
Abstract
Purpose
Health & Wellness Coaching is a promising health promotion intervention for patients with complex clinical needs. This study aimed to explore patterns and predictors of coaching use among patients with chronic obstructive pulmonary disease (COPD) receiving care from the U.S. Veterans Health Administration (VA).
Design
Retrospective cohort study using VA’s electronic health records (EHR).
Sample
400 829 patients with COPD receiving VA care during 2021-2023.
Measures
Geographic, demographic, and clinical characteristics associated with coaching use.
Analysis
Mixed effects logistic regression models to examine predictors of coaching use.
Results
Nationally, 4.4% of VA patients with COPD used coaching at least once during the study period. Use of coaching was highly concentrated at select sites, with half of all coaching users receiving care at only 13 VA Medical Centers. Intensive coaching use was limited, with less than 6% of users receiving the recommended 8+ sessions (median = 4.4 sessions). The demographic characteristic most strongly associated with coaching use was being female (OR = 1.64; 95% CI:1.54-1.74). Other demographics significantly associated with coaching use were being Black, Hispanic/Latino, and not married. Being older and living in a rural area were inversely associated with coaching use. Polypharmacy was the clinical characteristic most strongly associated with coaching use (OR = 1.73, 95% CI: 1.62-1.84). Other statistically significant associations with coaching use were obesity, chronic pain, mental health diagnoses, substance use disorders, and smoking were. Prior COPD-related hospitalizations were not significantly associated with using Coaching.
Conclusion
An array of geographic, socio-demographic, and clinical characteristics and patterns associated with coaching use among VA patients with COPD may indicate opportunities for improving coaching implementation. VA and other health systems may consider identifying, strengthening, and diversifying pathways through which patients with complex chronic conditions get connected to coaching.
Purpose
Health & Wellness Coaching is a person-centered, empowering approach to health promotion. Individuals typically pursue coaching when seeking support for initiating and sustaining lifestyle changes that are anticipated to lead to improved health and wellbeing. Health and Wellness Coaches leverage a partnership with the client to facilitate reflection and self-discovery, support goal setting, and provide accountability. While sharing some traits with various forms of counselling and health education, coaching is a distinct profession and modality. Coaches typically take a whole-person view rather than focus on addressing specific health conditions. Relatedly, coaches tend to work with client-determined rather than externally imposed (clinician-determined) goals. Finally, instead of prescriptive advice-giving, coaches facilitate self-inquiry and active learning, although targeted education is sometimes provided.1-3
Coaching is a promising approach for sustainably mitigating the burden of chronic illness.4,5 Engagement in coaching has been found to foster greater self-efficacy, life satisfaction, mental health status, and overall sense of wellbeing.6-8 Coaching clients may also develop a greater commitment to self-care and adopt a more active role in interactions with their healthcare team. Clinical outcomes associated with coaching include lower cardiovascular disease risk, improved pain control in cancer patients, improved HbA1c in diabetics, and reductions in obesity.9-12
While research on outcomes of coaching is increasing, little is known about its utilization – specifically, how well this important intervention is reaching various patient populations. The Veterans Health Administration (VA), the largest nationally integrated health system in the US, provides an ideal setting to explore the use of coaching. Coaching is a critical component of VA’s person-centered, holistic Whole Health System of Care.13-16 The coaching profession in the VA has its own scope of practice, training requirements, and coding standards. 3 VA’s coaches follow an iterative four-stage coaching process that includes (1) exploring the Veteran’s mission, aspiration, and purpose, (2) identifying an area of focus, (3) planning for action (eg, goal setting), and (4) executing the action. 17 Due to their non-clinical role, coaches do not provide health education (eg, inhaler use instruction), although they may point Veterans to appropriate clinical and non-clinical services/resources. VA’s unique integrated healthcare system with a shared electronic health record provides a unique opportunity to examine utilization characteristics and factors that may underlie them.
In this paper, we examine the patterns and predictors of coaching utilization among a specific population — Veterans with chronic obstructive pulmonary disease (COPD). COPD is a debilitating, life-limiting disease that profoundly disrupts patients’ physical, emotional, and social well-being.18-20 Individuals living with COPD often experience difficulties with everyday activities and exercise; this may lead to deconditioning, which further worsens the symptoms, as well as social isolation.20-22 Depression and anxiety are also common in this population. 23 Acute exacerbations of breathlessness, a common symptom, are not only distressing but may also worsen the health status of patients in the long run and result in costly emergency room visits and hospital stays. 24 Coaching is exceptionally well-positioned to support this population, as it assists in developing a stronger sense of meaning and purpose. Veterans are then provided with individually tailored support for establishing healthier habits. Establishment of a trusted coach-client relationship reduces social isolation while providing positive accountability for working toward personally meaningful goals. Indeed, coaching has been shown to improve health-related quality of life, reduce COPD-related hospital admissions, improve self-management, and increase self-efficacy and treatment adherence for patients with COPD.25-29
In practical terms, COPD is a high prevalence condition, 30 present in 14-45% of U.S. Veterans enrolled in VA healthcare.31,32 By focusing on VA patients with COPD, we can better understand patterns in Coaching utilization for a high-need population.
Methods
Design
We conducted a retrospective cohort study of Veterans with COPD receiving VA care between 1/1/2021 and 12/31/2023. The study was approved by the Institutional Review Boards of the VA Bedford Healthcare System and VA Puget Sound Health Care System. A waiver of HIPAA authorization for data collection was obtained.
Sample
Using VA’s Corporate Data Warehouse (CDW) data, we created a cohort of Veterans with 3+ outpatient, inpatient or fee-basis VA appointments with a COPD-specific diagnostic code (as defined by Chu et al 33 ) within any 365-day time window during the study period (n = 400 829). The 3+ appointment approach was chosen to maximize inclusion of patients with an established COPD diagnosis. The first visit of the earliest available 3-visit series was taken as the index date; the VA facility where the index date visit took place was designated as the patient’s home station. See Appendix 1 for methodology details.
Measures
Coaching Use
Use of coaching was identified using a validated algorithm that integrates CPT codes, internal VA accounting codes (CHAR4), and health factors fields that include tagged data elements similar to diagnostic codes34,35 (see Appendix 1 for more information). Only coaching use in the strict sense was assessed; we did not include allied approaches to health behavior change, eg, diabetes prevention or weight loss counselling. Veterans with ≥1 coaching visits after the index date were classified as users, the rest as non-users. We further subdivided the user subcohort based on the number of coaching visits (ie, 1, 2-4, 5-7, and 8+). For patients with >1 visit, only visits occurring within 6 months from the first visit were counted. This breakdown and the timeframe were selected based on literature consensus regarding the optimal coaching dose of 12-15 sessions over the course of 7-9 months, 3 and VA’s internal recommendations for 8-10 coaching encounters per client.
Sociodemographic and Clinical Characteristics
The following characteristics at index date were extracted from the CDW.
Sociodemographic Characteristics
Age, sex, race, ethnicity, marital status, and rurality based on rural-urban commuting area codes (RUCA). 36 Patients for whom demographic information could not be identified from the CDW were recorded as unknown/missing.
General Clinical Characteristics
To reflect the level of VA benefits Veterans are entitled to, VA designates Veterans to priority groups; the determination is made based on military service history, service-connected disability rating, income level, Medicaid eligibility, and other current benefits. 37 Priority group data was used as indicative of Veterans’ level of disability and/or socioeconomic need. To reduce complexity, we reclassified the eight priority groups into four categories: Poverty with no co-pay, high disability with no co-pay, low to moderate disability with partial co-pay, and limited disability with full co-pay. 38
Chronic pain was included under the assumption that utilization of coaching in Veterans with COPD may be tied to chronic pain, the original primary focus of VA’s Whole Health implementation. Presence of chronic pain was operationalized as the Numerical Rating Scale score of ≥1 (range 1-10) within 3 months before and after the index date; the score of 0 or missing score data were taken as indicative of the absence of chronic pain.39-41 Moderate/severe chronic pain was operationalized as the score of ≥4.
Polypharmacy was determined based on the number of unique medication prescriptions (including COPD medications) dispensed within ±3 months from the index date. Polypharmacy was defined as absent (<5 prescriptions), mild (5-9 prescriptions), or severe (≥10 prescriptions).42,43
The presence of 30 common comorbidities was determined within a 2-year lookback window using Elixhauser’s diagnostic code categories. 44 We calculated a score for the total number of comorbidities within the lookback window; “chronic lung disease” was removed from the count to avoid redundancy. We also assessed the presence of two additional mental health comorbidities (anxiety and PTSD).
COPD-Related Characteristics
The length of time with the COPD diagnosis was operationalized as the period between the earliest visit with a COPD diagnostic code in the EHR and the index date. Smoking status was determined at index date based on health factor data. The COPD medication status, a dichotomous variable, was operationalized as record of COPD medications dispensed within ±3 months from the index date. The number of COPD-related hospitalizations, ie, inpatient visits with a principal diagnosis of COPD or a principal diagnosis of acute respiratory failure with a secondary acute exacerbation of COPD diagnosis, 45 was calculated within a 3-year lookback period.
Analysis
We examined demographic and clinical characteristics at index date among coaching users and non-users using descriptive statistics. We further calculated standardized mean differences (SMDs) between these two groups to account for the large sample size of the non-users of coaching and imbalances between the size of the groups. We performed secondary analyses examining differences between subcohorts of coaching users described above. For each VA site we calculated (1) number and percentage of coaching users and (2) number and percentage of patients with 0, 1, 2-4, 5-7, and 8+ coaching visits (the denominator being the total number of patients with COPD at the site during the study period).
To examine the extent to which patients’ demographic and clinical characteristics predicted coaching use, we built a mixed effects multivariate logistic regression model. The dependent variable was the receipt of ≥1 coaching sessions after the index date. All variables previously examined for SMDs were included in the model, except severe chronic pain (dropped due to overlap with the chronic pain variable) and those comorbidities for which no meaningful differences were detected in the univariate analyses. We dropped patients with missing site information, as well as those located at the 10 sites with <1000 total patients in the cohort, from the model (resulting in 120 sites total). Because the overall amount of missing demographic and clinical information was low, patients with missing clinical or demographic characteristics were excluded from the multivariate regression model. Both odds ratios and average marginal effects (AME) were calculated. The AME represents the amount of how much the use of coaching changes on average when a predictor variable increases by one unit, holding all other variables constant.
Results
General Cohort Description
Overall Sample Characteristics
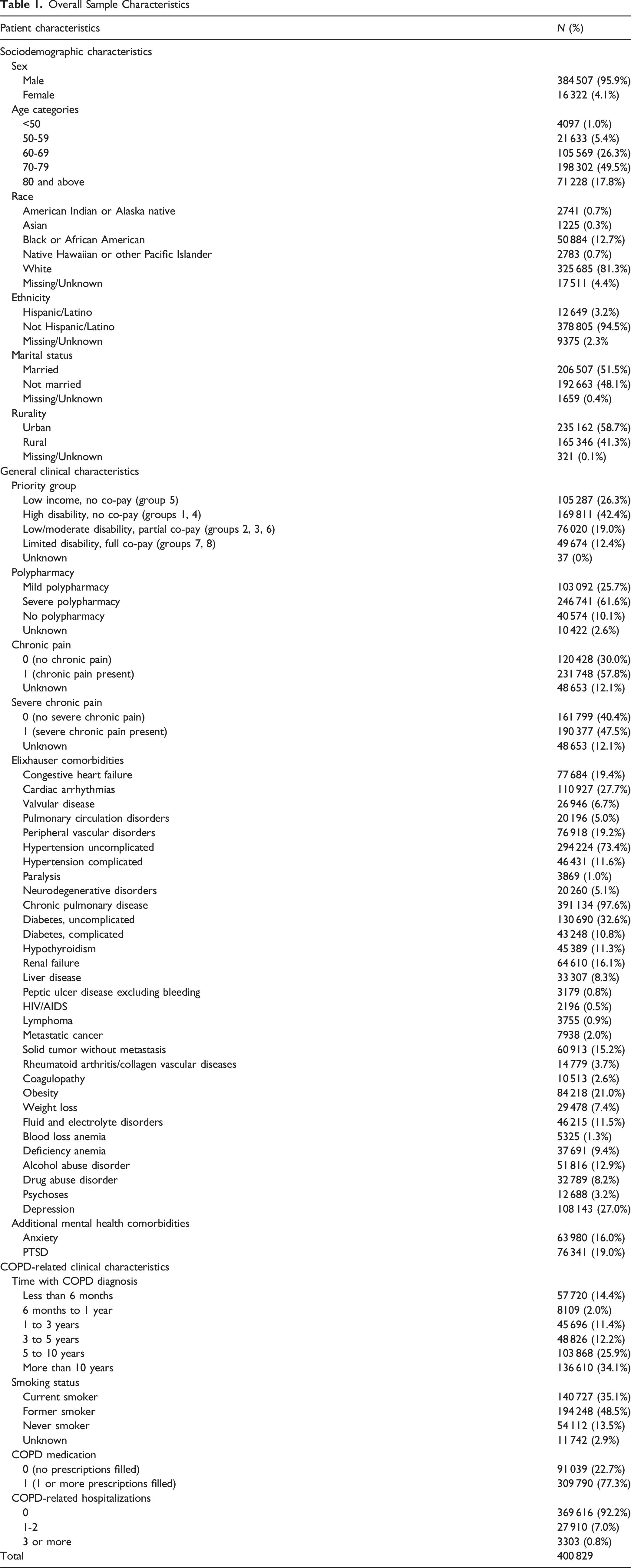
Coaching Use
Patterns of Use
Of the total cohort, 17 816 (4.4%) had ≥1 coaching visits during the study period. Of those, 53.4% (9520) had 1 visit, 33% (5901) had 2-4 visits, 7.5% (1343) had 5-7 visits, and 5.9% (1052) had 8 or more visits. Users had an average (mean) of 3 sessions; the median (4.4) indicated that half of users attended between 4 and 5 sessions.
The patients were located across 130 VA sites, of which 126 had coaching users during the study period. Approximately half of all users (8,986) were concentrated at 13 sites (10% of the cohort sites). Of these, 5 were Whole Health pilot sites (18 VA facilities that received support for Whole Health implementation during the initial rollout). 46
Across facilities, from 0% to 34.9% of patients with COPD at the site were receiving coaching during the study period, with the mean of 4.5%. Of note, among the 18 Whole Health pilot sites, between 0.8% and 26.5% of patients with COPD used coaching, with the mean of 7.6% (Figure 1). Of the 13 sites described above that accounted for almost half of all coaching users in the cohort, at 9 the proportion of Veterans with COPD receiving coaching reached or exceeded 10%. Percentage of Veterans with COPD using Health & Wellness Coaching by site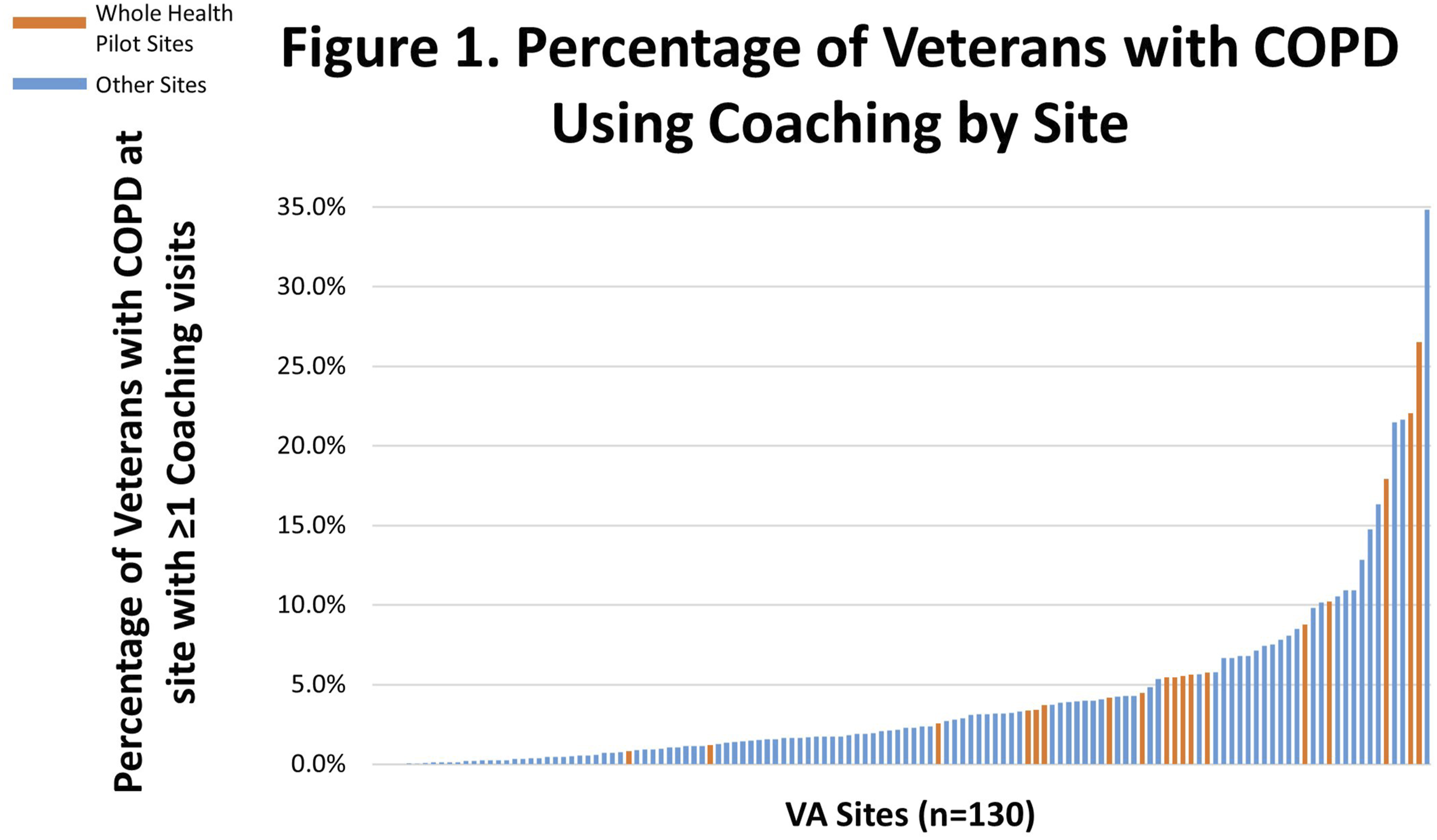
Intensity of engagement with coaching varied by site but was limited overall. At the 126 sites with coaching users, only 6.3% users per site, on average, had 8+ sessions. The largest percentage per site was 33.3%; however, this site had a very small overall (<10) number of users. The proportion of users with only 1 coaching session was 60% or higher at 50 out of the 126 sites.
Differences Between Coaching Users and Non-users
Differences Between Health & Wellness Coaching Users and Non-users on Demographic and Clinical Characteristics
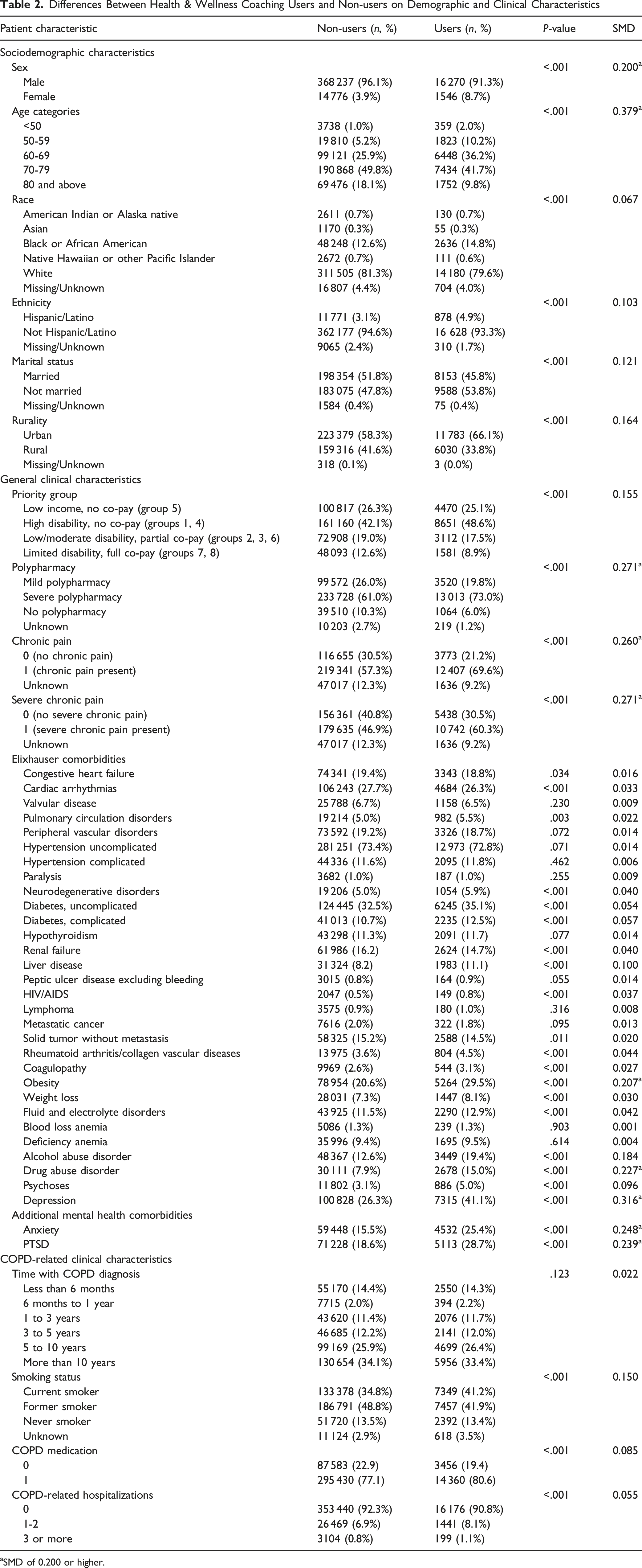
aSMD of 0.200 or higher.
Logistic Regression Model Output
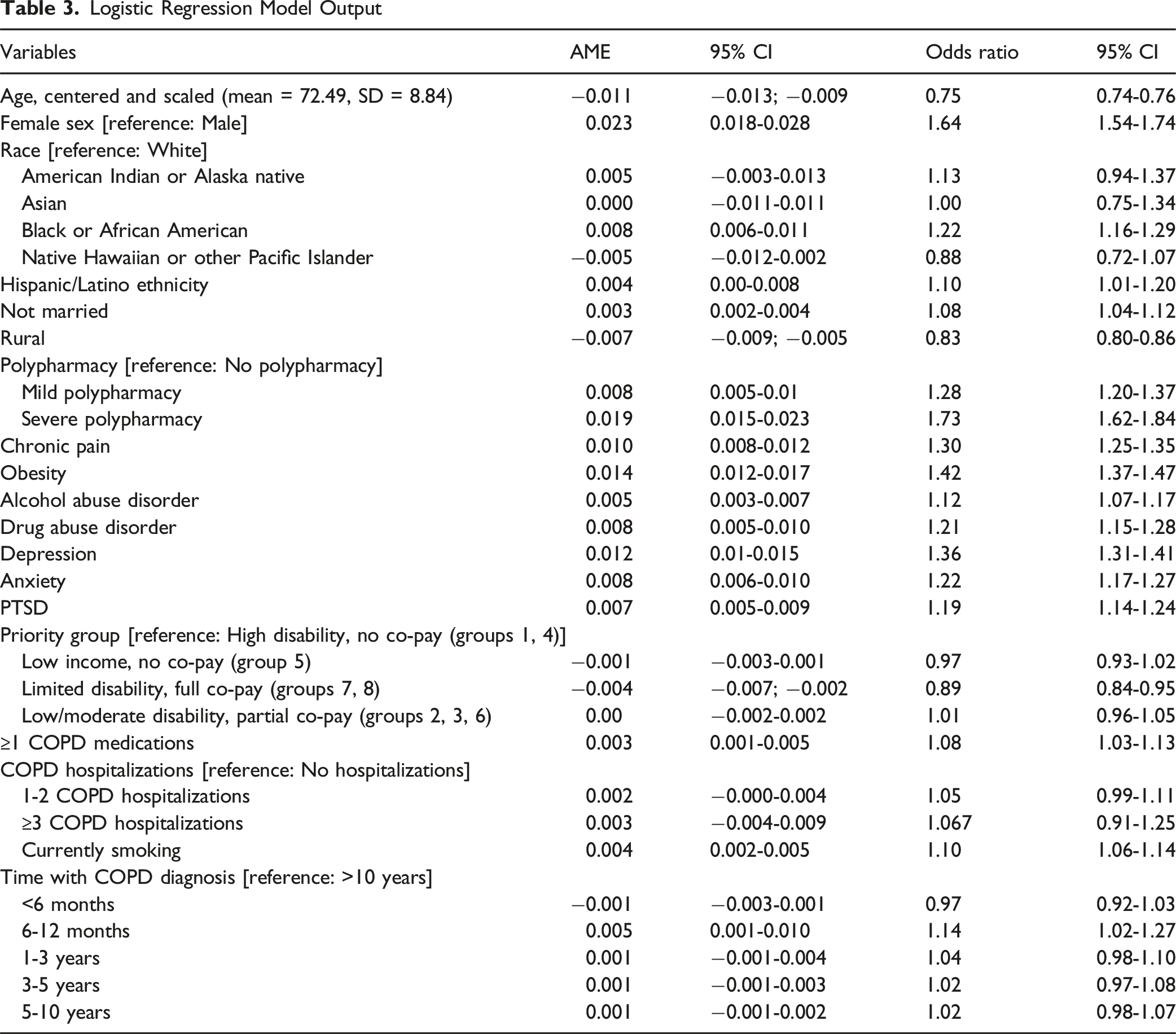
Veterans were more likely to receive coaching if they were female, Black, Hispanic/Latino, and not married. Veterans were less likely to receive coaching if they lived in a rural area. Age had a reverse association with the likelihood of receiving coaching, with each standard deviation increase from the mean (8.84 years) associated with a 1.1% decrease in the probability of receiving coaching. Among demographics, female sex had the strongest association with coaching use (OR = 1.64, 95% CI: 1.54-1.74).
Use of coaching was associated with the following clinical characteristics: chronic pain, mild polypharmacy, severe polypharmacy, obesity, substance use disorders, depression, anxiety, and PTSD. Coaching users were more likely to have higher rates of disability and have no co-pay for VA care. The clinical characteristic with the strongest association with coaching use was severe polypharmacy (OR = 1.73, 95% CI: 1.62-1.84).
Among COPD-related variables, coaching use was associated with having a COPD medication prescription, current smoking status, and a recent diagnosis of COPD (prior 6-12 months). The latter had the strongest association with coaching use in this category (OR = 1.14, 95% CI: 1.02-1.27). Notably, prior COPD-related hospitalizations were not predictive of coaching use.
The Nagelkerke pseudo R-squared for the final model was 0.06, suggesting that approximately 6% of the variability in coaching receipt was explained by the model’s variables. The standard deviation of the random effects measure was 1.205 for the final model; the Intraclass Correlation Coefficient (ICC) was 0.59.
Discussion
This retrospective cohort study of VA patients with COPD has yielded three primary insights: (1) coaching made some inroads into this population (although utilization was limited in intensity and concentrated at a few VA facilities); (2) users differed from non-users on various demographic characteristics; and (3) users tended to be more clinically complex than non-users. Taken together, these findings point to both positive developments in the spread of coaching to this population, as well as to some missed opportunities. There is a need to raise awareness of coaching among providers and Veterans alike and to identify and act upon barriers that may hinder initiating and maintaining use of coaching in this population.
The overall proportion of coaching users among the patients in our study was 5%. It is challenging to put this number into perspective, given that prior literature on coaching use among Veterans or in other populations is limited. However, in a notable example, Reed at al. 47 determined that more than 28% of Veterans with chronic pain and more than 40% of Veterans with co-occurring chronic pain and PTSD receiving care at Whole Health pilot sites reported already using coaching. The much lower proportion of coaching users among the patients in cohort may indicate opportunities to increase the utilization of coaching in this large, high-priority population that is well-positioned to derive benefits from this service.
The concentration of half of all users at 13 sites, many of them Whole Health pilot sites, is a notable finding. The site-level variation was shown to be one of the primary factors explaining patterns in coaching use, as illustrated by the ICC of 0.59, suggestive of high clustering. The higher rates of coaching use at these facilities might be related to their superior Whole Health infrastructure, including higher availability of coaches, established referral patterns, and/or greater awareness of and interest in coaching among patients and healthcare providers. Additional research is needed to identify and leverage organizational structures and practices conducive to optimal coaching utilization; the high-utilizing sites could serve as exemplars.
Intensive use of coaching was limited in our cohort, with <6% of users receiving 8+ sessions during the study period and the majority (53.4%) receiving 1 session. This finding may point to another opportunity for improving coaching utilization. Due to the iterative nature of coaching, a single session is unlikely to yield significant benefits to the client. Indeed, a recent literature synthesis of studies on coaching across a range of patient populations cites 12-15 sessions over the course of 7-9 months as the ideal coaching dose. 3 Future research may explore barriers to long-term engagement in Coaching and identify potential solutions.
Most of the demographic and clinical characteristics associated with coaching use, while statistically significant, were weak, with the highest odds ratio across all variables being 1.73 (severe polypharmacy) representing a 1.9% increase in coaching use compared to no polypharmacy and 1.64 (female sex) representing a 2.3% increase in coaching use compared to men. It is unclear why patients who received coaching were more likely than those who did not to be female, Black, and Hispanic/Latino, but the higher use of Whole Health services in general among these groups is documented in the literature.48-50 Age was also a significant factor distinguishing coaching users from non-users, with older patients less likely to use coaching.51,52 This is also consistent with prior literature. 53 The higher use of coaching among non-married patients may stem from their lower levels of and higher need for social support.56 The lower rates of coaching use among rural Veterans may be indicative of the documented barriers to accessing coaching (and Whole Health services more generally) in rural areas. 54 Why these demographic differences exist and how best to leverage coaching for patients from all backgrounds both remain an underexplored topic, warranting further investigation.
Finally, our findings point to the higher clinical and social complexity of coaching users, compared to non-users. The specific predictors we identified suggest several possible pathways through which Veterans with COPD are currently entering coaching, as well as indicate several potentially underexplored avenues. Coaching users in our cohort displayed higher rates of chronic pain, substance use disorders, depression, anxiety, and PTSD than non-users. This is consistent with prior literature documenting higher likelihood and more intensive use of Whole Health service use among Veterans with these conditions.47,55 It is possible that Veterans with COPD received referrals to coaching for assistance in coping with pain and/or mental health challenges. The salience of pain as a predictor is particularly unsurprising, given that the initial rollout of the Whole Health system was largely precipitated by the urge to provide non-pharmacological solutions to chronic pain. Subsequent efforts also sought to increase awareness of and engagement with Whole Health (which includes referrals to integrative services like coaching, when appropriate) among mental healthcare professionals. More research would be beneficial around best practices for coordinating pain and mental health care between primary care providers, specialists (including mental health professionals), and coaches.
We further discovered that coaching users were significantly more likely than non-users to be obese, currently smoking, on COPD medications, and taking ten or more medications in total. It is likely, thus, that referrals to coaching originate from healthcare providers who seek to draw on coaching as an additional support for Veterans with highly complex healthcare needs, including those who could benefit from lifestyle modifications. This is an encouraging development. Future research may explore in more detail how Veterans with complex clinical needs get connected to coaching, including the providers’ underlying assumptions about who is an appropriate candidate for coaching and the extent to which patients are involved in the decision-making, if at all. This is particularly important given the notably high proportion of Veterans with only 1-2 coaching sessions. If patients are more involved in the initial decision to pursue coaching, this could help their motivation and plausibly lead to more sustained engagement.
The higher likelihood of having had a COPD diagnosis for 6-12 months rather than 10+ years among coaching users vs non-users may appear puzzling. Possibly, Veterans with a more recent COPD diagnosis were also newer to the VA; as such, they may have discovered Whole Health through new patient orientation. If that is the case, it is both an encouraging sign that new VA patients are getting connected to coaching and a cause for reflection on whether special strategies are needed to introduce patients who have been in the VA system for years to Whole Health and coaching, in particular.
Finally, the finding that the number of prior COPD-related hospitalizations was not a significant predictor of coaching use may indicate an underexplored referral pathway. Veterans who had recently undergone a COPD-related hospitalization may benefit from being connected to coaching as a source of support before or immediately after discharge. Such efforts could emulate the approach of a recent pilot study of a post-discharge community health worker intervention for patients with COPD (which included coaching components). 53 Healthcare providers involved in managing post-discharge care for Veterans with COPD may need additional education to better leverage this promising service for their patients.
Health promotion research and practice would be enriched if future research explored demographic and clinical predictors of coaching utilization among patients with COPD in other health systems, as well as among other patient populations in VA and beyond, similarly identifying both the emerging/established pathways for connecting to coaching, as well as underutilized opportunities.
Limitations
Due to the use of EHR data, we are unable to account for determinants of coaching use that can only be evaluated via survey and interview methods (eg, social support, patient interest). Our inclusion criterion of 3+ healthcare visits with a COPD diagnostic code over a year may have resulted in only Veterans with sustained engagement in VA care being included in the dataset. The use of EHR data to identify COPD diagnosis may have resulted in false positives and/or false negatives. As we did not account for pre-study period coaching use, utilization of coaching among Veterans with COPD may be higher than our findings suggest. Conversely, we may have overestimated the rate of coaching use in our cohort, as we operationalized coaching use broadly instead of limiting it to CPT codes. Furthermore, some of the individuals listed as having received a single session may only have received an informational phone call from a coach that was recorded in the EHR as coaching (a practice known to authors from their prior work). Our sample includes an unexpectedly high percentage of Veterans diagnosed with COPD in the previous 6-12 months. It is not immediately clear what might explain this phenomenon. The PACT Act (a law expanding VA benefits for Veterans with a history of toxic environmental exposures), adopted in August 2022, might have played a role. Additionally, the study period (2021-2023) coincided with the COVID-19 pandemic, which undoubtedly affected both accessibility and use of healthcare services. This, in turn, may have impacted the cohort composition, coaching utilization rates, and other factors unaccounted for in this study. Furthermore, as VA’s implementation of coaching was still in relatively early stages at that time, the patterns of use we identified may not reflect the current or future state. Finally, the exclusive use of VA data may have limited the generalizability of our findings to other health systems.
Conclusion
Our findings highlight several key aspects of coaching use among patients with COPD in VA. Fewer than 5% of Veterans with COPD receive coaching, and even fewer receive the recommended dose. Those patients with COPD who do utilize coaching are concentrated at a small number of facilities. Coaching appears to be reaching Veterans with COPD who have complex clinical needs, which is an encouraging sign. The geographic, sociodemographic, and clinical patterns in coaching use indicate that several referral pathways may have emerged to connect Veterans with COPD to coaching; however, opportunities exist to better understand and optimize the existing pathways, as well as to develop new ones. When leveraged fully, coaching will be a powerful tool providing patients with COPD with skills and support for self-management. Lessons learned from this study may inform efforts to optimize implementation of coaching for patients with chronic conditions other than COPD and/or in other health systems, as part of their health promotion efforts. Health and Wellness Coaching is a promising approach to health promotion that has been shown to produce positive outcomes in patients with complex chronic conditions. However, little is known about who uses coaching and how well it is reaching various groups of patients well-positioned to benefit from it. We identified geographic, sociodemographic, and clinical patterns and predictors of coaching utilization among a large, high-risk population – patients with COPD receiving care in the U.S. Veterans Health Administration. Health systems may benefit from our suggestions on identifying, strengthening, and diversifying pathways through which patients with complex chronic conditions get connected to coaching.So What? (Implications for Health Promotion Practitioners and Researchers)
What Is Already Known on This Topic?
What Does This Article Add?
What Are the Implications for Health Promotion Practice or Research?
Supplemental Material
Suppplemental Material - Patterns and Predictors of Health and Wellness Coaching Use Among Patients With Chronic Obstructive Pulmonary Disease Receiving Care From the United States Veterans Health Administration
Suppplemental Material for Patterns and Predictors of Health and Wellness Coaching Use Among Patients With Chronic Obstructive Pulmonary Disease Receiving Care From the United States Veterans Health Administration by Ekaterina Anderson, Renda Soylemez Wiener, Alexandre Vilela Braga, Makayla Dones, Christian D. Helfrich, Justeen Hyde, Marla Clayman, Seppo T. Rinne, Barbara G. Bokhour, Steven Zeliadt in American Journal of Health Promotion
Supplemental Material
Suppplemental Material - Patterns and Predictors of Health and Wellness Coaching Use Among Patients With Chronic Obstructive Pulmonary Disease Receiving Care From the United States Veterans Health Administration
Suppplemental Material for Patterns and Predictors of Health and Wellness Coaching Use Among Patients With Chronic Obstructive Pulmonary Disease Receiving Care From the United States Veterans Health Administration by Ekaterina Anderson, Renda Soylemez Wiener, Alexandre Vilela Braga, Makayla Dones, Christian D. Helfrich, Justeen Hyde, Marla Clayman, Seppo T. Rinne, Barbara G. Bokhour, Steven Zeliadt in American Journal of Health Promotion
Footnotes
Acknowledgments
The contents of this paper do not represent the views of the U.S. Department of Veterans Affairs or the United States Government. This work was supported by Dr Ekaterina Anderson’s Career Development Award # IK2HX003538-01A1 from the United States (U.S.) Department of Veterans Affairs Health Services Research & Development Service. This material is the result of work supported with resources and the use of facilities at the VA Bedford Healthcare System. An earlier version of these findings was presented at the 2025 International Congress on Integrative Medicine and Health (ICIMH) in Seattle, WA (March 5-7, 2025).
Ethical Considerations
This work is part of the study “Optimizing the Implementation of Health and Wellness Coaching for Veterans with COPD” which was approved by the VA Bedford Healthcare System’s Institutional Review Board.
Author Contributions
EA – Conceptualization, Data curation, Funding acquisition, Investigation, Methodology, Project Administration, Writing – original draft, Writing – review & editing; RSW – Methodology, Supervision, Writing – original draft, Writing – review & editing; AVB – Data curation, Formal analysis, Methodology, Software, Visualization, Writing – original draft, Writing – review & editing; MD – Project administration, Writing – original draft, Writing – review & editing; CDH – Supervision, Methodology, Writing – original draft, Writing – review & editing; JH – Supervision, Methodology, Writing – original draft, Writing – review & editing; MC - Methodology, Writing – original draft, Writing – review & editing; STR - Methodology, Writing – original draft, Writing – review & editing; BGB - Supervision, Methodology, Writing – original draft, Writing – review & editing; SZ - Supervision, Formal analysis, Methodology, Writing – original draft, Writing – review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Dr Ekaterina Anderson’s Career Development Award # IK2HX003538-01A1 from the United States (U.S.) Department of Veterans Affairs Health Services Research & Development Service.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Due to regulatory restrictions on VA data, the dataset will not be shared.
Supplemental Material
Supplemental material for this article is available online.