
Abstract
Purpose
To evaluate cardiovascular disease (CVD) risk factors among smokeless tobacco (ST) users. Exclusive ST users were compared to exclusive cigarette smokers and non-tobacco users.
Design
Cross-sectional study
Sample
Data were used from 16,336 adult males who participated in one of the National Health and Nutrition Examination Surveys (NHANES) from 2003 to 2018.
Measures
Biochemically verified tobacco use, CVD risk factors (hypertension, cholesterol levels, BMI categories), physical activity, cotinine concentration, and sociodemographic variables.
Analysis
Weighted analysis of the aggregate data was performed. ST users were compared with cigarette smokers and nontobacco users for their association with CVD risk factors. Associations were examined using univariate and multiple logistic regression with odds ratios (OR) and 95% confidence intervals (CI) reported.
Results
Prevalence of exclusive ST use was 4.4% whereas, exclusive smoking was 22.2%. Among ST users, 36.2% were hypertensive, 24.5% had high cholesterol levels, and most of them were overweight (31.1%) or obese (52.6%). ST users were more likely to have hypertension compared to smokers (aOR = 1.48, 95%CI: 1.12, 1.95) and nontobacco users (aOR = 1.41, 95%CI: 1.09, 1.83) adjusted for other covariates. ST users were twice more likely to be obese than nontobacco users (aOR = 2.18, 95%CI: 1.52, 3.11). ST users had significantly higher cotinine concentration than smokers.
Conclusion
Study findings indicate substantial association of ST use among males with hypertension and obesity which are independent risk factors of CVD.
Keywords
Tobacco use is the leading preventable cause of mortality, morbidity, and disability. Each year 20% (480,000) of all deaths in the United States are caused by tobacco use. 1 Different types of tobacco products exist worldwide. Although the most common forms of smokeless tobacco (ST) products in the United States include moist snuff and chewing tobacco, the manufacturing and use of spitless ST products such as pouched moist snuff, snus, and lozenges is also increasing. 2 With the emergence of newer tobacco products, patterns of tobacco use are changing. In recent years the prevalence of cigarette smoking has declined in the United States, however the proportion of current smokeless tobacco users has not significantly changed as 2.4% of the adults are current ST users. 3 The prevalence of ST use is particularly high among males. 4.7% of the adult males in the US reported ST use in 2019. 3
Cardiovascular disease (CVD) is the leading cause of death in the United States that constitutes 30.4% of all-cause mortality.4,5 It is estimated that 49.2% (126.9 million) of adults suffer from CVD. 5 A number of risk factors for CVD have been identified. These include nonmodifiable risk factors, behavioral factors such as, cigarette smoking, obesity, poor diet, and lack of physical activity, and pathophysiological factors. High blood pressure, dyslipidemia, and insulin resistance are the pathophysiological processes that are considered major risk factors for CVD. 6
Cigarette smoking is a well-established independent risk factor of CVD; 25% of CVD-related deaths are attributable to cigarette smoking. 7 With regards to the high morbidity and mortality associated with tobacco use, ST use is considered less harmful than cigarette smoking but there is a lack of conclusive evidence related to risk of CVD. Tobacco products contain varying levels of nicotine and other hazardous chemicals hence, there are variations in disease-causing potential of these products. ST products have considerably high concentration of certain carcinogens, nicotine, and substances such as sodium bicarbonate and licorice.8,9 Therefore, increased exposure to these chemicals suggests that ST use may increase the risk of CVD. To date, the scientific evidence of the association between ST use and CVD is limited. Most of the past research has focused on examining the effect of ST use on CVD related mortality. Findings of these studies conducted in different countries showed significantly increased risk of ischemic heart disease and stroke related mortality among ST users. 10 Similarly, previously conducted studies in the United States have identified the potential impact of ST use on CVD related mortality. A prospective study consisting of two large cohorts (Cancer Preventive Studies – CPS I and CPS II) found that current ST users had 12% increased risk of mortality in CPS I and 25% increased risk of mortality in CPS II from coronary heart disease as compared to non-tobacco users. 11 The same study reported significantly greater risk of stroke related mortality among current ST users. Likewise, a study based on National Longitudinal Mortality Study data revealed that current ST users had significantly increased risk of dying from coronary heart disease compared to nontobacco users. 12
Conversely, the evidence from a limited number of studies regarding the effect of ST use on CVD risk is inconclusive. 9 Most of these studies were conducted in Sweden examining the CVD effect of snus.13-18 A few studies of ST users in the United States suggested no association between ST use and CVD.19,20 Unlike the United States where snuff and chewing tobacco are the most commonly used ST products, in Sweden snus is the primarily used ST product. Due to the worldwide variation in manufacturing, processing, and formulation of ST products, the potential CVD effect of ST products used in different regions may also not be the same.9,10,21 Therefore, the results from the studies conducted among Swedish ST users who predominantly use snus are not generalizable to the ST users in the United States. Given the high prevalence of ST use among males and its harm causing potential, it is important to examine the effects of ST use on important CVD risk parameters among male ST users in the United States. Findings of such research have far reaching implications for public health efforts to prevent the use of ST products.
This study sought to evaluate the association of exclusive ST use with CVD risk parameters among adult males in the United States. Specifically, exclusive ST use was compared to nontobacco use and exclusive cigarette smoking for its association with hypertension, high cholesterol, and obesity. The secondary aim of the study was to evaluate cotinine concentration among exclusive ST users and exclusive cigarette smokers.
Methods
Design
This cross-sectional study was based on secondary analysis of nationally representative survey data. The study was restricted to males because of the low prevalence of ST use among females (0.3%) in the United States. 3
Sample
Data were obtained from the National Health and Nutrition Examination Survey (NHANES) for eight 2-year cycles from 2003 to 2018. NHANES is one of the most in-depth national surveys that collects a variety of health-related data through personal interviews, standardized physical exams, and laboratory tests. 22 This study used information obtained from 16,336 adult male NHANES respondents for whom information on biochemically verified current tobacco use was present. Current users of any other tobacco or nicotine product (e-cigarette, hookah, pipe, cigar, and nicotine replacement therapy) were excluded. Those with missing information about any tobacco product used during the last five days before participating in the survey were also excluded. Similarly, those with missing cotinine data were not included in the study.
Measures
Tobacco Use: Self-reported tobacco use was verified with serum cotinine concentration. The serum cotinine threshold of 3 ng/ml was used to distinguish tobacco users from nontobacco users.23,24 Participants were categorized into three mutually exclusive groups based on their tobacco use. These groups included exclusive ST users, exclusive cigarette smokers, and non-tobacco users. Exclusive ST users were defined as those using ST (chewing tobacco and/or snuff) in the last five days, not currently smoking cigarettes (responded “not at all” to the question “Do you now smoke cigarettes), did not use any other tobacco product including cigarettes in the last five days, and had serum cotinine concentration ≥3 ng/ml. Exclusive cigarette smokers were defined as those who had smoked at least 100 cigarettes in their lifetime, were currently smoking cigarettes some days or every day, and smoked cigarettes in the last five days, were not currently using any other tobacco product, and had serum cotinine concentration ≥3 ng/ml. Non-tobacco users were those who reported not currently smoking cigarettes (some day or every day), were not former smokers (had not smoked 100 cigarettes in their lifetime), did not use any tobacco product in the last five days, and had serum cotinine concentration <3 ng/ml.
To examine the effect of former cigarette smoking on the association of current exclusive ST use with CVD risk factors, exclusive ST users were further categorized into two groups according to their former smoking status. Former smoking was defined as those who had smoked 100 cigarettes in their lifetime but were not current smokers.
Cardiovascular Disease Risk Factors: Three key CVD risk factors, hypertension, high cholesterol, and obesity, were evaluated as outcome variables. According to the guidelines of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure, hypertension was defined as having systolic blood pressure ≥140 mmHg or diastolic blood pressure ≥90 mmHg or reported taking medication to treat high blood pressure. 25 Blood pressure was measured by following a standardized protocol. 26 Average of all (three or four) blood pressure measurements taken during the same exam sessions were used to determine the systolic and diastolic blood pressure. 26 High total cholesterol level was defined as serum cholesterol concentration of ≥240 mg/dl or those who reported taking medication to lower cholesterol. 27 BMI was categorized into three levels: low or normal weight (<25 kg/m2), overweight (≥25 kg/m2 to <30 kg/m2), and obese (≥30 kg/m2).
Other variables: Age, race/ethnicity, education level, and physical activity were included as covariates. Age was used as a continuous variable; whereas, race/ethnicity was categorized as non-Hispanic (NH) white, NH black, NH Other, and Hispanic. Education level was classified into four groups: Less than high school, High school (including those with GED or equivalent education), Some college (those who had some college level education or associate degree), and College graduates or above. Physical activity was determined by the Global Physical Activity Questionnaire (GPAQ) that was included in NHANES cycles 2007-2008 through 2017-2018. Total number of minutes of moderate or vigorous physical activity per week was calculated to obtain the metabolic equivalent of task (MET). According to the WHO recommendations on physical activity for health and the Physical Activity Guidelines for Americans, a combination of moderate- and vigorous-intensity physical activity achieving at least 600 MET minutes per week was used to dichotomize study participants into physically active or not active groups.28,29
Analysis
Descriptive statistics were calculated for all study variables. Due to complex national survey data, weighted analyses were conducted by employing the recommended statistical weights, including design final weight, stratification, and cluster information provided by NHANES. 30 Sample based frequencies and weighted proportions were calculated for categorical variables; whereas, for age weighted mean and standard error (SE) were computed. Univariate associations of categorical variables were assessed by the Rao-Scott chi-square test and for the age variable t-test (proc surveymeans) and ANOVA (proc surveyreg) were used. Weighted logistic regression (proc surveylogistic) analysis was carried out to examine associations between individual outcome variable (CVD risk factors) with ST use. Separate weighted logistic regression models were used to compare ST users with cigarette smokers and nontobacco users for their association with CVD risk factors. Multiple logistic regression analysis was performed to assess confounding and effect modification of covariates. As the physical activity variable was available from NHANES 2007 to 2018, two multivariate models were used to obtain the adjusted odds ratios (aOR) and 95% confidence interval (95%CI). Model 1 included age, race/ethnicity, education level, and BMI, whereas in Model 2, physical activity was included in addition to the covariates identified in Model 1. The Taylor series (linearization method), which is the most commonly used method to estimate the covariance matrix of the regression coefficients for complex survey data, was used. It is the default variance estimation method used by proc surveylogistic. 30
Cotinine concentration was not normally distributed; therefore, instead of weighted analysis, nonparametric techniques were used to analyze cotinine data. For descriptive statistics, median (minimum, maximum) values were calculated; whereas, association of cotinine with hypertension was examined with Mann-Whitney U test. All analyses were performed using SAS version 9.4 and statistical significance was based on an alpha level of 0.05.
Results
Distribution of study variables according to cardiovascular disease risk factors among adult males (NHANES 2003 – 2018). a
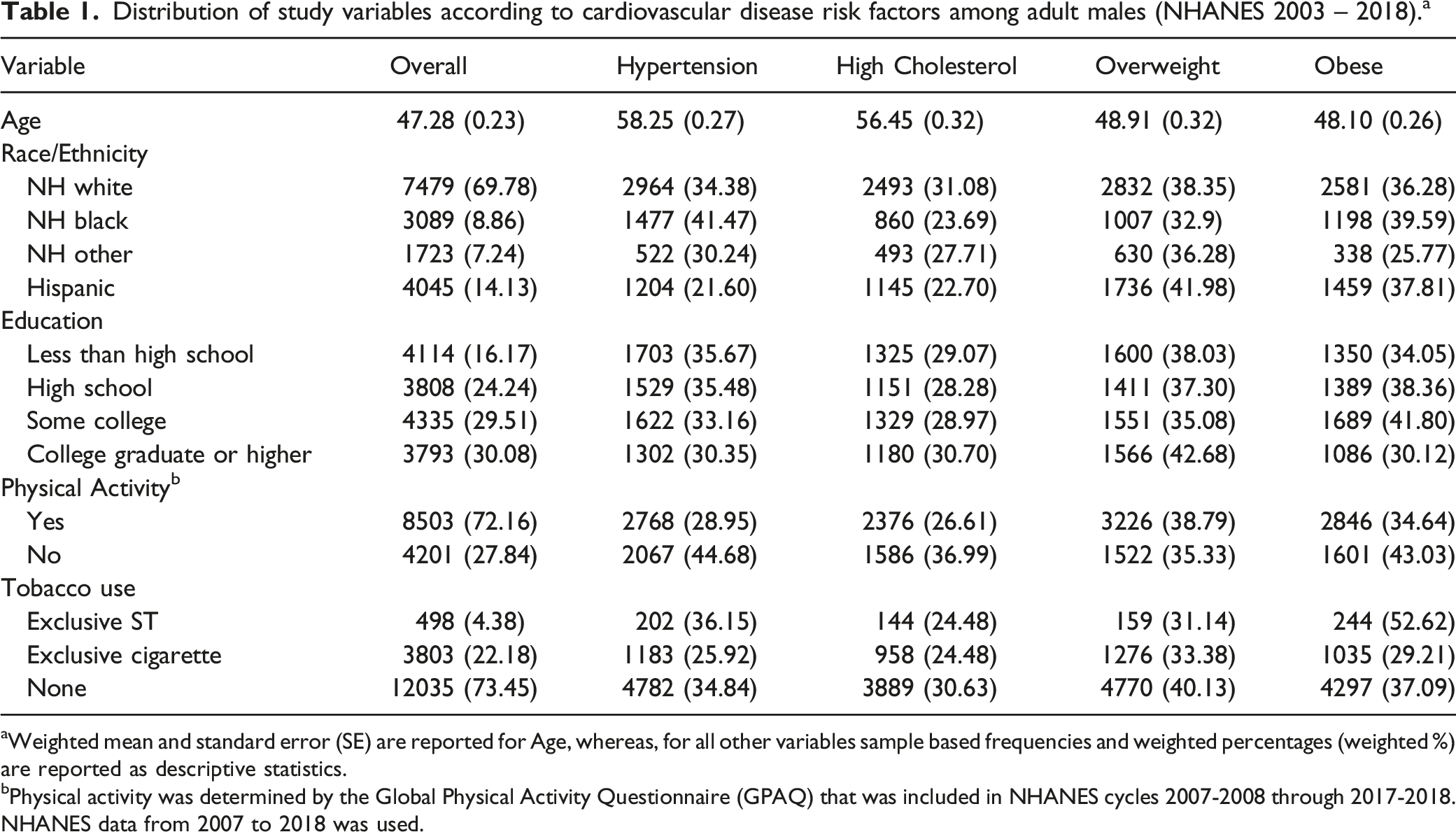
aWeighted mean and standard error (SE) are reported for Age, whereas, for all other variables sample based frequencies and weighted percentages (weighted %) are reported as descriptive statistics.
bPhysical activity was determined by the Global Physical Activity Questionnaire (GPAQ) that was included in NHANES cycles 2007-2008 through 2017-2018. NHANES data from 2007 to 2018 was used.
There were significant differences in tobacco product use across different racial/ethnic groups (Figure 1). NH whites had the highest prevalence of exclusive ST use (5.8%), whereas exclusive cigarette smoking was more prevalent (33.2%) among NH blacks compared to any other racial/ethnic group. Level of education was also significantly associated with the type of tobacco product used. ST use prevalence was the lowest among college graduates (2.0%) and highest among those who had a high school education (6.6%). There was a decrease in prevalence of exclusive cigarette smoking with an increase in educational attainment. (Figure 1). Although there was no significant difference in the mean age of exclusive ST users (43.6 ± 0.8 years) and exclusive cigarette smokers (42.9 ± 0.3 years), they were significantly younger than nontobacco users (48.8 ± 0.3 years, P < .0001). Tobacco use status according to race/ethnicity, physical activity, and education level of males (NHANES 2003-2018)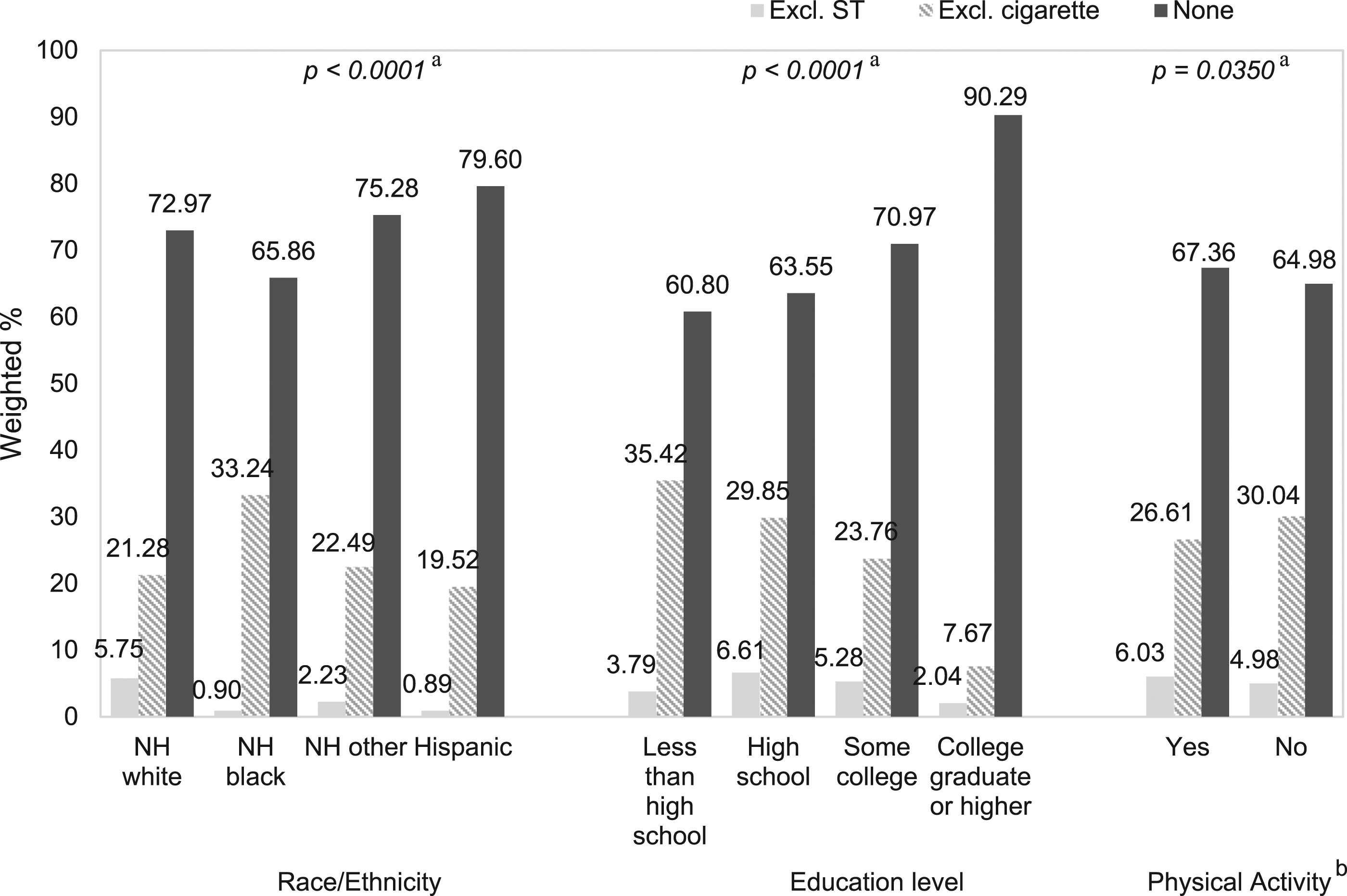
The prevalence of CVD risk factors varied by tobacco use categories. Hypertension was more prevalent among exclusive ST users (36.2%) than exclusive cigarette smokers (25.9%) and nontobacco users (34.8%). Almost a quarter of the exclusive ST users and exclusive cigarette smokers (24.5%) had high cholesterol levels. NH blacks had the highest prevalence of hypertension (41.5%), whereas, high cholesterol level was more prevalent among NH whites (31.1%). Mean age of those who had hypertension (58.3 ± 0.3 years) was significantly higher than those with normal blood pressure (42.0 ± 0.2 years, P < .001). Similarly, adult males with high cholesterol level were significantly older than those with normal cholesterol level (56.4 ± 0.3 vs. 43.5 ± 0.2 years, P < .0001). (Table 1)
Association of exclusive ST use with cardiovascular disease risk factors.
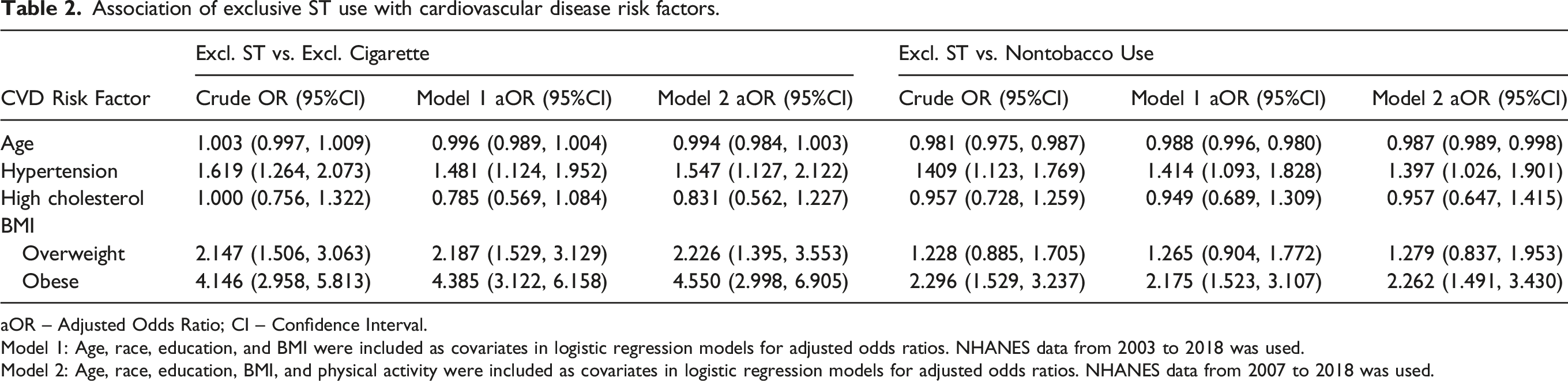
aOR – Adjusted Odds Ratio; CI – Confidence Interval.
Model 1: Age, race, education, and BMI were included as covariates in logistic regression models for adjusted odds ratios. NHANES data from 2003 to 2018 was used.
Model 2: Age, race, education, BMI, and physical activity were included as covariates in logistic regression models for adjusted odds ratios. NHANES data from 2007 to 2018 was used.
Exclusive ST users who were never smokers compared with exclusive ST users who were former smokers for cardiovascular disease risk factors.
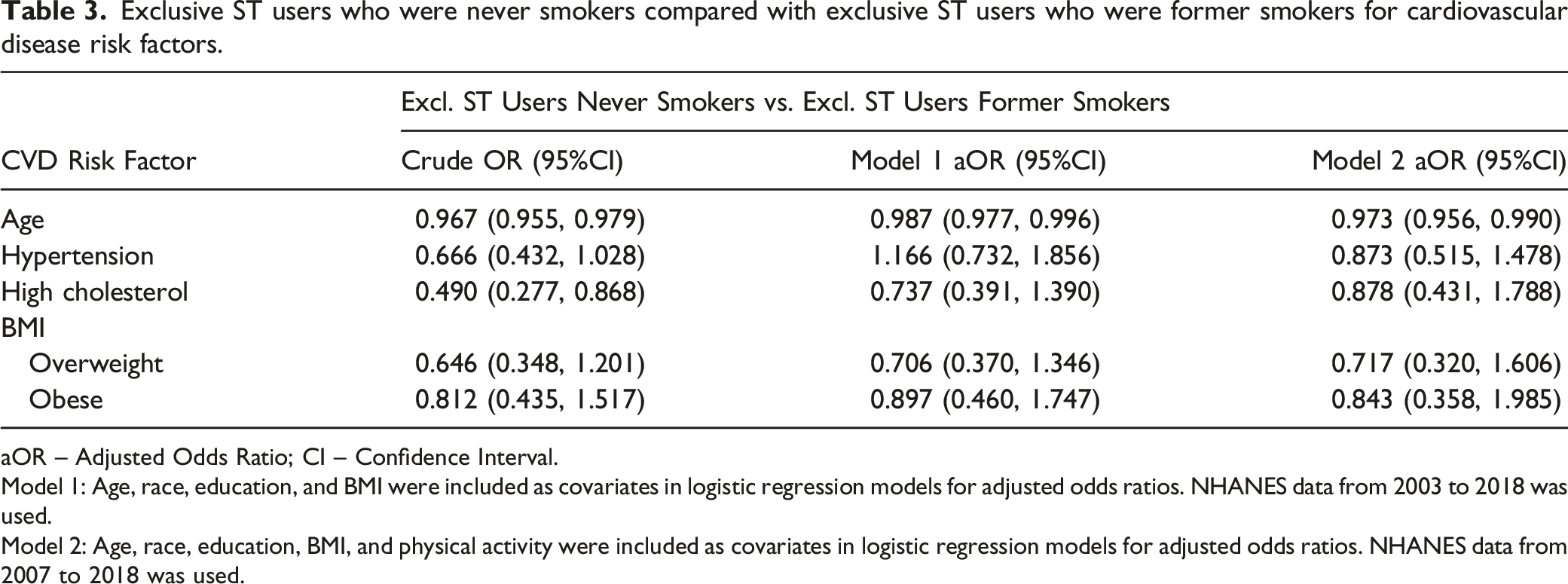
aOR – Adjusted Odds Ratio; CI – Confidence Interval.
Model 1: Age, race, education, and BMI were included as covariates in logistic regression models for adjusted odds ratios. NHANES data from 2003 to 2018 was used.
Model 2: Age, race, education, BMI, and physical activity were included as covariates in logistic regression models for adjusted odds ratios. NHANES data from 2007 to 2018 was used.
Analysis of the cotinine data exhibited higher cotinine concentration (ng/ml) among exclusive ST users (median = 346.5, min = 3.5, max = 1820.0) compared to exclusive cigarette smokers (median = 222.0, min = 3.3, max = 905.0, P < .0001). Figure 2 summarizes the comparison of serum cotinine concentration between exclusive ST users and exclusive cigarette smokers according to their blood pressure levels. Adult males in both tobacco use groups with hypertension had significantly increased serum cotinine concentration compared to those with normal blood pressure. Cotinine concentration among exclusive ST users and exclusive cigarette smokers by blood pressure. a p-values are based on Mann-Whitney U test.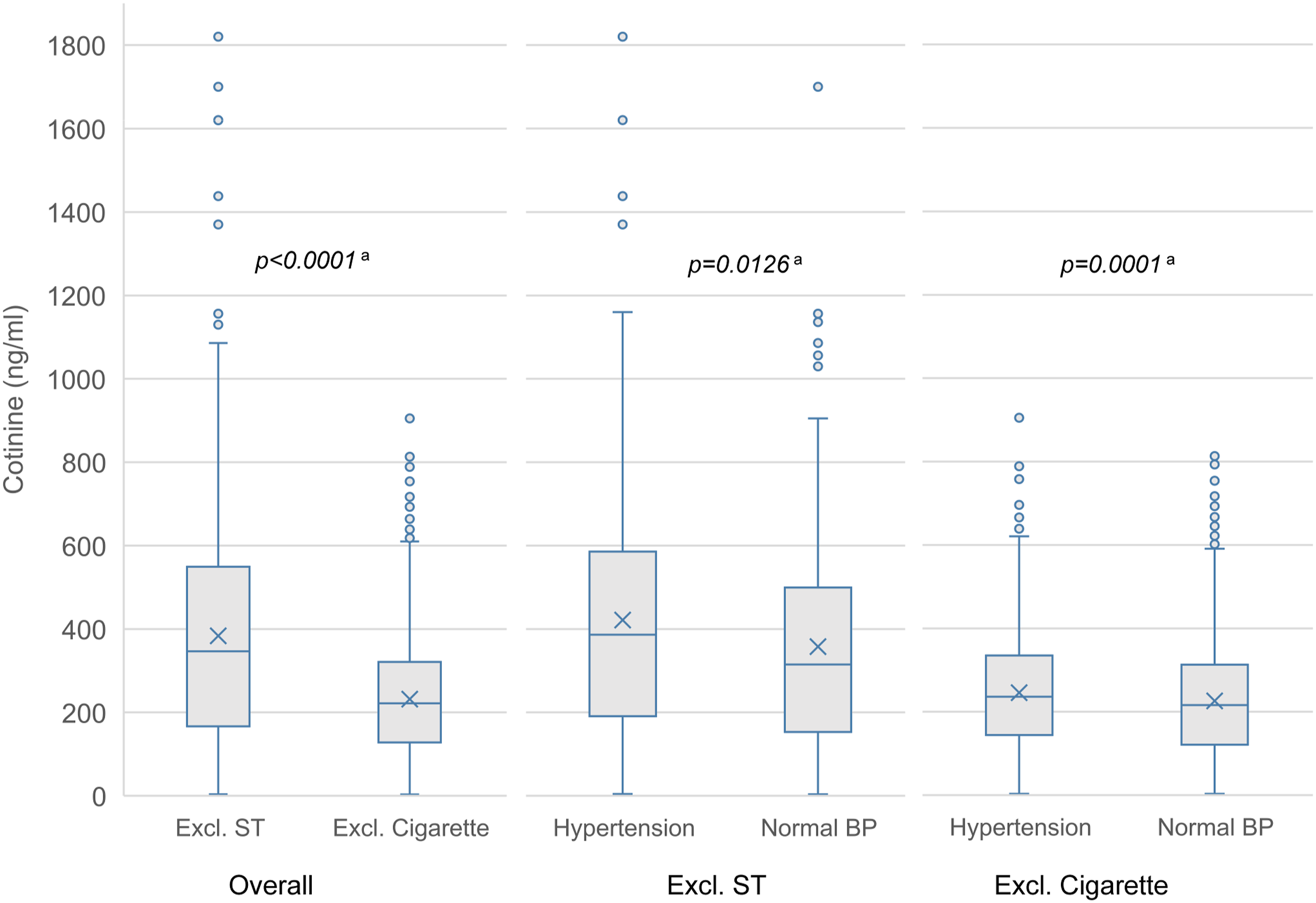
Discussion
Cigarette smoking is well established as a major risk factor for CVD but little is known about the adverse cardiovascular effects of smokeless tobacco products commonly used in the United States. In order to determine the association between ST and CVD, this study examined ST use among males relative to three strong predictors of CVD; hypertension, high cholesterol, and obesity. Exclusive ST users were studied to provide empirical information about the association of ST use alone with CVD risk factors. Furthermore, they were compared with exclusive cigarette smokers to provide preliminary evidence for future studies to explore potential use of ST as a safer alternative for cigarette smokers, which has not been well studied among tobacco users in the US. Results of this study demonstrated that ST use is significantly associated with hypertension and obesity among males, two strong risk factors for CVD.
Various mechanisms have been identified by which cigarette smoking causes CVD. Some of these involve products of tobacco combustion that cause inflammation, endothelial damage, increased thrombogenesis, atherosclerosis, and hypoxemia secondary to carbon monoxide. 31 In addition to these, nicotine from cigarettes has multiple cardiovascular effects which are either mediated by the sympathetic nervous system or directly induced by nicotine.31,32 Compared to cigarettes, ST has relatively low concentration of most of the combustion-derived products, however certain carcinogens, nicotine, and additives such as sodium bicarbonate and licorice are present in considerably higher concentration in ST products.8,9 Although the mechanism of action of ST in causing CVD is not fully known, high levels of nicotine and other chemicals delivered by ST products indicates its crucial role in causing CVD. There are differences in nicotine pharmacokinetics by tobacco products. After administration of ST, there is initial quick absorption of nicotine which is followed by slow but sustained absorption.31,33,34 This results in high plasma nicotine concentration for longer duration among ST users compared to cigarette smokers. Similar to the findings of past research, this study showed higher serum cotinine concentration among ST users than cigarettes smokers.
Most of the past studies have examined the effect of ST on CVD related mortality. There are a limited number of studies that have examined the relationship between ST and CVD risk factors. There is inconclusive evidence about the association of ST use and hypertension. A study of young baseball players in the United States and another study of adult male snuff users in Sweden showed no difference in blood pressure between exclusive ST users and non-users.19,35 However, a study of young adult ST users in the United States reported significantly higher blood pressure among ST users. 36 Similarly, studies of construction workers and adult males in Sweden suggested increased risk of high blood pressure among snuff users.37,38 Results of the current study confirm these findings of significant association of ST use with high blood pressure. It is noteworthy that ST users were more likely to have hypertension not only when they were compared to nontobacco users but also in comparison to exclusive cigarette smokers. These results suggest that the association of ST use with hypertension can be attributable to high nicotine levels in ST products. The study found high serum cotinine concentration, the primary metabolite of nicotine, among those who had hypertension. In addition to the increased amount of nicotine, ST products in the United States contain sodium bicarbonate and licorice which have important role in pathogenesis of hypertension. 9 Independent effect of these chemicals on hypertension and other CVD risk factors should be further investigated.
Obesity and high cholesterol are also important risk factors for CVD. Our findings of a strong association between ST use and obesity are in accord with the results of previous studies.15,37,39,40 Exclusive ST users were twice as likely to be obese compared to nontobacco users. Moreover, this likelihood increased to four fold when exclusive cigarette smokers were used as a comparison group. There are equivocal findings of past studies examining the relationship of ST use with cholesterol levels. A study of adult males in the United States showed that ST users were more than twice as likely to have hypercholesterolemia compared to nontobacco users. 41 In contrast, the study of baseball players and studies conducted in Sweden did not find significant association of ST use with total cholesterol. Although the results of the current study exhibit no association between ST use and cholesterol level but it is worth noting that exclusive ST users were not significantly different from exclusive cigarette smokers for high cholesterol levels.
Limitations
The study has some limitations that must be taken into consideration. First, tobacco use was determined based on self-reported questionnaire data. Except for cigarette smoking, information about other tobacco product use including ST use was reported for the past five days use of tobacco products. Therefore, some of the exclusive cigarette smokers and exclusive ST user might have been regularly using other tobacco products prior to five days of the survey resulting in possible information bias. Second, due to the cross-sectional data, temporal link between ST use and CVD risk factors could not be established. Third, detailed information about ST use such as quantity, frequency, and duration of use was not available, therefore, the effect of these important covariates on the observed associations were not evaluated. Furthermore, due to the lack of information about the duration of ST use and cross-sectional study design, it could not be determined if the observed high blood pressure was an acute effect of ST or it was chronic hypertension. Assessment of physical activity based on GPAQ was done from 2007-2009 through 2017-2018 NHANES cycles, therefore physical activity data from the prior cycles were not included. Hence, the results of the statistical analysis that included physical activity as a covariate would have less power. Lastly, cotinine data were skewed, therefore recommended weighted statistical analysis to account for the complex survey design was not performed. Although population level estimates for cotinine data were not calculated, we used nonparametric techniques to analyze sample data.
Despite these limitations, the study has notable strengths. Data from nationally-representative sample from 2003 to 2018 were used that provided national estimates and adequate power for the statistical analysis. Variables for CVD risk factors were based on physical examination and laboratory tests; therefore, the study results are less prone to misclassification bias. Similarly, stringent criteria were used to classify tobacco and nontobacco users based on cotinine concentration. Due to the biochemically verified tobacco use classification study results were less likely to be biased.
In tobacco research there is a greater emphasis on evaluating the health impact of cigarette smoking. This study addressed an important gap in research by evaluating the association of exclusive ST use with CVD risk factors. The study results indicate that male exclusive ST users are more likely to be hypertensive and overweight or obese. Furthermore, the findings based on the comparison of exclusive ST users and exclusive cigarette smokers underscores the harm associated with ST use. Future longitudinal studies focused on ST use and other tobacco use behaviors are warranted to further examine the CVD risk associated with ST use. Cigarette smoking is well-established as a major risk factor for cardiovascular disease (CVD) but little is known about the adverse cardiovascular effects of smokeless tobacco products commonly used in the United States. This study addressed an important gap in tobacco research by evaluating the association of ST use with CVD risk factors among males. Study results underscore significant harm associated with ST use. Findings of this study provide important evidence for public health efforts to prevent the marketing and use of ST products. This study also provides preliminary data for future research to evaluate the CVD risk associated with the use of ST products.SO WHAT?
What is already known on this topic?
What does this article add?
What are the implications for health promotion practice or research?
Footnotes
Author’s contribution
NM and LAB developed the research idea and designed the study. NM performed data curation, statistical analysis, and drafted the manuscript. LAB contributed to the interpretation and presentation of the results and performed critical revision of the manuscript. ZS and KK conducted the literature review and assisted with data curation, statistical analysis, and preparing the manuscript. RA contributed to the research design, interpretation of the results, and performed critical review of the manuscript. All authors contributed to and have approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Appendix
aOR – Adjusted Odds Ratio; CI – Confidence Interval. Model 1: Age, race, education and BMI were included as covariates in logistic regression models for adjusted odds ratios. NHANES data from survey years 2003 to 2018 were included. Model 2: Age, race, education, BMI, and physical activity were included as covariates in logistic regression models for adjusted odds ratios. NHANES data from survey years 2007 to 2018 were included.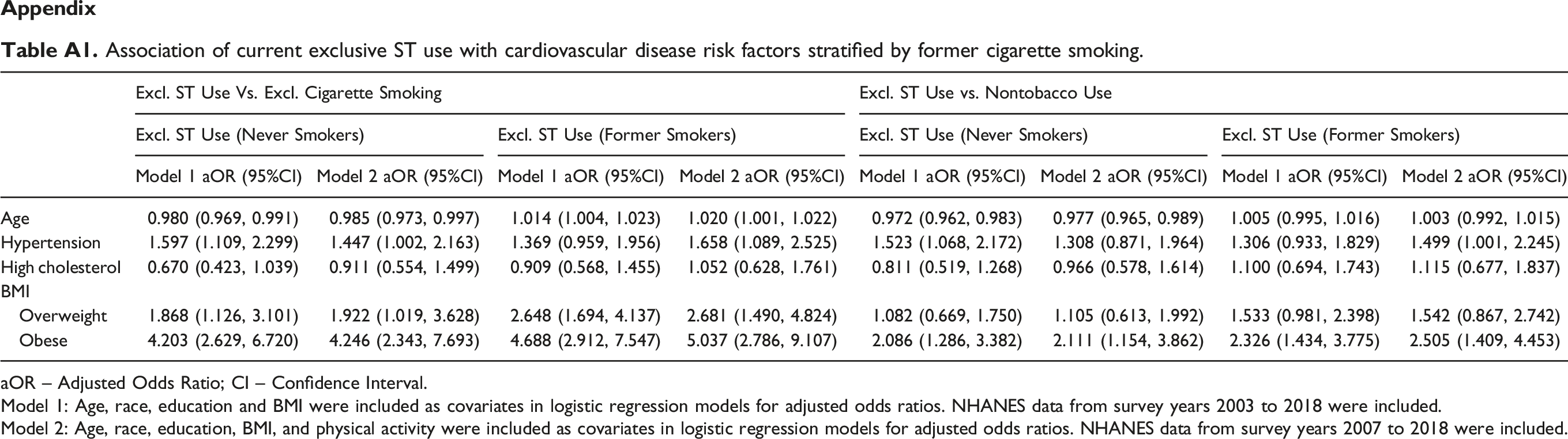
Excl. ST Use Vs. Excl. Cigarette Smoking
Excl. ST Use vs. Nontobacco Use
Excl. ST Use (Never Smokers)
Excl. ST Use (Former Smokers)
Excl. ST Use (Never Smokers)
Excl. ST Use (Former Smokers)
Model 1 aOR (95%CI)
Model 2 aOR (95%CI)
Model 1 aOR (95%CI)
Model 2 aOR (95%CI)
Model 1 aOR (95%CI)
Model 2 aOR (95%CI)
Model 1 aOR (95%CI)
Model 2 aOR (95%CI)
Age
0.980 (0.969, 0.991)
0.985 (0.973, 0.997)
1.014 (1.004, 1.023)
1.020 (1.001, 1.022)
0.972 (0.962, 0.983)
0.977 (0.965, 0.989)
1.005 (0.995, 1.016)
1.003 (0.992, 1.015)
Hypertension
1.597 (1.109, 2.299)
1.447 (1.002, 2.163)
1.369 (0.959, 1.956)
1.658 (1.089, 2.525)
1.523 (1.068, 2.172)
1.308 (0.871, 1.964)
1.306 (0.933, 1.829)
1.499 (1.001, 2.245)
High cholesterol
0.670 (0.423, 1.039)
0.911 (0.554, 1.499)
0.909 (0.568, 1.455)
1.052 (0.628, 1.761)
0.811 (0.519, 1.268)
0.966 (0.578, 1.614)
1.100 (0.694, 1.743)
1.115 (0.677, 1.837)
BMI
Overweight
1.868 (1.126, 3.101)
1.922 (1.019, 3.628)
2.648 (1.694, 4.137)
2.681 (1.490, 4.824)
1.082 (0.669, 1.750)
1.105 (0.613, 1.992)
1.533 (0.981, 2.398)
1.542 (0.867, 2.742)
Obese
4.203 (2.629, 6.720)
4.246 (2.343, 7.693)
4.688 (2.912, 7.547)
5.037 (2.786, 9.107)
2.086 (1.286, 3.382)
2.111 (1.154, 3.862)
2.326 (1.434, 3.775)
2.505 (1.409, 4.453)