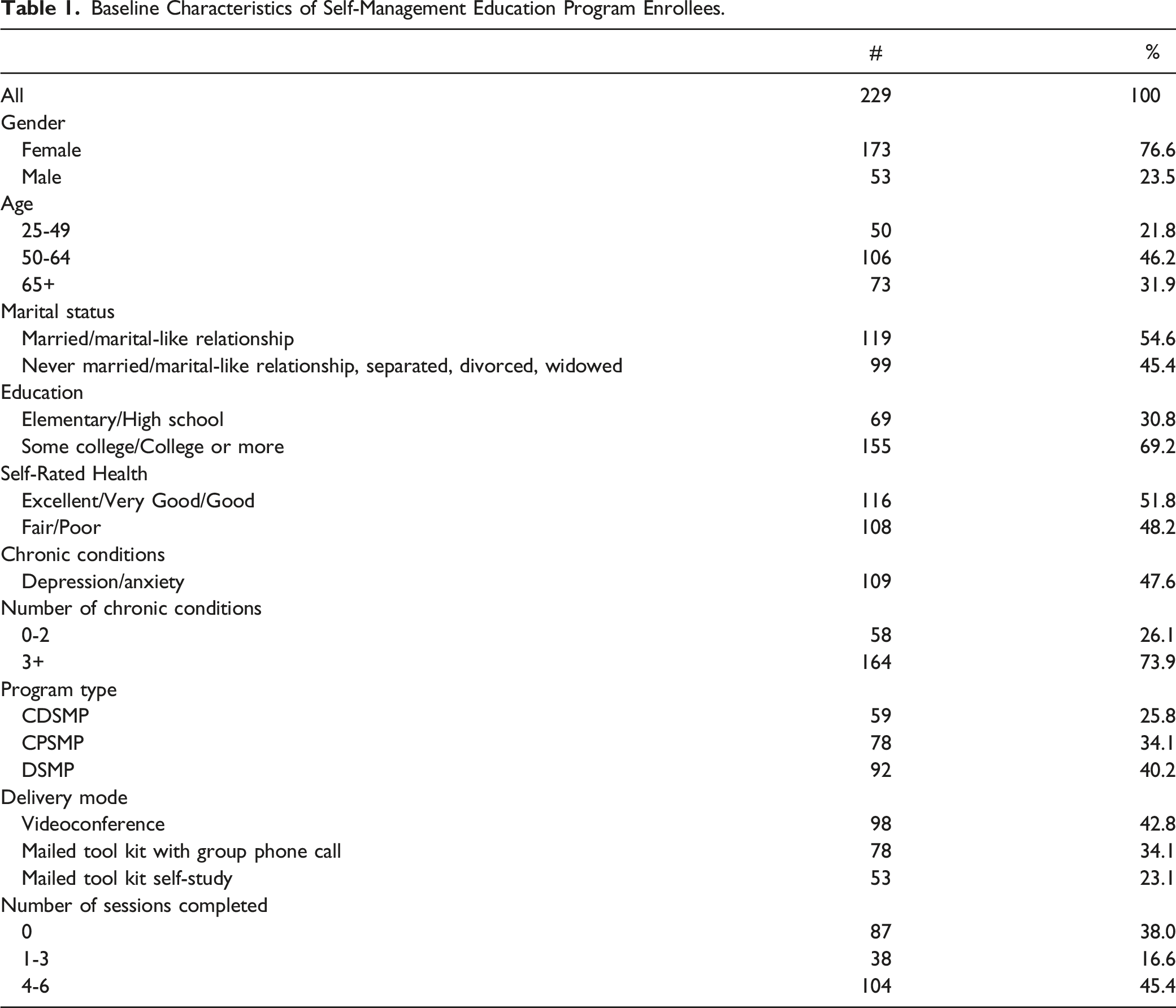
Baseline Characteristics of Self-Management Education Program Enrollees.
Baseline Characteristics of Self-Management Education Program Enrollees by Loneliness Scores.
Multivariable Linear Regression Analysis of Loneliness Among Self-Management Education Program Enrollees.
Discussion
The COVID-19 pandemic has created an environment of forced long-term physical isolation that most of us have not previously experienced. Like other community-based services around the nation and the world, our in-person self-management education programs were required to convert to remote delivery modes during the early stages of the pandemic. Given these circumstances, we felt it was important to examine the prevalence of loneliness in our rural, older, chronically ill population.
We found that 68% of our enrollees were categorized as lonely. While we do not have loneliness data from pre-2020 workshop enrollees for comparison, we can compare our results with other studies that used the same loneliness scale in similar populations during the COVID-19 pandemic. In their analysis of loneliness among adults age 65 and older in the Netherlands during the pandemic, Van Tilburg et al 18 report scores on the social loneliness and emotional loneliness scales that were similar to what we found for those 65 and older in our study population (1.17 vs 1.29 and .97 vs 1.10, respectively). In a study of adults in Hong Kong aged 60 and older with 2 or more chronic conditions that compared loneliness scores using the 6-item DeJong Gierveld Loneliness Scale, Wong et al 19 found increases in overall (paired mean difference=1.35, P < .001), social (.85, P < .001) and emotional loneliness (.50, P < .001) before vs during the pandemic. They report the mean overall loneliness during the pandemic was 2.9, with mean scores of 1.7 for social and 1.2 for emotional loneliness. 19
The strongest predictors of loneliness among our program enrollees were being not married/partnered, having a history of self-reported depression and/or anxiety, enrollment in the chronic pain workshop and enrollment in workshops delivered by phone. This could be due to the makeup of our study population (self-management program enrollees) and/or the unusual conditions of the pandemic. Interestingly, loneliness was not associated with program attrition (ie, the number of classes completed).
One of the most striking findings from our data was the effect of living with a partner on the different aspects of loneliness. Previous research suggests that being married/partnered is protective against loneliness, particularly emotional loneliness. 16 However, our findings indicate that being married/partnered was protective against social loneliness, but not emotional loneliness. This finding suggests that being engaged with a variety of people (not just one’s partner) is important during a period of physical distancing.
A similar pattern can be found for depression/anxiety. Those with self-reported depression and/or anxiety had higher levels of emotional loneliness; however, scores on the social loneliness subscale were similar between groups, indicating that regardless of the presence of depression, people missed their social networks.
Those enrolled in the chronic pain self-management program reported higher levels of social loneliness than those enrolled in the other programs. There is a complex relationship between chronic pain, self-isolation and social exclusion that has been documented in the literature. 20 The 3 questions comprising the social loneliness subscale (“There are plenty of people I can rely on when I have problems”, “There are many people I can trust completely”, “There are enough people I feel close to”) may very well represent a chronic pain trajectory where a person has either chosen to minimize social interaction or has been excluded from social interactions.
Our finding that those who chose the group phone call delivery mode were lonelier than those selecting videoconference or self-study raises questions about digital access and literacy in rural areas. Enrolling in the group phone call delivery mode was associated with social loneliness. A person who wanted to connect with a group and have extra support, may have been forced to choose this mode rather than Zoom if they did not have internet access. Even though two-thirds of rural dwellers have access to broadband internet, it is often too slow to allow for 2 ½ hour synchronous videoconferences, as required by the Zoom workshops. 13 Additional digital literacy concerns, such as knowing how and being able to utilize the internet, cost of internet access, as well as having access to a computer, tablet or smartphone are additional barriers. 21
There are several research and practice implications regarding the findings from the analysis. First, we need to establish how completion of the self-management workshops may impact social and emotional loneliness among rural populations. There is limited research exploring how self-management programs, particularly those delivered remotely, may alleviate loneliness. Additionally, as we continue to experience waves of the pandemic and the concomitant social distancing restrictions, it will be necessary to determine how rural populations continue to experience loneliness during these waves.
It is important to acknowledge limitations to this analysis. We added loneliness questions to our enrollment surveys beginning in May 2020 and thus do not have comparable pre-pandemic data from this population for comparison. There are clearly other factors impacting loneliness in our population that were not measured in this study. In the multivariable models, we found that more than 80% of the variance in loneliness scores was explained by unmeasured factors. While we were able to detect statistically significant differences in degrees of loneliness by enrollee characteristics, it is not clear what a unit change in overall loneliness scale or subscales represents. Given that moving from a score of 1 to 2 represents a change from not lonely to lonely, a .5 to 1-unit change on the overall scale may be clinically significant.
The workshop that a participant enrolled in may not necessarily represent their preferred mode of delivery. In some cases, a phone workshop may have been cancelled due to low enrollment and the participant was offered the opportunity to wait for the next offering or select their second choice (ie, videoconference or the mailed tool kit self-study). In other cases, a participant may have preferred videoconference, but did not have sufficient internet access to support that mode.
Conclusion
Reporting a history of depression and/or anxiety, being not married/partnered, enrolling in a chronic pain self-management program, and selecting phone-based program delivery were independently associated with different aspects of loneliness among rural adults during the COVID-19 pandemic. The latter may be explained in part by insufficient internet access in rural communities, which in turn may be associated with loneliness. Therefore, it is essential that health care providers routinely screen for loneliness and that non-internet-based interventions that are effective in rural areas be developed to help combat loneliness. Rural adults are at increased risk for social isolation and loneliness during the COVID-19 pandemic. We assessed aspects of loneliness among rural adults enrolled in self-management programs held remotely during the pandemic. In addition to previously identified risk factors, social loneliness was associated with enrollment in chronic pain programs and selection of a phone-based group program (versus videoconference platform or self-study options). Non-internet-based remote delivery modes should be considered for public health programming for rural adults particularly in areas with limited internet access and during periods of physical isolation.SO WHAT?
What is already known about this topic?
What is added by this report?
What are the implications for public health practice?
Footnotes
Author Contributions
All authors contributed to the conception and design of the study, data analysis, and interpretation of the study findings. WB and KP drafted the manuscript. All authors revised it critically for important intellectual content. All authors approve the final version to be published.
Ethics Statement
This project was declared exempt from continuing review by the Mary Imogene Bassett Institutional Review Board.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by a grant from the Health Resources and Services Administration Rural Health Care Services Outreach Grant Program (6 D04RH31785‐03‐03).