
Abstract
Purpose
To redevelop and improve Transtheoretical Model (TTM) exercise measures for Black and Hispanic/Latinx adults. The redeveloped scales will address barriers to exercise potentially relevant to populations of color in the United States (US).
Design
Cross-sectional, split-half measure development.
Setting
Online survey in the US.
Subjects
450 Black and/or Hispanic/Latinx adults.
Measures
Demographics, exercise engagement (IPAQ-SF), stage of change (SOC), decisional balance (DCBL), self-efficacy (SE), and barriers to exercise.
Analysis
Split-half exploratory (EFA) and confirmatory factor analyses (CFA) were executed to establish measurement structure and fit, followed by multivariate analyses to assess constructs by SOC.
Results
EFA/CFA for DCBL revealed three factors (α = .85, .70, .75) which represented Pros of exercise, Cons of exercise related to time and safety, and Cons of exercise related to physical or emotional discomfort. Model fit was adequate (CFI = .89). For SE, two factors (α = .85, .77) resulted with good model fit (CFI = .91). These factors reflected self-efficacy to exercise when confronted with generally challenging situations, and self-efficacy to exercise when specifically experiencing affective difficulties, such as depression or anxiety. Lastly, a novel Barriers measure resulted in three factors (α = .82, .77, .76), representing barriers encountered due to family responsibilities, work obligations, and health challenges, with good model fit (CFI = .95). Shifts in the core TTM constructs by SOC largely mapped onto the theoretical trends expected under the TTM.
Conclusion
This study produced systematically developed TTM exercise measures for Black and Hispanic/Latinx adults in the US that address and incorporate important barriers to exercise. This research represents an important step forward in broadening the inclusion of diverse populations to TTM measure development processes and may lead to a better understanding of relevant factors impeding exercise engagement in the US.
Introduction
Despite extensive and abundant scientific literature supporting the various benefits of exercise on human health and well-being, research has revealed that roughly 77% of American adults do not engage in the recommended amount of weekly exercise to reap such benefits. 1 This, in combination with poor nutrition, has contributed to increasing rates of illness, 2 obesity, 3 and reliance on pharmacological remedies. 4
Fortunately, research efforts aimed at increasing exercise engagement utilizing the Transtheoretical Model (TTM) have shown promising results.5-9 The TTM is a framework for assessing and guiding intentional behavior change. At the core of the TTM is the assessment of an individual’s Stage of Change (SOC), or their readiness to change a health behavior. 10 SOC is assessed categorically, with individuals being classified into one of five stages: precontemplation (no intention to change within the next 6 months), contemplation (intention to change within the next 6 months), preparation (intention to change within the next 30 days), action (successfully enacted change for 30 days), and maintenance (successfully enacted change for 6 months or more). 10 The theory posits that movement through the stages is initiated by shifts in three core constructs: decisional balance (DCBL), self-efficacy (SE), and processes of change (POC). DCBL considers how important the pros and cons of a behavior change are in one’s decision to engage in or abstain from the given behavior. SE assesses an individual’s confidence in their ability to complete a health behavior change under challenging and often relapse-triggering circumstances. Lastly, POC reflect overt and covert thoughts, activities, and behaviors that people engage in as they enact health behavior modifications. These constructs not only provide a basis for characterizing and assessing an individual’s preparedness for behavior change, but also establish the foundation of TTM-tailored interventions, which aim to accelerate progression through the change process. 11
Although initial studies applying the TTM to exercise show promise, generalizability of TTM exercise instruments appears limited. In a review of studies applying the TTM to exercise, results showed that most study populations have been primarily White, middle-class, and female. 6 This is an important limitation, as specialty exercise interventions may be indicated for ethnically diverse and low-income populations given significant health disparities that exist in the US. 12 For example, tailored exercise interventions may assist with closing current gaps in rates of obesity, 13 diabetes, 14 and overall inactivity. 15 Insufficient population diversity in these existing studies might explain the growing body of research demonstrating that certain TTM exercise constructs, as they are currently measured, do not function as expected when used with understudied populations.
For example, the two most widely used decisional balance instruments appear to be the 16-item 16 and 10-item 17 decisional balance questionnaires. Although these scales have demonstrated strong validity and reliability, they appear to yield limited generalizability beyond their established samples. For example, the 16-item decisional balance questionnaire was constructed from a sample that was 95% White and, within which, 70% of the sample worked in white-collar professions. 16 Meanwhile, the 10-item decisional balance questionnaire did not address race in its validation study. However, the census data in the year and region it was completed reveal that the region's population was over 80% White, 18 therefore, it is likely that the sample assessed for this study was also primarily White. As a result of these homogenous samples, the literature has revealed problems or unexpected results with the Cons scale, which measures how important various negative consequences of exercise (e.g., physical discomfort) are to one’s decision to regularly exercise, leading to uncertainty about the validity of these scales. Specifically, unexpected results occurred when these scales were used with a Black population, 19 both diverse 20 and White 21 older adults, low-income populations, 22 and adults with physical disability, 23 severe mental illness, 24 and HIV. 25
Based on these numerous research findings,19-25 it appears that the current Cons scales fail to comprehensively assess the negative consequences of exercise in more diverse populations. This suggests that item content relevant to certain populations’ decision to exercise is not being accurately captured in the present TTM exercise scales. In fact, numerous studies have outlined many barriers to exercise among Black and/or Hispanic/Latinx US populations that are not addressed in the current TTM exercise measures.26-31 Importantly, many barriers to regular exercise noted in the literature among these populations are secondary to economic insecurity, and therefore are not unique to people of color. However, Black and/or Hispanic/Latinx populations do experience significantly greater levels of economic insecurity compared to White populations in the US, 32 and therefore may disproportionately encounter exercise barriers related to income, such as limited gym access or community safety issues. Other barriers stem from the intersectionality of gender and different cultural values, such as Latina women citing spousal and other familial caregiving duties as a traditional role responsibility and major barrier to exercise, 27 or Black men referencing pressure to prioritize the “provider” role above their own health status. 31 Various cultural values, such as social norms or practices, may also interfere with exercise engagement and should be considered. Therefore, while income inequality plays a significant role in the presence or absence of various exercise barriers, additional barriers may arise for people of color and the intersectionality of different identities and lived experiences, and these must be comprehensively considered in the early phases of measure development.
These barriers may be relevant factors guiding one’s readiness or ability to exercise regularly, and behavior change researchers have indeed proposed a need for modified scales that account for possible environmental (e.g., neighborhood qualities, access to fitness centers) and personal (e.g., caregiving demands, health concerns) barriers to exercise.19,22 They note that adapted scales may improve the predictive utility of the TTM constructs to SOC 25 and apply more broadly to the lived experiences of people of color. Importantly, while it appears essential barrier content is lacking, it is unclear if this material fits psychometrically into existing TTM constructs (e.g., SE, DCBL Cons), or if it is best measured independently as a novel Barriers construct.
Black and/or Hispanic/Latinx populations are more likely to be physically inactive than any other population in the United States (US),
15
yet they have been largely excluded from prior TTM measure development procedures. The purpose of this research is to create novel TTM exercise scales developed on an entirely Black and/or Hispanic/Latinx adult sample, which may expand the inclusivity and relevance of TTM exercise scale items. As a result, this work may aid in addressing potential barriers to exercise encountered by populations of color. Further, this research aims to incorporate novel barrier items into all construct item pools, when applicable, to ensure comprehensive inclusion of this content across constructs and identify the appropriate location for this content under the TTM framework. This study will address the following hypotheses: 1. Measure development will yield updated SE and DCBL scales that demonstrate factor structures similar to previous TTM exercise measures with good model fit. The barriers construct is not designed with any a priori factor structure. 2. Constructs will change by SOC as expected under the strong and weak principles.
11
Specifically, stage progression will be associated with a 1 standard deviation (SD) increase in the importance of Pros, a .5 SD decrease in the importance of Cons, and an approximately .8 SD increase in SE from Precontemplation to Action. Additionally, individuals in later stages (Action, Maintenance) will endorse the importance of Pros significantly higher and the importance of Cons significantly lower than those in earlier stages (Precontemplation, Contemplation, Preparation). Based on prior work,
33
it is anticipated that the perceptions of barriers will decrease significantly from Contemplation to Action.
Method
Cognitive Interviews
Prior to survey dissemination, five adults who identified as Black (n = 2) or Hispanic/Latinx (n = 3) were recruited from a social media platform to participate in cognitive interviewing. Participants were asked to provide feedback about the understandability and clarity of instructions and items and were encouraged to suggest any additional scale items if they felt important content was missing. Participant feedback was used to improve survey instructions, fix unclear item wording, and add novel and relevant barrier items to the item pool prior to survey dissemination to the larger sample.
Participant Recruitment and Survey Administration
Survey construction and data collection were completed in Qualtrics (www.qualtrics.com), while participants were recruited from the data collection platform, Prolific (www.prolific.co). Prolific is an international data collection platform that recruits participants by word-of-mouth, collects comprehensive pre-screen information, and has several effective systems in place to prevent fraudulent accounts (www.prolific.co). The study was advertised only to individuals living in the US, aged 18+, and who listed their race as Black and/or their ethnicity as Hispanic/Latinx. Sampling was designed to yield representation for each SOC category such that the full range of readiness of exercise was represented.
Measures
Sources for item generation across all constructs included existing exercise TTM measures, existing barriers to exercise scales,34,35 qualitative literature investigating barriers to exercise within Black and/or Hispanic/Latinx populations, and cognitive interviewing feedback. To determine the need for an independent Barriers scale, barriers to exercise were assessed as a scale of their own. However, specific items were also reworded and adapted to reflect the Cons (negative consequences of exercise) and SE (situations that may challenge one’s confidence to exercise) constructs when applicable. For example, the barrier item “I do not have a safe place in my neighborhood or community to exercise” was reworded to “Getting exercise would put my safety at risk” to reflect a con of exercise. It was further adapted for SE by assessing one’s confidence in their ability to exercise if they “do not have a safe place to exercise.” Three instructed response items were used as attention checks throughout the survey. 36
Demographics
A demographics questionnaire assessed participant age, gender identity, race, ethnicity, employment status, height (feet/inches) and weight (pounds). Participants were also asked about educational attainment and subjective perspective of standing within the US social-economic power hierarchy (i.e., poor, working class, middle class, affluent) to serve as a proxy for income. 37
Exercise Behavior
Current exercise engagement was measured using the International Physical Activity Questionnaire- Short Form (IPAQ-SF). 38 The IPAQ-SF is a self-report questionnaire that assesses recent physical activity. Participants were given a description of each category of exercise (vigorous, moderate, and walking) and asked on how many days in the past week and for how long they engaged in that type of activity. Previous literature has established that the IPAQ-SF has strong reliability and validity.38,39
Stage of Change
Exercise SOC was assessed using an established staging algorithm. All participants were given the definition of regular exercise according to the 2018 U.S. Department of Health and Human Services 40 physical activity guidelines for Americans and were asked how ready they were to engage in regular exercise. Participants were placed into Precontemplation (no intention to engage in the next 6 months), Contemplation (intention to engage in the next 6 months), Preparation (intention to engage in the next 30 days), Action (engaged for less than 6 months), or Maintenance (engaged for more than 6 months). The reliability and validity of this staging algorithm has been previously established.41,42
Self-Efficacy
Exercise SE was assessed using a 35-item questionnaire developed from two existing SE scales17,43 and other aforementioned sources. Relevant barrier items were reworded and adapted to assess one’s confidence in their ability to engage in regular exercise despite encountering a given barrier. Participants were given a list of situations in which some people might choose not to exercise when something gets in the way (e.g., I am under a lot of stress) and were asked to rate how confident they were that they would participate in regular exercise in face of such challenges from “Not at all confident” (1) to “Extremely confident” (5).
Decisional Balance
Exercise DCBL was assessed using a 33-item questionnaire incorporating items from two DCBL scales,17,44 as well as barrier scales and qualitative literature. As with the SE scale, barrier content was reworded and adapted to reflect negative consequences of exercise to be consistent with the Cons construct assessing negative outcomes of regular exercise, rather than elements that prevent someone from performing the behavior. Participants were asked to rate how important each item was in their decision to exercise from “Not Important” (1) to “Extremely Important” (5). The pros of exercise included positive consequences of exercise (e.g., “I would sleep better”) and the cons reflected negative consequences of exercise (e.g., “Exercising prevents me from spending time with my friends”).
Barriers
A 21-item questionnaire based on existing barriers scales,34,35 cognitive interviews, and the qualitative literature was developed. Participants were asked to rate to what extent they perceived the listed barriers to inhibit them from exercising regularly from “Not at all” (1) to “Extremely” (5) inhibiting (e.g., “I have too many social and family responsibilities”).
Statistical Analyses
A sequential approach to measurement development was used. 45 Participants were randomly split into two groups for exploratory (n 1 = 221) and confirmatory (n 2 = 229) analyses. An exploratory factor analysis (EFA) was conducted on n 1 using principal components analysis with varimax rotation on the item intercorrelation matrices using SPSS. Inclusivity of items took priority to scale brevity in this process, as the goal was to ensure that breadth of construct was adequately addressed within these populations. Next, a confirmatory factor analysis (CFA) was conducted using R on n 2 to confirm the structure of the EFA results. Three different fit indices were examined, including the comparative fit index (CFI), the root mean square error of approximation (RMSEA), and the standardized root mean squared residual (SRMR). A CFI of .95 or greater is considered an acceptable fit, while a value of .08 for SRMR and a value close to .06 for RMSEA are considered acceptable values indicating good fit. 46
Next, a correlation matrix between scales was conducted. Lastly, external validation was assessed using a series of ANOVAs to examine the constructs by stage to evaluate if the expected SOC patterns were sustained, 47 as well as to assess if self-reported exercise, as measured by the IPAQ-SF, changed as expected across SOC.
Results
Participants
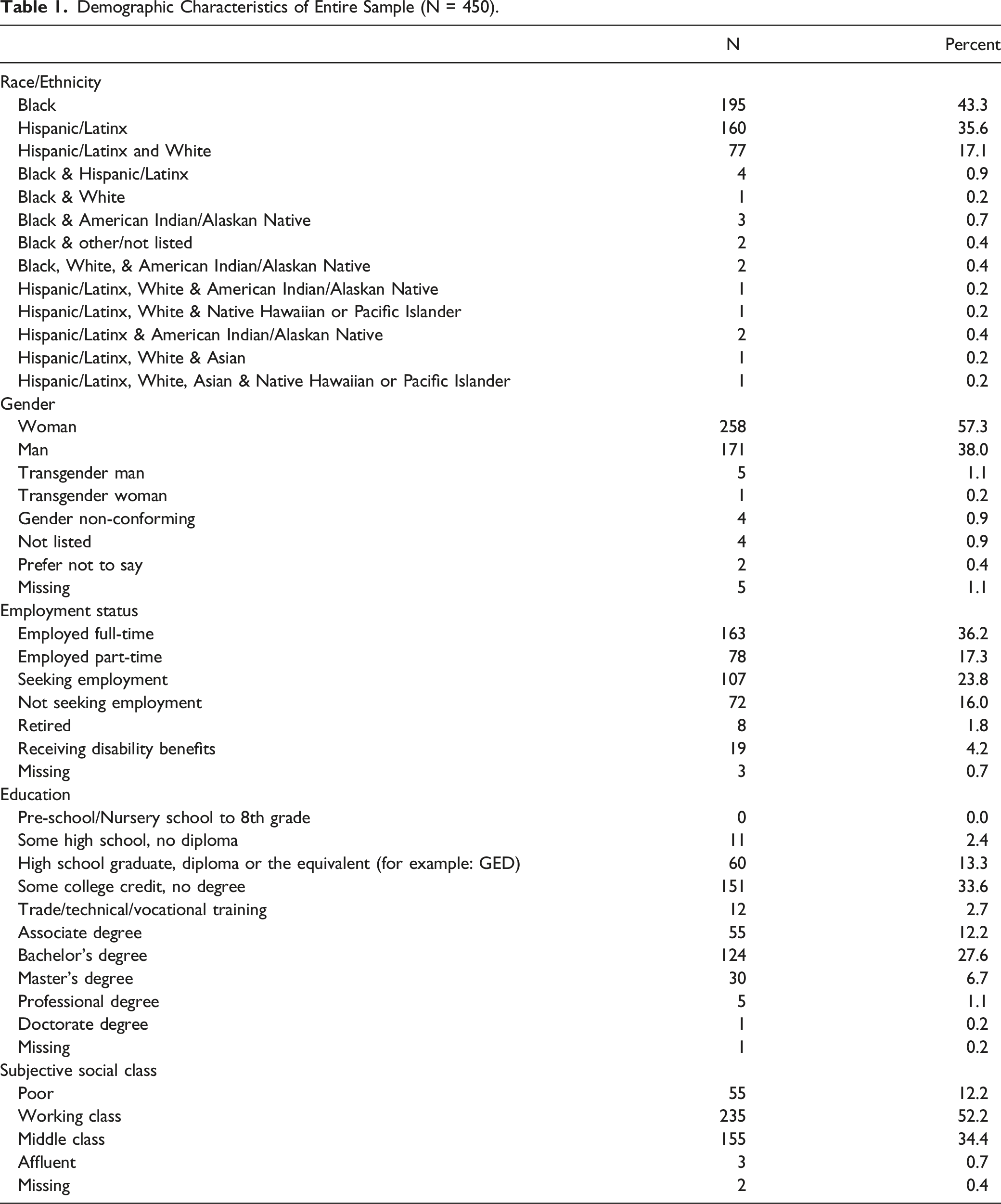
Demographic Characteristics of Entire Sample (N = 450).
Exercise Engagement
Participants in different SOC differed significantly in weekly moderate physical activity (F(4, 449) = 24.88, P < .001), vigorous physical activity (F
(4, 449)
= 40.06, P < .001), and walking (F
(4, 449)
= 8.99, P < .001). Specifically, participants in Action and Maintenance completed significantly more days of walking, as well as more days of moderate and vigorous exercise weekly than those in Precontemplation, Contemplation, and Preparation (Figure 1). Weekly exercise as reported by the IPAQ-SF by SOC.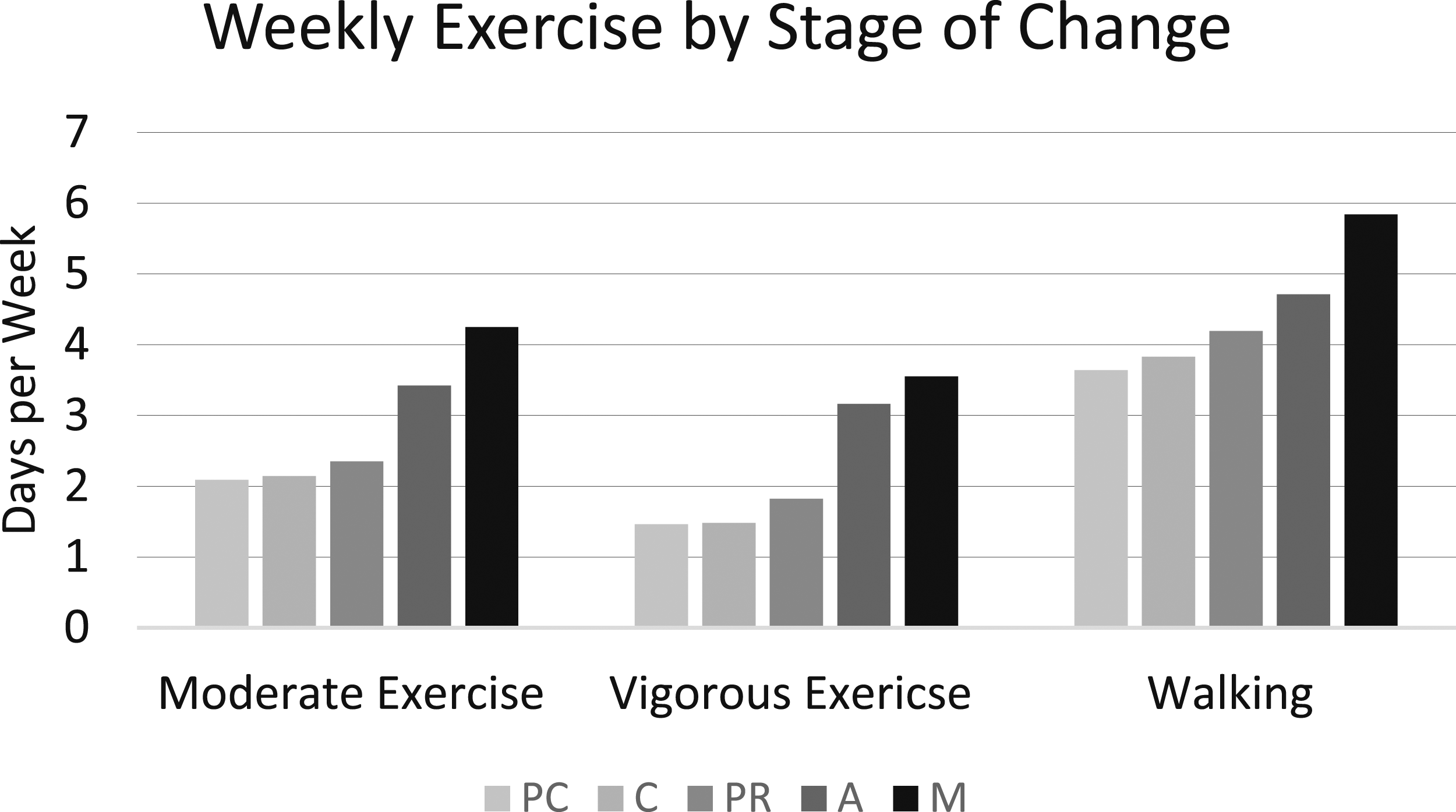
Decisional Balance
Exploratory factor analyses suggested a three-factor solution. The first factor reflected Pros of regular exercise, and two factors independently reflected different Cons of regular exercise. The first Cons factor (Time and Safety Cons) consisted of items associated with safety and time taken away from social, family, and work responsibilities. The second Cons factor (Discomfort Cons) consisted of items associated with emotional discomfort. Internal consistencies within n 1 for the Pros scale and Time and Safety Cons scale were good (α = .84; α = .76) and the internal consistency for the Discomfort Cons Scale was adequate (α = .71).
The three-factor correlated model showed an adequate model fit (CFI = .89, RMSEA = .08, SRMR = .06). Internal consistencies remained good (Pros α = .85, Time and Safety Cons α = .70, Discomfort Cons α = .75). The three scales were minimally correlated (Pros and Time and Safety Cons: r = .15, Pros and Discomfort Cons: r = −.11, Time and Safety Cons and Discomfort Cons: r = .18).
Self-Efficacy
Exploratory factor analyses established a two-factor solution. The first factor (General Self-Efficacy) reflected situations involving social challenges, weather, and other circumstances under which participants would be challenged to exercise. The second factor (Affective Self-Efficacy) specifically reflected difficult affective challenges, such as feeling stressed or depressed. The internal consistency within n 1 for the General Self-Efficacy scale was excellent (α = .84) and the internal consistency for the Affective Self-Efficacy scale was adequate (α = .71).
The two-factor correlated model showed good model fit (CFI = .91, RMSEA = .08, SRMR = .06). The alpha coefficients of the General Self-Efficacy and the Affective Self-Efficacy scales were .85 and .77, respectively. The scales were moderately correlated (r = .34).
Barriers
Exploratory factor analyses revealed a three-factor solution. The first factor (Family Barriers) reflected competing family obligations, the second factor (Work Barriers) represented items concerning work barriers, and the third factor represented physical or health-related barriers (Health Barriers). The internal consistencies within n 1 of the Family Barriers scale and Work barriers scale were good (α = .84; α = .77) while the internal consistency of the Health Barriers scale was adequate (α = .68).
The three-factor correlated model showed good model fit (CFI = .95, RMSEA = .09, SRMR = .07). The alpha coefficients for the Family Barriers, Work Barriers, and Health Barriers scales were .82, .77, and .76, respectively. The Family Barriers and Work Barriers scale were moderately correlated (r = .52), while Work Barriers and Health Barriers (r = .16) and Family Barriers and Health Barriers (r = .29) were minimally correlated.
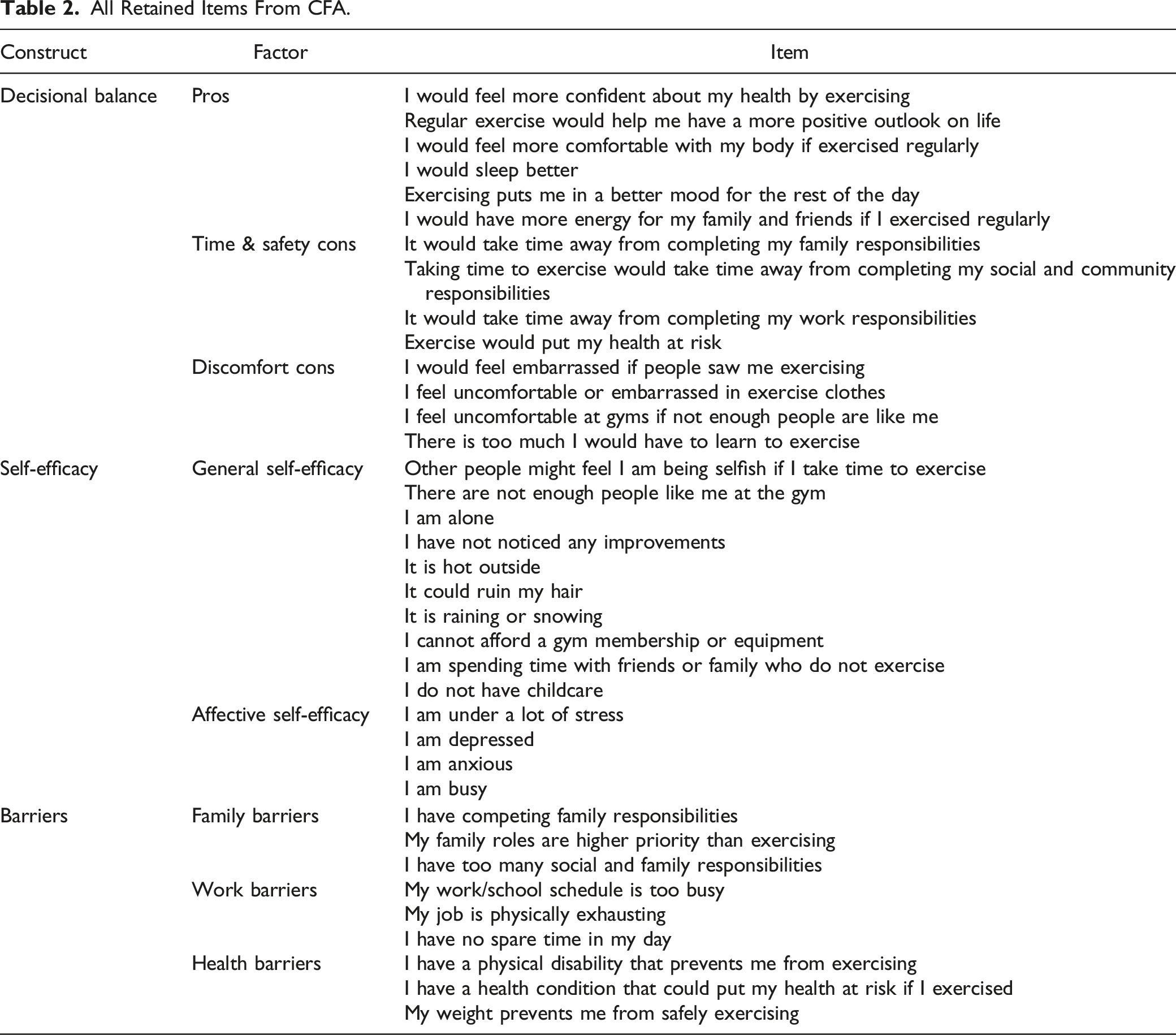
All Retained Items From CFA.
External Validation
Decisional Balance
Multivariate analysis of variance (MANOVA) revealed that individuals at different SOC differed significantly on their subjective importance of the pros and cons of regular exercise (F
(12, 1169)
= 7.62, P < .001, η2 = .06). Follow up ANOVAs indicated that those in different SOC differed significantly on the Pros of exercise (F
(4, 444)
= 17.98, P < .001, η2 = .14) and the Discomfort Cons of exercise (F
(4,444)
= 3.05, P = .017, η2 = .03). Individuals in different SOC did not differ significantly on Time and Safety Cons (F
(4,444)
= 1.74, P = .14, η2 = .02). Post-hoc analyses showed that those in Precontemplation and Contemplation endorsed significantly lower Pros of exercise than those in Preparation, Action, and Maintenance. Those in Precontemplation and Contemplation also reported significantly higher Discomfort Cons than those in Maintenance. The Pros increased 1.1 SD from Precontemplation to Action, the Time and Safety Cons decreased .11 SD, and Discomfort Cons decreased by .29 SD from Precontemplation to Action (Figure 2(a)). Decisional balance (a), self-efficacy (b), and barriers (c), by stage of change.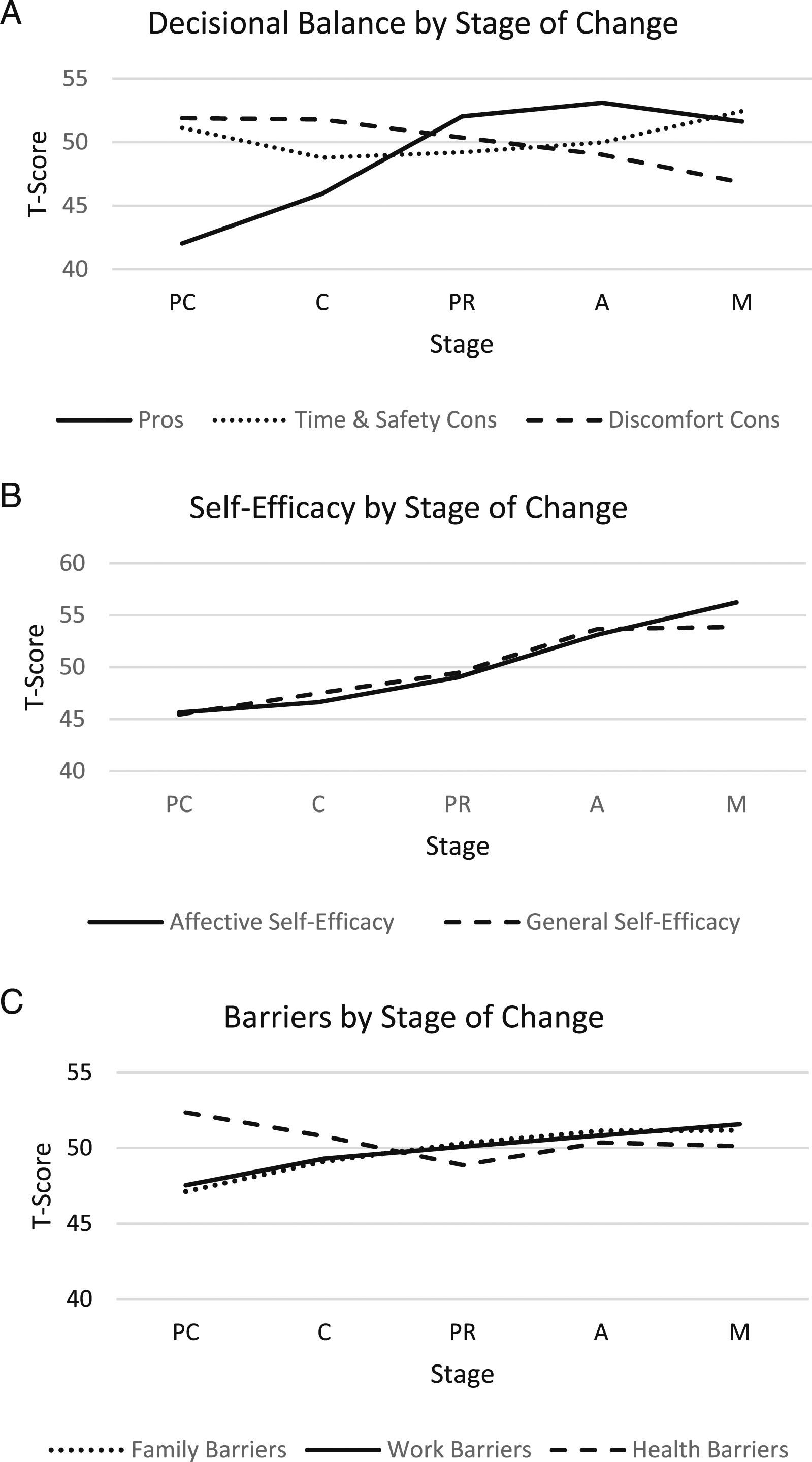
Self-Efficacy
A second MANOVA revealed that individuals in different SOC differed significantly on their SE to exercise (F (8, 888) = 9.48, P < .001, η2 = .08). Follow-up ANOVAs showed that those in different stages of readiness differed significantly on both the General Self-Efficacy scale (F (4, 445) = 9.63, P < .001, η2 = .08) and Affective Self-Efficacy scales (F (4, 445) = 14.96, P < .001, η2 = .12). Post-hoc analyses revealed that both General Self-Efficacy and Affective Self-Efficacy were significantly lower in Precontemplation, Contemplation, and Preparation, than they were in Action and Maintenance. Overall, General Self-Efficacy increased .82 SD from Precontemplation to Action and Affective Self-Efficacy increased .74 SD from Precontemplation to Action (Figure 2(b)).
Barriers
A final MANOVA showed that individuals at different SOC did not differ significantly on their endorsement of Barriers (F (12,1159) = 1.46, P = .131, η2 = .013). However, a visual trend revealed a nonsignificant increase in Family Barriers and Work Barriers from Precontemplation to Action by .4 and .33 SD, respectively. Health Barriers showed no clear trend (Figure 2(c)).
Discussion
The present study provides comprehensive and systematically developed TTM exercise measures for use with Black and/or Hispanic/Latinx adult populations. These measures incorporate important material potentially relevant to exercise readiness and accessibility among populations of color in the US, do not disrupt normal construct shifts by SOC expected under the TTM, and take into account important sociocultural racial/ethnic disparities in the US that may disproportionately affect Black and/or Hispanic/Latinx populations’ readiness to engage in regular exercise.
The construct validity of the SOC algorithm in representing actual exercise behavior as measured by the IPAQ-SF was confirmed. This result was expected given the staging algorithm’s success in predicting exercise behavior in previous studies using different exercise measurements.41,48-50 However, to our knowledge, this is the first study to use the IPAQ-SF to provide support for the external validity of the exercise staging algorithm.
A correlated two-factor solution for the SE construct was retained, which is inconsistent with the anticipated one-factor outcome generated in most general 51 and exercise-specific TTM SE scales.43,52 Research shows that SE increases significantly across SOC for many health behaviors. 51 Equivalent results were found in the current study, with both General Self-Efficacy and Affective Self-Efficacy increasing significantly across SOC. Further, it was anticipated that exercise SE would increase .8 SD from Precontemplation to Action. This hypothesis was supported, as results showed that General Self- Efficacy increased .82 SDs from Precontemplation to Action while Affective Self-Efficacy increased .74 SDs from Precontemplation to Action. These results are encouraging as they indicate that barrier content, when conceptualized within the SE construct, do not disrupt the expected cross-sectional SE stage progression within the TTM.
The measure development process for DCBL yielded a three-factor solution, with one Pros scale and two Cons scales. Most DCBL measure development studies have yielded two-factor solutions: one Pros and one Cons scale; 11 however, a three-factor solution is not unusual.53,54 The three-factor solution in the current study is also not surprising given that significantly more Cons items were added to the item pool than Pros items to incorporate comprehensive barrier content. The fit of the DCBL scales was also adequate.
It was hypothesized that individuals in Action and Maintenance would endorse the importance of Pros significantly higher and the importance of Cons significantly lower than those in Precontemplation, Contemplation, or Preparation. This result was supported for Pros and Discomfort Cons, but not for Time and Safety Cons. This finding suggests that the subjective importance of the time and environmental consequences of regular exercise were similarly important across SOC. It was also hypothesized under the strong and weak principles 11 that stage progression would be associated with a 1 SD increase in the importance of Pros from Precontemplation to Action and a .5 SD decrease in the importance of Cons. These hypotheses were partially supported, as Cons decreased to a lesser degree than expected. These findings contribute to a growing body of evidence which suggest that the Cons construct does not vary significantly across SOC for exercise. Considering that many of the studies outlined prior, in addition to the present study, were completed cross-sectionally, it is possible that this result is specific to cross-sectional research only.
Given the novel measurement of barriers within the TTM framework, no hypotheses were made regarding the factor structure of the Barriers construct. The resultant three-factor solution encompassed three distinct barriers involving family, work, and health challenges. Barriers did not differ significantly by stage. There were change patterns that suggested an unexpected trend, in which Family Barriers and Work Barriers increased across SOC. This pattern suggests that as some individuals progress in their readiness to regularly exercise, they become more aware of the impact of certain barriers to the behavior. Therefore, addressing barriers to exercise may be an important intervention in the middle stages of readiness in these populations. Notably, lack of significance with SOC may suggest that the barrier content is better assessed within the SE and DCBL constructs in the TTM, rather than as an independent scale. It is also possible that Barriers may be better assessed as a single index rather than an overall measure mean. Given that barriers to exercise represent inhibiting scenarios, it is possible that even one barrier item reported to be highly inhibiting is enough to prevent stage progression. Therefore, given this potential impact, future work may consider looking at barriers individually in an index, as opposed to as an overall measure.
It is crucial to note that although barrier items were drawn from literature on Hispanic/Latinx and Black participants’ barriers to exercise, these represent two distinct populations and cultures with numerous subcultures. Not only is there vast heterogeneity between these two populations, but there is also heterogeneity within each. Therefore, although the literature showed overlap, some culturally specific barriers may be unique to one population over the other, leading to under-endorsement of those items from the whole sample. Additionally, to our knowledge, there are no TTM exercise studies involving primarily working-class or low-income White people. Therefore, we are unable to assess how the present findings compare to those found among low-income White populations, or the impact of income more broadly in this sample.
Limitations
Several study limitations should be noted. First, the cross-sectional methodology limits our understanding of how barriers and TTM constructs shift longitudinally and how these changes are associated with actual changes in exercise behavior. Additionally, despite efforts to recruit participants with a wide range of exercise engagement, the resulting stage groupings were skewed towards Preparation, with about 40% of the sample indicating readiness to engage in regular exercise in the next 30 days. The study could have benefitted from a larger representation of participants in early stages. Also, it is important to note that data collection began in February of 2021 when, due to the COVID-19 pandemic, much of the country was instructed to abide by safety restrictions that impacted the nature of work, childcare, gym access, and more. These changes in lifestyle might have influenced some participants perceptions of barriers, exercise access, or other relevant factors to their responses. Future studies should consider assessing the measurement invariance of the new scales across key demographic factors, such as race/ethnicity, age, gender, and socioeconomic status to verify that these measures can be used reliably with each population, and to better understand if and how various identities may influence perceived exercise barriers. Decades of research has demonstrated that the Transtheoretical Model (TTM) is an effective model for conceptualizing and promoting changes in exercise. However, TTM exercise measures were previously developed on relatively homogenous samples, and researchers have called for a redevelopment of these scales for populations of color. This article provides updated and inclusive TTM exercises measures of DCBL, SE, and barriers to exercise developed on a Black and/or Hispanic/Latinx adult sample. These new measures systematically incorporate relevant environmental and personal barriers to exercise that were previously unaddressed in prior measures. This research represents a meaningful step forward in broadening the inclusion of and applicability of the TTM to diverse populations. These measures allow researchers and interventionists to better understand relevant factors impeding exercise engagement and may lead to improved tailored interventions following subsequent research and validation.So What? Implications for Health Promotion Practitioners and Researchers
What is Already Known on this Topic?
What Does This Article Add?
What are the Implications for Health Promotion Practice or Research?
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.