
Abstract

Purpose
Physical activity is a strong and modifiable protective factor for many adult health outcomes, including mental health and several chronic diseases. 1 Physical activity guidelines recommend that adults participate in at least 150 minutes of moderate-intensity equivalent aerobic activity and at least two muscle-strengthening sessions per week. 1 In 2015, Carlson, et al., estimated that insufficient participation in leisure-time aerobic physical activity accounted for $117 billion in annual healthcare spending among US adults. 2 Since then, adult physical activity 3 and healthcare costs 4 have increased, necessitating an updated estimate. Our purpose was to provide updated estimates of healthcare expenditures associated with inadequate leisure-time aerobic physical activity in a nationally representative sample of non-institutionalized U.S. adults.
Methods
Design
A cross-sectional econometric analysis of surveillance data.
Sample
Data from the 2010-2018 National Health Interview Survey (NHIS) were merged with the 2012-2019 Medical Expenditure Panel Survey (MEPS) at the individual level. NHIS is a multistage probability sample survey of U.S. households conducted annually. MEPS participants are drawn from the NHIS sample. We included adults aged 21 years or older with non-missing MEPS records (N = 82,939 respondents). Adults with missing data on physical activity and covariates were excluded (N = 3651), as were those who were pregnant during data collection (N = 2304) or who reported being unable to do physical activity (N = 968). The final sample included 76,016 participants.
Measures
Participants reported the frequency and duration of vigorous and light or moderate intensity aerobic physical activity. We doubled the weekly minutes of vigorous activity 1 and added them to minutes of light or moderate intensity activity to classify participants into inactive (0-<10 minutes per week), insufficiently active (10-149 minutes per week), and active (meeting the aerobic guideline [≥150 minutes per week]). Participants self-reported general medical expenditures (e.g., outpatient, inpatient, pharmacy).
Analysis
This study replicated the methods in Carlson, et. al., which contains a detailed analytic plan. 2 We used the same four-part weighted econometric model to compare healthcare expenditures among inactive/insufficiently active adults to expenditures among active adults. Models controlled for sex, insurance status, census region, race and ethnicity, marital status, poverty, and age (from MEPS), and education, smoking status, and obesity (from NHIS). We repeated all analyses after excluding adults who reported difficulty walking. Cost estimates were inflation-adjusted to 2019 US dollars (USD) using the Personal Consumption Expenditure - Health Price Index*.
Results
Selected Participant Characteristics, Medical Expenditure Panel Survey, 2012-2019
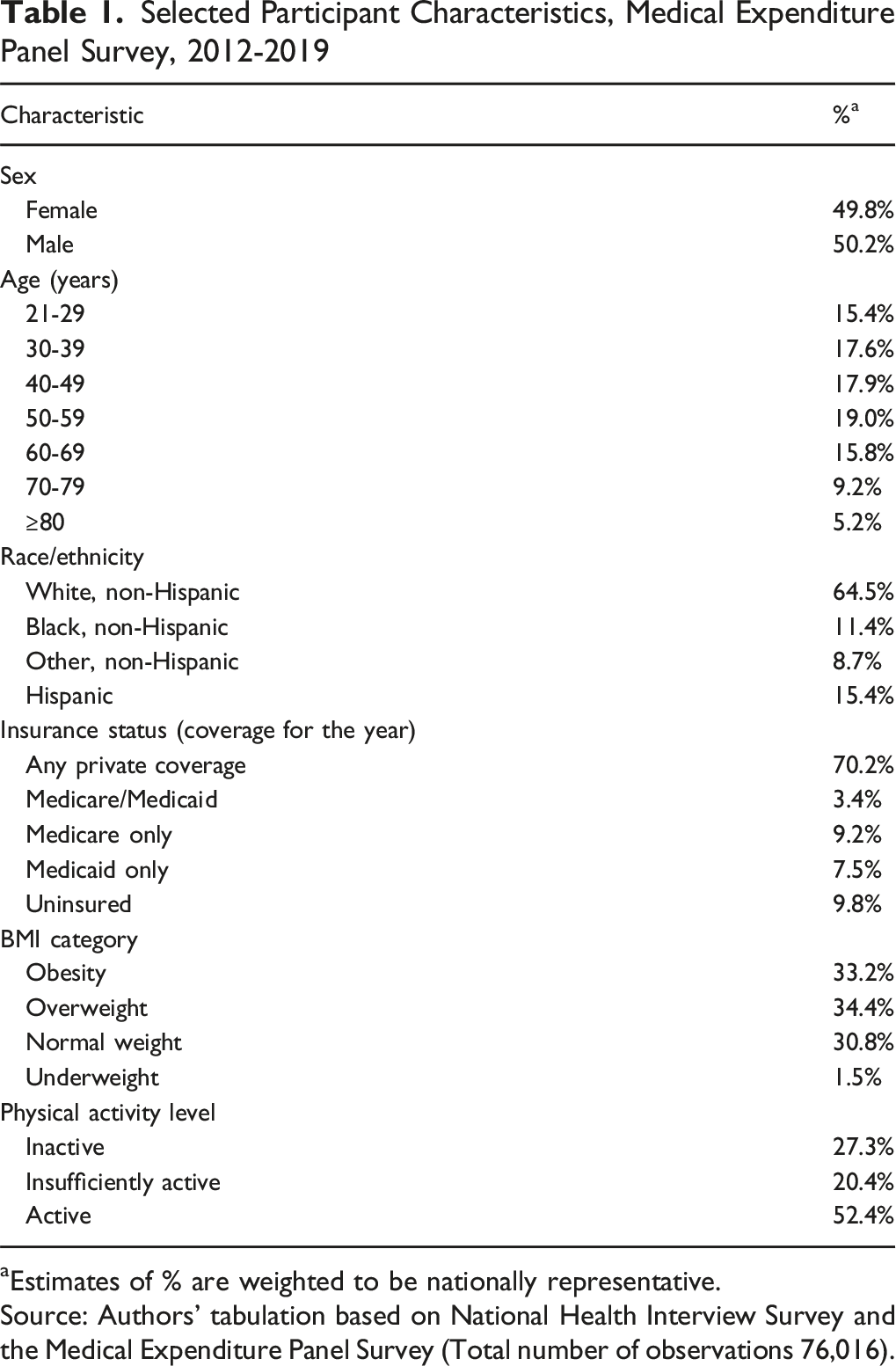
aEstimates of % are weighted to be nationally representative.
Source: Authors’ tabulation based on National Health Interview Survey and the Medical Expenditure Panel Survey (Total number of observations 76,016).
Differences in Healthcare Expenditures by Physical Activity Levels—US Adults, NHIS and MEPS 2012-2019
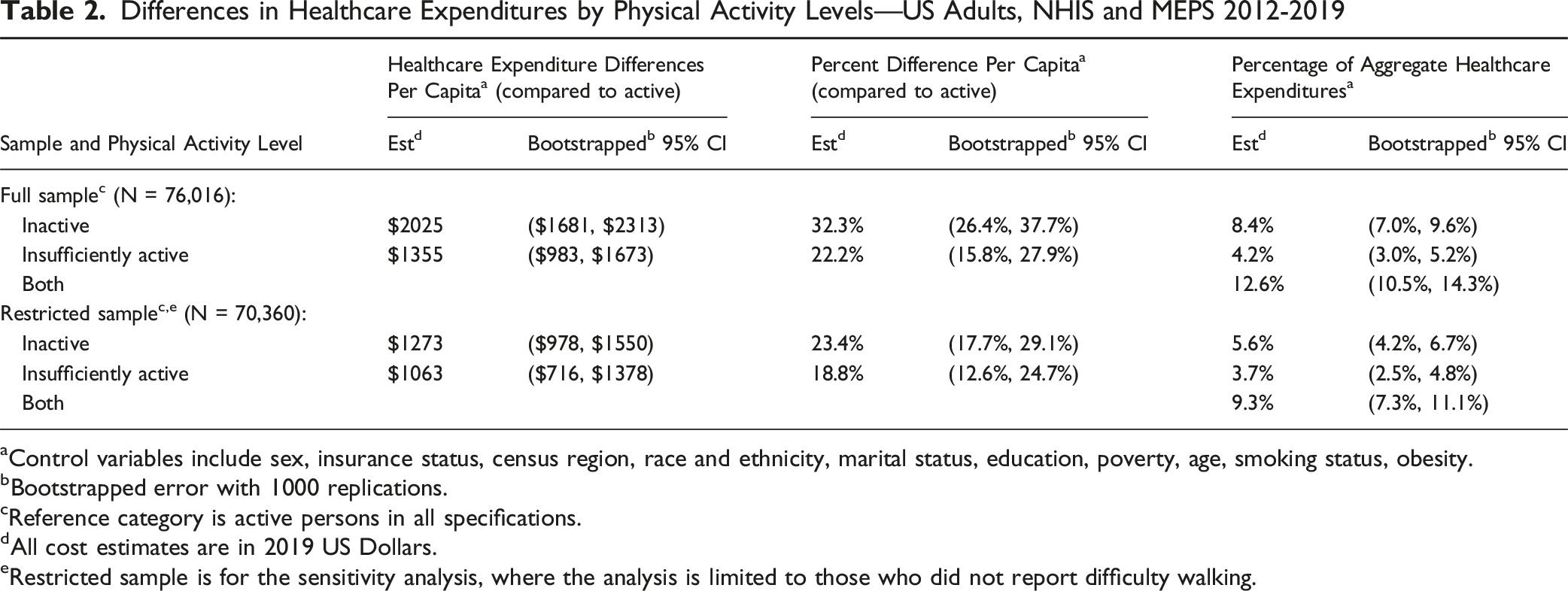
aControl variables include sex, insurance status, census region, race and ethnicity, marital status, education, poverty, age, smoking status, obesity.
bBootstrapped error with 1000 replications.
cReference category is active persons in all specifications.
dAll cost estimates are in 2019 US Dollars.
eRestricted sample is for the sensitivity analysis, where the analysis is limited to those who did not report difficulty walking.
Discussion
Summary
An estimated 12.6% of healthcare expenditures ($192 billion in 2019 USD or $205 billion in 2024 USD) were associated with inadequate levels of aerobic physical activity, updating a previous estimate by Carlson et al. (11.1%, $117 billion in 2012 USD). 2 When the result from Carlson, et al., is inflation-adjusted to 2019 USD ($130 billion), our estimate is considerably higher. Despite a higher prevalence of meeting the aerobic guideline, reasons why our estimates may be higher include: a slightly older sample; potentially greater healthcare utilization from wider health insurance coverage; and an increase in healthcare costs during the 2010s that plausibly overwhelmed any benefit of increased physical activity. 4
Limitations
Potential limitations include reliance on self-reported leisure-time physical activity and expenditure data, restriction to only aerobic physical activity, and potential bias from unmeasured confounding factors. Outpatient encounters are underreported in MEPS and adjusting for obesity, which could be on the causal path between inactivity and healthcare expenditures, could both yield conservative estimates. 5 Future research can expand this estimate by including muscle strengthening activity.
Significance
Inadequate physical activity continues to be associated with a significant percentage of healthcare expenditures in the US. Evidence-based strategies exist to increase population participation in physical activity
1
and may be important tools for controlling healthcare expenditures.
• Despite increases in adult leisure-time aerobic physical activity since 2008, inadequate aerobic physical activity continues to be associated with considerable burden of healthcare expenditures among US adults ($192 billion per year). Increasing physical activity may be important for controlling healthcare costs.So What
Footnotes
Acknowledgements
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Institutional Review Board Statement
Data collection for was approved by the National Center for Health Statistics (NCHS) Research Ethics Review Board (ERB). Analysis of de-identified data from the survey is exempt from the federal regulations for the protection of human research participants. Analysis of restricted data through the NCHS Research Data Center (RDC) is also approved by the NCHS ERB. Research data is restricted and cannot be shared as a part of this RDC agreement.