
Abstract
Purpose
To describe acceptability, feasibility, and preliminary effectiveness of a community-based weight management program for overweight/obese Latino children in immigrant families.
Design
Mixed methods evaluation of an exploratory single-arm pragmatic intervention trial.
Setting
Community sites in Maryland and Colorado.
Sample
Latino immigrant families with 5-12-year-old overweight/obese children with 93 participants (39 index children, their parents and siblings).
Intervention
Community Active and Healthy Families, an adaptation of an evidence- and behavioral-theory based, culturally tailored weight management program delivered in Spanish.
Measures
(1) Height and weight; (2) Surveys of sociodemographics, diet, and physical activity (PA) and (3) Parent/child interviews.
Analysis
(1) Pre and post means, standard deviations, differences in means and the P-value of the difference. (2) Thematic analysis of interviews.
Results
Mean index child age was 9.8 years. Mean change in %BMIp95 was −2.24 (7.49), P = 0.12. Families attended a mean of 4.5/8 program sessions. Interviews with 15 parents and 5 children demonstrated program content was acceptable, and both parent/child respondents reported liking the hands-on learning activities and child PA time. Parents reported making some recommended dietary changes and increased physical activity via family outings. Barriers to change included fresh food costs, child diet preferences and time.
Conclusion
Our evaluation demonstrated a preliminary signal of effectiveness, acceptability and feasibility of Community Active and Healthy Families demonstrating readiness for a larger-scale implementation and effectiveness trial.
Keywords
Introduction
Childhood obesity is a risk factor for adult cardiovascular disease the leading cause of death in the United States (US).1,2 One in four children in the US is Latino and Latino children have among the highest childhood obesity rates of any racial/ethnic group.3–5 Comprising half of the US Latino child population, US-born Latino children of immigrant parents experience higher obesity rates than immigrant Latino children or those with US-born parents.6–8 Current guidelines recommend referral of children with obesity to an intensive weight management program to support behavior changes and decreases in body mass index (BMI).9,10 Intensive programs are limited in number, typically found in clinical settings, and frequently not feasible for Latino immigrant families.11,12 Sustaining participation of Latino immigrant families in intensive community-based weight management programs has been difficult due to the time commitment required and cultural and language barriers.13,14 Reducing obesity disparities for Latino children in immigrant families requires the development of evidence-based obesity treatment programs that are tailored to their sociocultural needs and delivered at a feasible intensity.
Active and Healthy Families (AHF) is a weight management intervention specifically designed for Latino immigrant families with demonstrated effectiveness in reducing child BMI. 15 AHF was designed in California with partner input to generate specific tailoring for Latino immigrant families including: family dynamics, food preferences and cultural perceptions. We subsequently engaged community members in adapting AHF through photovoice 16 and through intervention-mapping adapt with a Partnership Network that included Latino immigrant families, community leaders and healthcare delivery and policy experts.17,18 Major adaptations included a change to delivery in a community setting with lower-cost and fewer bilingual facilitators, changes intended to improve delivery fit and likelihood of adoption. Community-AHF retains the content of the original intervention with its focus on family diet and physical activity (PA) while equipping parents with skills to motivate behavior change, set limits, and manage general and immigration-associated stress. Initial piloting of the adapted intervention in Baltimore, MD demonstrated lower post-intervention BMI in participants than EHR-matched controls. 19 In this study, we implemented Community-AHF at 2 sites and evaluated the acceptability, feasibility, and preliminary effectiveness at reducing child BMI of Community-AHF using a mixed methods approach.
Methods
Study Population and Design
We conducted a single-arm exploratory intervention trial evaluated using quantitative and qualitative methods to provide a comprehensive picture of participant experiences and outcomes to inform future hypotheses and large-scale hybrid implementation/effectiveness research. This pre-post evaluation of Community-AHF was conducted at 2 study sites, Aurora, Colorado and Baltimore, Maryland. Participating families were recruited via referral from their primary care provider at academic-based general pediatrics clinics (both sites) or community-based recruitment at a Latino immigrant-serving family resource center and nearby elementary schools (Colorado only). Inclusion criteria were: child age 5-12 years, child BMI ≥85th percentile for age and sex, and parent/caregiver (hereafter parent) self-identification as foreign-born, Latino/Hispanic with a primary language of Spanish. Exclusion criteria were a child health condition that prevents diet modification or engaging in physical activity.
Following referral, potential participants were called by a bilingual (English/Spanish) study team member to describe the program and invite the family to participate. The staff member consented eligible and interested parents by reading aloud the Spanish-language consent form, answering questions, and ascertaining understanding. Children ≥7 years completed an assent process in conjunction with the parental consent. Participants recruited at community sites were assessed in person for eligibility, including measurement of height/weight and calculation of child BMI, followed by completion of the consent and assent process. Study sample size was determined based on funding constraints with a 2-month timeline for recruitment and maximum intervention cohort size of 13 index children with a maximum of 2 cohorts per site. Figure 1 displays information on sample recruitment and retention. The Colorado Multiple Institutional Review Board approved this study and served as the single-site IRB. The study is registered at ClinicalTrials.gov (NCT04414553). Study participant tracking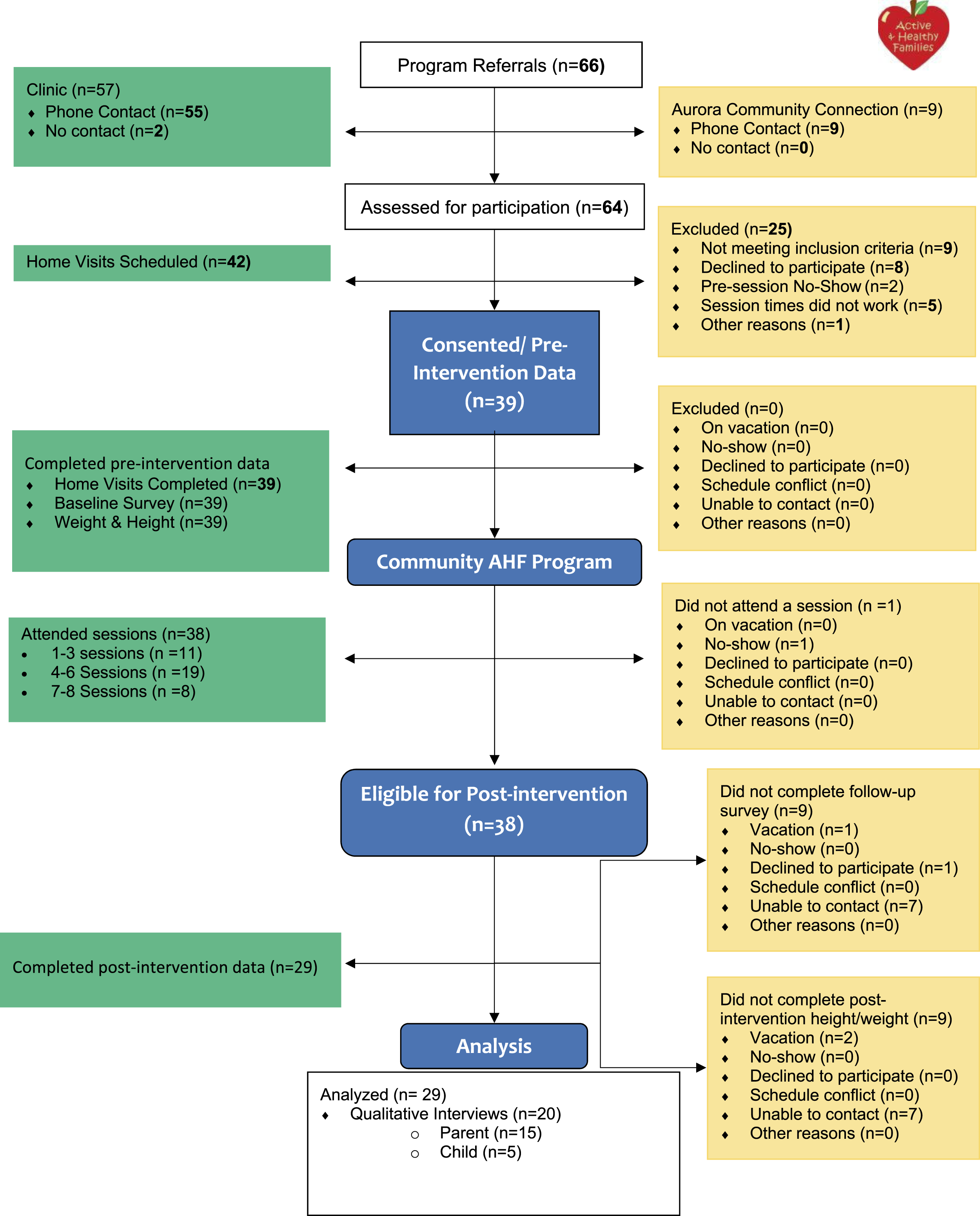
Intervention
Community-AHF is a 10-month intervention with 20 contact hours (16 during the active phase, 4 during the maintenance phase). A priori, this trial only included the active phase of the intervention occurring from March-June 2023 due to the time constraints of the funding. AHF, the evidence-based intervention from which Community-AHF was adapted, also evaluated effectiveness following the 4-month active phase. 15
Community-AHF Active Phase (4 months)
Participants attend eight 90-minute group education sessions every 2 weeks at a community site (eg, church, recreation center) co-facilitated by a trained bilingual/bicultural registered nurse and a community health worker (CHW). A parent must accompany each index child to sessions; additional parents and siblings of the index child may attend. Each session follows a curriculum with specific objectives that includes hands-on activities and breakout groups for children. At each session, participants receive take-home materials to facilitate behavior change. Participants also complete 7 CHW coaching calls (15-20 minutes) during weeks without a group session.
The curriculum provides practical information and demonstrations to increase knowledge and perceived importance of healthy diet and PA practices, skill building in problem-solving and positive parenting to overcome barriers to behavior change at the child and family-level, PA, and parent-only discussions to assist parents in managing stressors and social determinants of health (SDOH) barriers to healthy weight.
Training for Community-AHF facilitators occurs via the curriculum manual. The manual includes checklists for sessions activities to promote fidelity. In this study the facilitators at the Maryland site had been previously trained and provided in-person training to the Colorado facilitators using the curriculum manual. At least half of sessions at both sites were observed by study staff using the sessions checklists to guide observations and feedback.
Community-AHF Maintenance Phase (6 months-Not Implemented or Evaluated in This Study)
Participants complete monthly 15-20 minute coaching calls and attend a graduation ceremony.
Data Collection
Pre- (February/March 2023) and post-intervention (June/July 2023) data collection occurred in the participant’s home and included a survey assessing child and family sociodemographic characteristics, child lifestyle behaviors (diet, PA, sleep and screen media use) and parent stress and self-efficacy for promoting healthy child weight as well as child anthropometric measurements. Surveys were administered via guided oral administration by an English/Spanish bilingual research staff member owing to a high risk of limited literacy in this study population. 20 A small number of families completed some or all of the survey by phone or had child anthropometrics measurements completed at the intervention site owing to scheduling challenges. The research staff member completed anthropometric measurements by twice measuring height to the nearest 0.1 cm and weight (light clothing, no shoes) to the nearest 0.1 kg using stadiometers (Hopkins Road Rod) and portable digital scales (Seca 874).
A subset of parents (Spanish-language interview) and children (English-language interview) age 9-12 years also completed post-intervention interviews to explore behavior changes made, facilitators and barriers to change and intervention acceptability and feasibility. We conducted purposive sampling across intervention site, child age, and family intervention engagement (Low-attended 0-2 sessions, moderate-attended 3-5 sessions, high engagement-attended >5 sessions) and concluded interviews once no new program assessments or behavior change topics emerged. Age-eligible children were invited to participate in an interview following the corresponding parent interview. Interviews were conducted by one of 2 English/Spanish bilingual, bicultural research staff by phone, Zoom or at the family’s home based on their preference. Interviewers had not participated in any other study activities to decrease social desirability bias. Parent interviews lasted 45-60 minutes and child interviews lasted 15-30 minutes. Digital interview recordings were transcribed and translated (as applicable) by a commercial transcription company and de-identified prior to coding. Parent interview transcripts included both the original Spanish-language transcript and English translation to allow for coding/analysis in the original language. Participants received $50 in Colorado and $75 in Maryland for pre- and post-intervention survey/measurements, $50 for a parent interview, and $25 for a child interview. Survey remuneration was lower in Colorado due to institution-specific gift card restrictions.
Outcome Measures
Our primary outcome was change in age- and sex-specific BMI expressed as percent of the 95th percentile (%BMIp95) based on Centers for Disease Control’s 2000 growth charts. 21 %BMIp95 is recommended in longitudinal studies due to constraints of BMI z-scores among children with severe obesity.22–24 Our diet-related secondary outcomes were changes in the domains of sugar-sweetened beverages, savory junk food, fast food, fruits and vegetables based on questions from the Texas School Physical Activity and Nutrition Project (SPAN) and converted into diet risk categories based on dietary guidelines and in a format shown to be align with patient preferences.25–27 Additional secondary outcomes were changes in parent-reported days in the past week in which their child was physically active for ≥60 minutes, screen media use and nighttime sleep duration, and child obstructive sleep apnea risk (validated 3-item scale). 28 We also assessed change in parent stress (validated 10-item scale) 29 and self-efficacy for promotion of healthy child weight (validated 5-item scale). 30
Sociodemographic Measures
Sociodemographic characteristics included: (1) child age, gender, race/ethnicity, country of origin and insurance status; (2) parent age, gender, race/ethnicity, country of origin, length of time in the US, English proficiency (US Census question), 31 educational attainment, health literacy(validated single question), 32 and employment; and (3) household family structure, income, public benefit use, economic insecurity (validated single question) 33 and food insecurity (Hunger Vital Sign).34,35
Analysis
Quantitative Analysis
We conducted within-individual analyses for each outcome of interest. We calculated pre and post means, standard deviations, differences in means and the P-value of the difference. For outcomes analyses, we analyzed only participants who contributed pre and post measures to avoid biases that can occur when analyses are conducted with all available data. Analyses that examined characteristics by site included all available data. All statistical analyses were conducted using R (nlme package). 36
Qualitative Analysis
Coding and thematic analysis were completed by four study team members (LRD, SGH, IPC and JVG) using Atlas.ti (Scientific Software Development GmbH, Berlin, Germany). We developed a preliminary codebook using concepts in the interview guide related to acceptability, participation feasibility and strengths and challenges implementing behavior changes to promote healthy child weight. We then employed a mixed inductive and deductive strategy to develop additional codes based on topics that emerged from the data. The first four parent transcripts were coded by all coders to compare, reconcile and reach consensus on code definition and consistent application by all coders. The remaining 11 parent transcripts were divided between three of the study team members and each transcript was coded by one coder. Child interviews had a separate codebook owing to a distinct interview guide to be appropriate in length and content for children though the same broad topics were covered, when applicable the same codes as parent interviews were retained. Coding followed the same process as parent interviews with one transcript coded by all coders and the remaining four transcripts coded by one coder. We completed code queries to summarize and explore the data and compare parent/child opinions. Member checking occurred via sharing preliminary findings with Community-AHF staff and the Colorado community site advisory board who provided feedback on and refined themes and endorsed the overall results.
We used the STROBE and SRQR reporting guidelines to draft this manuscript, and the STROBE and SRQR reporting checklists when editing; both are included as Supplemental Materials.
Results
Quantitative Results
Sociodemographic Characteristics of Families Participating in Community-AHF (n = 39 Families)
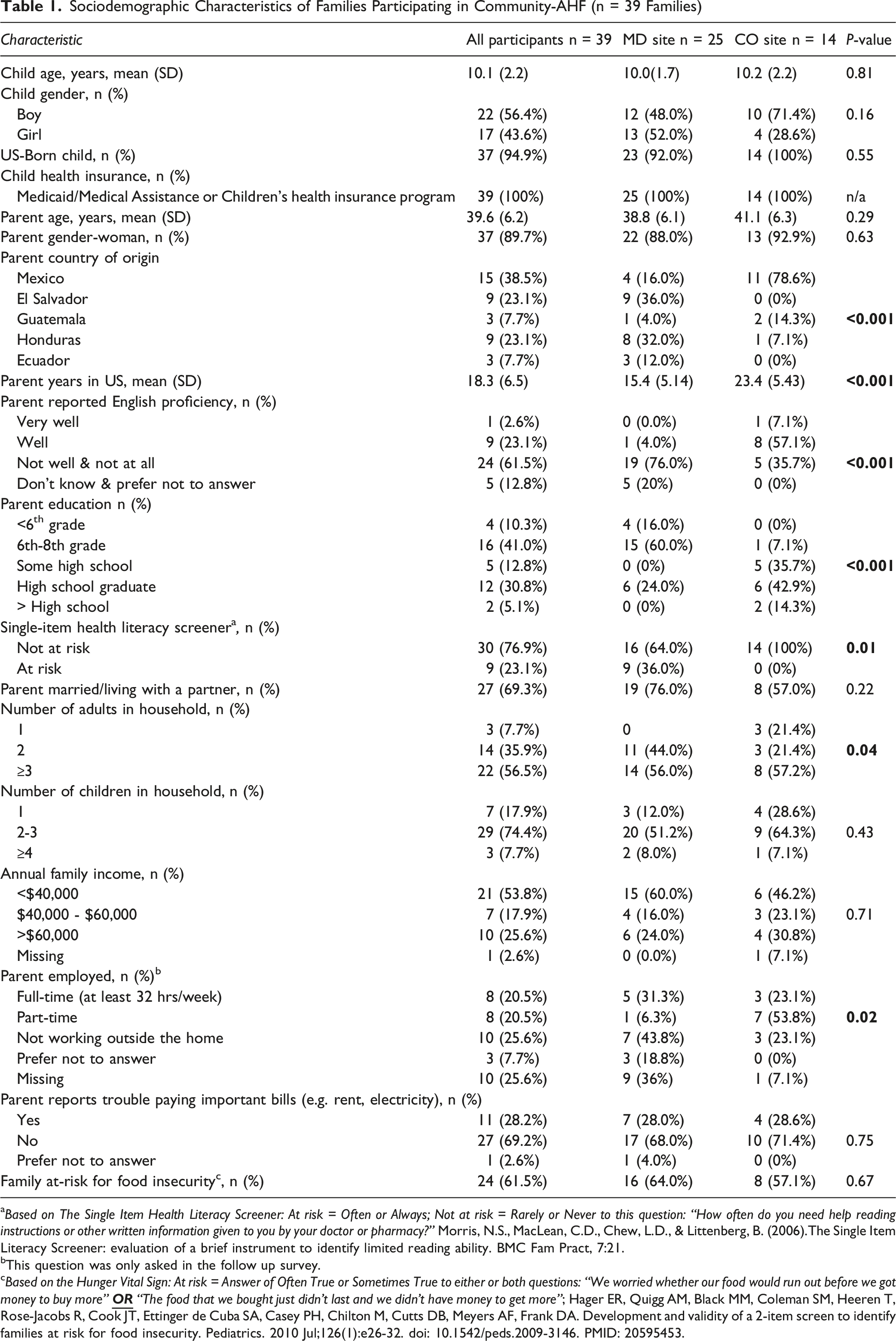
aBased on The Single Item Health Literacy Screener: At risk = Often or Always; Not at risk = Rarely or Never to this question: “How often do you need help reading instructions or other written information given to you by your doctor or pharmacy?” Morris, N.S., MacLean, C.D., Chew, L.D., & Littenberg, B. (2006).The Single Item Literacy Screener: evaluation of a brief instrument to identify limited reading ability. BMC Fam Pract, 7:21.
bThis question was only asked in the follow up survey.
cBased on the Hunger Vital Sign: At risk = Answer of Often True or Sometimes True to either or both questions: “We worried whether our food would run out before we got money to buy more”
Weight and BMI Characteristics of Index Children Participating in Community-AHF (n = 39)
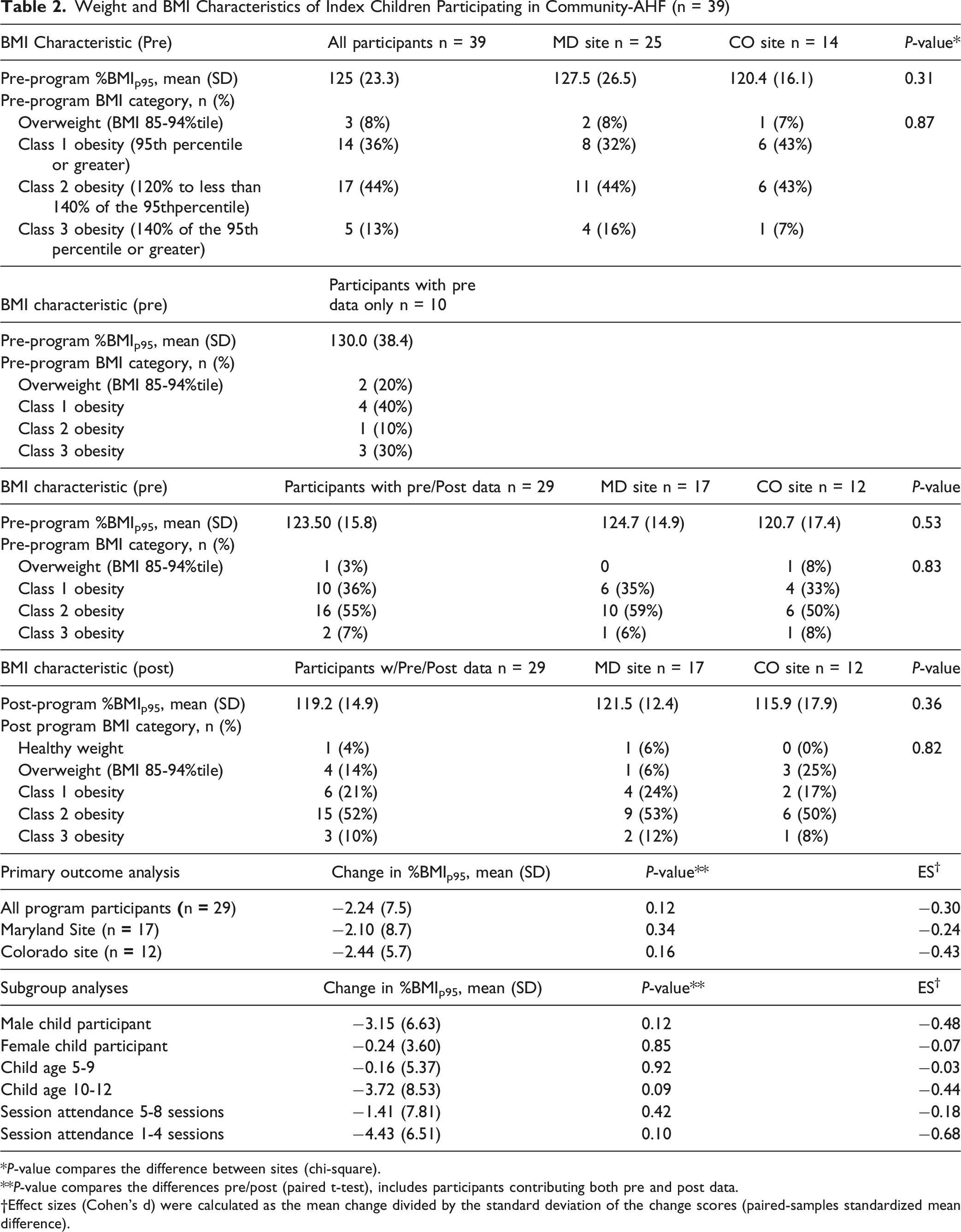
*P-value compares the difference between sites (chi-square).
**P-value compares the differences pre/post (paired t-test), includes participants contributing both pre and post data.
†Effect sizes (Cohen’s d) were calculated as the mean change divided by the standard deviation of the change scores (paired-samples standardized mean difference).
Pre/post Changes in Secondary Outcomes for Index Parent and Child Participating in Community-AHF
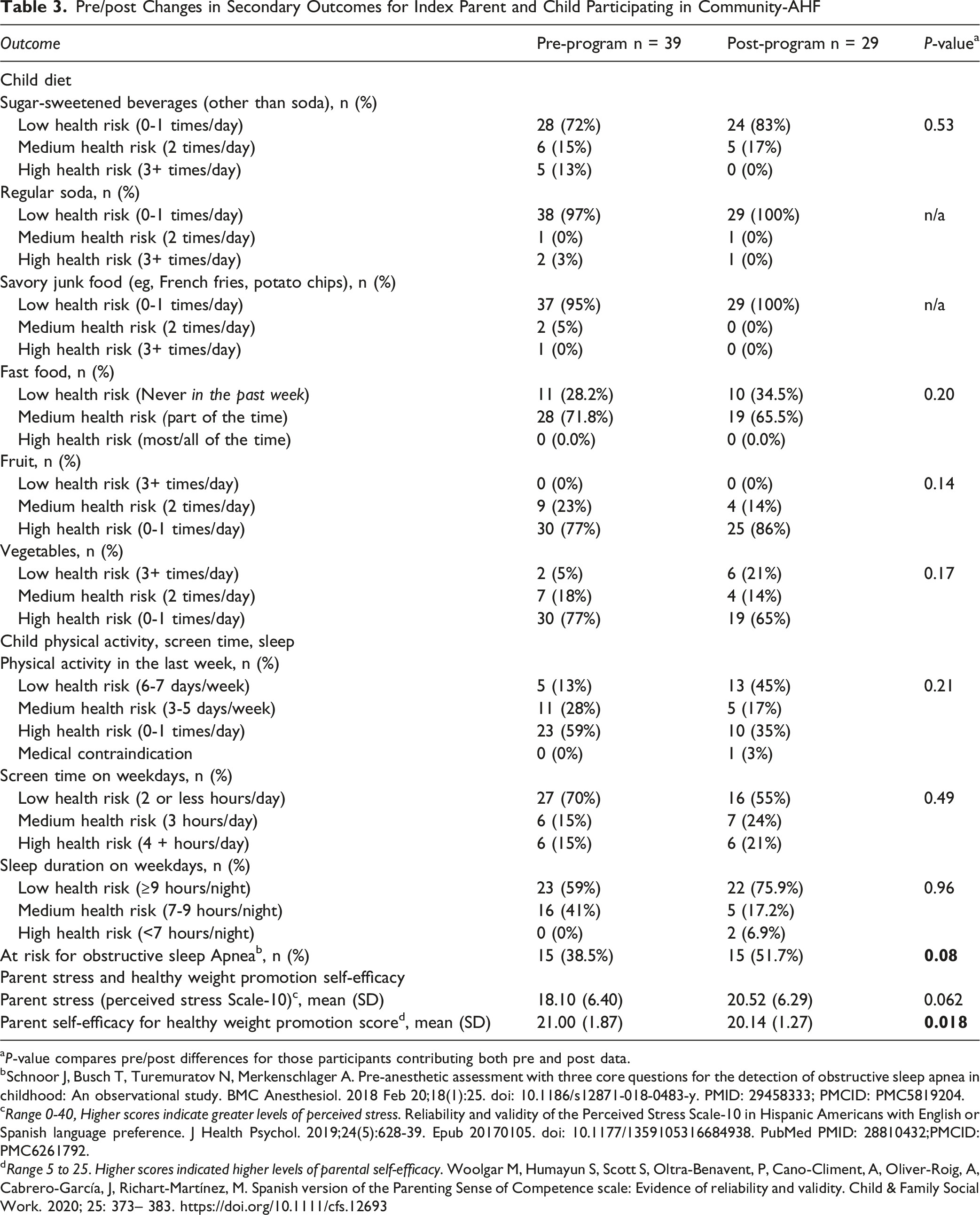
aP-value compares pre/post differences for those participants contributing both pre and post data.
bSchnoor J, Busch T, Turemuratov N, Merkenschlager A. Pre-anesthetic assessment with three core questions for the detection of obstructive sleep apnea in childhood: An observational study. BMC Anesthesiol. 2018 Feb 20;18(1):25. doi: 10.1186/s12871-018-0483-y. PMID: 29458333; PMCID: PMC5819204.
cRange 0-40, Higher scores indicate greater levels of perceived stress. Reliability and validity of the Perceived Stress Scale-10 in Hispanic Americans with English or Spanish language preference. J Health Psychol. 2019;24(5):628-39. Epub 20170105. doi: 10.1177/1359105316684938. PubMed PMID: 28810432;PMCID: PMC6261792.
dRange 5 to 25. Higher scores indicated higher levels of parental self-efficacy. Woolgar M, Humayun S, Scott S, Oltra-Benavent, P, Cano-Climent, A, Oliver-Roig, A, Cabrero-García, J, Richart-Martínez, M. Spanish version of the Parenting Sense of Competence scale: Evidence of reliability and validity. Child & Family Social Work. 2020; 25: 373– 383. https://doi.org/10.1111/cfs.12693
Qualitative Results
Example Quotes From Parent/Child Follow up Interviews
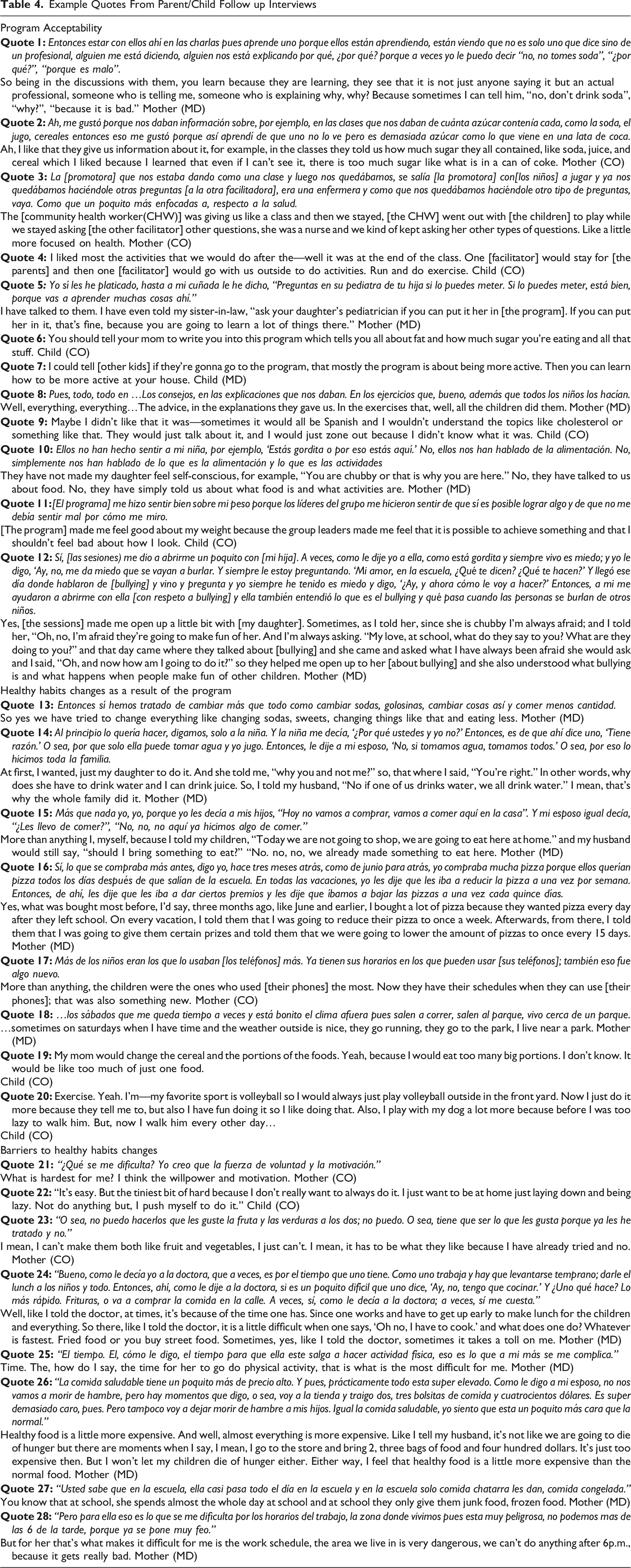
When asked what was most helpful about the program, most participants cited some aspect of the healthy habits’ curriculum; many cited several aspects of the curriculum as most helpful (Quote 8). No part of the curriculum emerged as most helpful across participants. Regarding recommended changes, most participants focused on logistical aspects (eg, session times) not intervention content. However, some participants provided feedback that the children did not always understand the session learning content delivered in Spanish and recommended having the group parent/child learning content available in both English and Spanish (Quote 9). No parent or child interviewed reported a negative impact on child self-esteem. In fact, many participants reported that the program had a positive impact on self-esteem (Quote 10, 11). Some participants expressed appreciation for the socio-emotional content focused on positive parenting approaches to behavior change and for child content focused on bullying (Quote 12).
Families reported many efforts at home to implement program recommendations. Parent participants reported making changes to meal content and portions, sugary drinks, PA, fruits and vegetables consumption and reported that it was important for changes to apply to the entire family (Quotes 13,14). In most cases, the mother led these changes, particularly when it came to meal planning and choosing healthier options. Parents reported using strategies such as incorporating new vegetables into the meal (pureeing them and adding them to dishes) or changing to whole grains without alerting their children. Several also reported diluting juices with water or limiting the amount of sugary drinks and junk food they were buying. Some incorporated more naturally flavored water like hibiscus or lemon water. There were also several mentions of changing sugary cereals to healthier options. Parents adopted changes in junk food consumption by being more aware of what groceries they were buying, reading labels and cooking more at home to try to avoid eating out or buying fast food (Quotes 15,16). Some started to buy smaller portions of foods such as mini drinks or snacks to limit the amount kids were consuming. Some changes were met with resistance; one mother commented that she had to lock up all the unhealthy snacks so the kids did not have access to them.
Regarding physical activity, a few parent participants also commented on attempts to reduce screen time to encourage their children to be more active (Quote 17). Many families also reported attempting to increase PA by encouraging the children to do more activity outside while at home or taking more family walks or trips to the park (Quote 18).
Youth participants shared changes that were implemented at home in their diet and PA. All youth reported implementing more PA into their routines at home. Changes in their diet included changing cereals and breads for healthier alternatives, increasing their fruit and vegetable consumption, reducing portion size and decreasing sugary beverage consumption (Quote 19). A few youth provided examples of the exercises they were practicing at home; one mentioned they were riding their bike every day and another one mentioned using the TV to follow along dances and sing. Some of them had already been involved in sports such as soccer and volleyball, but participating in the program encouraged them to exercise more (Quote 20). Overall, the youth were excited to engage in more PA after participating in the program and noticed the changes that their parents were making in their food.
Though families reported attempting to make changes recommended by the program, they also reported many barriers to making and sustaining change. Almost all parents mentioned that barriers to implementing healthier food into their diet were attributed to disliking the taste of healthier foods, such as brown rice. Several parents and youth commented that they struggled with the internal motivation needed to make changes and parents reported that they struggled to get their children to cooperate with changes they desired to make in the family (Quotes 21-23). Others felt that their family lacked the routines and structures needed to sustain changes.
However, many barriers were beyond the family’s control. Parents expressed that work and childcare responsibilities did not leave them enough time to implement changes such as cooking healthy food as it takes longer for them to prepare and that the cost of healthy food made it difficult to purchase these foods to incorporate in their diet (Quotes 24-26). Some mothers reported they struggled to implement changes because they lacked sufficient support or help from their husbands. Additional external factors reported by families included poor school lunch quality, neighborhood safety concerns, lack of neighborhood resources (eg, recreation centers, sidewalks), and weather conditions (eg, winter weather, poor air quality) (Quotes 27, 28).
Discussion
Our mixed methods evaluation of a community-based adaptation of an evidence-based weight management program demonstrated that content was acceptable and well-liked. Changes in %BMIp95 trended in a favorable direction, while changes in diet and other healthy behaviors were mixed. Interviews demonstrated that families felt sessions were feasible to attend and that families attempted multiple changes in the household but faced barriers sustaining changes due to food preferences, healthy food affordability and challenges maintaining new routines and structures. These barriers may have contributed to our finding of a decrease in parent self-efficacy for healthy weight promotion pre/post participation. This finding was unexpected but was also reflected in qualitative findings in which families reported difficulties sustaining behavior change due to cost, time or child taste preferences. The findings from this exploratory trial generally indicate that the program is a promising tool to address child overweight/obesity among Latino children in immigrant families and that a larger-scale evaluation of the program is warranted and give us insights that will help guide such a larger intervention.
Though we identified barriers to sustaining behavior changes, our findings demonstrate a potential signal of a clinically relevant reduction in BMI. Although a clinically meaningful weight loss for prepubertal children, who comprised most of the children in our study, has not been definitively established, the available data show that modest BMI reductions (BMIz reduction of <0.1 units) are associated with an improvement in cardiovascular risk factors and obesity-related comorbidities which may be clinically important. 37 In our study, %BMIp95 decreased in 51.7% of children; and the mean change in %BMIp95 of −2.24 met the threshold for modest reductions. A reduction of 5 percentage points in%BMIp95 is gaining traction as the threshold for clinically significant change. 38 This was achieved in 21% of our participants. Our %BMIp95 change is consistent with findings from similar efforts. In a weight management intervention trial, Fiechtner et al compared a health center based-program to a recreation center-based group program and electronic medical record controls. Compared to controls, %BMIp95 decreased by −1.03 (−1.61,-0.45) and by 0.22 (NS) for health center and recreation center participants respectively. 39 Our change in %BMIp95 of −2.24 was greater than that found at 4-6 months after baseline for 6-11 year old participants at sites in the Pediatric Obesity Weight Evaluation Registry (POWER Registry) (−0.29(−1.10 to 0.44)). 38
When comparing across programs, attention must be paid to dose of the weight management intervention. Many children receive low doses of interventions.40,41 In our study, 40% of families attended four (of 8) sessions or fewer. The decrease in %BMIp95 was greater in this group compared with those with higher attendance, though was non-significant in both groups. The intervention dose for the Fiechtner et al trial was even lower at 4 sessions overall in comparison to the 25 intended sessions for recreation center participants. 39 The POWER registry did not publish intervention dose data. Session attendance, thus intervention dose, reflects many factors including competing priorities and concerns and participation cost (time, transportation, loss of work, childcare). Future implementation of Community-AHF should focus on supporting families to attend sessions but the BMI outcome signal in our study may indicate that even a low intervention dose could result in BMI reductions.
In our qualitative work, many families focused on changes that were feasible for them to implement such as reducing sugar-sweetened beverages, portion sizes and screen time and finding opportunities for family PA. Changes to child and household habits and how much change is needed to make a positive impact on child BMI, remain elusive. Mechanism and pathway models for healthy child weight describe numerous interrelated factors under the umbrella of the social ecological model.42,43 Factors include family dynamics and family participation in positive lifestyle changes. Parents serve as ‘agents of change’ for their children through their influence on child diet, PA, screen media use and sleep and through monitoring behaviors, modeling healthy behaviors and determining the characteristics of the home environment.10,44,45 As family systems change over time due to parent changes in jobs, stress or relationships as well as normal child developmental changes, successful strategies may not be sustainable or may need to be adapted to changing family circumstances. The Community-AHF program has curricular activities that provide positive parenting skills and management of parental stress intended to be responsive to changing family circumstances.
Our qualitative findings are also similar to those of other studies exploring Latino families’ perspectives on participating in a weight management program. Across studies families reported that they enjoyed the experience, learned valuable information, attempted changes but faced challenges in implementing and sustaining these changes.46–49 These challenges were likely reflected in the decrease in parental self-efficacy for promoting healthy weight pre/post program. We do not believe this decrease in self-efficacy represents a failure of the intervention, rather it may indicate that through participation parents are more aware of barriers to behavior change at the individua/family and systems level. While more exploration of how weight management participation affects parent self-efficacy is needed, the findings highlight opportunities to adapt Community-AHF to address some of these challenges. For example, focusing on the changes that may be a higher yield may allow families to be more successful in sustaining healthier habits. Our findings suggest that we should increase the focus on reducing sugar sweetened beverages and portion sizes and reduce the focus on increasing whole grains and vegetables as these changes were less palatable to children. Children particularly enjoyed increasing PA, both by themselves and with their family, suggesting that expanding ways to address PA barriers and connecting families to resources to increase PA (eg, free/reduced cost recreation center memberships) may also be beneficial. As with other studies and in our preparatory work for implementing Community-AHF, Latino immigrant families in this study reported the cost and availability of healthy food is a persistent challenge.16,46–49 The Community-AHF curriculum includes information on buying and preparing healthy food on a budget, but the challenge posed by the cost of healthy food cannot be overcome at the individual family level. Sustaining healthy food changes requires that food policies and programs reorient and innovate to increase consistent access to affordable healthy foods.
Policy change is needed in areas beyond the food system to address child obesity. Stressors that families in our study, and across the country, face consistently relate to low-income status. The chronic stress of poverty has myriad negative impacts on parent and child health. 50 We will continue to face a child obesity and chronic health condition epidemic in the US without substantial policy investment in comprehensive support for low-income families. Parents in our study reported many types of stressors negatively impacting healthy lifestyle behavior change including managing costs, neighborhood safety, school bullying and limited time for food preparation. Though the Community-AHF curriculum addresses stress, the stressors parents identified were beyond parents’ locus of control and that of Community-AHF support. There have been mixed results on whether parent stress is associated with child weight status, which likely reflects the complex and changing stressors families face. 51 One study found that positive outliers for healthy weight as compared with overweight among families experiencing similar stress were those families with consistent family routines and able to limit negative health influences of other family members. 52 Using Community-AHF coaching calls to focus on family routines may be a key way to support family changes in the face of their stressors. While this approach may support additional individual family-level changes, complementary policy change is needed to create population-level reductions in child obesity. Despite the need for policy change to increase family supports as part of a comprehensive strategy to reduce child obesity, recent federal legislation represents a disinvestment in support for low-income families. 53
This study has certain limitations. Our study included a relatively small number of families, did not have a control group and retention was 74%, which may have led to random error and bias in the results. Retention was impacted by the program’s timing, in Colorado sessions extended beyond the end of the school year and summer travel plans resulted in non-completion of sessions and study activities by some participants. These participants reported they would have completed sessions and study activities had the program timing been different. Future implementation should schedule program completion prior to the end of the school year for areas where family summer travel to a parent’s country of origin is common. This type of travel was less common at the Maryland site and due to differences in the school calendar more sessions and study activities were completed prior to the end of the school year. Our study also included a relatively small number of child interviews, thus findings from these interviews should be interpreted with caution. However, it is rare to have feedback from youth younger than 13 who are participants in weight management interventions. Findings from child interviews particularly around their enjoyment of increased PA provide a compelling reason to ensure future evaluations capture perspectives of younger youth. Finally, this study did not formally assess child mental health. There are known connections between child mental health, overweight/obesity status and successful behavior change. 10 In our qualitative data families expressed appreciation for the discussion of bullying at school and the connections this has with child mental health. In interviews, parents and children endorsed that the program had a neutral or positive effect on mental health. A formal assessment of child mental health could uncover results that would require immediate action on part of the program and research team and parents. A connection to mental health services in the long term could be beneficial to the child, but it is unclear if limited resources in this community-based program should be spent focused on screening for and responding to mental health concerns.
Conclusion
The findings of our exploratory single-arm trial indicate that Community-AHF is acceptable and feasible for Latino parents and children in different communities, shows promise as a community-based weight management program for Latino families and merits further study in a large-scale trial. Child obesity is a significant public health problem with negative long-term implications for individual health and societal healthcare costs. Nonetheless, solutions to the epidemic of child obesity remain elusive. No single weight-management program will solve the problem, but Community-AHF fills a niche as an introduction to healthy behavior change in a safe and welcoming environment and may increase readiness for participation in additional child, parent or family programs. Family investment in program participation over time may promote sustained behavior change and BMI reduction. Given what we heard from the parent interviews regarding cost and access barriers to healthy food and prevalent parental general and financial stress, we should start to match the responsibility we place on families with societal investment. Our food system must move towards incentives to provide reliable access to fresh, healthy food at an affordable price, and we must expand, not reduce, support for low-income families. The future health of our nation rests on this mutual commitment. Latino children of immigrant families experience some of the highest obesity rates in the U.S. Sustaining participation of Latino immigrant families in the recommended treatment, intensive weight management programs, has been difficult due to the time commitment required and cultural and language barriers. What does this article add? We report that Community Active and Healthy Families, a behavioral-theory based, culturally tailored, Spanish language weight management program delivered at trusted community venues, demonstrates promise as a solution for addressing Latino child obesity disparities. Findings demonstrate that program content was acceptable and well liked and changes in child weight outcomes trended in a favorable direction. A larger-scale pragmatic trial of the Community Active and Healthy Families program is warranted.So What?
What is Already Known on This Topic?
What Does This Article Add?
What are the Implications for Health Promotion Practice or Research?
Supplemental Material
Supplemental Material - Mixed Methods Evaluation of a Community-Based Weight Management Program for Latino Children
Supplemental Material for Mixed Methods Evaluation of a Community-Based Weight Management Program for Latino Children by Lisa Ross DeCamp, Jenifer Valdez-Vormezeele, Ellen Molino, Rashelle Musci, Jonathan Vuillier, Marina Delgado Hernandez, Maria Yessica Marroquin Miranda, Isabella Perea Caicedo, Sandra Garcia-Hernandez, Amy G. Huebschmann, Meredith P. Fort, Darcy A. Thompson, Eliana Perrin, Sarah Polk in American Journal of Health Promotion
Supplemental Material
Supplemental Material - Mixed Methods Evaluation of a Community-Based Weight Management Program for Latino Children
Supplemental Material for Mixed Methods Evaluation of a Community-Based Weight Management Program for Latino Children by Lisa Ross DeCamp, Jenifer Valdez-Vormezeele, Ellen Molino, Rashelle Musci, Jonathan Vuillier, Marina Delgado Hernandez, Maria Yessica Marroquin Miranda, Isabella Perea Caicedo, Sandra Garcia-Hernandez, Amy G. Huebschmann, Meredith P. Fort, Darcy A. Thompson, Eliana Perrin, Sarah Polk in American Journal of Health Promotion
Supplemental Material
Supplemental Material - Mixed Methods Evaluation of a Community-Based Weight Management Program for Latino Children
Supplemental Material for Mixed Methods Evaluation of a Community-Based Weight Management Program for Latino Children by Lisa Ross DeCamp, Jenifer Valdez-Vormezeele, Ellen Molino, Rashelle Musci, Jonathan Vuillier, Marina Delgado Hernandez, Maria Yessica Marroquin Miranda, Isabella Perea Caicedo, Sandra Garcia-Hernandez, Amy G. Huebschmann, Meredith P. Fort, Darcy A. Thompson, Eliana Perrin, Sarah Polk in American Journal of Health Promotion
Footnotes
Acknowledgments
We are grateful for the partnership of Aurora Community Connection in the planning and implementation of Community Active and Healthy Families intervention in Colorado.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the National Institutes of Health/National Heart Lung and Blood Institute, [1R56HL157048-01A1].
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.