
Abstract
Purpose
This study examined the effect of intervention treatment preference in a post-smoking cessation weight management trial.
Design & Setting
Participants were randomized to a weight management intervention (Stability, Loss, or Bibliotherapy); all participants received a standard smoking cessation program. Adults aged 18+ were recruited from Memphis, TN, and nationally.
Participants
Individuals were eligible if they had a BMI of 22 kg/m2 or greater.
Measures
Participants were asked about their preferred weight intervention at screening. Weight change and self-reported point-prevalence abstinence were assessed (Month 12). Participants rated perceived effectiveness, difficulty (screening, Month 2), and intervention satisfaction (Month 12).
Analysis
We examined the effect of intervention preference match on 12-month weight change, smoking cessation, perceived effectiveness, difficulty, and satisfaction.
Results
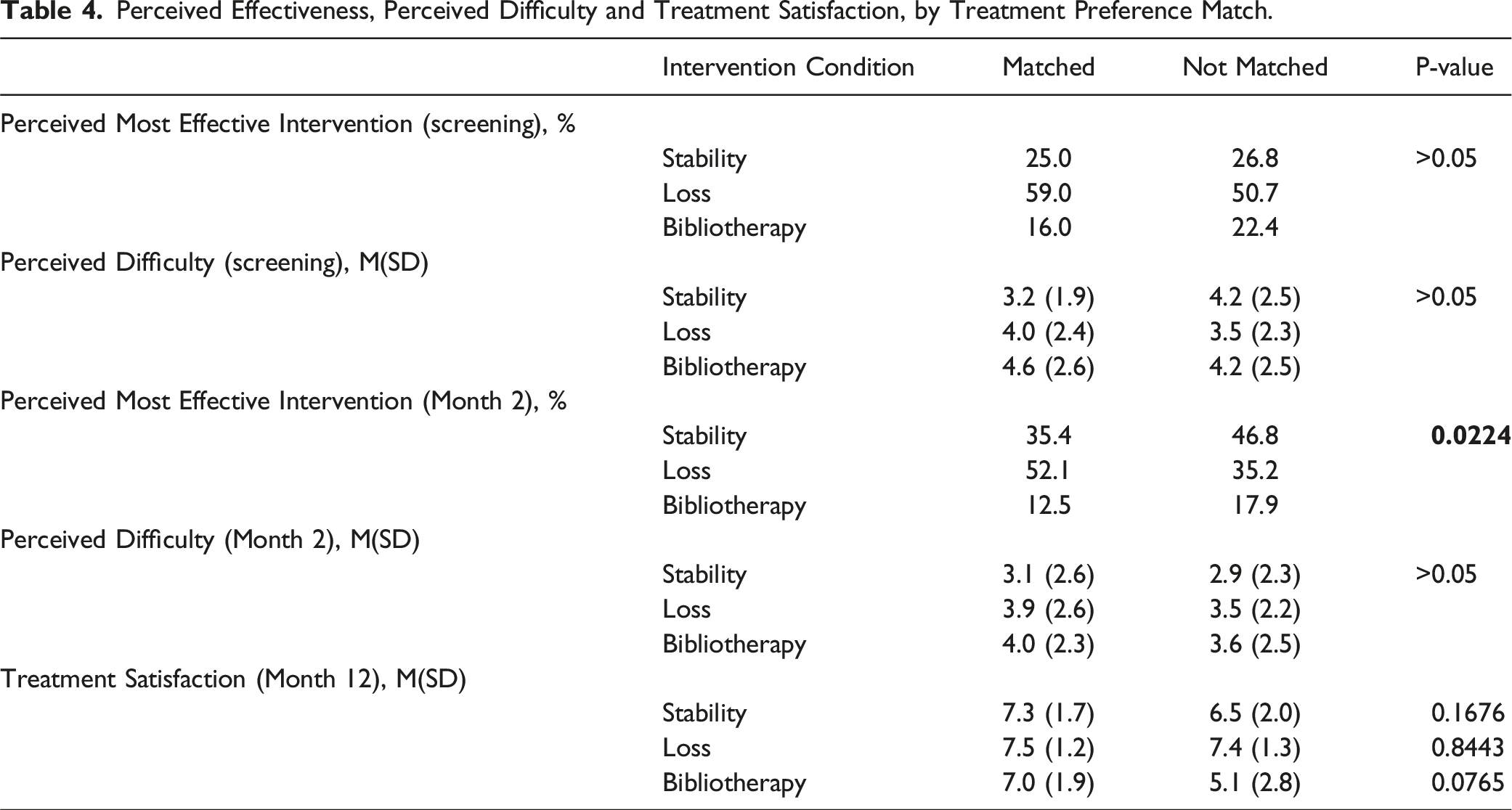
Participants (n = 305) were majority female (68%); white (52%); and had overweight/obesity (87%). At screening, most participants perceived the Loss intervention as most effective; at Month 2, Stability was perceived as most effective. The Stability intervention was perceived as easiest at screening and Month 2. Those who were matched to their treatment preference had greater 12-month weight loss, but similar rates of smoking cessation.
Conclusions
Participants who were matched to their preference were more successful in preventing post-cessation weight gain, compared to those who were not matched. Future research should systematically test intervention preference effects with the aim of precision health.
Keywords
Purpose
The hallmark of randomized controlled trials (RCTs) is unbiased assignment to 2 or more conditions (ie, treatments). However, this design ignores participants’ potential preferences for treatment, which might have motivated them to join the study or might have developed during the informed consent process. 1 Research has found that sometimes participants have strong preferences for the type of treatment they want to receive, even when the treatments are similar. 2
Meta-analyses indicate that participants who receive their preferred treatment may have better outcomes in psychotherapy studies 3 as well as in other types of studies. 4 However, weight management studies have largely shown either no effect for preferences on outcomes5,6 or an effect opposite of the study’s intended outcome (eg, less weight loss when participants received their preferred treatment). 7 Specifically, in terms of weight loss studies, Burke et al found similar weight losses regardless of whether participants were matched to their preferred diet type, 5 and Borradaile et al 7 found lower weight loss among those who received their preferred diet type. In addition, Renjilian et al 6 found that a group-based weight loss intervention was more effective than a one-on-one weight intervention, regardless of treatment preference. Thus, there are limited and mixed outcomes regarding the impact of participant preference in weight management studies, and there is a need for more research to elucidate preference effects.
In examining preference effects, it is also important to consider other important variables like recruitment and retention. 8 One review of psychotherapy treatment preference studies found that those who were given their preferred treatment were less likely to drop out of treatment. 3 However, another systematic review that more broadly examined treatment preference effects reported that matching participants to their desired treatment was associated with better recruitment but not with reduced attrition beyond recruitment. 1 The one weight loss trial that examined the impact of preference on retention found no effect. 7
The effect of preference matching on adherence to and satisfaction with interventions is similarly uncertain. In a study of medical treatments for chronic diseases, matching participants’ treatment preferences improved satisfaction with treatment. 8 However, other researchers have found no effect of preferences on later adherence or satisfaction. 9 Thus, the effect of preferences on both overall outcomes as well as engagement (eg, retention, adherence, satisfaction) remains uncertain, particularly in the area of weight management.
Thus, the current study is a secondary analysis of a post-smoking cessation weight management trial, with the aim to examine associations between participants being assigned their preferred weight management treatment and their eventual weight and smoking cessation outcomes, as well as their retention, attendance at sessions, satisfaction, and perceived effectiveness of treatment. We hypothesized that participants matched to their preferred weight management intervention would have lower weight gain, greater engagement in the intervention (ie, greater session attendance), and lower attrition compared to those who were not matched. In addition, we hypothesized that, since all participants received the same smoking cessation intervention, there would be no effect of treatment preference matching on smoking cessation outcomes. Finally, we hypothesized that participants matched to their preferred weight management intervention would be more satisfied.
Methods
Design
Data for this secondary analysis study was obtained from the Fit & Quit post-cessation weight gain randomized controlled trial; details related to the trial design and primary outcomes are available elsewhere.10,11 Briefly, participants were randomly assigned to 1 of 3 intervention conditions: Stability (ie, learning evidence-based behavioral strategies to facilitate weight stability), Loss (ie, learning evidence-based strategies to facilitate weight loss), and Bibliotherapy (ie, receiving a self-guided weight management book, “The Eating Well Diet”). Regardless of weight management condition randomization, all participants were given the same smoking cessation intervention (ie, behavioral intervention sessions plus varenicline/Chantix®). In terms of the main outcomes, Loss participants lost significantly more weight than participants in the Bibliotherapy condition, while weight change in the Stability condition was not significantly different from the Bibliotherapy condition due to lower than expected weight gain in this self-guided comparison condition. 11 There were no significant between-condition differences in smoking cessation outcomes.
Sample
A total of 305 participants aged 18 and older were initially recruited from Memphis, Tennessee and then nationally (with the start of the COVID-19 pandemic) for Fit & Quit trial. 12 Participants were recruited for the Fit & Quit trial through periodic advertising via both traditional (eg, radio, television, print) and electronic (eg, social media posts, university listserv announcements) media advertisement. Individuals were eligible if they had a BMI of 22 kg/m2 or greater, and were able to participate in study activities (eg, ability to engage in 10 minutes of exercise). Participants did not have to express interest in losing weight or maintaining their weight to be eligible. Individuals with a contraindication to varenicline, current depression or suicidal thoughts, and other physical health conditions that may contraindicate participation in a weight loss intervention (eg, pregnancy) were excluded. Further, those who were involved in other weight management and smoking cessation programs, had weight loss surgery, lost 10 or more pounds in the past 6 months, or were taking medication that influenced weight were also excluded.
Prospective participants completed a brief screening call to determine eligibility; screening visits were then conducted to confirm eligibility as well as to obtain informed consent. Those who continued to express interest were asked to complete a 3-day diet and exercise journal and obtain medical clearance for participating in the study. After completion of the baseline visit, participants were randomized to 1 of the 3 conditions and given an electronic BodyTrace scale along with other intervention materials specific to their assigned condition. Recruitment was ongoing from 2018 to 2021; final data collection visits took place in 2022.
Weight Management Interventions
The weight management interventions for the Fit & Quit trial have been described previously.
10
In brief, the “Stability” intervention was adapted from the “small changes” protocol in the “Study of Novel Approaches to Weight Gain Prevention” trial,
13
and focused on small 100 calorie changes and increases in steps to prevent weight gain. Participants were encouraged to maintain a stable weight, which they could monitor through a personalized weight trajectory graph and customized feedback. Participants in the Stability condition received small prizes weekly for maintaining their weight in the green zone. The “Loss” intervention (adapted from the Look AHEAD intensive lifestyle intervention
14
) aimed to help participants reach their exercise (ie, 175 minutes per week), calorie, and fat goals (based on their baseline weight), facilitated by meal replacements. Both the Stability intervention and Loss intervention conditions had weekly 60-minute group phone sessions during the first 8 weeks of the study. Additionally, both the Stability and the Loss intervention conditions received monthly booster sessions via telephone, after completion of the smoking cessation intervention during months 4-8 of the study. Participants in the “Bibliotherapy” intervention condition were given “The Eating Well Diet” book and were asked to use it independently for the first 8 weeks of the study; the Bibliotherapy condition did not receive booster sessions in months 4-8 of the study (Figure 1). Study design.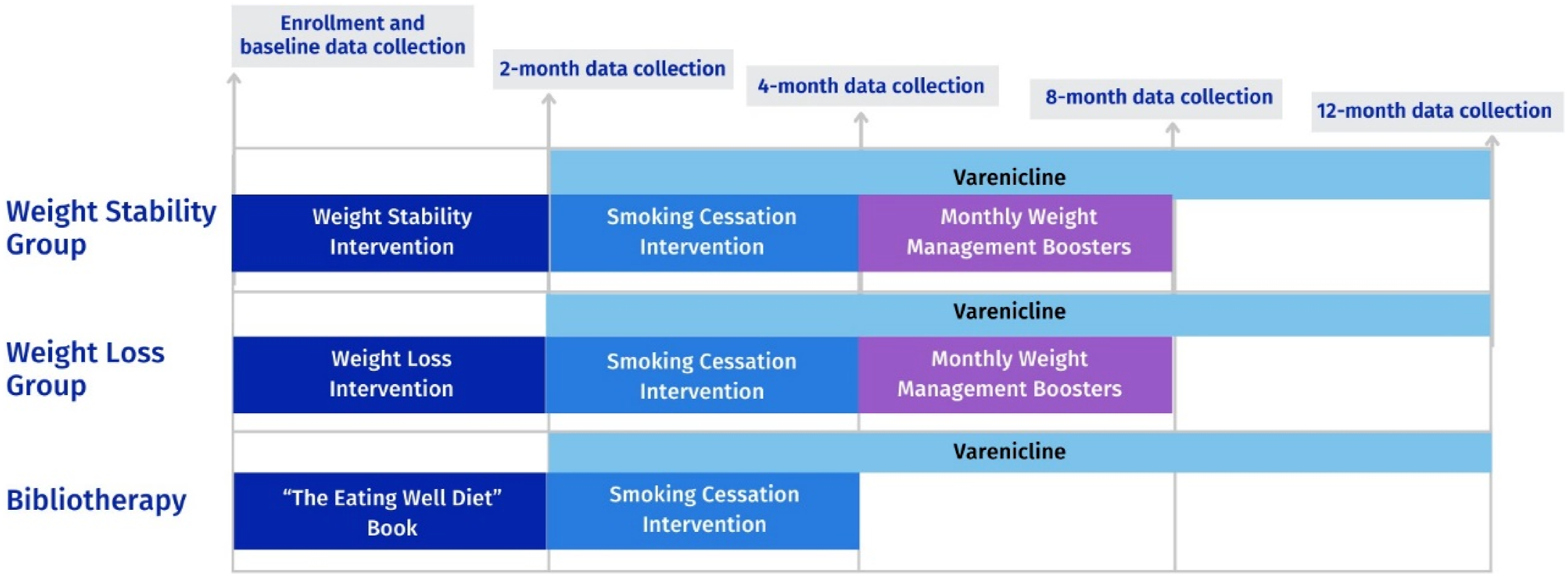
Smoking Cessation Intervention
All Fit & Quit participants received a smoking cessation intervention that followed the Clinical Practice Guidelines recommendations 15 and included 6 total weekly 60-minute group smoking cessation phone sessions that started in week 9 of the study. During week 11 of the study, which was the week of the recommended quit date, participants also received an individual phone session. Varenicline was provided to participants for 6 months.
Measures
Treatment preference
Participants’ preferred treatment was assessed at screening only; individuals were asked to indicate to which condition they hoped to be randomly assigned (three response options: Stability, Loss, or Bibliotherapy).
Anthropometrics
Body weight was obtained through measurements at baseline and Months 2, 4, 8, and 12 either in-person on a calibrated clinic scale or using the participants’ BodyTrace electronic scales after the start of the COVID-19 pandemic. Weight change was calculated as the change in body weight (in kilograms) between baseline and Month 12. Participant height was collected at the baseline visit by research study staff, measured prior to the COVID-19 pandemic and self-reported during the pandemic; BMI was calculated as weight in kilograms / height in meters. 2
Point-Prevalence Abstinence
At every data collection visit, participants were asked if they had smoked a cigarette, even just a puff, in the past seven days. Biochemically-verified smoking abstinence rates were concordant with the self-reported results, 16 and thus, just self-reported abstinence is reported in these secondary analyses.
Treatment Attendance
For weight management session attendance (Loss and Stability conditions), study staff recorded participant attendance for 8 weight management sessions and 5 booster sessions. Mean percentage of sessions attended within each condition was calculated. Study staff coded participant attendance as present or absent for the 7 smoking cessation sessions (range = zero to 7). Mean percentage of sessions completed within each condition was used as the treatment attendance measure.
Perceived Treatment Effectiveness and Difficulty
Two items assessed perceived effectiveness and difficulty of the 3 weight management interventions at screening and at Month 2: (1) perception of which treatment approach would be most effective (3 response options: Loss, Stability, or Bibliotherapy), and (2) perceived difficulty of each intervention (10-point scale; “not at all difficult” – “Very difficult”).
Treatment Satisfaction
Weight treatment satisfaction was measured at Month 12 by 1 item that assessed satisfaction with the assigned weight management approach (8 point scale: “Not at all satisfied” (1) – “Very Satisfied” (8)), consistent with previous weight loss studies. 17
Demographics and Sample Characteristics
Demographic information was collected from all participants at the screening visit, including age, gender, race, ethnicity, marital status, education level, and income. Nicotine dependence was also assessed at baseline using the Fagerström test for nicotine dependence. 18
Statistical Analyses
All analyses were performed using SAS/STAT, version 15.2. Descriptive statistics (means and standard deviations for continuous variables and frequencies and proportions for categorical variables, respectively) were calculated to examine the dependent variables (weight change, smoking cessation, attendance, satisfaction, and perceived effectiveness) overall and by treatment condition. We also examined demographic variables overall and according to treatment preference match. Comparison of characteristics between treatment preference match and non-match conditions were carried out with the two-sample t test and chi-square test, for continuous and categorical variables respectively. Perception of the most effective intervention over time by treatment assignment and treatment match was tested using a stratified chi-square analytical approach. Perceived difficulty of each intervention between screening and 2-month follow-up was compared using a simple linear mixed model while accounting for correlation in data related to repeated measures. This model was extended to test the effect of actual treatment assignment and treatment match on perceived condition difficulty. Treatment satisfaction at Month 12 between conditions was compared using analysis of variance model with Bonferroni adjustments for multiple comparisons relative to Bibliotherapy which was considered a referent condition. This model was extended to incorporate and examine the effect of treatment match on satisfaction. Multivariable linear (weight change models) or logistic (smoking cessation models) regression models were applied to assess the relationship between treatment preference match with weight and smoking cessation outcomes. Multivariable models were adjusted for age, gender, BMI, baseline weight (weight change models only), race, ethnicity, marital status, education, income, and Fagerström dependence score. Additionally, models included a treatment preference match by gender interaction term. Results were considered significant at the alpha level of 0.05 along with other evidence such as effect sizes, magnitude of association and variability. Multiple comparisons between intervention arms were performed with Bonferroni adjusted P-values.
Results
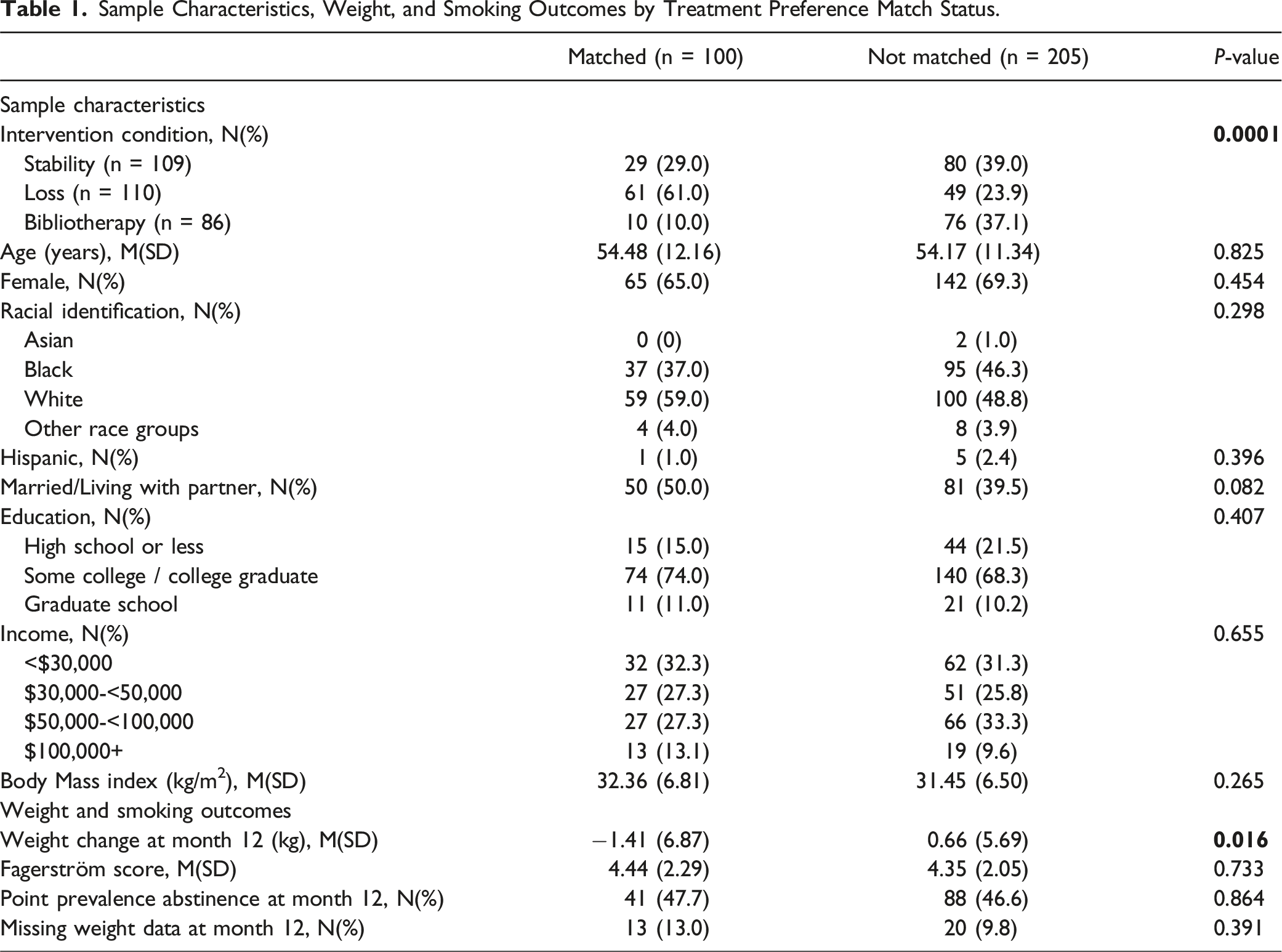
Sample Characteristics, Weight, and Smoking Outcomes by Treatment Preference Match Status.
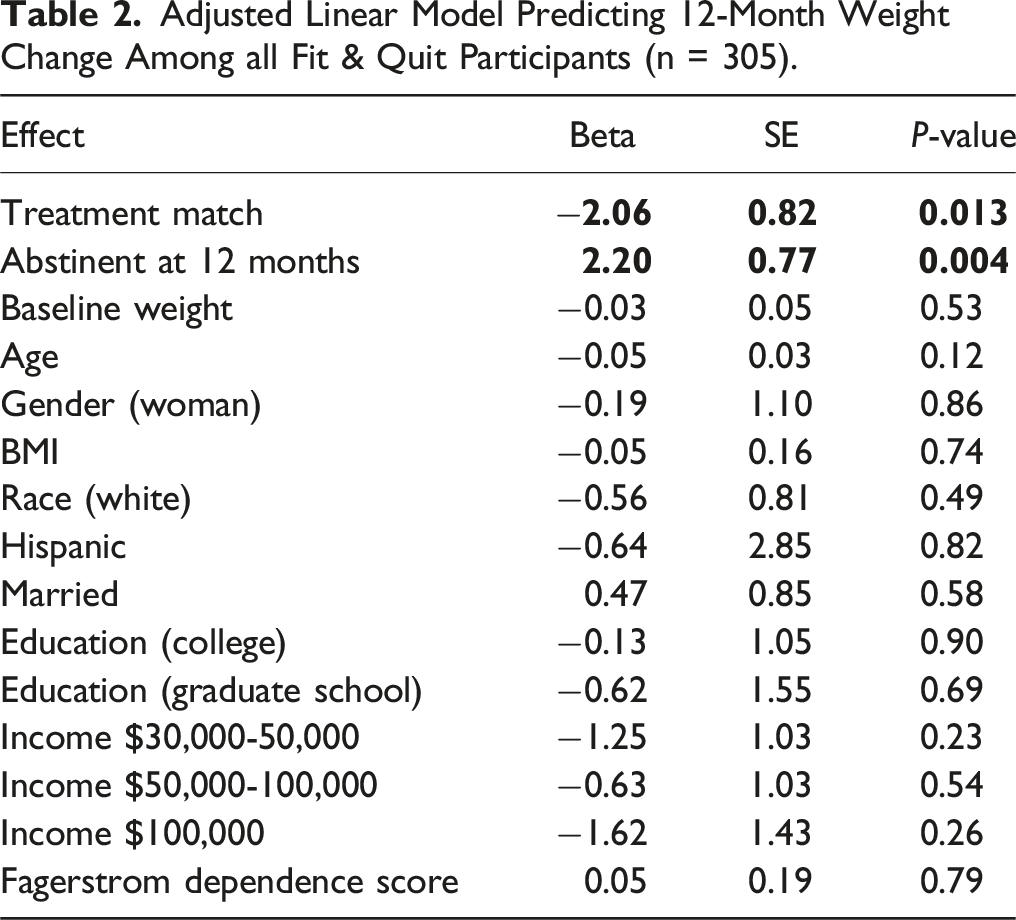
Adjusted Linear Model Predicting 12-Month Weight Change Among all Fit & Quit Participants (n = 305).
Contrary to our hypotheses, there were no differences in retention or session attendance in the intervention by treatment preference match. Specifically, at Month 12, 10.8% of participants had missing weight outcome data, with no significant differences by treatment preference match (Table 1). Attendance at the weight management sessions was 64%, for both those who were matched to their preferred treatment and those who were not. Attendance at the smoking cessation sessions was 53%, with no difference based on treatment preference match. Booster session attendance for those matched to their preferred treatment was 37%, which was not significantly different from those who were not matched to their preferred treatment (33%).
Perceived Effectiveness, Perceived Difficulty, and Treatment Satisfaction by Intervention Condition.
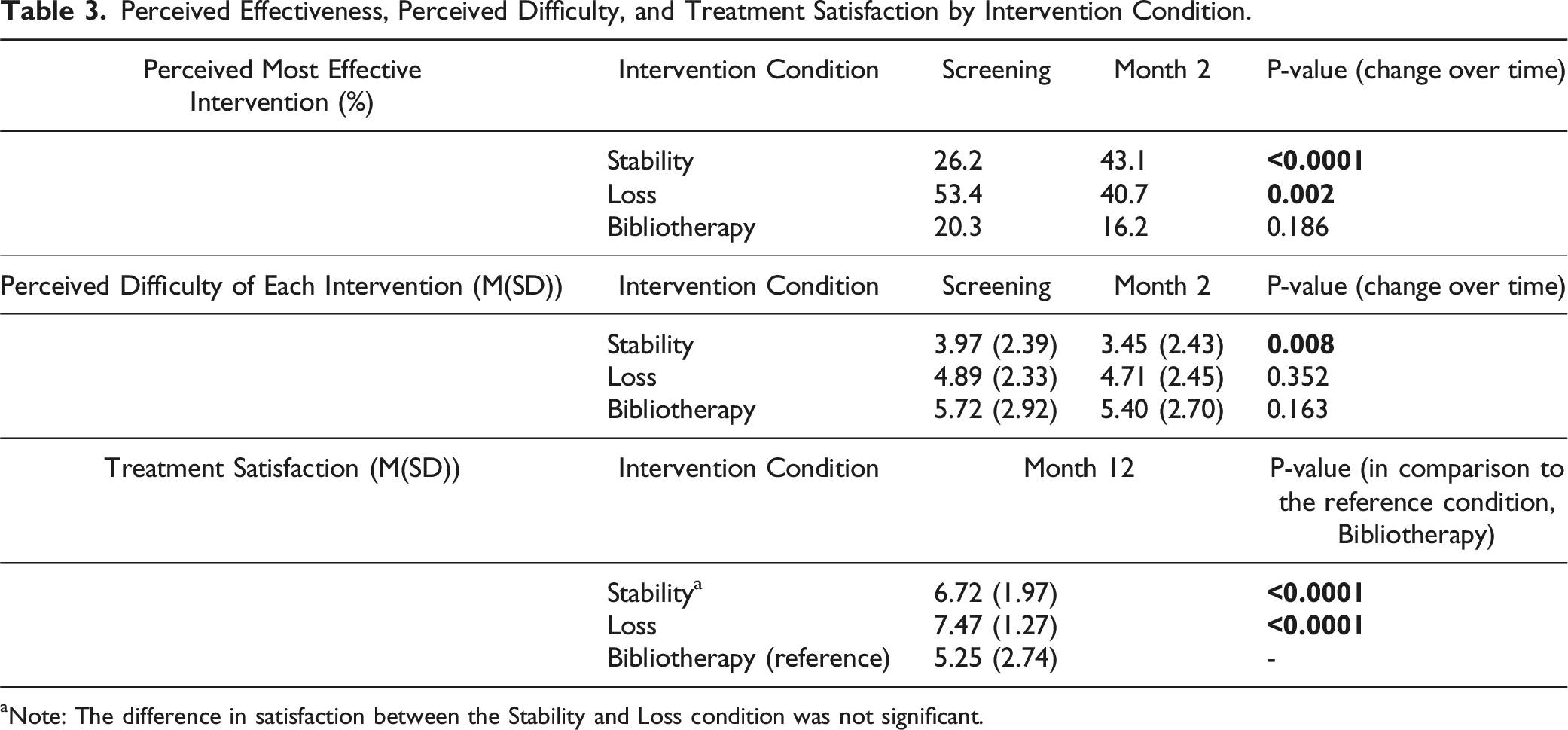
aNote: The difference in satisfaction between the Stability and Loss condition was not significant.
Perceived Effectiveness, Perceived Difficulty and Treatment Satisfaction, by Treatment Preference Match.
Discussion
Despite previous evidence indicating that participant treatment preference may not impact outcomes in weight management interventions,6,7,19-21 we found that treatment preference match significantly predicted 12-month weight change among our study participants. Specifically, those who were matched to their treatment preference experienced weight loss of 1.41 kilograms, or roughly 3 pounds, more than those who were not matched (P = .02) (Table 1). However, individuals who were matched to their preferred program did not have significant differences in treatment attendance or treatment satisfaction. As expected, we did not find any association between preferred weight loss treatment match and the odds of smoking cessation, since all participants received the same smoking cessation intervention. We also did not find systematic differences in attrition at Month 12 by treatment preference match, inconsistent with previous literature. 21
Thus, focusing on dissemination of the Loss intervention for post-cessation weight management may be most fruitful, given that most participants perceived that this intervention approach would be most effective initially (53%) as well as the fact that this intervention was most efficacious in preventing post-cessation weight gain. 11 Nonetheless, more participants perceived that the Stability approach would be most effective at Month 2 (43% at Month 2 vs 26% at screening), indicating that after experiencing the Stability intervention or weight management in general, more participants had confidence in the Stability approach. Indeed, participants in the Stability condition were successful at remaining weight stable at Month 12, 22 in contrast to epidemiological data indicating that 5 kg of weight gain is typical in the year after quitting smoking. 23 Further, at both screening and Month 2, participants rated the Stability approach as least difficult, with the Stability approach perceived as even easier at Month 2. Thus, the Stability intervention may be a promising approach, as it may be less intimidating than a weight loss intervention for individuals who are already making a substantial health behavior change (smoking cessation). In addition, the Stability approach may also be a better fit for those individuals in the normal weight or underweight BMI ranges where weight loss may not be recommended.
Finally, in terms of satisfaction, participants rated the Loss and Stability approaches similarly, while satisfaction with the Bibliotherapy intervention was lower, perhaps because those in the Bibliotherapy intervention had less social support and supportive accountability from the group facilitator and fellow group members in their weight management efforts. In addition, the Bibliotherapy intervention was rated as most difficult and perceived as least likely to be most effective, which is not surprising given the self-guided approach for the Bibliotherapy condition.
Strengths and Limitations
Our study was strengthened by several factors, including the diversity of the sample and the low rate of attrition. Despite this, although we did not observe systematic differences in demographic characteristics by treatment preference match, participants were not randomly assigned to be matched or mismatched to their treatment preference, which precludes inferences of causality. In addition, it may be that the preference for the Loss approach among participants matched to their preference influenced the conclusion of these secondary analyses, as participants in the Loss condition ultimately lost more weight than those in the Stability or the Bibliotherapy condition. 11 Furthermore, although we only measured treatment preference at baseline in the current study, treatment preferences may change over time, particularly after experiencing a treatment; future research should examine how treatment preference changes over time. Finally, our sample was comprised of primarily non-Hispanic White (52%) and Black (43%) participants and females are overrepresented (68%). Thus, sample representation should be considered when generalizing findings beyond the current study.
Conclusions
In the context of a post-cessation weight management trial, we found that participants who were randomly matched to their weight loss program of choice lost 1.4 kilograms (or ∼3 pounds) at Month 12, while the unmatched condition gained roughly 0.7 kg (or ∼1.5 pounds). While these results diverge from the few available studies of treatment choice in the context of weight management programs, they indicate that participant treatment choice may positively predict weight outcomes, particularly in multiple health behavior change interventions. Further, despite the relatively small magnitude of the weight change in the matched group, it may be sufficient to improve metabolic risk factors: there is strong evidence that weight losses of as little as 2% of total body weight result in improvements to fasting plasma glucose concentrations and hemoglobin A1c.
24
Therefore, consideration of participant treatment preference may be an important aspect of improving long-term health in weight management interventions. Future studies may wish to use random assignment to assess the effect of match/no match on participant outcomes in the context of post-cessation weight gain trials and weight management trials in general, as our results point toward a positive effect of treatment match. Additionally, more research is needed on pre-intervention assessment of treatment preference and post-hoc analyses to determine whether or how treatment preference impacts health behavior change outcomes, as there is a great need to improve the precision of behavioral medicine.
• Participants who receive their preferred treatment may have better outcomes in health promotion interventions; there is limited evidence on the impact of participant preference in weight management studies.
• We examined the effect of intervention preference match on 12-month weight change and smoking cessation in a post-cessation weight management trial. We also examined retention, session attendance, perceived. effectiveness and difficulty, and satisfaction. • When participants were matched to their preferred intervention, they experienced greater 12-month weight loss. • Participants initially preferred a weight loss approach; ultimately a weight stability approach was perceived to be easiest and more effective at Month 2 follow up.
• Pre-intervention assessment of treatment preference may help determine how treatment preference affects health behavior change and could lead to improvements in the precision of health promotion interventions.So What? (Implications for Health Promotion Practitioners and Researchers)
What is already known on this topic?
What does this Article Add?
What are the Implications for Health Promotion Practice or Research?
Footnotes
Author Contributions
Kelsey Day: Writing-Original Draft; Erin Solomon: Writing-Original Draft; Jamie Zoellner: Writing-Review & Editing; Zoran Bursac: Conceptualization, Funding Acquisition, Writing-Review & Editing, Data Curation, Data Analyses; Rebecca Krukowski: Writing-Review & Editing, Funding Acquisition, Supervision, Conceptualization, Methodology, Investigation
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Diabetes and Digestive and Kidney Diseases (R01 DK107747).
Ethical Statement
Trial Registration
The trial is registered on clinicaltrials.gov (NCT03156660).