
Abstract
Purpose
Worksite health promotion programs (WHPPs) can promote a healthier lifestyle for blue-collar workers, yet their participation is generally low. From a social ecological perspective, this study aims to identify determinants associated with blue-collar workers’ initial WHPP participation.
Design
Observational study.
Setting
A freight transport sector-initiated WHPP in the Netherlands.
Participants
The study sample included 3916 blue-collar workers. Data from 976 white-collar workers were used for comparisons.
Measures
Data were obtained from an online health survey as part of the WHPP. Participation in a follow-up intervention was measured by attendance registration of the first consultation.
Analysis
Associations between determinants and participation were tested, using logistic regression. Interactions of determinants with job group were studied to explore differences in associations with participation between blue- and white-collar workers.
Results
The final multivariable logistic model identified contract security (OR = 2.06), a neutral work-life balance (OR = 1.24), more chronic conditions (OR = 1.67), poorer self-rated health (OR = 2.17), and insufficient sleep (OR = 1.24) as being associated with WHPP participation. The determinants were largely consistent across blue- and white-collar workers. The model showed good fit, but provided little explanatory power (Nagelkerke R2 = .058).
Conclusion
While a sector-initiated WHPP may be able to reach workers not typically reached by employer-based programs, barriers still seem to exist for workers with less secure contracts, poor work-life balance, and fewer health complaints.
Keywords
Purpose
Blue-collar workers face markedly poorer health outcomes compared to the general working population and to white-collar employees. They have a shorter life expectancy and higher prevalence of physical health problems.1-4 Unhealthy lifestyle choices, including smoking, poor diet, lack of physical activity, and inadequate sleep, contribute to these disparities.5-7 While worksite health promotion programs (WHPPs) have been shown to be promising in promoting healthier behaviors and improving health among blue-collar workers,8-11 participation remains lower in this group compared to white-collar workers.12-14
Previous research has provided substantial insight into factors associated with participation among the general workforce (such as gender, education level, shift work, and contract security).12,14-16 However, a recent scoping review on blue-collar workers’ participation highlights that the evidence base is dominated by qualitative studies and that quantitative research remains relatively scarce. 17 Evidence indicates that blue-collar workers are more likely to experience irregular work hours, job insecurity, and limited social support at work. 4 These contextual disparities may restrict both their ability and motivation to participate in WHPPs. 18 Moreover, the aforementioned review highlights that barriers such as shift work and not yet experiencing health complaints are repeatedly identified, but rarely examined within multivariable models or compared across occupational groups.
To address this gap and to guide a more systematic examination of participation patterns, a theoretical framework that explicitly accounts for reach and contextual influences is needed. According to the RE-AIM framework, equitable reach is a key dimension of successful health promotion interventions.19,20 From a social-ecological perspective, participation in WHPPs is not driven solely by personal motivation or health status, but also by contextual factors such as job demands, employment security, and social support at work.21-23 Considering different types of determinants, more specifically intrapersonal, interpersonal and work-related determinants as they are more amenable to change, 23 is therefore essential to understand disparities in WHPP participation and to inform more equitable health promotion strategies.24-26
The Dutch Sector Institute for Transport and Logistics (STL) is a national collaboration between employer organizations and labor unions in the Netherlands that provides a sector-initiated WHPP to improve vitality, work ability, and overall health across the sector. Designed to ensure equal access regardless of company size or employment status, the WHPP operates independently from individual employers. This sector-wide structure may help to overcome barriers typically observed in organization-based programs, such as limited financial or organizational resources, implementation constraints, and concerns about confidentiality.27-29 All employees of affiliated organizations can participate voluntarily, anonymously, and free of charge through the STL platform. 30
The WHPP begins with an online health assessment questionnaire (HAQ) assessing workers’ current health status and lifestyle behaviors. Workers identified as ‘at risk’ (eg, obesity, low work capacity, smoking, or high stress) are invited by a vitality coach for a personal consultation offering tailored lifestyle advice and access to interventions, such as smoking cessation, weight management, or stress reduction programs. Consultations are scheduled at a time and location convenient to the participant.
Studying determinants of participation within this sector-wide context offers an opportunity to examine whether broader, collective approaches to health promotion are successful in engaging groups that are traditionally underrepresented in WHPPs, such as blue-collar workers and employees in small or medium-sized enterprises. These insights can guide the development of tailored and inclusive WHPP offerings and implementation strategies, ensuring that interventions reach those most in need rather than reinforcing existing disparities.
Aim and Research Questions
The aim of this study is to provide insight into which intrapersonal, interpersonal, and work-related characteristics are associated with initial participation in a sector-initiated WHPP among blue-collar workers in the freight transport sector and to explore whether similar or different determinants underlie participation across occupational groups. Adopting a reach-oriented perspective, the social-ecological framework is used to structure determinants across levels, with the contribution lying in the empirical identification of participation characteristics rather than in explaining individual participation decisions.
The research questions are: 1. Which intrapersonal, interpersonal, and work-related determinants are associated with initial WHPP participation in a sector-initiated WHPP among blue-collar workers in freight transport in the Netherlands? 2. Do these determinants show similar or different associations with initial WHPP participation among white-collar workers in the same sector?
Methods
Design
We conducted a secondary analysis on data obtained from the WHPPs online HAQ, examining which determinants were associated with participation in the first follow-up consultation within 1 year. Reporting followed the STROBE checklist for cohort studies (see Supplemental File 1).
Sample
Between 2014 to 2021, 19 564 workers in the freight transport industry completed the HAQ. All participants provided informed consent. Based on the International Standard Classification of Occupations (ISCO), 31 truck drivers, warehouse workers, technicians, cleaners, crane operators, and movers (ISCO codes 1-5) were categorized as “blue-collar” and included in the analysis. Office workers, planners, and managers (ISCO codes 6-9) were categorized as “white-collar”. Their data were used as a reference group for comparative analyses. Respondents who selected “other” as their occupation were classified as “other” and excluded from the analysis.
Measures
Determinants for this study were selected from the online HAQ and included characteristics that were associated with WHPP participation in previous studies.12,15,18,22,32 In line with social-ecological perspectives, they were grouped into intrapersonal, interpersonal, and work-related characteristics. Numerical determinants with the exception of age were categorized.
Intrapersonal Determinants
Respondents were asked to state their gender (“man” or “woman”), age (measured in years), and education level (classified following the International Standard Classification of Education 2011 (ISCED) 33 : “basic education” (ISCED 0-2), “practical education” (ISCED 3-5), or “theoretical education” (ISCED 6-8)). With regard to health, respondents were asked if they had ever been diagnosed with specific chronic diseases. The list, derived from the Work Ability Index (WAI), 34 contained 13 predefined conditions. Respondents were categorized as having “no”, “one”, “two or three”, or “four or more” chronic diseases. Additionally, self-rated health (SRH) was measured by asking respondents to rate their overall health on a 5-point Likert scale (“poor” (=1) to “excellent” (=5)), derived from the Short Form 12 (SF-12). 35 Self-rated sleep involved respondents rating their own sleep quality as sufficiently healthy, with options of “yes” or “no”. Financial concern was assessed with a single item “Are you ever concerned about your financial situation?”. Respondents could answer “no, never”, “yes, sometimes”, or “yes, often”, and were classified into ‘having no financial concerns’ or ‘having often or sometimes financial concerns’.
Interpersonal Determinants
Employee-supervisor relationships and co-worker relationships at work were assessed using scales adapted from the conceptual framework of the VBBA (Questionnaire on the Experience and Evaluation of Work). 36 Internal reliability of each scale was assessed in the present sample. Response categories were “always”, “often”, “sometimes”, and “never”. Employee-supervisor relationships was assessed with five items (α = .85). An example item was “Can you count on your supervisor when you are having a hard time at work?”. Co-worker relationships was assessed using two items: “Do you have conflicts with your co-workers?” and “Is there a pleasant atmosphere between you and your colleagues?” (α = .44).
Work-Related Determinants
Subjects were asked to estimate the size of their company. Estimates were categorized into “micro” (1-9 employees), “small” (10-49 employees), “medium” (50-249 employees), or “large” (≥250 employees) companies, in accordance with European Union definitions. 37 Furthermore, they were asked their type of contract (“permanent”, “temporary contract, permanent likely”, “temporary contract, permanent not likely”, “secondment, on-call employee”), and to indicate if they had irregular working hours (“yes” or “no”). Work pace was assessed using a six-item scale adapted from the conceptual framework of the VBBA. 36 Internal reliability of the scale was assessed in the present sample (α = .85). Response categories were “always”, “often”, “sometimes”, and “never”. An example item was “Do you have to work very fast?”. Work-life balance was assessed using nine items from the Survey Work-home Interaction Nijmegen (SWING) 38 (α = .86, in our sample). An example item was “how often does it occur that it is difficult for you to do your duties at home because you are constantly thinking about your work?”. Scale scores were then classified into “good”, “neutral”, or “poor”.
Financial concern, SRH, and self-rated sleep were measured using single-item indicators to limit respondent burden. Because such measures may reduce reliability, 95% confidence intervals were reported to indicate uncertainty. Of the multi-item scales, only co-worker relationships showed low reliability. The other scales showed good reliabilty.
Participation
Workers identified as ‘at risk’ were invited to meet with a vitality coach. Participation was measured through the coaches’ registration of acceptance of the invitation, and attendance at this first consultation session, resulting in two possible outcomes: “participation” (acceptance and attendance) or “no participation” (no acceptance and/or no attendance).
Analysis
All analyses were performed using SPSS (version 27). Descriptive statistics were first computed, including average and frequencies of intrapersonal, interpersonal and work-related determinants for the total sample of blue-collar workers, as well as separately for participants and non-participants in the follow-up intervention. Characteristics were compared to the reference group of white-collar workers, and differences were assessed using Pearson’s chi-square test and t-test.
Subsequently, binary logistic regression analyses were conducted. ‘Participation’ served as the outcome variable, with intrapersonal, interpersonal, and work-related determinants as independent variables. Age was modeled using linear and quadratic terms to allow for non-linear associations. Each determinant was entered separately adjusted for gender, age, and education level. The association for each determinant with ‘participation’ was tested using a chi-square test, and adjusted odds ratios were calculated.
Next, we applied the purposeful selection of covariates method as described by Hosmer, Lemeshow, and Sturdivant.39,40 Following this method, all covariates were examined, individually and uncontrolled, using univariate logistic regression. Variables with a Wald P-value less than .25 were selected for inclusion in the preliminary multivariable model. These covariates were entered simultaneously into a logistic regression model. Non-significant variables were assessed for confounding based on their impact on the estimated regression coefficients of other variables (a change >20% was considered indicative of confounding). Then, excluded variables were reintroduced one at a time to reassess potential confounding effects. Interaction terms were added and assessed for statistical significance (P < .05). Interaction terms included the confounding variables. Non-significant interactions were removed. We tested for multicollinearity between all independent variables using the Variance Inflation Factor (VIF), with VIF values higher than 2 indicating possible distortions from multicollinearity, and higher than 5 indicating excessive collinearity. 41 The final model was built including all significant main associations and interactions, and evaluated using the Hosmer-Lemeshow goodness-of-fit test, modified for large samples by Nattino et al (using R version 4.5.0.), 42 and Nagelkerke R2.
To explore whether the associations between the identified determinants and participation differed between blue- and white-collar workers, we constructed a multivariable logistic regression model including all determinants retained after the purposeful selection procedure for both groups. Interaction terms between job group (blue-vs white-collar) and each determinant were added to the final main effects model. Additionally, a likelihood ratio test was used to compare the model with and without the interaction terms.
Results
Sample Characteristics
The initial sample for this study consisted of the 4014 blue-collar workers who, based on their answers in the online HAQ, were invited to a follow-up consultation; 998 white-collar workers served as a reference group.
From this initial sample of blue-collar workers, 22 respondents were excluded due to having zero response variance on at least three questionnaire scales, 71 respondents due to missing data on at least one determinant with the exception of company size, and five respondents due to a period of more than one year between completing the HAQ and participating in the consultation. This resulted in a final sample of 3916 blue-collar workers. For company size, a slightly smaller sample (N = 3677) was used for the analyses due to the many missings on this variable.
Sensitivity analysis using student’s t-test indicated no significant differences in terms of age (t = −.612, P = .540) and education level (t = −.014, P = .989) between included and excluded respondents. However, included respondents were more likely to be female (t = −2.521, P = .013).
Most respondents were male (96.3%), with an average of 51.3 years (SD = 12.0) and a basic level of education (53.8%). The number of participants in the initial consultation was 942 (24.1%), and the average time between HAQ and initial consultation ranged from two to 339 days, with an average of 58.4 days (±50.4). All sample characteristics and percentages can be found in Supplemental File 2.
Binary Logistic Regression Analyses With Independent Variables
Associations Between Intrapersonal, Interpersonal, and Work-Related Determinants and Initial WHPP Participation Within a Year After Questionnaire Completion for Blue-Collar Workers, Controlled for Age, Gender, and Education Level (N = 3916)
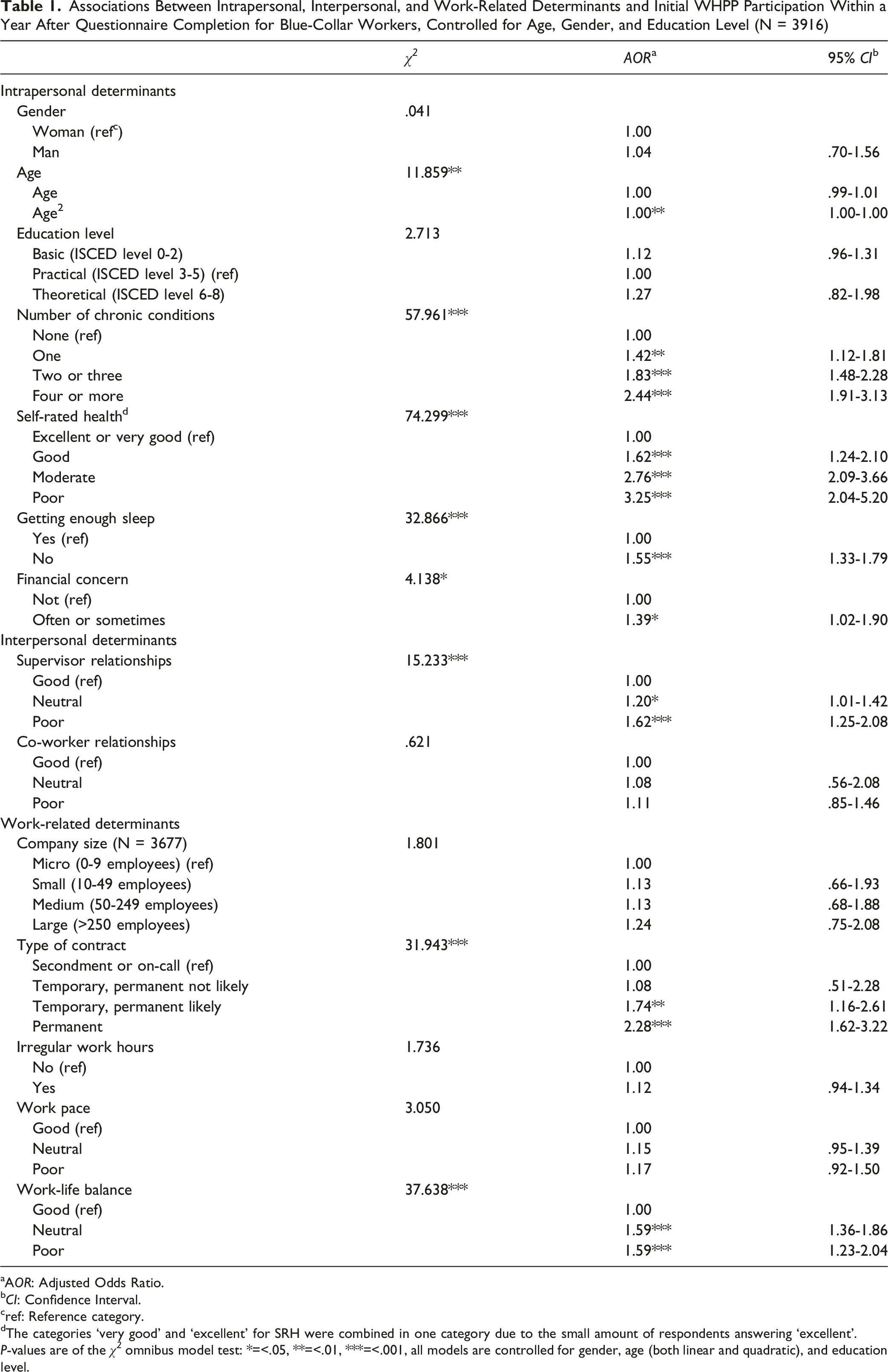
aAOR: Adjusted Odds Ratio.
bCI: Confidence Interval.
cref: Reference category.
dThe categories ‘very good’ and ‘excellent’ for SRH were combined in one category due to the small amount of respondents answering ‘excellent’.
P-values are of the χ 2 omnibus model test: *=<.05, **=<.01, ***=<.001, all models are controlled for gender, age (both linear and quadratic), and education level.
Purposeful Selection of Variables
The purposeful selection of variables resulted in a preliminary final model that was tested for multicollinearity between all significant determinants. The test indicated no problematic correlations between indicators, with all VIF values below 2,ranging from 1.1 to 1.29. The modified Hosmer–Lemeshow goodness-of-fit test indicated no evidence of lack of fit (χ 2 = 13.49, df = 8, P = .098). However, Nagelkerke R2 (.058) showed little explanatory power of the model.
Final Multivariable Model of Determinants Associated With Initial WHPP Participation Within a Year After Questionnaire Completion for Blue-Collar Workers (N = 3916)
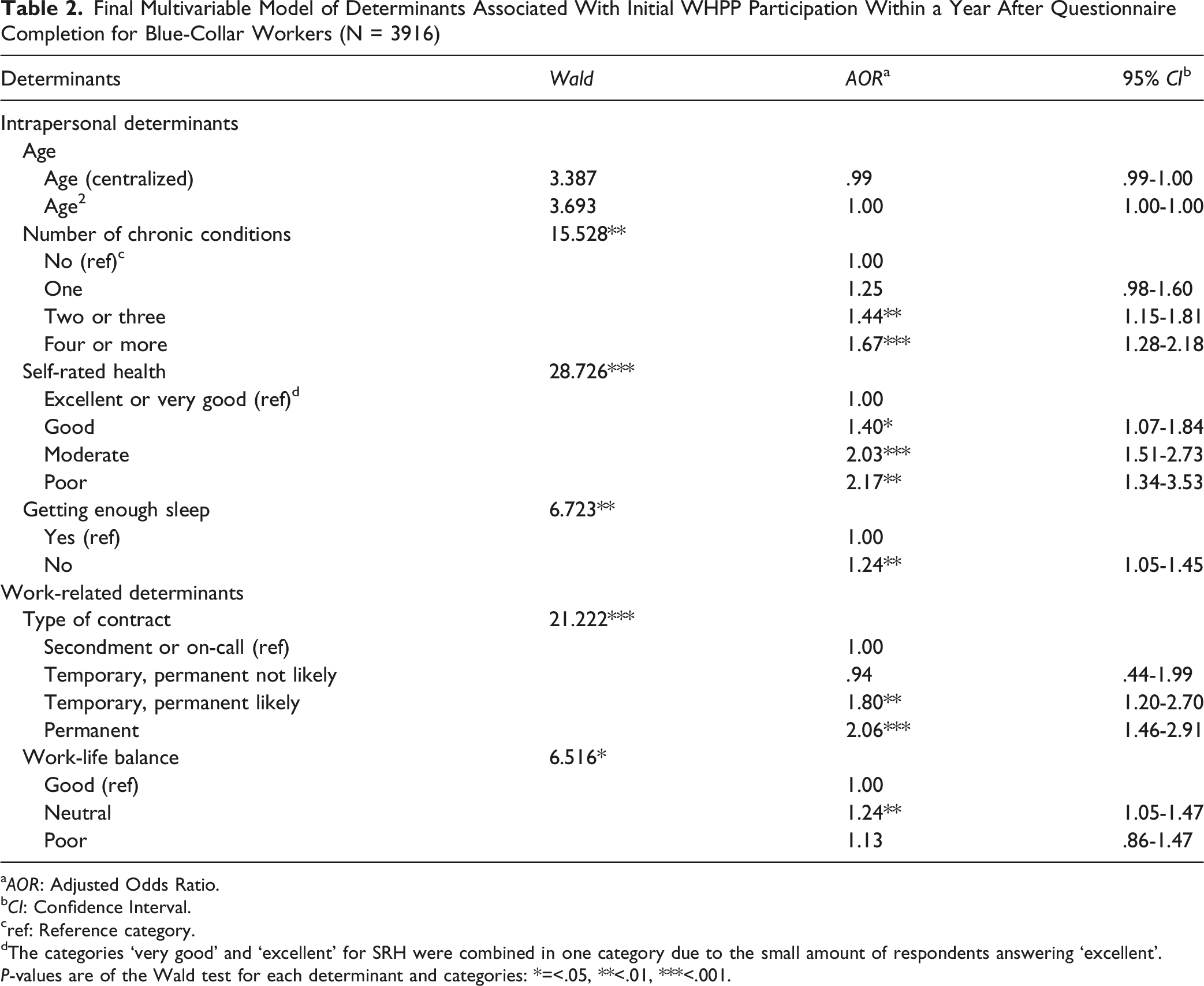
aAOR: Adjusted Odds Ratio.
bCI: Confidence Interval.
cref: Reference category.
dThe categories ‘very good’ and ‘excellent’ for SRH were combined in one category due to the small amount of respondents answering ‘excellent’.
P-values are of the Wald test for each determinant and categories: *=<.05, **<.01, ***<.001.
Comparisons Between Blue- and White-Collar Workers
Pearson’s chi-square tests revealed no significant differences between blue- and white-collar workers regarding initial participation in the follow-up intervention. However, blue-collar workers were generally older, more often male, less educated, worked in smaller firms with less secure contracts and irregular hours, and reported poorer health and more chronic conditions.
Final Multivariable Model of Determinants Associated With Initial WHPP Participation Within a Year After Questionnaire Completion for Both Blue- and White-Collar Workers and the Multivariable Model Including Job Group Interactions (N = 4892)
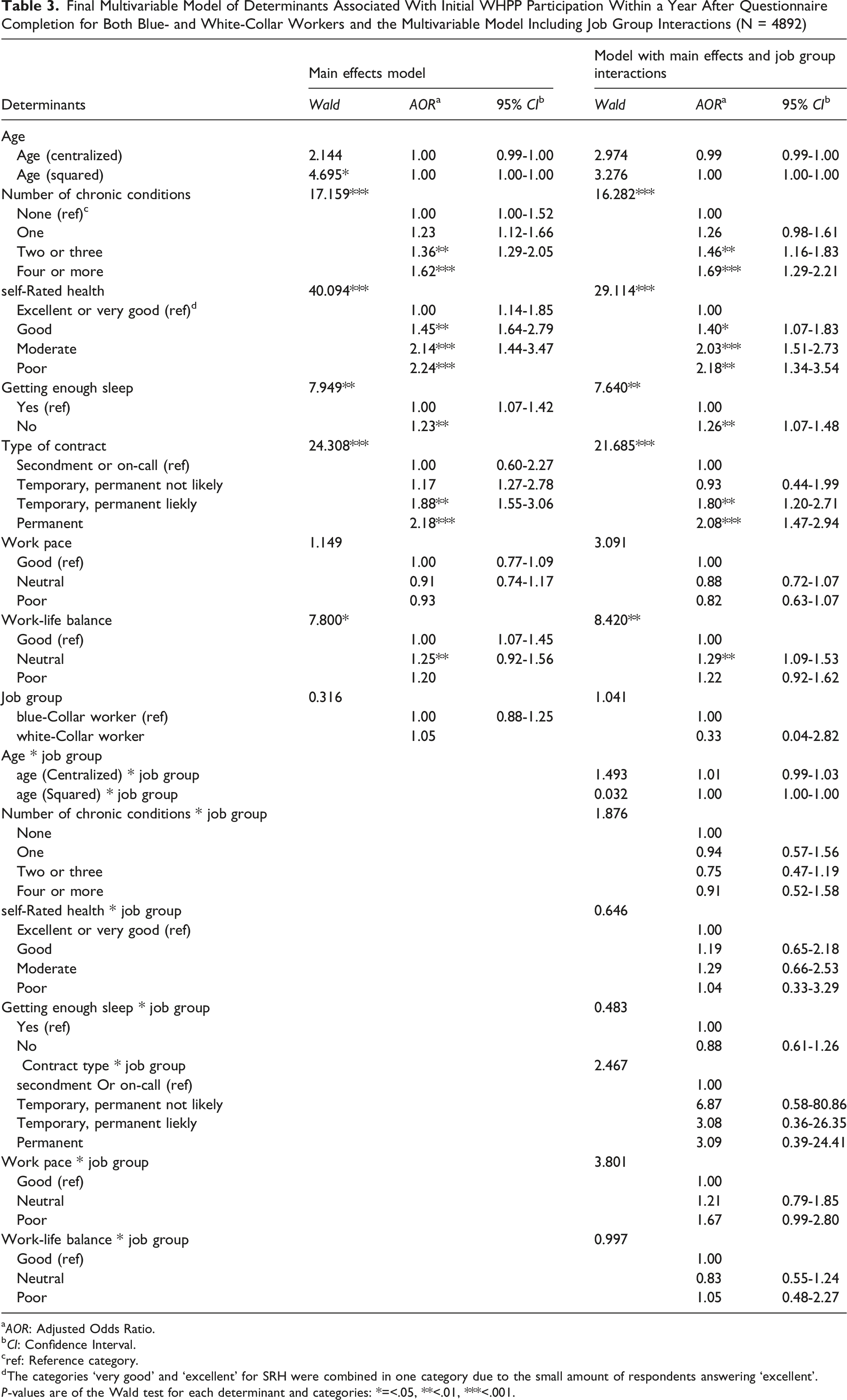
aAOR: Adjusted Odds Ratio.
bCI: Confidence Interval.
cref: Reference category.
dThe categories ‘very good’ and ‘excellent’ for SRH were combined in one category due to the small amount of respondents answering ‘excellent’.
P-values are of the Wald test for each determinant and categories: *=<.05, **<.01, ***<.001.
Discussion
Our findings confirm that, in line with social-ecological models, both intrapersonal and work-related characteristics are significantly associated with blue-collar workers’ participation in WHPPs. Three key findings emerge. First, indicators of poorer health were consistently associated with higher participation. Second, employment security was a strong determinant of participation, with workers in more secure contracts substantially more likely to attend the initial consultation. Third, participation was not associated with several contextual factors commonly reported in employer-based WHPPs, such as company size, irregular working hours, or supervisor relationships.
Health indicators showed clear and consistent links with initial uptake: poorer self-rated health, multiple chronic conditions, and insufficient sleep were each associated with a higher likelihood of attending the consultation. This pattern aligns with previous research17,32 and is in line with the Health Belief Model, 43 which posits that greater perceived susceptibility and severity foster engagement in health-protective behavior. Higher participation among workers reporting a neutral work-life balance compared to those with a good or poor balance suggests that a favorable balance may reduce perceived need to engage, whereas an unfavorable balance may introduce practical barriers such as limited time or energy.
The association between employment security and participation underscores that participation in WHPPs is shaped not only by individual motivation, but also by structural employment conditions. Workers in insecure or on-call contracts may face greater time constraints, uncertainty, or concerns about confidentiality, reducing their willingness or ability to engage, which is consistent with earlier studies.12,15
In contrast to prior literature,12,15,17,22,32 company size, irregular work hours and supervisor relations were not significantly associated with participation in our study. This deviation may reflect the greater flexibility, a broader offer of interventions and more confidentiality in a sector-wide WHPP. Because these mechanisms were not directly measured, these interpretations should be considered hypothesis-generating rather than confirmatory.
Taken together, workers showing signs of health decline and workers enjoying stable employment are most likely to engage, whereas healthier workers and those with insecure contracts or poor work-life balance remain underrepresented. These determinants appear to outweigh both demographic and interpersonal factors. However, overall participation was modest (24.1% in the initial consultation) compared to other WHPPs targeting blue-collar workers. 17 This may reflect the absence of workplace-based social support mechanisms in a sector-initiated WHPP. Peer involvement and collective participation may serve as important motivators, as supported by prior research.23,44
Regarding the second research question, determinants of participation did not differ significantly between occupational groups. Interestingly, while other studies typically report lower participation among blue-collar workers,12-14 our study found no such disparity. This may reflect the well-targeted recruitment strategy, which was specifically designed to engage truck drivers. In addition, opposing influences may be at play, whereby the motivating effect of poorer health is offset by the constraining effect of greater employment insecurity and poorer work-life balance among blue-collar workers in our sample. This finding suggests that while similar factors may underlie WHPP uptake across occupational groups, these factors are unevenly distributed between them.
The low Nagelkerke R2, indicates that the included variables explained only a small share of the variance in participation. Such modest explanatory power is common in studies of complex health behaviors, and suggests that contextual (eg, organizational culture) and more proximal determinants (eg, norms or intention) likely play an additional role.
Strengths and Limitations
A key strength of our study lies in its large sample size and inclusion of both occupational groups, facilitating a comparative analysis. The use of purposeful covariate selection also improved the robustness of our modeling approach, avoiding overfitting and increasing replication stability. However, there are some limitations to be considered.
First, selection processes may have introduced sampling bias, which is likely to have influenced multiple aspects of the study. Participation in the HAQ was likely lower among workers with lower education and limited health awareness, while ‘at risk’ classification partly depended on both health complaints and, for some behaviors, willingness to change. This may have led to an overrepresentation of motivated workers with poorer health, inflating health-related associations. This selective inclusion may have amplified the observed associations between health indicators and participation. Similarly, workers with low health awareness are likely underrepresented in both occupational groups, but this underrepresentation is probably more pronounced among blue-collar workers, which may have led to an overestimation of their participation and obscured true differences between groups. Second, the study’s exploratory design and reliance on univariate pre-selection of variables introduces potential biases, including omitted-variable bias.45,46 Third, categorization may have obscured more subtle, linear associations with WHPP participation. In addition, some constructs were measured using single- or two-item indicators, which likely reduced measurement reliability and increased random error, thereby attenuating observed associations. Fourth, all measures were self-reported, introducing risks of recall and social desirability bias. Fifth, participation was defined as attending the first consultation, which does not capture long-term engagement. Previous research has shown that higher levels of participation are associated with greater reductions in health risks. 47 Consequently, the present findings relate to initial uptake rather than to the intensity or duration of participation needed to achieve sustained health benefits. Sixth, part of the data was collected during COVID-19 lockdown measures. Because lockdown did not significantly influence participation levels or confound with covariates in the multivariable model, we decided to leave this determinant out of our analyses completely. Last, while the comparison of associations between blue- and white-collar workers revealed no statistically significant differences, our analytical approach may not have been sufficiently sensitive to detect subtle forms of heterogeneity. The inclusion of interaction terms provides an initial exploration rather than a definitive test of between-group variation. Future research could apply stratified analyses to more rigorously examine potential differences in the strength or direction of associations across occupational groups.
Practical Implications
The findings from this study have several practical implications for reaching groups that are less likely to participate. First, to prevent future health deterioration, implementation strategies should focus not only on high-risk individuals but also on preventive engagement strategies for those not yet experiencing health problems. For example, programs can be framed not only as recovery-oriented interventions but also as tools to maintain work ability, which may be particularly relevant in physically demanding occupations.
Second, contract security and work-life balance were both associated with participation. This is relevant given that workers in temporary or flexible roles, and those experiencing a poor work-life balance are at increased risk of both physical and mental health problems.48-50 Sector institutes could consider offering flexible scheduling, minimizing required time investment, and clearly communicating confidentiality safeguards to address concerns related to job security, while employers could facilitate employees by allowing them to participate during working hours.
Third, while sector-level implementation appears to mitigate several organizational barriers, it may lack the social reinforcement typically provided by workplace-based initiatives. Hybrid approaches that incorporate workplace involvement and sector-wide resources may prove more effective. For example, employers may make use of peer ambassadors or support participation by embedding sector-initiated WHPPs within existing workplace routines and encouraging collective participation.
Conclusion
This study identified contract security, neutral work-life balance, and poorer health as key determinants of WHPP participation among blue-collar workers. These findings underscore the importance of reducing barriers for workers in less secure employment and those not yet experiencing health complaints to promote equitable access to health promotion programs. Importantly, the determinants of participation were largely consistent across blue- and white-collar workers, supporting the development of integrated WHPP strategies that address shared determinants underlying participation across occupational groups. Moreover, our findings suggest that sector-level WHPPs may offer unique advantages in reaching workers who are typically underserved by employer-based programs, particularly those in small companies, those working irregular hours, and those experiencing poor supervisory relationships. However, overall participation in the studied WHPP remained modest, suggesting that social support and contextual relevance of workplace-based delivery are necessary for successful implementation of WHPPs. Participation of blue-collar workers in worksite health promotion programs (WHPPs) is typically low, despite the potential benefits for this high-risk group, particularly in sectors like freight transport. This study identifies key determinants of WHPP participation among blue-collar workers. These include having a secure contract, and reporting poorer health and a neutral work-life balance. It also shows that these determinants are similar across blue- and white-collar workers and that sector-level WHPPs can engage typically hard-to-reach populations. To improve participation and equity in WHPPs, interventions should target those with insecure contracts, those with a poor work-life balance, and those not yet experiencing health concerns. Combining sector-level reach with workplace-level social support may enhance engagement.So What?
What is Already Known on This Topic?
What Does This Article Add?
What are the Implications for Health Promotion Practice or Research?
Supplemental Material
Supplemental material - Determinants of Blue-Collar Workers’ Participation in a Sector-Initiated Worksite Health Promotion Program in Freight Transport: An Observational Study
Supplemental material for Determinants of Blue-Collar Workers’ Participation in a Sector-Initiated Worksite Health Promotion Program in Freight Transport: An Observational Study by Marc A. W. Damen, Sarah I. Detaille, Bouwine E. Carlier, Josephine A. Engels and Annet H. De Lange in American Journal of Health Promotion
Supplemental Material
Supplemental material - Determinants of Blue-Collar Workers’ Participation in a Sector-Initiated Worksite Health Promotion Program in Freight Transport: An Observational Study
Supplemental material for Determinants of Blue-Collar Workers’ Participation in a Sector-Initiated Worksite Health Promotion Program in Freight Transport: An Observational Study by Marc A. W. Damen, Sarah I. Detaille, Bouwine E. Carlier, Josephine A. Engels and Annet H. De Lange in American Journal of Health Promotion
Supplemental Material
Supplemental material - Determinants of Blue-Collar Workers’ Participation in a Sector-Initiated Worksite Health Promotion Program in Freight Transport: An Observational Study
Supplemental material for Determinants of Blue-Collar Workers’ Participation in a Sector-Initiated Worksite Health Promotion Program in Freight Transport: An Observational Study by Marc A. W. Damen, Sarah I. Detaille, Bouwine E. Carlier, Josephine A. Engels and Annet H. De Lange in American Journal of Health Promotion
Footnotes
Acknowledgments
The authors want to thank the Sector Institute for Transport and Logistics (STL), and Adaptics for collecting and providing the data for this study.
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of HAN University of Applied Sciences (ECO 197.09/20, September 4th 2020).
Consent to Participate
Informed consent was obtained from all subjects involved in the study.
Author contributions
All authors contributed to the study conceptualization and methodology. Formal analysis was done by MD, SD and BC. Funding acquisition was done by SD and AdL. SD was responsible for project administration, and AdL provided supervision. The first draft of the manuscript was written by MD and all authors reviewed and edited the manuscript. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research has been funded by The Netherlands Organization for health Research and Development (ZonMW), project number: 531001401, and by a HAN University of Applied Sciences Nijmegen PhD-scholarship, project number IN1313; The Article Processing Costs (APC) were funded by the Open Universiteit, Heerlen.
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy restrictions.
Supplemental Material
Supplemental material is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.