
Abstract
Purpose
To develop a culturally-tailored American Indian/Alaska Native (AI/AN) women’s Facebook group supporting opioid recovery as an adjunct to medication.
Design
Community-based, qualitative approach.
Setting
Minnesota, U.S.
Participants
AI/AN women in opioid recovery, interested parties, and a Community Advisory Committee (CAC) of AI/AN women with lived experience, health care providers, and community members.
Intervention
We developed evidence-based content focusing on stress/trauma and substance use, mindfulness, responding to triggers, and supportive community resources. Additional content centered on AI/AN culture was also selected.
Method
Interviews were conducted by two women, then transcribed and coded using content analysis with NVivo software. Results were presented to CAC for further content refinement.
Results
CAC members (n = 10) guided study methods, intervention development, and dissemination activities. 14 AI/AN women (mean age 36.4 years; mean 6.7 months opioid abstinence) and 12 interested parties (7 men, 5 women) were receptive to an AI/AN gender-specific Facebook group, preferring content with AI/AN people and/or text resonating with AI/AN culture (e.g., Native traditions, family, personal stories, historical trauma). Recommendations included (1) protect confidentiality, (2) retain positivity, (3) incorporate resources and exercises to build coping skills, and (4) moderators should be authentic and relatable to build trust.
Conclusions
Our approach provides a model for developing culturally tailored, appealing and effective social media interventions to support AI/AN women in recovery from opioid use disorder.
Keywords
Purpose
Opioid Use Disorder (OUD) is a major public health problem associated with significant morbidity and mortality1-3 that disproportionately affects American Indian and Alaska Native (AI/AN) adults. 4 Behavioral strategies to promote the use of medications for OUD (MOUD) (i.e., buprenorphine, methadone, and naltrexone) and evidence-based support for OUD recovery are crucial to prevent return to use.5-11
Elevated OUD risk among AI/AN adults is due in part to inequities across social determinants of health and generations of historic trauma.12,13 In Minnesota, drug overdose deaths are 7 times more likely among AI/AN adults than white adults, with opioids as the leading drug. 14 Although gender-specific risk factors for return to use in women have been identified, including perceived and biological stress reactivity, trauma, and perceived social isolation,15,16 gender-specific interventions for AI/AN women recovering from OUD do not exist. 17
Strong social networks have been shown to support opioid recovery. 18 Pilot studies found that face-to-face interventions involving concerned others or peer outreach workers to support MOUD engagement and opioid recovery resulted in higher treatment retention.19,20 Other research indicates that individuals in recovery utilize online social networks (e.g., Reddit) for peer support.21,22 Such networks align with the AI/AN value of interdependence.23-26 A previous study developed by members of this research team with others 27 demonstrated that a moderated Facebook group could be successfully developed, culturally tailored, and implemented using similar CBPR principles and intervention approaches to promote smoking quitline utilization among Alaska Native adults living in Alaska. In the pilot randomized-controlled trial of the intervention (N = 60), the proportion of study participants utilizing an evidence-based quitline was double for those participating in the Facebook group compared to control group participants, a signal toward intervention efficacy. However, the feasibility of a social media group intervention specifically supporting opioid recovery for AI/AN women has not been explored.
Addressing these gaps, we developed a 3-month, moderated, private Facebook group intervention promoting stress management and social support for opioid recovery among AI/AN women in Minnesota receiving MOUD. Social media group interventions supporting opioid recovery could lead to greater adoption and sustainability of opioid recovery by encouraging AI/AN women and leveraging community resilience for stress management.28-31 The study has 3 phases, consistent with Stage I early behavioral addictions treatment development 32 : (1) qualitative development of content, (2) content refinement and moderator training, and (3) intervention beta-testing. In this paper, we describe our community-based participatory research (CBPR) approach and phase 1, the qualitative development of content.
Approach
This pilot study, supported by the National Institute on Drug Abuse Clinical Trials Network (CTN-0123), received approval from the Mayo Clinic Institutional Review Board (IRB 22-000477). We registered the study with clinicaltrials.gov (NCT05340855) and conducted phase 1 participant enrollment and data collection from April 2022 to October 2022.
Our CBPR approach optimizes the relevance, acceptability, and cultural congruence of study materials and methods.33,34 The Minnesota Indian Women’s Resource Center identified the need for a gender-specific opioid intervention for AI/AN women and co-created the study concept. The research team includes Indigenous persons and experts in CBPR and opioid addiction within AI/AN communities. We also formed a Community Advisory Committee (CAC) with diverse Tribal representation from AI/AN women with lived experience, Elders, health care providers, and community members. We obtained study input during 5 video meetings. Additionally, the research team met twice with the Healthy Nations Advisory Board (HNAB) of Tribal health leaders representing AI/AN communities throughout Minnesota. The HNAB provided input on the study eligibility criteria, preliminary qualitative findings, and content before and after interviews were conducted. CAC and HNAB members received an honorarium for meeting attendance.
Setting
Minnesota’s Tribal communities comprise 1.1 percent of the state’s population (MN Department of Health, 2018) and include 11 tribes: 4 Dakota communities in southern MN (Upper Sioux, Lower Sioux, Shakopee Mdewakanton, and Prairie Island) and 7 Anishinaabe reservations in northern MN (Mille Lacs Band of Ojibwe, Leech Lake Band of Ojibwe, White Earth Nation, Red Lake Nation, Boise Forte Band of Chippewa, Fond du Lac Band of Lake Superior Chippewa, and Grand Portage Band of Lake Superior Chippewa). 35 Many live within their Tribal communities, but some have relocated to urban areas including the Minneapolis/St. Paul region. These individuals are described as urban AI/AN people and can originate from any of the 574 federally recognized tribes across the United States.
Participants
Interview Participants
Sampling Strategy
We used a purposeful sample 36 of AI/AN women in opioid recovery and interested parties (e.g., health care providers or community experts in opioid recovery, culture, and AI/AN health), estimating 12 interviews for each subsample based on recommended guidelines for the number of interviews needed to reach data saturation. 37
AI/AN Women
We recruited AI/AN women via clinician and staff referrals from addiction treatment and community health care settings that specifically treat and/or serve the needs of AI/AN people in Minneapolis and St. Paul, MN. A recruitment flyer and a 1-page study information sheet for their staff were developed with the CAC. The research team held in-person information meetings and handed out flyers, sheets, and business cards.
Study eligibility criteria
Interested women called or emailed the study team. Women were eligible if they: (1) self-identified AI/AN race; (2) identified as a woman; (3) were ≥18 years old; (4) resided in Minnesota; (5) met criteria for OUD based on the DSM-5 Checklist (American Psychiatric Association, 2013); (6) self-reported ≥30 days of opioid abstinence (e.g., oxycodone, heroin, fentanyl) based on the Timeline Follow-Back Interview 38 ; (7) self-reported current MOUD use; (8) were comfortable speaking and reading in English; (9) had broadband internet access; and (10) were familiar with Facebook. Individuals were excluded from participating if they reported current suicidality (based on 3 items from the Concise Health Risk Tracking—Self Report (CHRT-SR) Suicidal Behavior Evaluation). 39 If women did not meet the eligibility criteria, we provided them with referral resources.
Interested Parties
Interested parties were health care providers or community partners with a role in promoting opioid recovery for AI/AN women. We sought their input on improvements for use of the intervention within AI/AN health care settings and communities. The CAC, HNAB, and community partners referred interested parties. Additional eligibility included: (1) knowledge of AI/AN culture and/or OUD treatment/recovery among AI/AN people; (2) comfortable speaking and reading in English; (3) broadband internet access; and (4) familiarity with Facebook. All genders and races were eligible.
Intervention
Drawing upon evidence-based practices, the research team identified key content areas to promote recovery, which were then presented to the CAC for feedback. Key content areas included: stress/trauma and substance use, mindfulness techniques, recognizing and responding to substance use triggers, and community resources supporting opioid recovery. The content drafted utilized core concepts from evidence-based treatments: mindfulness-based relapse prevention (MBRP) 40 and the Stress Management and Resiliency Training (SMART) program. 41 MBRP is a group-based treatment integrating mindful meditation with traditional cognitive behavioral return to use prevention skills, 40 is effective for a variety of substances,42-44 and is a promising adjunct to MOUD.45,46 Treatment components include increasing awareness of substance use triggers and cravings and learning new ways (e.g., mindfulness strategies and behavioral skills) to respond to elicited sensations. 40 The SMART program utilizes 4 concepts to decrease stress and enhance resilience: gratitude, mindful presence, kindness, and resilient mindset. 40 SMART has reduced perceived stress among women and diverse populations. 47 The research team identified publicly available content, including AI/AN imagery where possible, and developed text aligning with these treatments. We also identified publicly available content relevant to AI/AN culture and the arts and highlighting women’s experiences of AI/AN opioid recovery. Finally, we developed an online landing page so participants could access resources and referral information addressing a variety of needs related to opioid recovery.
In selecting and refining our content for cultural relevance, the research team applied cultural variance and surface/deep structure frameworks,48,49 accounting for AI/AN cultural influence on health behaviors. Surface structure matches materials to observable sociobehavioral characteristics (e.g., AI/AN people, music, and clothing) and enhances receptivity, comprehension, and acceptance of messages. Deep structure incorporates cultural beliefs and norms (e.g., communication styles and social rejection of opioid use), values (e.g., interdependence), and ways of knowing,29,31,50,51 and imparts meaningful relevance.
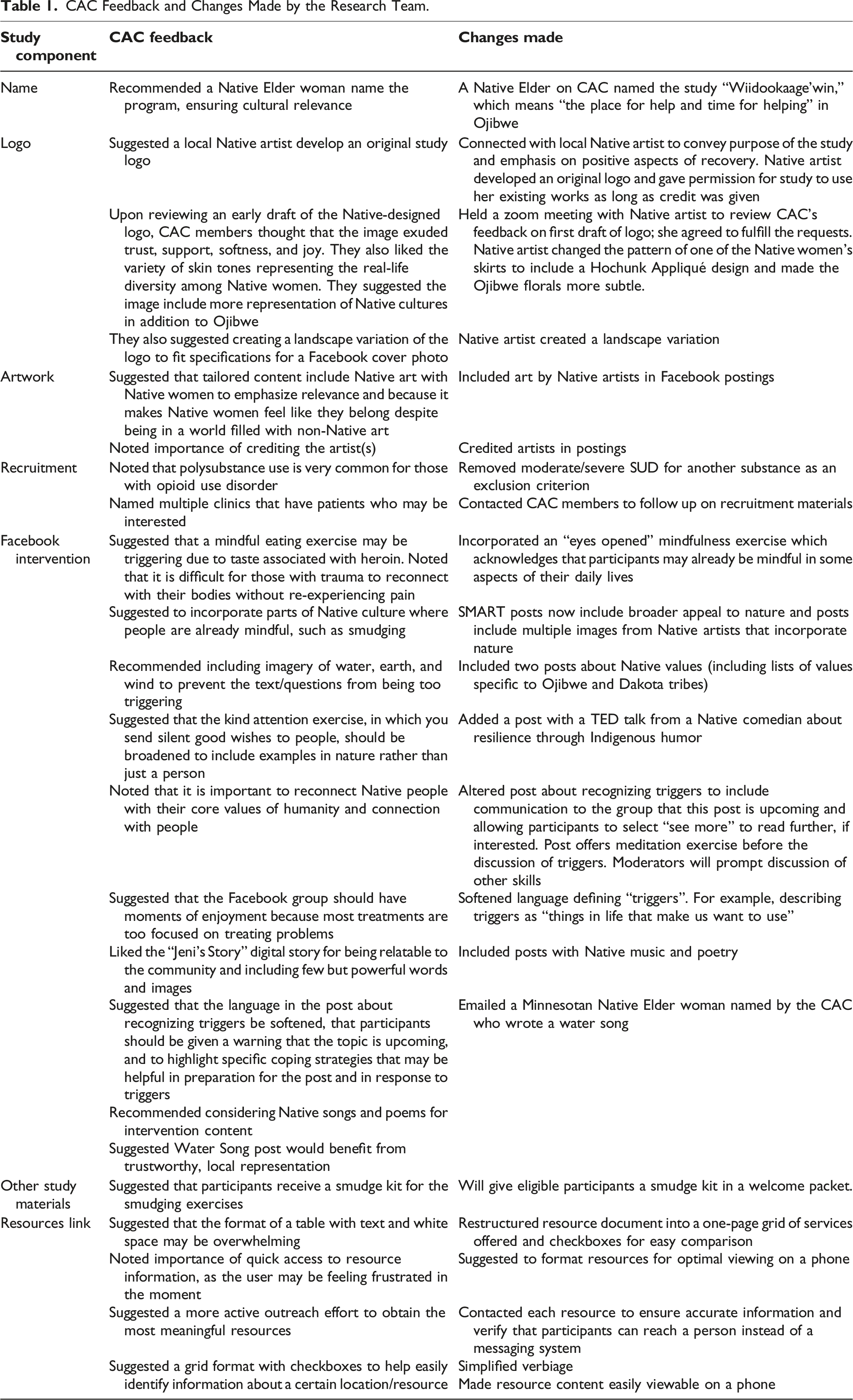
CAC Feedback
CAC Feedback and Changes Made by the Research Team.
Selection of Content Postings for Qualitative Interviews
After incorporating CAC feedback, we selected 7 postings to evaluate qualitatively: 3 publicly available videos and 4 image/text-based postings. The videos, all featuring AI/AN women, included: (1) Jeni’s Story, a Native woman’s opioid recovery story published by the CDC, 52 (2) a discussion by Faith Spotted Eagle, a member of the Yankton Sioux Nation, activist and politician, who published a YouTube video about historical trauma and healing from addiction, 53 and (3) a video presentation of the Algonquin Water Song, where generations of AI/AN and non-Native women, the water-protectors, are invited to celebrate water, the giver of all life. The video features water, nature, and women connecting and singing about the interconnectedness of all life, and the protection of water from pollution and drought. 54 The remaining 4 text/image-based posts were drafted by 2 study team clinical psychologists and paired with existing AI/AN imagery. Each described the concepts “Urge Surfing,” “Triggers,” “Gratitude,” and “The 2-Minute Rule,” which align with the MBRP/SMART programs.
Method
Informed Consent
The informed consent and enrollment processes were conducted by phone.
Interviews
Interviewers emailed or texted participants a link to the 7 postings. Interviews were conducted by phone or Zoom. Interviewers included 2 women (1 American Indian) trained in qualitative interviewing and active listening. Active listening was employed to increase rapport by reflecting the participant’s responses, allowing the participant to elaborate, confirm, or correct the interviewer’s interpretation. 55 Interviewers took field notes and audiotaped each interview, which was then transcribed by a professional transcription service. Upon completion, participants received a $50 cash card for their time.
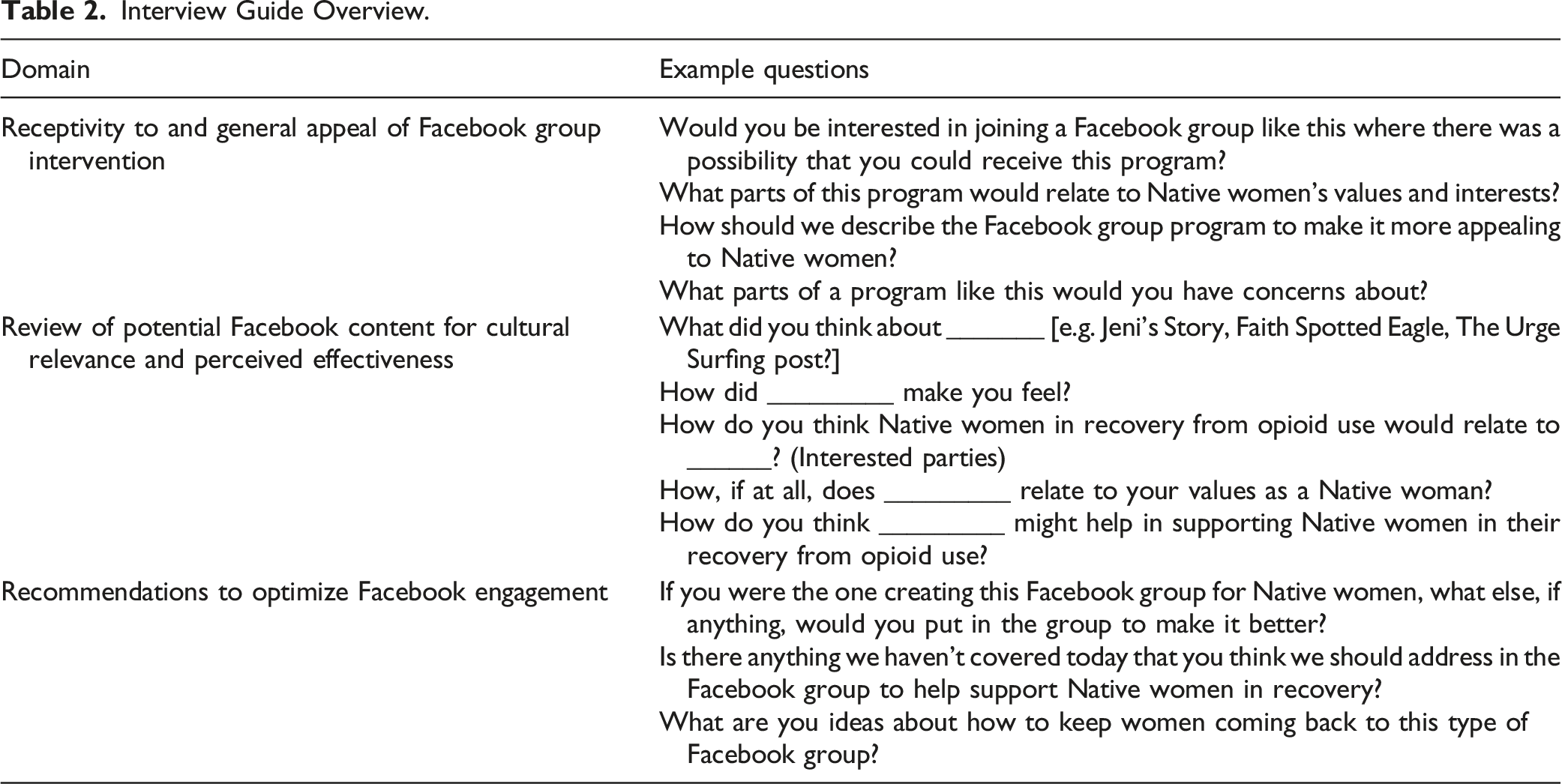
Interview Guide
Interview Guide Overview.
Qualitative Analysis
We summarized sample characteristics using descriptive statistics. We used content analysis 58 supplemented with QSR NVivo software 59 to generate response themes that were primarily deductive in that they were based on the semi-structured interview guide. Three study team members (PS, AY, CS) independently reviewed 4 transcripts each and identified codes. They then met to discuss codes until they came to consensus on the codebook. A fourth team member reviewed the codebook and provided feedback (CP). Once the final codebook was established, 2 study team members coded jointly on Zoom (PS, AY), with 1 member coding and the other observing for quality control. Coding jointly allowed rich discussion of any new or emerging themes as well as whether we were starting to obtain no new information from interview participants, known as data saturation.37,60 A third team member resolved any major coding discrepancies as needed (CP or CS). When it was determined that data saturation was likely achieved, these findings were discussed with the third team member as well as with our CAC. Coded data were examined for patterns across the AI/AN women and interested parties. The CAC and HNAB then guided the interpretation and integration of the qualitative findings into content refinement.
Results
Participant Socio-Demographics and Time in Opioid Recovery.
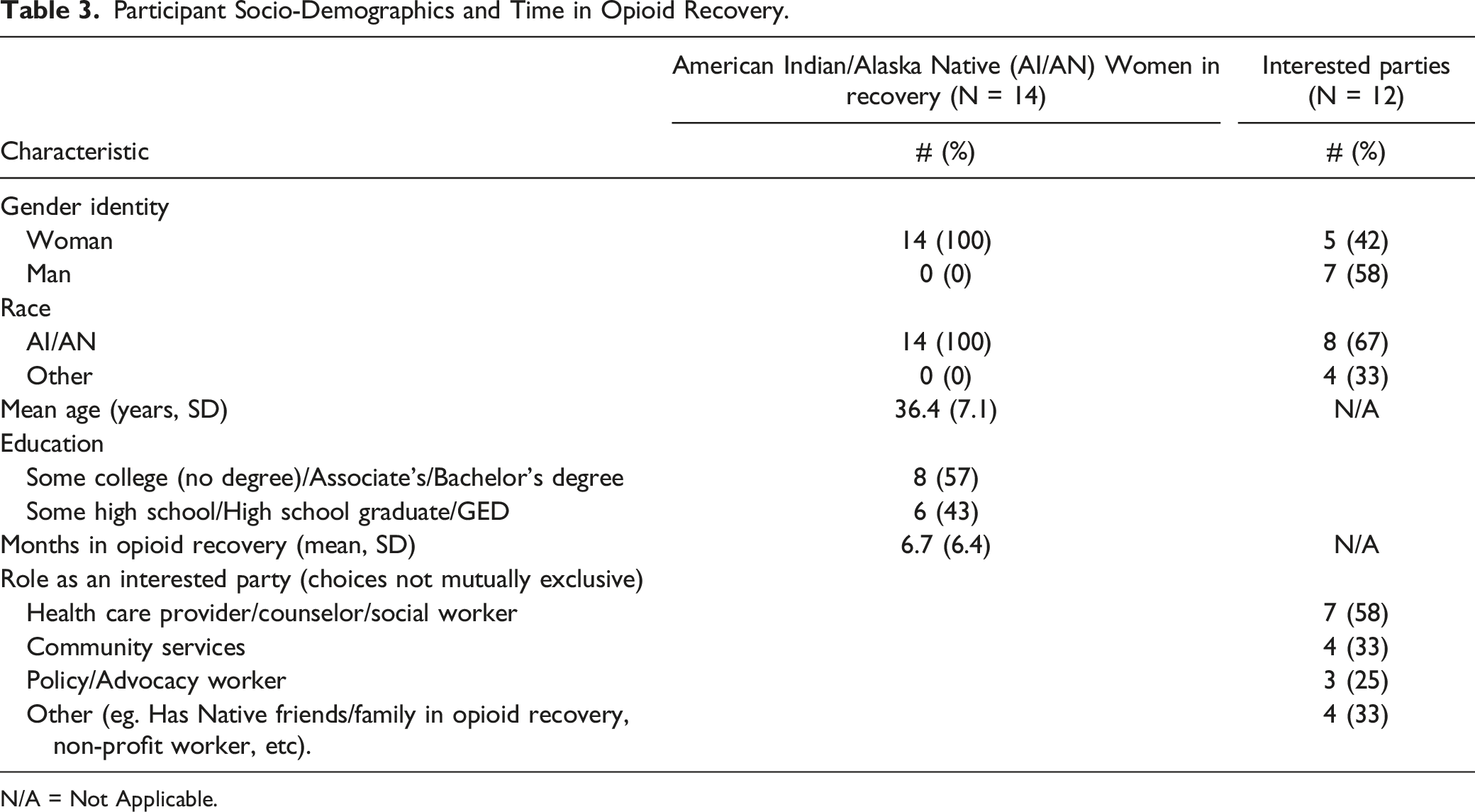
N/A = Not Applicable.
The overarching interview domains included (1) receptivity to the Facebook intervention, (2) cultural relevance and perceived effectiveness of the content, and (3) recommendations to optimize Facebook engagement. Many themes emerged, including AI/AN culture, positivity, relatability, recommendations, and concerns, which are described below with representative quotes. The supplemental material provides additional illustrative quotes highlighting our findings.
Receptivity to a Facebook Intervention Specifically for AI/AN Women
Overall, receptivity to the concept was positive, with few concerns. One interested party thought the idea was interesting because AI/AN women in recovery may not be ready for an in-person group, and the Facebook group could be a private space away from their current treatment. Both groups raised concerns about building trust and maintaining confidentiality, especially if someone returns to use (e.g., sharing screenshots and “gossiping”). One interested party expressed: Since you’re recruiting women in recovery of opioids, what if they relapse and what if they break confidentiality? That’s the biggest issue with any of these type of groups is that trust factor. We can’t heal if…we can’t be honest with each other. If you feel like, “Oh, no, somebody’s gossiping,” …you’re gonna hold back, and you’re really not going to get the full potential of the group. (IP1)
Similarly, 1 woman expressed how important it was to have an AI/AN-only space to build trust: …Alotta women will come just because it's Native-American-based. Like for myself, I won't go to a Facebook page if there's other ethnicities. What you're doin' right now has never really happened before. What you're doin', it will entice people to come into your group even without the extra words and whatnot. (W5)
To allay concerns about confidentiality, recommendations were that moderators should also be AI/AN and that the women in the group should have a role in creating group guidelines. To capture general receptivity succinctly, participants were asked for 1 word to describe the group. All responded with positive words (e.g., “hope”). Some chose descriptive phrases in their culture, such as “wiizokeatatiwin” (“the way to seek what is cherished but hidden” in Ojibwe) (Figure 1). One word to describe the Facebook group.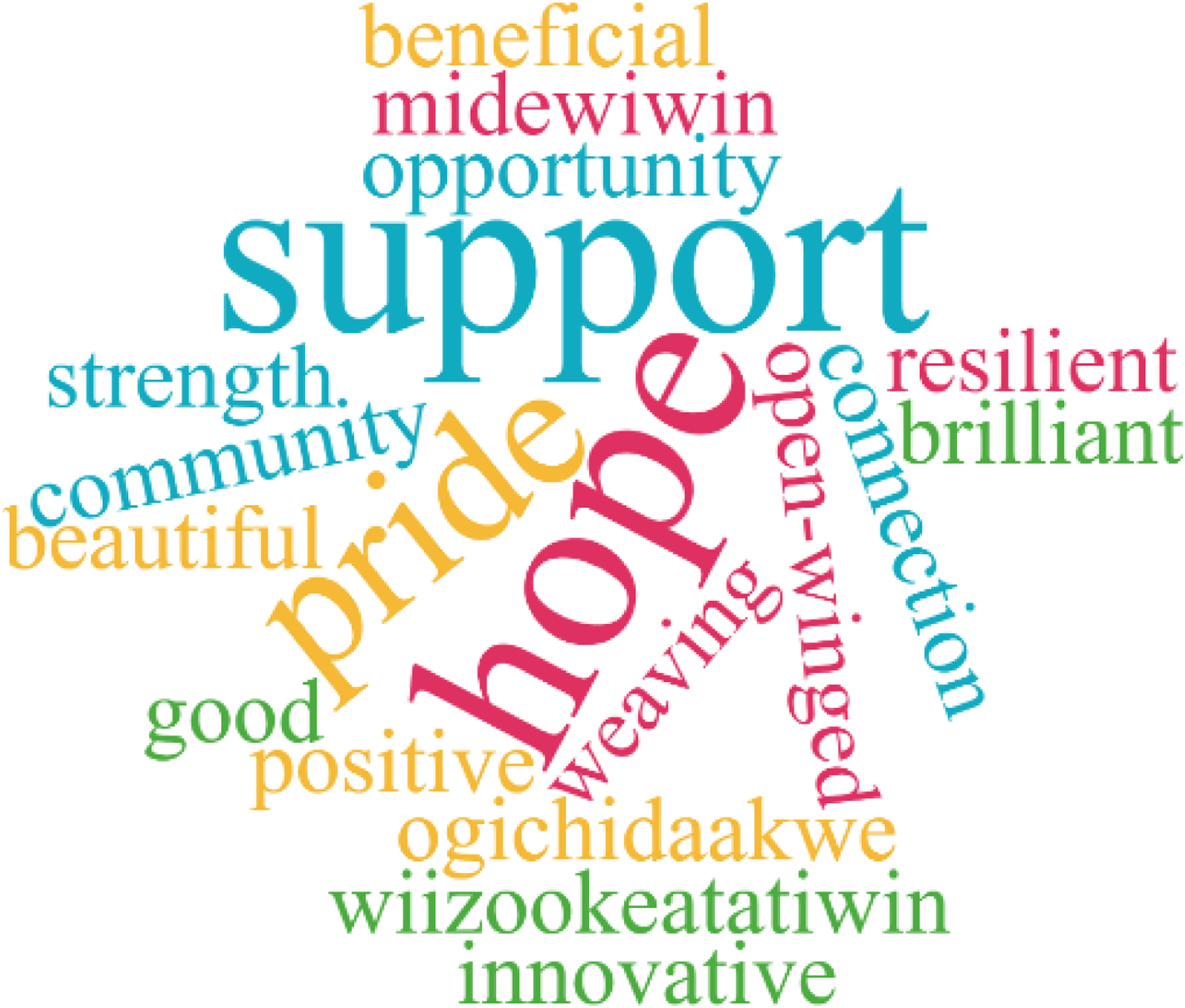
Cultural Relevance and Perceived Effectiveness/Helpfulness of Content
Overall, receptivity to the text and imagery was positive, with few concerns. Social media posts reflecting AI/AN imagery and values (i.e., nature, family, community, storytelling, AI/AN practices and events) were perceived as relatable, helpful, and/or effective. For example, most participants liked the gratitude post with nature imagery because both are prevalent in AI/AN culture. One woman explained: Anytime there’s a feast or anything, we give thanks for that food. If somebody shot a deer,…we put tobacco down for the creator to just give thanks for that animal, for sustenance for our bodies. Yeah, we do. We give thanks for everything. We’re very grateful people. We are very… grateful for Mother Earth. (W2)
For Jeni’s Story, participants expressed distrust in the CDC and wished that the video was longer. However, participants liked Jeni’s Story for its representation of a young Native woman wearing traditional Native clothing, drumming, and telling her recovery story and how she reconnected with her culture, providing hope that any AI/AN woman can do the same. One woman stated: …you'll need to do a lot of those. [We] have to be in this support group so we can see that there is hope. A lotta people don't—a lot of women don't think there's hope, that they can't get out of addiction or even stay sober. They have to see a lot of stories like that to see that it is possible. Yes. I like her story. I lost my culture. I wanna be able to practice it again. (W5)
An interested party noted the benefits of reconnection for support and recovery maintenance: When you get sober and you get back into your culture, you start to become surrounded by all those smiles that were in the video, and all that positivity. That was a good aspect that they showed. ‘Cause I can only imagine the Native American women in the group seeing that video, seeing those people dancing at the powwow, stuff like that, and instantly getting reminded maybe of when they were a kid, and they felt their joy. If they didn’t experience it as a kid, it’s something that they can look forward to actually experiencing. (IP3)
Content featuring triggers and cravings was perceived as a neutral or negative fit with AI/AN culture. As 1 woman stated, “Like I said before, there isn’t no drug addiction…in Native American culture.” (W7) However, most participants thought including such content was relatable and important. One interested party noted, I think this would be helpful to Native women or anybody really working through recovery ’cause they’re building awareness of their triggers…it’s little by little building that toolkit of awareness of my environment…awareness of my inner landscape…and how it might be urging me to use or link to cravings or link to reaching for a coping mechanism that is not healthy. (IP2)
Participants offered suggestions to improve the imagery’s resonance with AI/AN values (e.g., nature) or include AI/AN people practicing culture-specific activities. In fact, 1 participant suggested the Urge Surfing image include an AI/AN woman surfing. Few suggestions to the text were made besides improving clarity. One interested party felt that mindfulness had been culturally appropriated, so participants could reclaim it with culture-specific exercises such as smudging or expressing gratitude. One woman explained how culture-specific exercises, including smudging, helped her during her recovery: When I was in active addiction, I too went away from my culture and all the practicing of my tradition, with the medicines. That’s what actually helped me stay on my road of recovery, on the Red Road, was to smudge when I needed to, and start going back to my tradition. Now that I’m sober, I want to start teaching it to my kids, and I do. (W1)
The Water Song received the most mixed response from both samples. Participants responded positively to its message. One woman stated, “It gives you strength…That you can do it. You’re not alone.” (W9) Participants responded both positively and negatively to the inclusion of non-Native women. One example of a positive response was a perceived relevance to AI/AN culture because “every tribe can relate to singing and dancing.” (W3) One example of a negative response from a woman was, “I get their point they’re trying to make. I don’t know. I kind of really didn’t like seeing those other people in here.” (W6) They also noted that the high production value of the video felt inauthentic, describing it as “way too New Age.” (IP8) One interested party suggested replacing it with a local water song to improve connection to the content: I think the women would probably benefit more from the Women’s Midewiwin Lodge in Madeline Island where that song comes from if they had the teaching that comes with that song and the women that are empowered that run the ceremony… I think that would be 10 times more impactful than a commercialized version of the song… But I think if these things are gonna be portrayed, then they should be portrayed from the people where it originated from and where it’s still utilized. That way you’re paying homage or service to the originality or the area of which this demographic of people comes from. (IP4)
Regarding perceived effectiveness/helpfulness of content, a subtheme emerging from most interviews was the importance of positivity. Participants tended to praise images that elicited relaxation and/or positive memories (e.g., their children singing/dancing). One woman noted that negative habits and thoughts tend to linger, so having positive coping techniques may lead to better recovery outcomes. One interested party noted, …tapping into what I call…resilience and brilliance of…our women is very important, ‘cause I think there can be a heavy trauma emphasis and being burdened by our traumas and then also layers of mental health issues and then substance use, it can feel like a lot together. (IP2)
Interested parties recommended caution when discussing potentially difficult topics. For example, they suggested limiting the word “triggers” in the “Recognizing Triggers” post. Other suggestions were to preface the triggers post with a warning that a discussion of triggers was coming, so women can decide if they would like to view the content. They also recommended waiting to share the post until after women had viewed skill-building posts and built rapport with moderators and other participants, increasing their chances of accessing support, exercises, or resources when interacting with challenging content. Another recommendation was that moderators closely monitor group discussions surrounding triggers, traumas, and return to use and be ready to offer resources and guidance after each discussion. One interested party stated: …it's not just a “how to do this” but just, I think, really connecting people to their local resources. Beyond their Facebook group, then where can I go to be in a sober community, where I'm not gonna get triggered? Talking about that, I think…that'll be super helpful. (IP6)
We asked for their favorite video to gauge what resonated with our participants. Most selected the Faith Spotted Eagle video linking historical trauma to addiction and then healing. She noted the resilience of AI/AN people and how they still laugh and come together despite their traumas. One AI/AN woman explained how the video may help the participants: Just to let 'em know there is people that did go through it. They’re still here. They made it… That there’s help…you don’t have to be embarrassed. There’s other people that went through it… It’s okay to talk about it. Just to make sure you heal, and get a better understanding of all of it, and heal…yeah, just heal. (W9)
Another woman expressed that it felt “amazing” to hear her words and she “felt like [she] was in her shoes.” She stated: “I got to learn a little bit more about how trauma is and the layers and how…that trauma could pass down to your kids…I don't want that to happen. I don't want them to carry my burden.” (W8) One interested party explained how the video could promote healing: Your trauma becomes your strength, and even Native language it's your shield. It's like, no, you don't get to do that to me no more. You have no place here. You can't even get inside this, 'cause I have a shield of restorative trauma, no one's ever gonna treat me that way again. (IP7)
Recommendations to Optimize Facebook Engagement
Participants emphasized the importance of AI/AN culture, support, confidentiality, and trust when asked for recommendations to optimize Facebook engagement. One interested party summarized: I think just immerse the [Facebook group] into…our culture, nobody else’s. This is women that can share or ask for things that this group will try to support them in. Do they wanna make a change in their life and they don’t know what or how to go about it? That’s where the support comes in. Sometimes you’re not lookin’ for an answer. You’re just lookin’ for somebody to listen. (IP1)
The theme of positivity returned in this area with women saying that they needed a “relaxing and calming” and “inviting” (W8) healing space to engage. One woman stated, “Being in addiction, you need to have fun things in your life to keep your mind right.” (W2) One interested party noted the importance of engaging with the arts: … I'm big on empowering…I love our people, our culture, so bringing in Native women, Native stories, Native artists, Native bands, Native whatever of people that are in recovery ’cause the recovery community within Natives is very large…and a lot of us create art. A lot of us create music. A lot of us create poetry. (IP4)
Interested parties stressed the importance of group moderators maintaining a positive atmosphere stating, “[the moderator] can become the first positive active listener in their life in a long time,” (IP8) with recommendations that moderators be “less professional” and “more real” (IP4) in their communication, showing compassion in their language and the posts.
Participants recommended including Minneapolis-specific resources, especially family services, childcare, and shelter. Other recommendations included posting an AI/AN word of the week and a document where women can provide feedback on local resources. Many suggested live events, chats, interactive discussion prompts, and polls. Finally, an interested party suggested having the women create the group guidelines with an Elder and have opportunities to post their own content. One interested party said: “Sometimes I can see, like, people hurting each other, and those are some ground rules that I would definitely emphasize and taking care of each other as women, making their Facebook kind of, like, a sacred place as well.” (IP5)
Final Content Refinement with CAC
After analyzing the qualitative data, we discussed our findings with the CAC. We particularly sought recommendations to refine the “Recognizing Triggers” and “Water Song” posts. The CAC agreed that the “Recognizing Triggers” post should not overuse the word “trigger” and should be prefaced with preparatory resources and exercises (e.g., grounding). They also advised how moderators could respond to participants’ concerns about non-Native representation in the Water Song video, suggesting a local Native Elder woman who could share a local Water Song. In response, we revised the posts accordingly and finalized our content library of 9 videos and 22 text/image posts. Figure 2 illustrates how we synthesized our qualitative data and CAC feedback into our content. Examples of content revisions.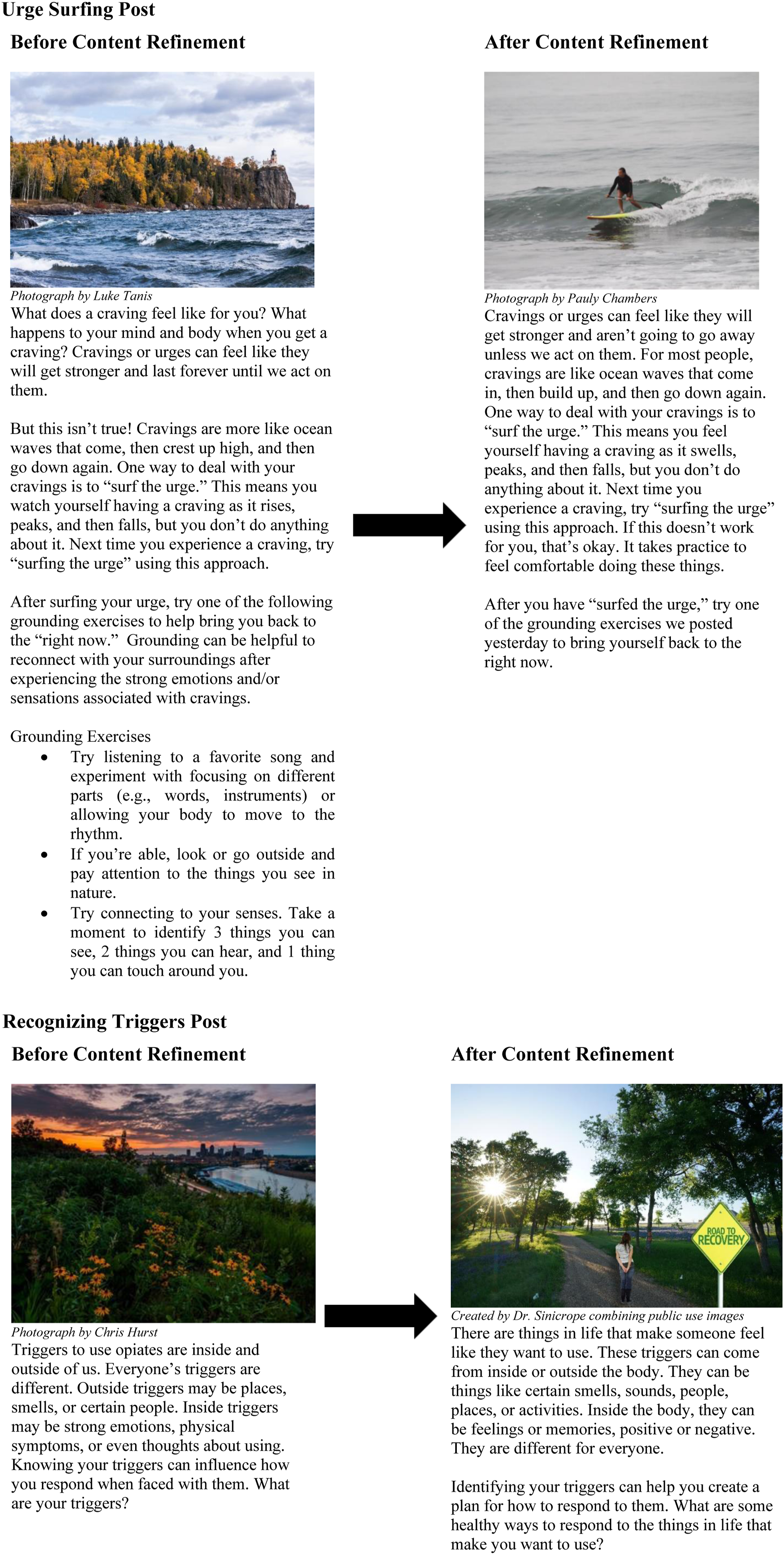
Conclusions
Our study provides information for developing a Facebook group intervention to support AI/AN women in recovery and taking MOUD that incorporates evidence-based practices with the preferences of AI/AN women and interested parties. Participants agreed there is a need for a private, closed Facebook group solely for Native women in recovery. AI/AN women said they would feel most comfortable participating in a group that only includes other AI/AN women, providing an environment where they would feel safe to share and improve their ability to trust and build rapport. They also liked that the participants would learn stress management and mindfulness skills and have access to resources covering a wide variety of needs. Interested parties recommended that moderators use a solution-focused, authentic approach for content and engagement. Though substance use is not a historical part of Native culture, participants felt it was important to address it directly. Overall, participants preferred positive content focused on stress management and mindfulness, addressing safety, privacy, and trust concerns. Throughout the interviews, it became apparent that participants preferred content to be centered on connecting with AI/AN culture and to feature AI/AN women and their stories, which aligns with current literature that supports recentering OUD recovery within an AI/AN cultural framework to promote acceptability, engagement, and recovery.61,62
Data saturation was reached despite a small number of participants, likely because we enrolled individuals with particular experiences and expertise and asked for feedback on specific aspects of intervention content. Furthermore, interview content had already been reviewed and revised for cultural congruence with our CAC, and the semi-structured guide tightened the interview’s focus. In addition, interviews with interested parties lasted longer than anticipated, (111 minutes on average), giving respondents the opportunity to provide detailed feedback, which likely contributed to data saturation.
Study limitations include the small number of primarily urban participants from whom we gathered data, so findings may be different for AI/AN women living on reservations or rurally. Despite this, our purposeful sample size reflects qualitative analysis needs for deep understanding vs generalizability, and saturation of data was reached. Relatedly, it is important to note that though our study broadly represents participation from AI/AN women, we screened for AI/AN identity using a yes/no self-report question, which does not richly explore an individual’s connection to AI/AN culture or its importance to them. Additionally, we did not ask about participant Tribal affiliation, and cultural traditions and practices vary across tribes. A deep understanding of participants’ connection to their cultural identity is important in contextualizing feedback and developing culturally-relevant interventions. As such, for the next phase of the study, a beta-test of the intervention, we included a question assessing the degree to which participants identify with their AI/AN culture. 63 Despite these limitations, no other social media group interventions are currently offered for AI/AN women, so this intervention represents a strong start toward offering such services. Study strengths include the community-based and qualitative approach throughout. Since no gender-specific social media groups for AI/AN women in opioid recovery exist, our interviews allowed us to gather rich description about a topic where little is currently known. Our community-based approach helped ensure we developed a meaningful intervention meeting an expressed need. Our next steps are to beta test the intervention with 10 AI/AN women and then to conduct a randomized pilot trial.
This formative study is the first step to developing a social media intervention that could be widely disseminated as an adjunct to addiction treatment. The process of developing and refining content to fit with AI/AN culture contributes to a growing body of knowledge on how to apply effective risk communication strategies on social media, an approach that could be replicated in future studies. Opioid Use Disorder (OUD) affects American Indian and Alaska Native adults more than others. To stop a return to use, we need to promote the use of culturally-centered approaches. Women and men use opiates for different reasons. For women, some of these reasons include stress, trauma, and being socially isolated. To address these unique needs, we developed an online Facebook support group just for AI/AN women who are already taking medications for OUD. This article adds information on how to develop a FB group that is centered on AI/AN culture and the specific needs of women using an approach that incorporates the expressed needs of this community. This will be the first online group intervention just for AI/AN women in recovery and receiving medications for opioid use disorder.So What?
What is Already Known on This Topic?
What Does This Article Add?
What are the Implications for Health Promotion Practice or Research?
Supplemental Material
Supplemental Material - Wiidookaage’Win: A Community-Based Qualitative Approach to Developing a Facebook Group Intervention for Native Women to Support Recovery From Opioid Use
Supplemental Material for Wiidookaage’Win: A Community-Based Qualitative Approach to Developing a Facebook Group Intervention for Native Women to Support Recovery From Opioid Use by Antonia Young, Pamela Sinicrope, Sydney Kelpin, Anne I. Roche, Corinna Sabaque, Cuong Pham, Lisa A Marsch, Aimee N. C. Campbell, Kamila Venner, Emily Bastian, Teresa Nord, Gail Mason, Laiel Baker, Thomas Wyatt, Amy Fish, Gavin Bart, and Christi A. Patten in American Journal of Health Promotion.
Footnotes
Acknowledgments
We thank the members of the Community Advisory Committee who helped to guide all aspects of the project. We appreciate the members of the Healthy Nations Advisory Board who provided substantial input on the project. A special thank you to Sharyl WhiteHawk for naming the study, to Celina Downwind-Jubera for creating the artwork for the study logo, and to Kimberly Kinnoin for preparing our manuscript for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Institute on Drug Abuse, Clinical Trials Network (UG1DA040316-07S3, CTN-0123).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.