
Abstract
Purpose
Understand how weekly monetary incentives for dietary tracking and/or weight loss impact 6-month weight loss behavioral adherence.
Design
Secondary analysis of participants randomized to one of four conditions in a behavioral weight loss intervention: incentives for dietary tracking, incentives for weight loss, both, or none.
Setting
Participants were asked to self-weigh at least twice weekly, log food and drink in a mobile application five days weekly, and attend bi-weekly, group-based classes.
Sample
Data from (n = 91) adults with obesity who completed a 24-week behavioral weight loss intervention of whom 88% were female and 74% Non-Hispanic White, were analyzed.
Measures
Non-adherence to weight and dietary self-monitoring was defined as the second week of not meeting criteria. Class attendance was also tracked.
Analysis
Kaplan-Meier analyses were used to examine differences across the four conditions.
Results
Participants incentivized for dietary self-monitoring had an average 15.8 weeks (SE:1.2) until the first non-adherent week compared to 5.9 weeks (SE:0.8) for those not incentivized for dietary self-monitoring (P < .01). Those incentivized for weight loss had an average 18.0 weeks (SE:1.02) of self-weighing until the first non-adherent week compared to 13.5 weeks (SE:1.3) for those not incentivized for weight loss (P = .02). No difference in class attendance was observed.
Conclusions
Incentivizing behaviors associated with weight loss improved adherence to those behaviors and does not appear to spill over to non-incentivized behaviors.
Purpose
The Centers for Disease Control and Prevention (CDC) estimates that 42% of adults in the U.S. have obesity, defined as a body mass index of at least 30 kg/m2. 1 Obesity is linked to diseases such as cardiovascular disease, stroke, type 2 diabetes mellitus, and various cancers. 2 Obesity is associated with diminished quality of life and increased financial strain on individuals. Increased rates of obesity threaten public health and pose financial stresses on the US health system.2,3 Recommended treatments for patients with obesity, including bariatric surgery, pharmacotherapy, and lifestyle modification through behavioral interventions, have shown significant improvement in weight loss and obesity-associated health outcomes. 4
Behavioral interventions have few adverse effects and are relatively low cost and thus are an optimal first-line therapy for weight loss. 4 While curricula, behavioral techniques, frequency, and duration of programs vary widely, behavioral interventions typically focus on changing dietary intake and increasing physical activity. When added to behavioral weight loss programs, dietary tracking and weight self-monitoring facilitate self-regulation and help individuals lose weight.5,6
Adherence to these behaviors tends to decline over the course of behavioral interventions. Individuals who successfully lose weight regain approximately 30% of initial weight lost in the following 12 months.4,7,8 Identifying predictors of adherence to these behaviors may help identify strategies to increase adherence. One strategy to increase behavioral adherence is delivering small monetary incentives to provide reinforcement and aid in habit formation. Incentives have been shown to impact various health outcomes including smoking cessation, contraception utilization, and weight loss9-11 Previous work in the context of weight loss has incentivized a variety goals including amount of weight lost and behaviors such as physical activity.12-16 Additionally, different incentive types, including lotteries, monetary contracts with deposits, and direct incentives, have been tested.17-19 Many previous studies were limited to incentivizing participants only after turning in electronic or paper logs, most often at the end of the intervention period. These methods required participants to travel to the study team for in-person visits to deliver the logs and receive payment, thus increasing burden on participants and delaying receipt of incentive relative to the desired behavior. With the advent of accessible remote monitoring technology such as cellular-connected body weight scales and smartphone applications for food logging, data can now be collected from afar and in real time from participants in their everyday environment. Thus, it is now possible for incentives to be provided closer in time to when behaviors occur, allowing for quicker feedback and reward delivery. The few studies that have used these methods have shown that incentivizing weight loss behaviors can lead to short-term weight loss.13,18,20,21 These studies, though, have incentivized only weight loss outcomes or a combination of behaviors. Thus there remains a gap in the literature around the effectiveness of incentivizing a single behavior such as dietary tracking or incentivizing weight loss. It is not yet known if weekly incentives, given in response to real-time data collection, affect adherence to behaviors that can facilitate weight loss, including dietary tracking, monitoring weight, and attending intervention sessions.
In the Log2Lose pilot trial, participants were offered thirteen group classes and were randomized to receive (or not) weekly incentives for dietary tracking and/or weight loss. This work examined the relationship between incentives and disengagement of behavior directly incentivized (dietary self-monitoring), indirectly incentivized (weight self-monitoring, which was necessary to incentivize weight loss), and not incentivized (class attendance).
Methods
Design
The Log2Lose pilot trial was designed to establish the feasibility of delivering weekly financial incentives for weekly dietary tracking and weight loss. Details were previously published. 22 Briefly, community-dwelling adults (N = 96) with obesity enrolled in a 24-week weight loss program delivered via in-person group sessions every other week. 23 The sessions lasted up to 1.5 hours each and provided participants with information and behavioral skills for dietary management and exercise necessary to promote weight loss.
The trial was delivered in three cohorts of 31 to 34 participants. Within each cohort, participants were randomized 1:1 to one of four arms, three of which involved incentives and a control group with no incentives. The three incentive arms were: receive financial incentives for both dietary self-monitoring and weekly weight loss (group A), financial incentives for dietary self-monitoring only (group B), and financial incentives for weekly weight loss only (group C). The maximum incentive amount was the same across each arm. Incentive amounts varied each week between $0 and $30 in cohorts 1 and 2 and between $2 and $30 for cohort 3 and were delivered on an intermittent reward schedule. Participants were not informed of the schedule and thus did not know ahead of time how much they could earn that week. Group D in this analysis represents the control group that received no incentives.
At the baseline visit, participants were provided with a debit card and a BodyTrace™ cellular scale that transmitted weights to the study team in real time. They also signed up for MyFitnessPal accounts for dietary tracking. A calorie budget was calculated for each person using the Mifflin St. Jeor formula and provided at the beginning of the trial. 24 All participants, regardless of incentive arm, were instructed to weigh themselves at least twice per week and to log everything they ate and drank in the MyFitnessPal application at least five days per week, one of which should be a weekend day.
In order to receive the weekly financial incentives for dietary tracking, people assigned male at birth were required to log at least 1200 kcals/day and females at least 1000 kcals/day, both for 5 days (including 1 weekend day). These values are below the calorie budget calculated for each person and thus required that participants record much, but not all, of what they ate during the day. At the beginning of each week, participants received a text message stating whether they logged enough the previous week to receive the incentive as well as how much money they would be receiving that week. This money was deposited onto a debit card. If participants did not log enough calories on enough days, they received a text message stating how much money they could have earned for that week and encouragement to continue logging the next week for a chance to earn an incentive.
To receive the weekly incentive for weight loss, participants were required to weigh at least twice per week to calculate weight change, and the last weight of the week must have been lower than the first. Their text message detailed if they had lost enough weight to receive the incentive and how much. If participants did not lose weight, they received a text message detailing that and how much they could have earned, with encouragement to keep trying to earn an incentive the next week. If participants did not weigh at least twice to calculate weight change, they received a text message detailing that and how much they could have earned if they had weighed and lost weight, along with encouragement to try again next week.
Sample
Full eligibility criteria have been reported. 22 With institutional review board approval, participants were adults who provided informed consent, aged 18-70 years, with a BMI of at least 30 kg/m2 who were in stable health and who desired to lose weight. Additionally, because the intervention required the use of the dietary tracking application, participants were required to own a smart-phone with data and texting plan. An upper weight limit of 380 lb. was necessary due to the weight limit on the cellular-connected scales.
Measures
Dietary self-monitoring
Caloric intake entered in MyFitnessPal was transmitted to a study-developed mobile health platform through the cellular network. 23 Each week, participants were classified as either adherent or nonadherent depending on whether they met self-monitoring criteria. Nonadherence for self-monitoring was defined as the second week with fewer than 5 days of meeting the calorie threshold including a weekend day.
Weight self-monitoring
Self-weighing throughout the trial was captured in real-time from cellular-connected scales (Model BT004, BodyTrace™, New York, NY). All weights collected along with a corresponding date and timestamp were captured in the study platform. Because two weights were required to calculate weight change each week and all groups were instructed to weigh at least twice per week, nonadherence to weight self-monitoring was defined as the second of two consecutive weeks when fewer than two weights were transmitted.
Class attendance
Attendance at biweekly classes was recorded during each session. To correspond to the 2-week period defining nonadherence to self-monitoring, nonadherence was defined as the first missed class.
Demographic characteristics
Age, sex assigned at birth, race, ethnicity, education level, income level, and employment status were collected at the baseline visit via self-report.
Analysis
Data cleaning involved removing implausible and excessive weights (ie, more than one weight transmitted in a day). First, any weight differing by greater than 10% from the prior weight in a single day was removed. Second, weights were invalidated if they differed by more than 20% of the baseline weight. These steps helped to ensure the weights collected were from the participant and not someone else in the household. Finally, if more than one weight was provided in a day, the first weight of the day was used. No cleaning algorithms were applied to the dietary or class attendance data.
Analyses were performed using SAS/STAT® 15.1 (SAS Institute, Inc., Cary, NC) and R (version 4.2.1) statistical software.25,26 Descriptive statistics and visualizations of nonadherence were produced. Figures generated in R show nonadherence over time for each participant by incentive group. Separate analyses for weight and dietary self-monitoring and class attendance were conducted to examine nonadherence in each of the different treatment groups.
Survival analysis was used to compare the patterns of time-until-nonadherence over the course of the study. Differences across treatment groups for each of the behavioral targets (ie, dietary self-monitoring, weight self-monitoring, or attendance) were examined. To test the effect of incentives for dietary self-monitoring on adherence to dietary tracking, the two groups receiving incentives for tracking (groups A and B), were combined and compared to the two groups not receiving this incentive (groups C and D). To test whether incentives for weight loss indirectly affected adherence to weight self-monitoring, the two groups receiving incentives for weight loss (groups A and C) were combined and compared to the two groups not receiving this incentive (groups B and D). Finally, differences across the four incentive groups in class attendance were examined as a test of whether incentives for dietary tracking and/or weight loss affected a non-incentivized behavior. A log-rank test was used to test for statistical significance.
Because the goal was to establish feasibility and not efficacy, we did not perform a power analysis. We aimed to enroll 8 participants per cell in each cohort to enable group cohesion.
Results
Baseline Characteristics Stratified by Incentive Group and Overall.
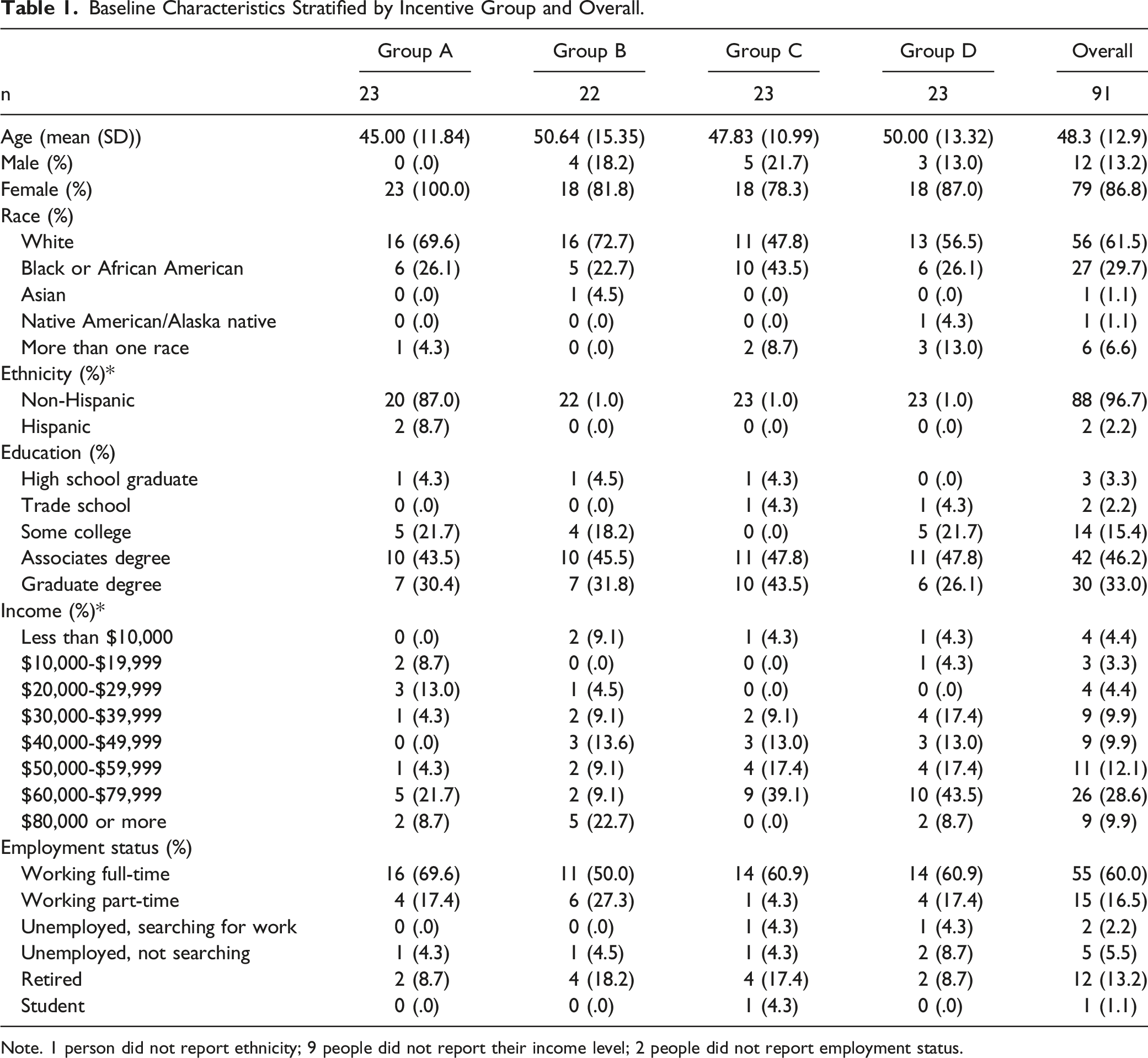
Note. 1 person did not report ethnicity; 9 people did not report their income level; 2 people did not report employment status.
Nonadherence to dietary tracking is displayed in Figure 1A-D. The average time until the first nonadherent week was 15.8 weeks (SE: 1.2) for groups incentivized for dietary self-monitoring (A and B) compared to 5.9 weeks (SE: .8) in the groups not incentivized for doing so (C and D). The log-rank test of the combined groups (comparing A and B to C and D) was statistically significant, χ2(1) = 27.21, P < .01. Although the log-rank test comparing all four groups was significant, χ2(3) = 27.33, P < .01, the test comparing the combined incentives group (A) to incentives for dietary self-monitoring alone (B) was not, χ2(1) = .01, P = .93. A-D: Nonadherence to dietary self-monitoring over the 24-week intervention by treatment group*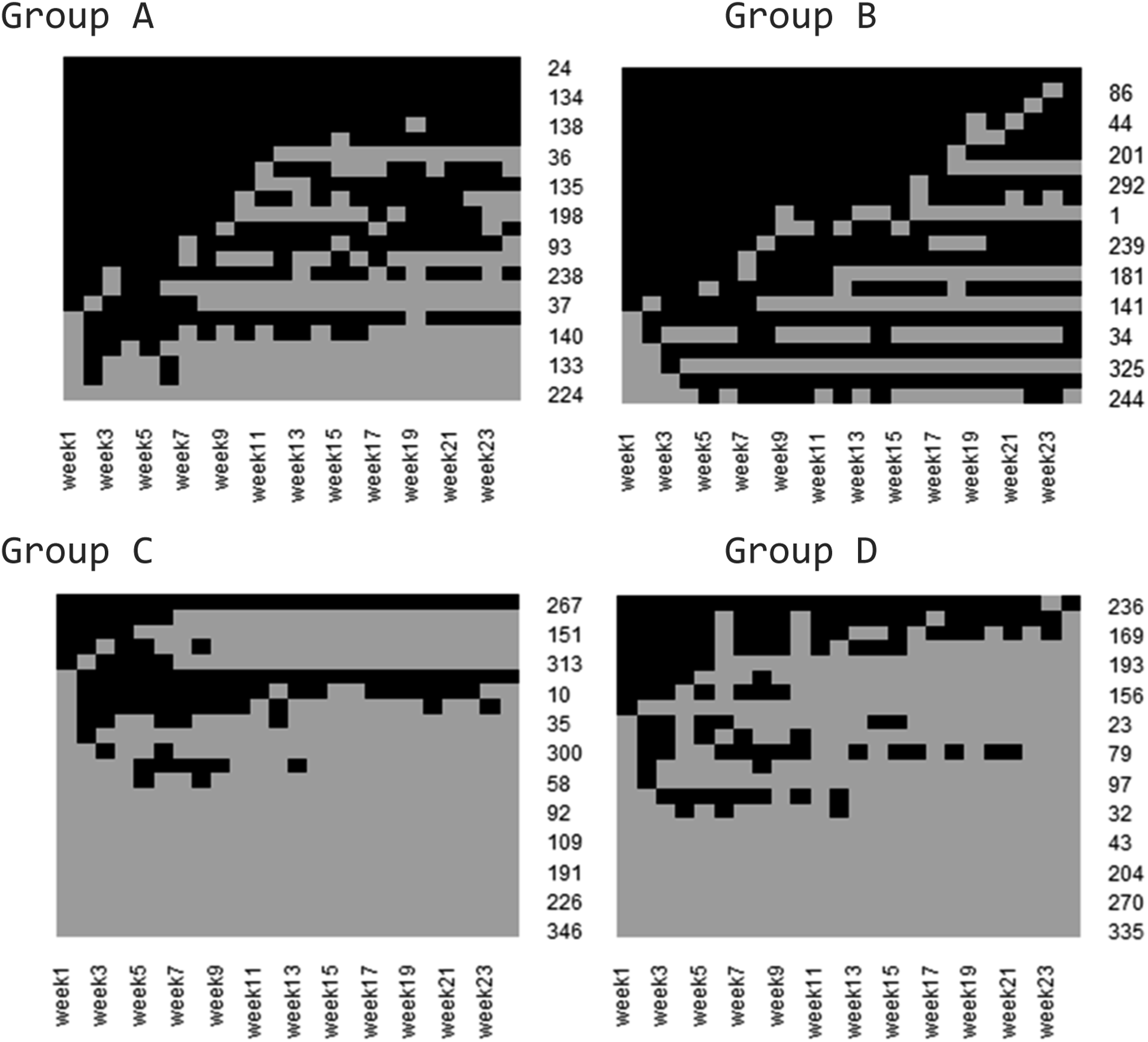
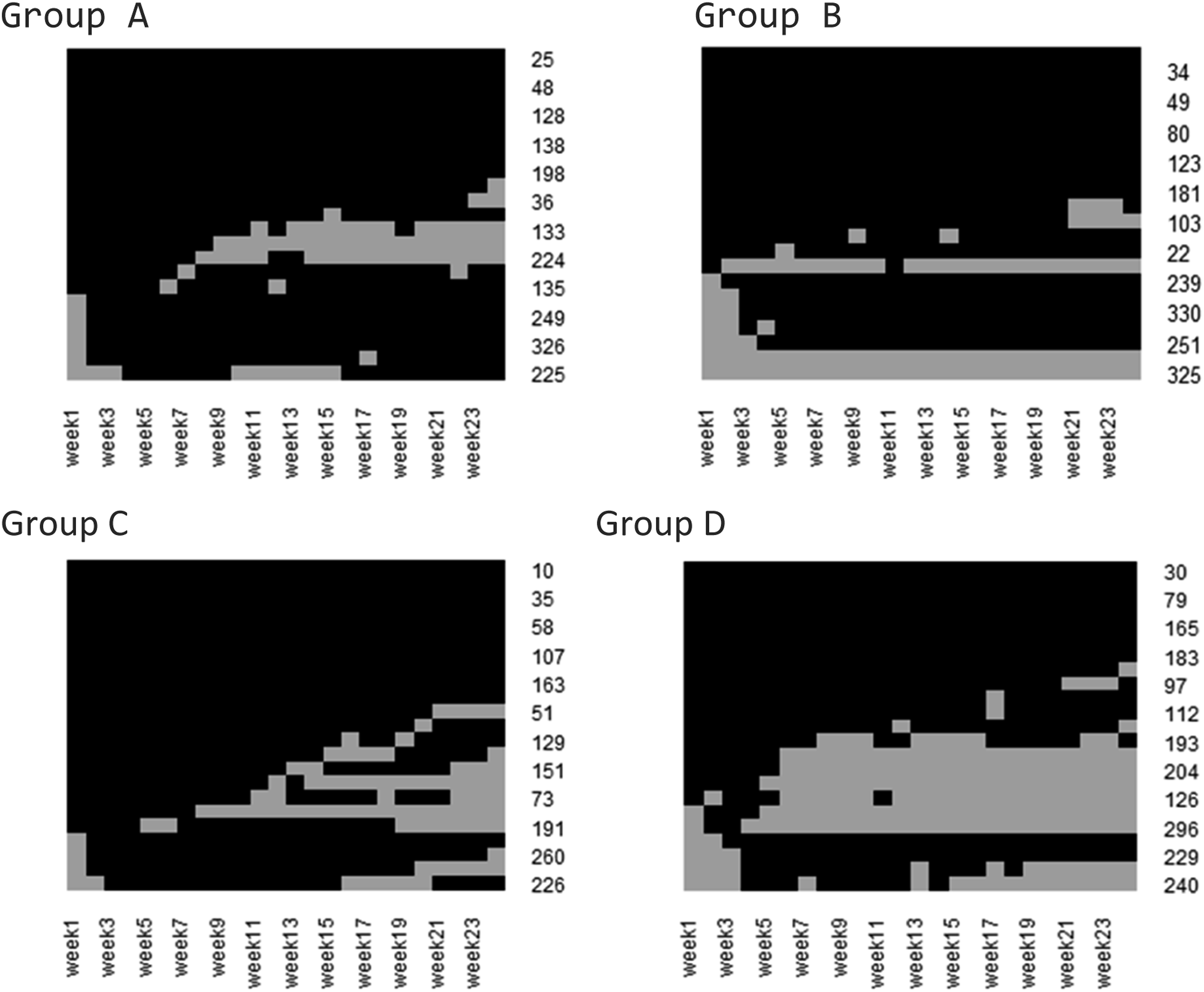
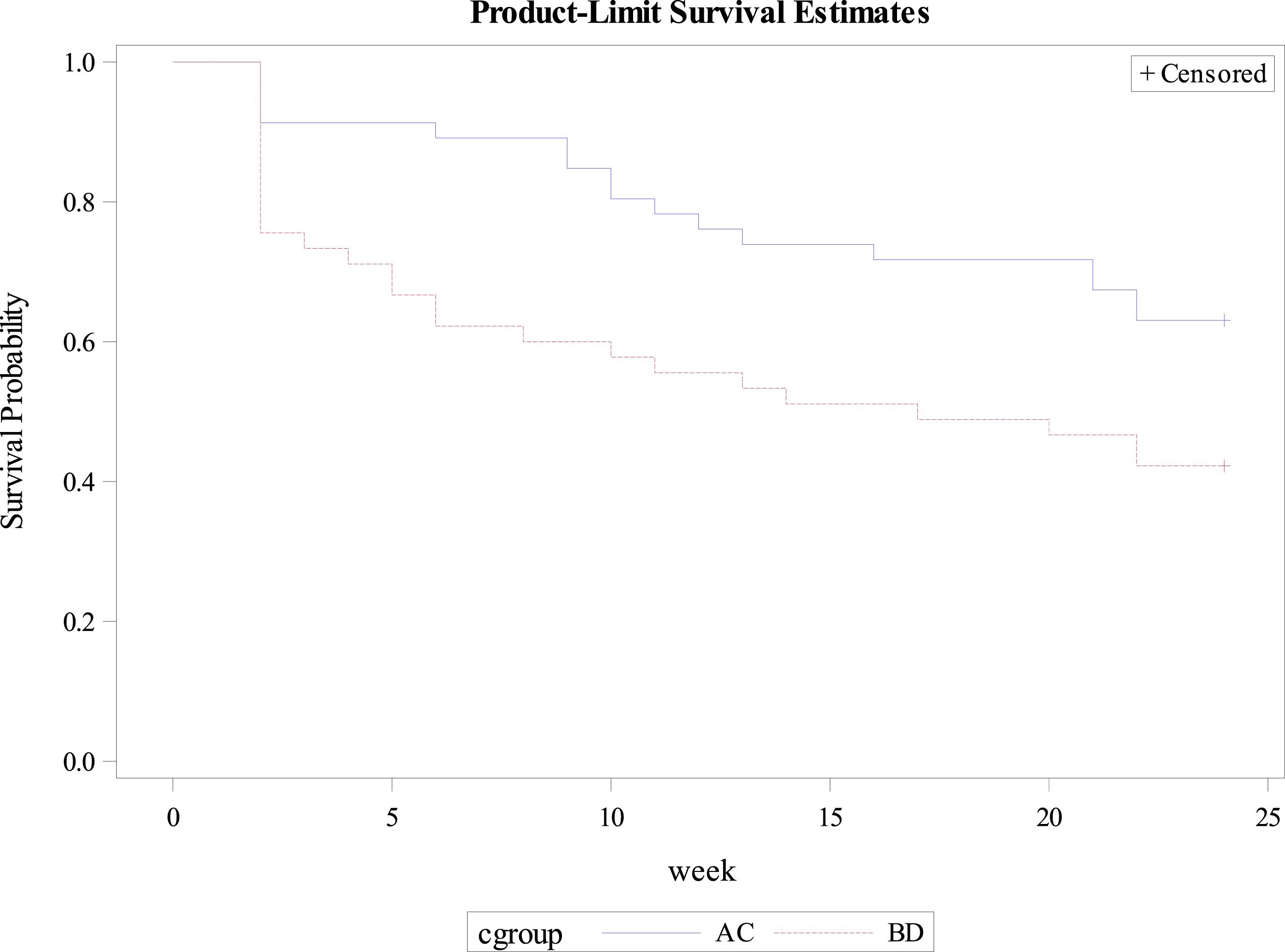
Adherence to self-weighing is displayed in Figure 2A-D. The average time until the first nonadherent week of self-weighing was 18.0 weeks (SE: 1.02) for the groups incentivized for weight loss (A and C) compared to 13.5 weeks (SE: 1.3) in the groups not incentivized for weight loss (B and D). The log-rank test of the combined groups (comparing A and C to B and D) was statistically significant, χ2(1) = 5.09, P = .02. The log-rank test comparing all four groups was not significant, χ2(3) = 7.29, P = .06, nor was the test comparing the combined incentive group (A) to the group incentivized for weight loss alone (C), χ2(1) = .76, P = .38. Kaplan-Meier survival curves for dietary self-monitoring.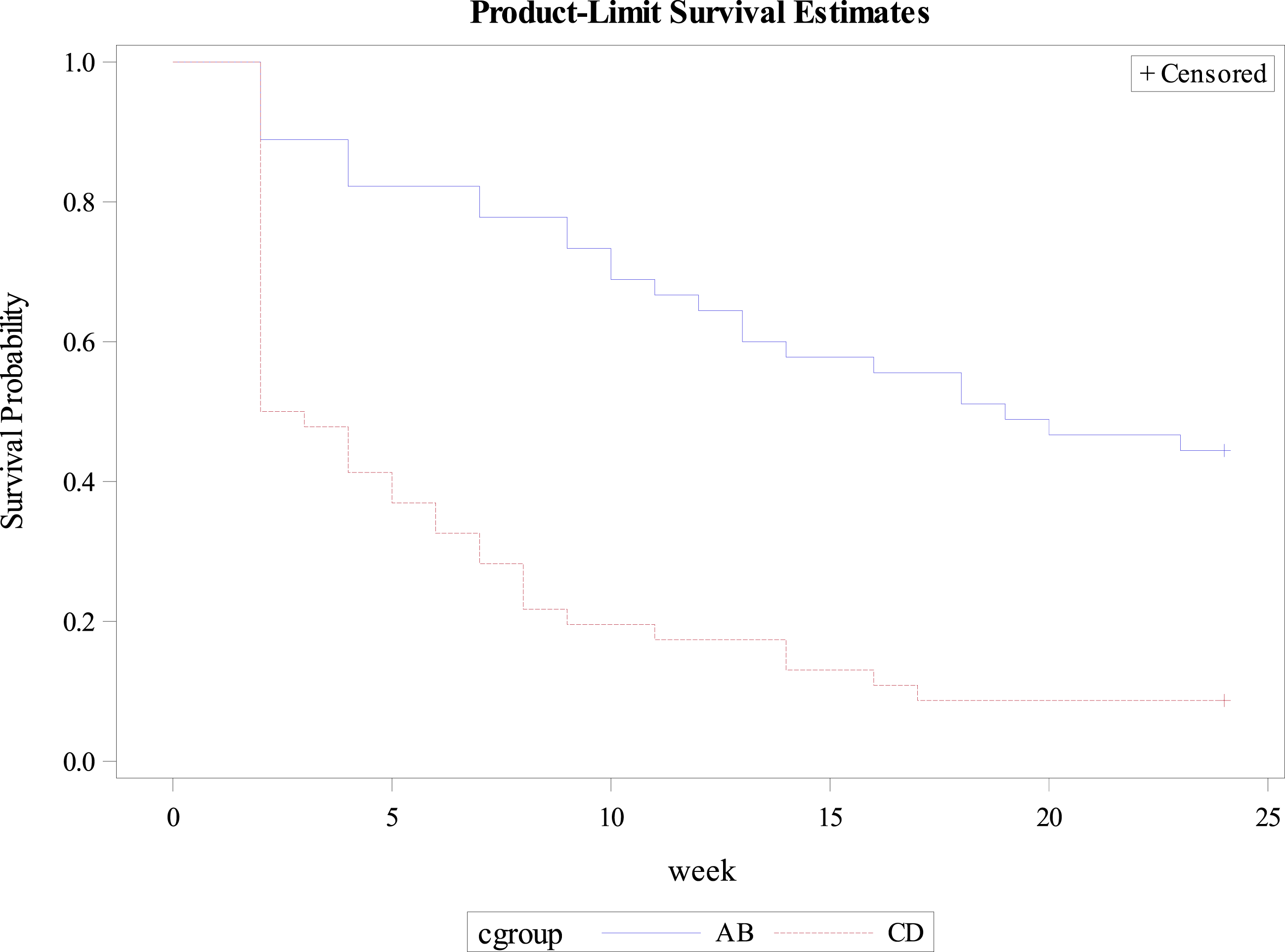
Analyses of class attendance (Figure 3A–D) showed that group A had an average of 8.0 weeks (SE: 1.1) of attendance before the first missed class; group B an average of 8.2 weeks (SE: 1.2); group C an average of 6.4 weeks (SE: .8); and group D an average of 9.3 weeks (SE: 1.2). The associated log-rank test for differences across the four groups did not reach statistical significance, χ2(3) = 1.35, P = .72 (Figure 4).
Discussion
Nonadherence to dietary and weight self-monitoring and class attendance was examined within the context of an intervention testing incentives for dietary self-monitoring, weight loss, a combination of the two, or neither. The time-to-event analyses provide a unique understanding of behavioral adherence when incentives are directly or indirectly related to the behavior of interest. These analyses offer information about when individuals had their first episode of nonadherence instead of reporting total adherence across the intervention period. This provides insight into how long individuals are adherent and how different incentives might prolong this adherence.
Findings suggest that incentives led to adherence to behaviors that were directly and indirectly incentivized (ie, dietary tracking and weight loss) but not a behavior that was not incentivized (ie, class attendance). Participants directly incentivized (Groups A and B) for dietary self-monitoring were, on average, adherent for 10 weeks longer than those in groups that did not receive incentives for this behavior. This finding is both statistically significant and clinically important given that dietary tracking, while effective for weight loss, is a behavior for which adherence and corresponding weight loss often decline quickly after initiation. This finding potentially supports the use of variable incentive schedules in promoting behavioral adherence.
Incentivizing weight loss appeared to improve adherence to self-weighing twice per week. Although the incentive was for weight loss, text messages still provided feedback that participants missed out on an incentive if they did not weigh at least twice the previous week. The self-weighing literature has typically explored weight self-monitoring daily and weekly.27,28 This study required weighing two times per week in order to calculate weight change. An alternative method for delivering incentives in the future is requiring once weekly weighing and incentivizing based on the difference from one week to the next instead of within a week. This would allow for more time between weight assessments, which could allow more people to meet criteria for an incentive. Our design did not allow us to disentangle the effect of incentivizing weight self-monitoring vs weight loss. Future research could examine which strategy is more effective for improving weight loss.
Of note, burden of the behavior should be considered when designing incentives. For example, participants who did not receive incentives for weight loss were still adherent to self-weighing out to 13 weeks on average, while those not incentivized for dietary tracking were adherent out to 5 weeks. This may be due to the relative ease of weight monitoring, which could be done on two separate days over an entire week, compared to dietary monitoring, which required individuals to track multiple foods potentially several times daily on five different days. Future work should consider behavioral burden and response to better optimize incentives for individual participants.
Finally, we compared class attendance across the groups to provide insight as to whether incentivizing certain behaviors, like self-monitoring, may encourage other behaviors associated with successful weight loss. The weight loss classes offered education and behavioral skills training to promote sustained weight loss. The dietitians leading the classes could also identify unsustainable weight loss behaviors and provide support for healthy weight loss through discussion. Despite these benefits, individuals could have received incentives for weight loss and dietary self-monitoring even without attending class. Thus, the success of these behaviors was not confounded with class attendance, a strength of this work. Perhaps unsurprisingly, no differences were seen across the groups, suggesting that incentives should be applied directly to the behavior of interest.
Our findings can be interpreted in of light findings from other studies examining the impact of financial incentives on weight loss and/or related behaviors such as session attendance. These studies differ in the populations targeted, behaviors and outcomes incentivized, and outcomes assessed. Ladapo et al. randomized 668 participants from low-income neighborhoods participating in a commercial weight loss program to receive incentives for achieving behavioral goals (to include dietary, physical activity and weight self-monitoring as well as attendance), weight loss, or a no-incentive control group. 29 They found that both incentive structures led to a greater proportion of people achieving at least 5% weight loss, and to greater mean weight loss, at 6 months compared to control. The impact on self-monitoring was not reported. Moreover, the behavioral goal group was incentivized for many different behavioral goals rather than isolating the impact on any one of them. Ratliff et al. randomized 30 participants with serious mental illness receiving antipsychotic drug therapy and participating in a lifestyle management program to receive incentives for attendance at weight loss group sessions, for purchasing healthy food items, for weight loss, or no incentives. 30 Weight loss and session attendance were both measured but did not show significant between-group differences, perhaps owing to the small sample size. VanEpps et al. randomized 703 people with prediabetes receiving Medicaid and participating in the Diabetes Prevention Program to receive incentives for session attendance, weight loss, both, or neither. 31 They found that session attendance was higher among participants rewarded for session attendance than people who received incentives for both attendance and weight loss or no incentives, but equivalent to participants incentivized for weight loss. Our study adds to this literature by using a rigorous design that isolates the impact of incentives for a single behavior (namely, dietary self-monitoring) vs weight loss and by evaluating the impact of financial incentives on a behavior that occurs outside of the group weight loss setting (namely, logging) as well as a behavior that is incentivized indirectly (namely, self-weighing via incentives for weight loss). Consistent with VanEpps, and with expectations from psychological theory, we found that incentivizes increase incentivized behaviors but not non-incentivized behaviors.
This work has several limitations. This trial included participants who identified as non-Hispanic, White, and female. Participants were required to own a smartphone, further limiting generalizability of our findings. However, there is some evidence to suggest that 85% of adults in the US now own a smartphone.
32
As this trial was designed to assess feasibility and acceptability of the trial procedures, it could be underpowered for post-hoc analyses such as those reported herein. Additionally, part of the pilot trial included testing the feasibility of the incentive structure. The resulting incentive structures were not uniform over the cohorts, so that in cohort 3 the lower limit of incentives was 2$ compared to $0 in cohorts 1 and 2. This may have slightly impacted results for individuals who may have perceived a difference between $0 and $2 and as a result have been motivated differently. Yet, qualitative interviews with a subset of these participants suggested that these lower bounds were perceived similarly. Finally, we did not systematically collect reasons for nonadherence across the trial. Participants received text reminders about the date and time of class the day prior. While our study highlights the benefit of incentivizing self-monitoring behaviors to promote weight loss, further work is needed about how incentives affect behaviors for longer periods into weight loss maintenance and whether behaviors continue after incentives end. A better understanding of whether incentivizing weight loss behaviors influences other weight loss behaviors is also needed. Future work will extend findings to weight loss outcomes in an adequately powered trial. A-D: Nonadherence to self-weighing over the 24-week intervention by treatment group* Kaplan-Meier survival curves for self-weighing.So What?
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a grant awarded to Drs. Voils and Shaw by the National Heart, Lung, and Blood Institute (NHLBI; 1R34HL125669). Effort on this study or manuscript was also made possible by a Research Career Scientist award (RCS 14-443) to Dr. Voils from the Department of Veterans Affairs Health Services Research & Development service.
Informed Consent
The contents of this manuscript do not represent the views of the Department of Veterans Affairs or the United States Government.