
Abstract
Purpose
To evaluate the pathways through which preconception health knowledge relates to preconception health behaviors via behavioral skills among Chinese reproductive-aged individuals and couples using the Information–Motivation–Behavioral Skills model, and to assess dyadic partner effects.
Design
Cross-sectional study with individual-level mediation and dyadic path models.
Setting
Population-based survey in Zhejiang Province, China (July–September 2023).
Sample
1991 individuals (1086 women; 905 men), including 458 heterosexual couples.
Measures
Preconception health behavior score (0-100) summing >20 guideline-recommended behaviors; preconception health knowledge; behavioral skills; sociodemographics.
Analysis
Individual-level mediation estimated with Sobel–Goodman tests; dyadic effects estimated using Actor–Partner Interdependence Model extended to Mediation (APIMeM) via path analysis; two-sided tests with P < 0.05.
Results
Mean behavior scores: women 71.27 ± 9.03; men 71.12 ± 9.96. Women: total effect of knowledge on behaviors 0.896 (P = 0.001); direct 0.785 (P = 0.003); indirect via skills 0.111 (P = 0.033). Men: total 1.731 (P < 0.001); direct 1.313 (P < 0.001); indirect 0.418 (P < 0.001). Dyadic analyses showed partner skill-to-behavior effects: women’s skills → men’s behaviors β = 0.127 (P = 0.003); men’s skills → women’s behaviors β = 0.153 (P = 0.001).
Conclusion
Preconception knowledge and behavioral skills are linked to healthier preconception behaviors, with meaningful partner interdependence. Couple-centered, skill-building interventions may improve preconception health and pregnancy outcomes. Cross-sectional design limits causal inference; self-reported behaviors may introduce bias; findings from one province may limit generalizability.
Keywords
Purpose
Preconception health behaviors are vital for enhancing fertility and improving health outcomes of both mothers and infants. 1 Engaging in healthy practices, such as proper nutrition and avoiding harmful substances, significantly reduces complications during pregnancy.2,3 However, the complexity and specificity of these behaviors may create obstacles to effective implementation, 4 underscoring the need for substantial improvements and targeted interventions. Understanding the mechanisms and determinants that shape these behaviors is crucial for developing targeted interventions.
The Information-Motivation-Behavioral Skills (IMB) model offers a valuable framework for understanding these complexities of preconception health behaviors. The model proposes that information and motivation influence behavior both directly and indirectly through behavioral skills as a key mediator. 5 This mediation pathway is particularly relevant for preconception health behaviors, which involve a broader spectrum of activities such as pregnancy planning, lifestyle modifications, and disease prevention.6,7 The complexity and multifaceted nature of these behaviors demand not only comprehensive knowledge but also the practical skills to translate that knowledge into action. Further, since preconception care is a relatively recent concept compared to established health interventions, 4 many individuals may lack both the foundational knowledge and the corresponding behavioral skills needed for optimal health practices. Within the IMB framework, knowledge serves as the foundation for skill development, and this sequential pathway from knowledge to skills to behavior represents a central mechanism through which health interventions can influence outcomes.8-10
In this study, we apply the IMB framework by focusing on the knowledge to behavioral skills to behavior pathway in preconception health. Preconception health knowledge refers to individuals’ understanding of key concepts, risk factors, and recommended practices before pregnancy, including health screening, nutritional supplementation, avoidance of harmful exposures, and management of existing health conditions. Behavioral skills reflect individuals’ perceived ability to obtain relevant information and to translate knowledge into concrete preparation for pregnancy. Preconception health behaviors refer to the health-related practices undertaken prior to pregnancy, which commonly include lifestyle modification, preventive healthcare use, nutritional management, and risk avoidance. This framework provides a clear basis for examining how knowledge and skills are linked to preconception health behaviors.
Moreover, existing research on preconception health behavior has predominantly focused on individual-level factors, often overlooking the significant influence of intimate relationships on health behavior construction.11,12 This perspective is particularly limiting since pregnancy necessitates collaboration and coordination between partners. The dynamics of a couple’s relationship (eg, communication, mutual support, and shared decision-making) play a critical role in shaping health behaviors that support successful pregnancy outcomes.12,13 Therefore, the interdependence of behaviors in couples emphasizes the importance of a dyadic approach to understanding preconception health behaviors. The Actor-Partner Interdependence Model extended to Mediation (APIMeM) offers a technical framework for analyzing dyadic data related to the IMB model, 14 effectively integrating the individual-level and dyadic-level influences of knowledge and behavioral skills on preconception health behaviors.
Given these research gaps, this study aims to enhance the understanding of preconception health behaviors by integrating individual and dyadic perspectives through the application of the APIMeM in conjunction with the IMB model. As depicted in Figure 1, we explicitly test whether behavioral skills mediate the relationship between knowledge and preconception health behaviors at both the individual and couple-levels. By emphasizing the knowledge—skills—behavior pathway, we aim to identify not only how individual knowledge and skills influence health behaviors but also how the interactions between partners jointly shape these behaviors. Ultimately, this study will provide a more comprehensive framework that can inform the development of targeted interventions. Theoretical Framework and hypotheses of the study. Note. This figure illustrates the hypothesized actor–partner interdependence model extended to mediation (APIMeM). Black arrows denote actor effects (within-person pathways), and orange arrows denote partner effects (cross-partner pathways). Rectangles represent observed variables (women’s/men’s preconception knowledge, behavioral skills, and preconception health behavior scores), and circles (E1–E4) represent residual terms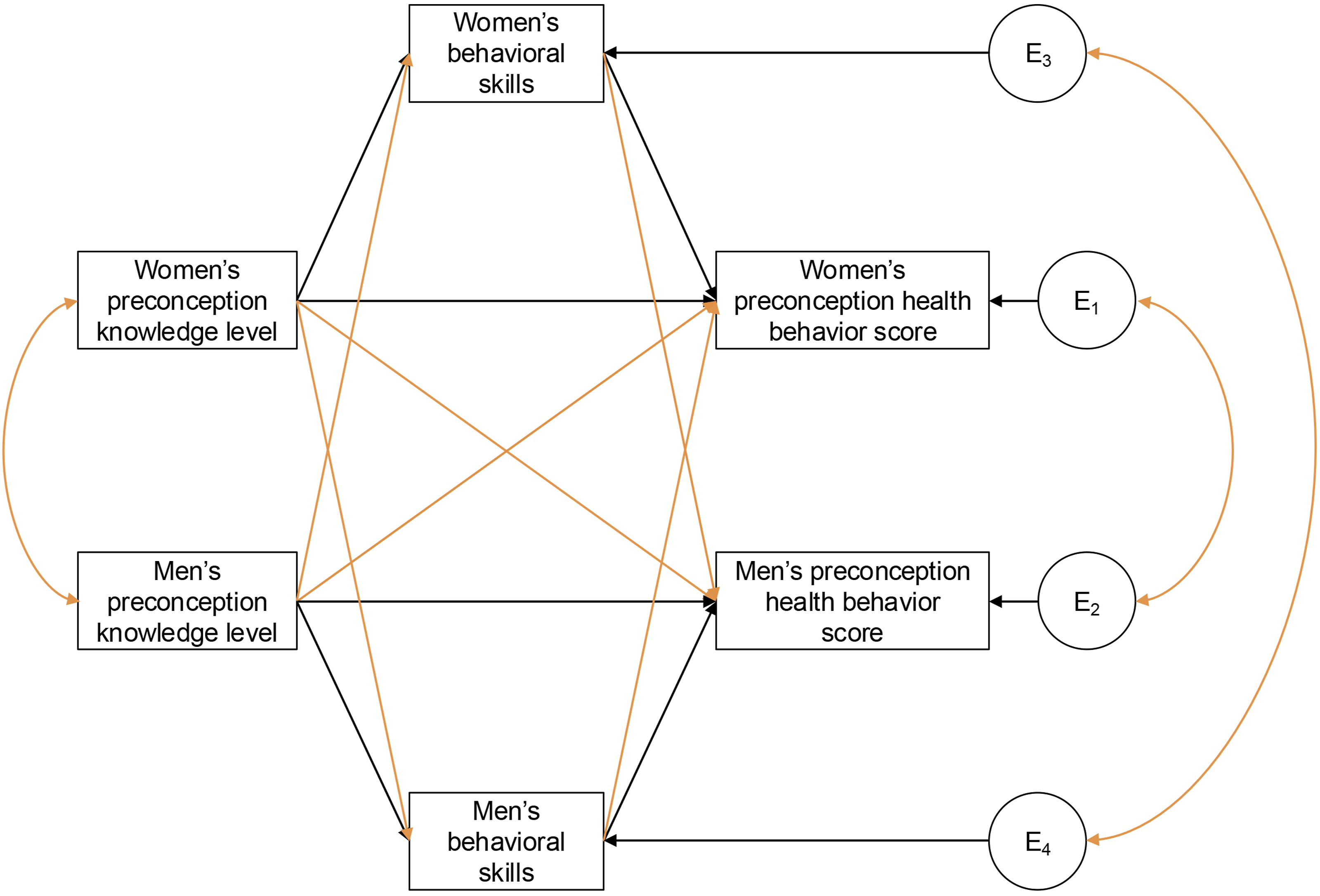
Methods
Design
A cross-sectional survey was conducted between July and September 2023 in Zhejiang Province, located in eastern China. This province was selected as the study site due to its geographical advantages as a coastal region and its heterogeneous demographic composition, including both native residents and internal migrants (ie, individuals relocated from other regions within China).
Sample
The target population were reproductive-aged adults (both women and men) with childbearing intentions. Participant recruitment occurred at various reproductive outcome contexts, including both positive pregnancy outcomes (including unintended pregnancies without termination plans) and adverse reproductive outcomes (fertility challenges and pregnancy loss). This recruitment strategy resulted in three sampling subgroups: respondents with natural pregnancy, infertility, and miscarriage.
A multistage stratified sampling approach was implemented. Initially, two representative cities, Hangzhou and Quzhou, were deliberately chosen to reflect the urban-metropolitan and rural-transitional characteristics of Zhejiang Province. Subsequently, two administrative districts or counties were randomly drawn from each selected city. The final recruitment stage utilized convenience sampling methods at community healthcare facilities and maternal and child medical centers within the four chosen administrative areas. Details regarding the sampling considerations have been published in another study. 15
All valid participants were included in the individual-level analyses, while only data from coupled participants were used in the dyadic analyses. A small number of participants who reported unaware of the concept “pregnancy planning” were not included, as this was required for assessing relevant knowledge and skills.
Two largely parallel survey instruments (man and woman versions) were used, differing mainly in sex-specific reference wording for behavioral recall and a small number of sex-specific behavior items. Data collection was facilitated through a digital survey platform Wenjuanxing. Recruitment activities were conducted face-to-face at local healthcare institutions, with participants completing the digital questionnaires via their mobile devices. Paired responses from couples were verified through a shared identifier: the last four digits of the woman’s phone number. No direct identifiers (eg, names or full phone numbers) were collected. The matching code was used only for couple linkage and was replaced with a random couple ID prior to analysis, so analyses were conducted on de-identified data. All survey instruments included comprehensive informed consent documentation that outlined data protection protocols, voluntary participation principles, and withdrawal rights.
Measures
Instrument Development and Validation
The questionnaires used in this study were developed specifically for the target population based on preconception care guidelines and the IMB model. To ensure validity, a multi-stage development process was followed. First, item pools were generated based on literature review and clinical guidelines. Second, face and content validity were verified through qualitative interviews with experts and target couples. Third, a pilot study was conducted with 131 women and 122 men (excluded from the final analysis) to assess item clarity, response ease, time to complete, and to validate the instrument’s reliability. Based on pilot feedback, minor wording adjustments were made to minimize measurement error and enhance instrument effectiveness.
Dependent Variable
Preconception Health Behavior Score
The primary outcome variable was the comprehensive preconception health behavior score, derived from a validated behavioral assessment model developed on the basis of national and international preconception care guidelines.16-19 The framework was refined through a structured Delphi process to identify and define key behavioral indicators, and the relative importance of each indicator was subsequently determined using the Analytic Hierarchy Process. 20 This scoring system generates sex-specific composite scores reflecting overall adherence to evidence-based preconception health recommendations. The complete list of behavioral indicators and their weight coefficients is provided in Supplemental Tables S1–S2.
Preconception health behaviors were assessed through participant recall of practices during the three months preceding pregnancy (among those with successful pregnancies or miscarriages) or current behavioral patterns (among those experiencing infertility). Complete harmonization of reference periods was not feasible because some subgroups (eg, infertility) lack a clearly defined pre-pregnancy window. The behavioral assessment encompassed over 20 evidence-based practices applicable to both partners, including: planned pregnancy; avoidance of advanced maternal age conception; optimization of parental health status; completion of standard preconception health screening; preconception genetic counseling; receipt of professional preconception health education; maintenance of balanced nutritional intake; psychological well-being preservation; smoking cessation; alcohol abstinence; engagement in appropriate physical activity; maintenance of healthy body weight; establishment of balanced work-life patterns; avoidance of noise exposure; prevention of domestic violence; avoidance of toxic and harmful substance exposure; avoidance of unsupervised medication use; prevention of secondhand smoke exposure; completion of recommended immunizations; management of pre-existing medical conditions; and infectious disease prevention measures. Sex-specific behaviors were additionally assessed, including folic acid supplementation and oral health maintenance for women, and avoidance of hyperthermia exposure for men.
Individual behavioral components were scored on a 0-100 scale, with higher values representing better adherence to recommended practices. Assessment methods varied by behavior complexity: single-item measures were used for straightforward practices (eg, domestic violence prevention, toxic substance avoidance), while multi-dimensional assessments captured frequency, intensity, and duration parameters for complex behaviors (eg, alcohol consumption patterns, smoking behaviors, and physical activity engagement). The final preconception health behavior score was calculated as a weighted composite, where each individual behavior score was multiplied by its corresponding weight coefficient (derived from the expert consensus model) and summed to generate the total score (possible range: 0-100).
Independent Variables
Preconception Health Knowledge
Preconception health knowledge was assessed using a 22-item criterion-referenced knowledge test (true/false/don’t know). Items were drafted by the research team based on preconception care guidelines and relevant clinical recommendations to cover key knowledge points for both partners16-19; the draft was reviewed internally for completeness and wording clarity (Supplemental Table S3 lists all items). Twenty items were presented in the correct format, while two reverse-coded items were included to mitigate acquiescence bias. Each correct answer scored 1 point (total possible score: 0-22). Given the near-ceiling distribution (median = 20) and to improve interpretability, scores were categorized into four levels: below adequate (<20), adequate (=20), good (=21), and excellent (=22). These thresholds were chosen to differentiate near-ceiling performance by each additional correct response while anchoring “adequate” at the sample median. For mediation analysis and path analysis, knowledge levels were treated as approximately continuous variables.
Behavioral Skills
Behavioral skills were assessed using a 3-item scale with 5-point Likert responses (1 = strongly disagree, 5 = strongly agree). Aligned with the IMB model, behavioral skills in this study were operationalized as perceived behavioral skills (self-efficacy/confidence). 21 The three items captured complementary facets: (1) perceived knowledge adequacy (“I have preconception health knowledge”), assessing confidence in one’s existing knowledge base; (2) information-seeking competence (“I can skillfully obtain preconception health knowledge and information”), measuring self-efficacy in accessing resources; and (3) mastery of practical preparation skills (“I have mastered how to prepare for pregnancy”), evaluating confidence in executing preparatory behaviors. We examined dimensionality using both confirmatory and exploratory factor analyses (CFA, EFA). A one-factor CFA model was specified, and all items loaded strongly on a single latent factor (standardized loadings λ = 0.880-0.945, all P < .001). EFA results supported unidimensionality (eigenvalue = 2.70; variance explained = 89.9%; second eigenvalue = 0.19; KMO = 0.76). Item scores were summed and averaged to create a composite score (possible range: 1-5), with higher scores indicating greater behavioral skills (Cronbach’s α = 0.94).
Confounding Variables
Potential confounding variables included (1) sampling subgroup; (2) sociodemographic characteristics including age, ethnicity, education level, monthly household income, and current residence area; and (3) health and reproductive history variables, including self-rated health status, history of induced abortion, history of miscarriage, and self-reported pregnancy planning. Notably, self-reported pregnancy planning should not be confused with the behavioral indicator “planned pregnancy.” In the Chinese context, pregnancy planning (“Beiyun”) emphasizes whether individuals have actively prepared for pregnancy, reflecting a broader concept that encompasses personal readiness and intentional preparatory actions. In contrast, the “planned pregnancy” behavior indicator simply assesses whether the pregnancy was intended.
Analysis
Descriptive analyses were conducted to summarize participant characteristics and core study variables. ANOVA was used to compare preconception health behavior scores across knowledge level categories and sociodemographic subgroups. The Pearson correlation test was conducted to detect the correlation between behavioral skills and behavior scores. The individual-level mediation analyses were performed using the Sobel-Goodman test (implemented with the sgmediation2 package in Stata 18), accounting for potential confounding variables and utilizing 1000 bootstrap resamples to estimate indirect effects and their confidence intervals. The analyses were performed separately for each sex.
For dyadic data, we adopted the APIMeM to evaluate both actor and partner effects as well as mediation pathways within couples. The Actor-Partner Interdependence Model (APIM), and its extension APIMeM, are widely used analytical frameworks for studying dyadic interactions.14,22,23 APIM explicitly models the interdependence between individuals within a dyad, allowing for the examination of how a person’s predictors affect their own and their partner’s outcomes (actor and partner effects, respectively).24,25 The APIMeM further incorporates potential mediators into this framework, enabling simultaneous assessment of direct and indirect (mediated) effects for both members of the dyad. 14 APIMeM analyses were performed in Mplus 8 using maximum likelihood estimation and 2000 bootstrap resamples to construct bias-corrected confidence intervals.
Finally, to address the potential loss of variability and statistical power associated with categorizing knowledge scores, we conducted sensitivity analyses by re-estimating both the individual mediation models and the APIMeM using the original continuous knowledge scores. In addition, to address the subgroup-specific reference window of the behavior measure, we conducted a sensitivity analysis by excluding participants in the infertility subgroup and re-estimating the individual mediation models. All statistical tests were two-sided, and a P-value <.05 was considered statistically significant.
Ethical Considerations
The study protocol was reviewed and approved by two Institutional Review Boards: School of Public Health (ZGL202303-6) and the Women’s Hospital, School of Medicine (IRB-20230245-R) at Zhejiang University.
Results
Characteristics and Comparison of Preconception Health Behavior Scores, by Sex
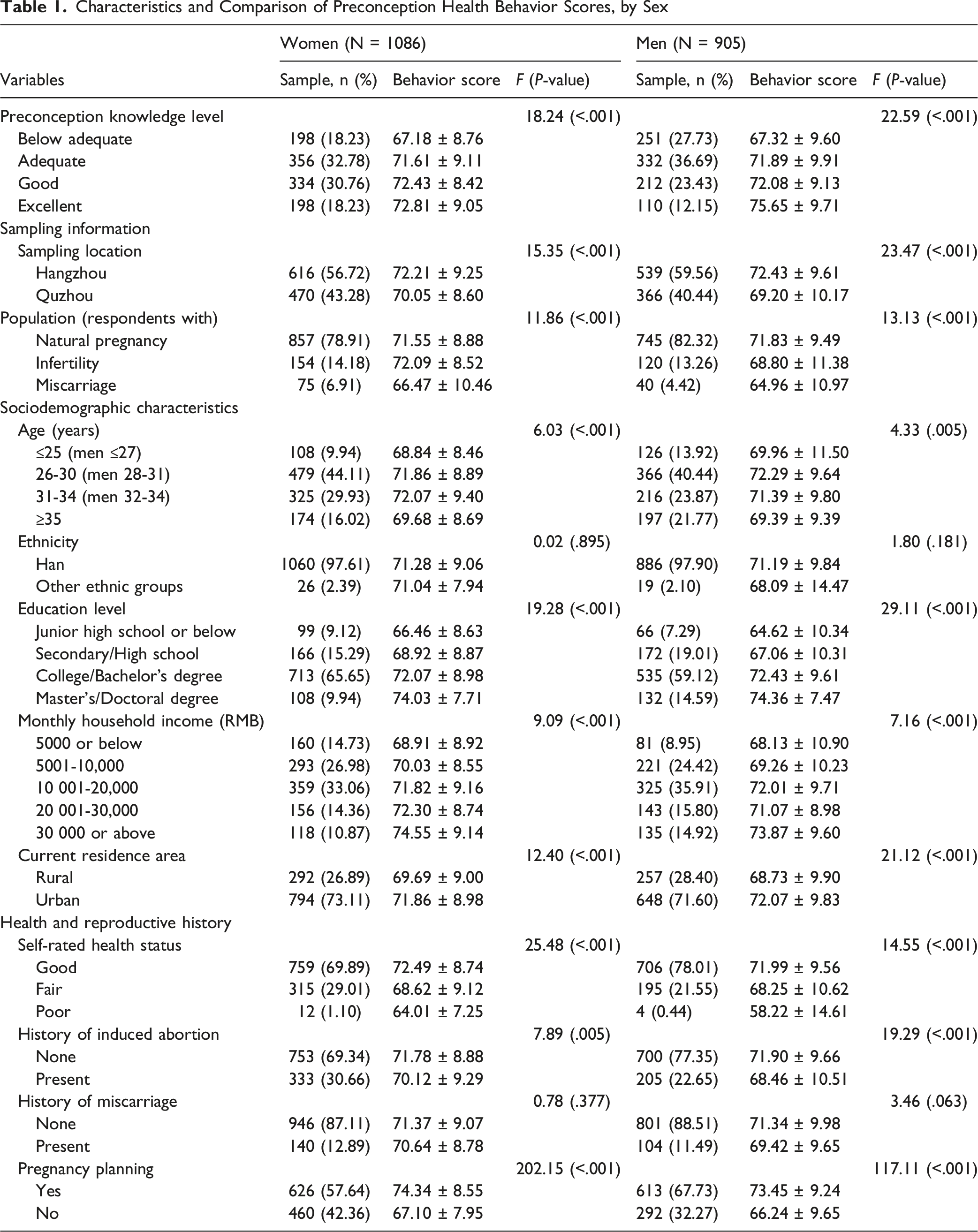
Regarding preconception health knowledge, only 198 women (18.23%) and 110 men (12.15%) exhibited an excellent knowledge level. Meanwhile, 198 women (18.23%) and 251 men (27.73%) reported below adequate knowledge, while the remainder demonstrated adequate or good knowledge levels. The average behavioral skills scores were 3.94 ± 0.79 for women and 3.97 ± 0.84 for men. The preconception health behavior scores averaged 71.27 ± 9.03 for women and 71.12 ± 9.96 for men. ANOVA tests indicated that sampling location and subgroup, age, education level, household income, current residence, self-rated health status, history of induced abortion, pregnancy planning, and preconception health knowledge levels were significantly associated with preconception health behavior scores in both women and men. Additionally, Pearson correlation analyses showed significant correlations between behavioral skills and behavior scores for women (r = 0.323, P < .001) and men (r = 0.369, P < .001).
Estimated Bootstrapped Total, Direct, and Indirect Effects of Preconception Health Knowledge on Preconception Health Behavior Score via Behavioral Skills, by Sex
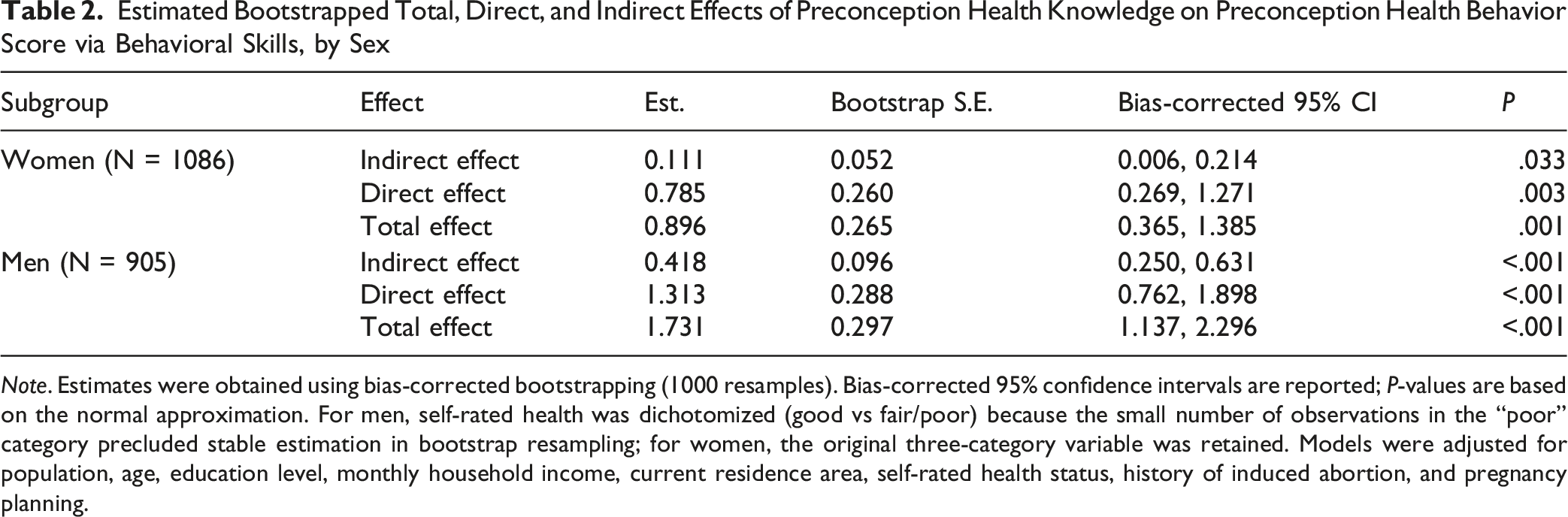
Note. Estimates were obtained using bias-corrected bootstrapping (1000 resamples). Bias-corrected 95% confidence intervals are reported; P-values are based on the normal approximation. For men, self-rated health was dichotomized (good vs fair/poor) because the small number of observations in the “poor” category precluded stable estimation in bootstrap resampling; for women, the original three-category variable was retained. Models were adjusted for population, age, education level, monthly household income, current residence area, self-rated health status, history of induced abortion, and pregnancy planning.
In the couple-level analysis, 458 heterosexual couples were included, demonstrating similar distributions across all variables compared to the total population (Table S4). The correlation matrix of the IMB model constructs is presented in Table S5, indicating significant associations between partners’ preconception health knowledge (r = 0.220, P < .001), behavioral skills (r = 0.234, P < .001), and preconception health behavior scores (r = 0.341, P < .001). These findings highlight the interdependence between partners within couples.
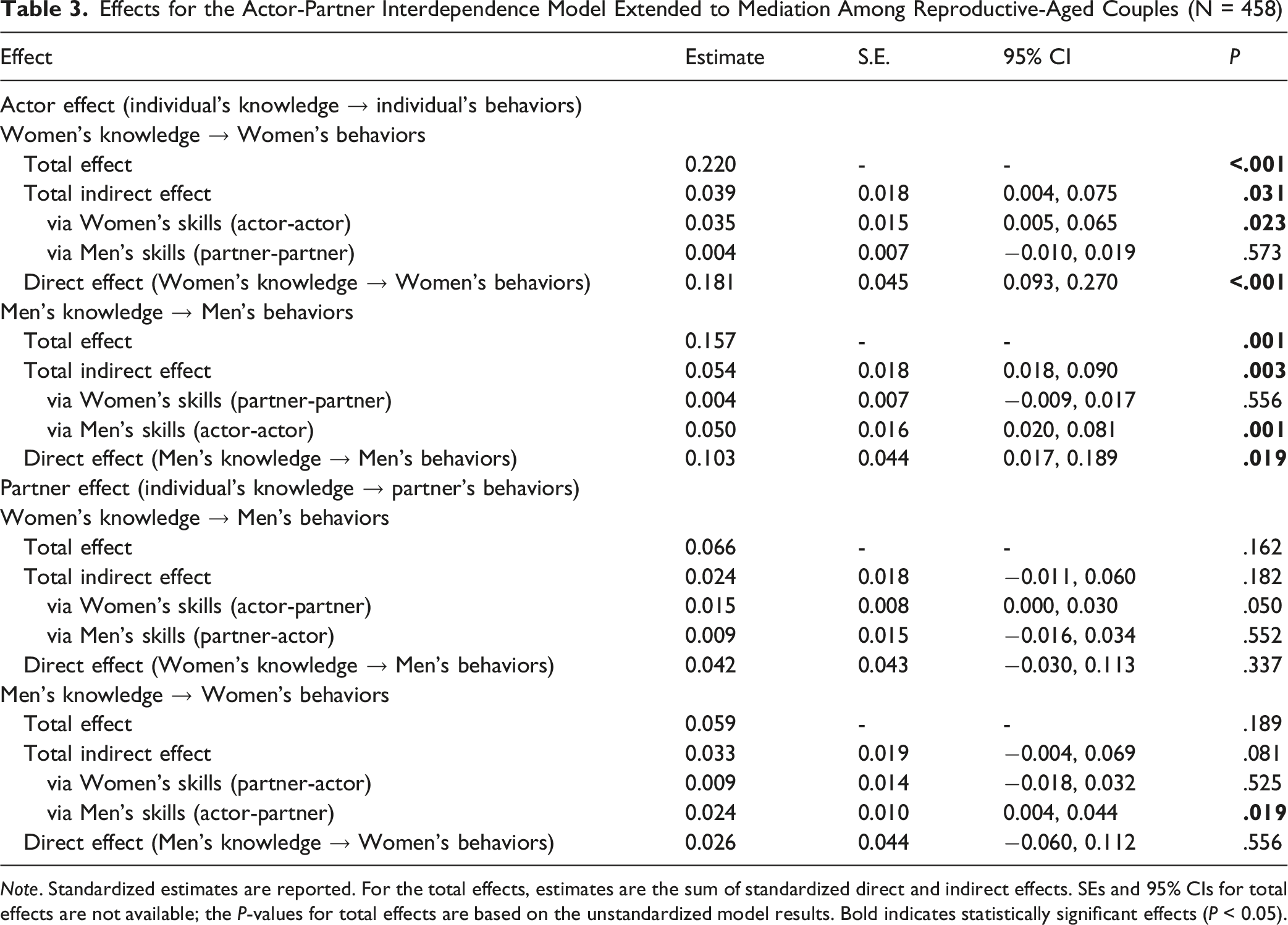
The APIMeM results are presented in Figure 2 and Table 3. The actor effects (total, direct, and indirect) remained significant in both women and men, although the indirect effects via the partner-partner paths were not significant. For partner effect, path analyses showed that women’s skills were positively associated with men’s behaviors (β = 0.127, P = .003), and men’s skills were similarly associated with women’s behaviors (β = 0.153, P = .001). However, the indirect effect of the “women’s knowledge—women’s skills—men’s behaviors” path was nonsignificant (β = 0.015, P = .050). In contrast, the indirect effect of the “men’s knowledge—men’s skills—women’s behaviors” path remained significant (β = 0.024, P = .019), although the total indirect effect of men’s knowledge on women’s behaviors was nonsignificant (β = 0.009, P = .525). The APIMeM was a saturated model (df = 0) with CFI and TLI of 1.0. This model accounted for 18.4% of the variance in women’s behaviors and 17.0% of the variance in men’s behaviors in these couples. Dyadic associations between preconception knowledge, behavioral skills, and preconception health behaviors (APIMeM). Note. Standardized path coefficients are shown. Solid lines represent significant paths (P < 0.05); non-significant paths are omitted for clarity. Black arrows denote actor effects and orange arrows denote partner effects. ∗∗∗ P < 0.001, ∗∗ P < 0.01, ∗ P < 0.05 Effects for the Actor-Partner Interdependence Model Extended to Mediation Among Reproductive-Aged Couples (N = 458) Note. Standardized estimates are reported. For the total effects, estimates are the sum of standardized direct and indirect effects. SEs and 95% CIs for total effects are not available; the P-values for total effects are based on the unstandardized model results. Bold indicates statistically significant effects (P < 0.05).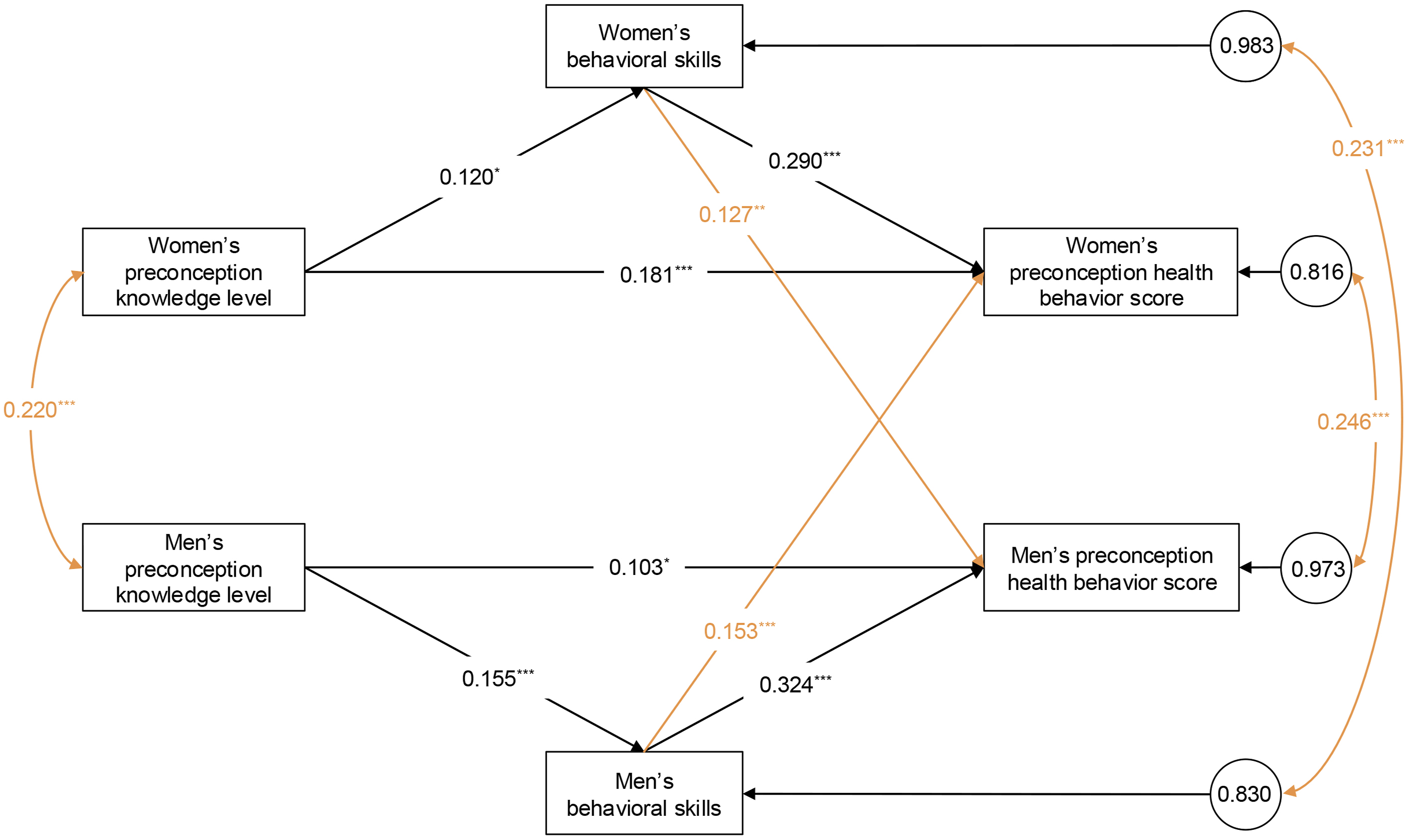
The sensitivity analyses using continuous knowledge scores yielded patterns consistent with the primary findings based on categorical scores (see Supplemental Tables S6 and S7). Specifically, the key actor effects and the mediating roles of behavioral skills remained significant and consistent in direction, indicating that the study conclusions are robust to the categorization strategy. Similarly, when excluding participants in the infertility subgroup, the estimated indirect, direct, and total effects remained consistent in direction (Supplemental Table S8), suggesting that the main conclusions are unlikely to be biased by the asymmetric behavior reference window across subgroups.
Discussion
This study found that preconception health knowledge was positively associated with preconception health behaviors, and the results of the mediation analysis suggest that behavioral skills partially account for this association in both women and men. The dyadic analysis further indicated that behavioral skills were significantly associated with partners’ preconception health behaviors through partner-level direct paths, whereas partner-mediated indirect associations involving knowledge were limited.
Interpretation of Findings
The positive associations between preconception health knowledge and preconception health behaviors among reproductive-aged individuals align with findings from previous studies.8,10,26 Together, these results suggest that increasing knowledge levels is linked to healthier behavioral patterns, emphasizing the need for public health interventions focused on preconception health, particularly in communities with lower awareness levels. However, the mediating role of behavioral skills highlights that knowledge alone may be insufficient; individuals likely need to acquire practical skills to effectively apply this knowledge. This observation is consistent with the theoretical framework of the IMB model, 5 and aligns with a previous qualitative study utilizing the IMB model, which identified knowledge as a crucial component associated with behavioral skills and preconception weight change behaviors. 27 Furthermore, the similarities between sexes observed in the mediated pathways underscore the universal need to develop behavioral skills among all individuals involved in preconception care. Based on the IMB model framework, preconception health programs could consider an integrated approach combining comprehensive education with skills-building workshops to help translate knowledge into practice. Interventions should assess both knowledge gaps and skill deficits, offering tailored support to bridge the knowledge-to-action gap.
At the couple level, the APIMeM results suggest a more differentiated pattern of interdependence. While most partner-mediated indirect associations involving knowledge were nonsignificant and small in magnitude, behavioral skills showed significant partner-level direct associations with preconception health behaviors. This pattern suggests that skill-related behaviors may be more readily shared or aligned between partners than knowledge alone. From a theoretical perspective, these findings are partially consistent with Interdependence Theory and communal coping, which refers to the process by which couples collaboratively confront shared challenges.12,13,28 In the context of preconception health and pregnancy, couples experience a transformation of motivation from being individually centered to being relationship centered,13,28 where a shared assessment of pregnancy-related issues leads to coordinated actions for managing those issues, creating communal coping.12,29 However, the modest effect sizes (β = 0.127 and β = 0.153) indicate that such partner-level associations are limited and likely represent a supplementary, rather than central, component of preconception health behavior patterns.
In the APIMeM, the only significant partner mediation effect identified was the pathway “men’s knowledge—men’s skills—women’s behaviors.” This finding suggests that men’s knowledge was indirectly associated with women’s preconception health behaviors through men’s behavioral skills. In other words, men’s higher knowledge tended to co-occur with higher skills, and higher skills were associated with women’s behavior scores, although the magnitude of this indirect association was small. Importantly, this pattern should not be interpreted as evidence of causal influence, given the observational design and the limited partner pathways that reached statistical significance. In contrast, the pathway “women’s knowledge—women’s skills—men’s behaviors” did not show significant effects. This suggests that women may face greater challenges in influencing their male partners, since their efforts to create change may be more effective when men are open and receptive to new ideas.30,31 This disparity may reflect a meaningful barrier; societal norms often position men as primary decision-makers, which can make it more difficult for women to share health-related knowledge and advocate for change within their relationships.31,32 These interpretations remain tentative because we did not directly measure receptivity, communication, or power dynamics; future longitudinal and qualitative studies are needed to test these mechanisms.
Other partner indirect effects were all nonsignificant, as preconception health knowledge did not show significant partner effects on either behavioral skills or behavior scores. Overall, the APIMeM results indicate that partner-mediated indirect associations were limited and pathway-specific; the more consistent associations were observed in actor pathways rather than partner pathways. It appears that behavioral skills are more strongly associated with an individual’s own knowledge rather than the knowledge of their partner, with a similar pattern observed for health behaviors. Unlike skills, which are practical abilities frequently linked to actions, knowledge represents an understanding of concepts and information, 5 which can vary in its relevance and application depending on individual circumstances.
Methodologically, knowledge scores showed a ceiling effect; thus, we categorized knowledge in the primary analysis to better reflect the observed distribution and to facilitate interpretation. We acknowledge that categorizing a continuous measure can reduce information and statistical power. However, sensitivity analyses treating knowledge as a continuous score yielded a highly similar pattern of results. The consistency across specifications increases confidence in the mediation and APIMeM findings and indicates that the main conclusions are not sensitive to how knowledge was coded.
In summary, interventions should combine knowledge enhancement with behavioral skills training to support preconception health behaviors. Couple-based elements may be positioned as complementary, given the modest partner associations observed, and engaging men in skills-building and communication-focused content may be particularly relevant. Healthcare systems should integrate skills assessment and training into routine preconception care, moving beyond knowledge dissemination to practical skill-building that helps couples implement recommendations.
Strengths and Limitations
This study has several notable strengths. First, the inclusion of men participants allows for a more comprehensive understanding of preconception health behaviors and acknowledges the significant role men play in reproductive health. Additionally, by incorporating both individual-level and couple-level data, the study effectively considers the mutual influences between partners, providing a more comprehensive view of how knowledge, skills and behaviors are interrelated within couples. However, there are also notable limitations to this research. First, the use of cross-sectional data restricts the ability to draw causal relationships, as it captures a snapshot in time rather than longitudinal changes in knowledge, skills and behaviors. Second, the sample being drawn from a single province and recruited through health facilities may limit the generalizability of the findings to other regions and introduce selection bias toward more health-aware and care-seeking individuals. Third, a selection bias regarding socioeconomic status was observed, as the participants had a relatively high education level (over 70% holding a college degree or above) compared to the general Chinese population of similar age. This may limit the applicability of our findings to populations with lower educational attainment. Future studies should aim for more diverse samples to verify these associations across different socioeconomic strata. Fourth, self-reported alcohol use, smoking, and avoidance of domestic violence are sensitive and may be affected by social desirability bias, leading to underreporting. Although surveys were completed privately on participants’ own devices and analyzed using de-identified data, some measurement misclassification may remain and could attenuate associations. Finally, although our measures were developed through a rigorous process involving expert consensus (Delphi method), qualitative interviews, and pilot testing, they are study-specific instruments. This may limit direct comparisons with studies using other standardized scales.
Conclusions
This study highlights the critical role of preconception health knowledge and behavioral skills in relation to preconception health behaviors among reproductive-aged individuals. At the individual level, both knowledge and behavioral skills were strongly associated with preconception health behaviors. At the couple level, behavioral skills exhibited modest partner-level direct associations, whereas knowledge showed limited partner-mediated associations. These findings suggest that intervention strategies could primarily focus on enhancing individuals’ knowledge and practical skills. Couple-based components may be considered as a complementary strategy rather than the primary mechanism for addressing behavioral differences. Preconception behaviors are linked to fertility and pregnancy outcomes; the IMB model links knowledge and skills to health behaviors, but dyadic evidence is scarce. In a large Chinese sample, knowledge was associated with behaviors partly via skills. Furthermore, partners’ skills were positively linked to each other’s behaviors, providing empirical evidence for these dyadic pathways. Couple-centered, sex-inclusive interventions that build behavioral skills may be beneficial for promoting healthier behaviors; longitudinal and experimental tests are warranted.So What?
What is Already Known on This Topic?
What Does This Article Add?
What are the Implications for Health Promotion Practice or Research?
Supplemental Material
Supplemental material - Associations of Knowledge and Skills With Preconception Health Behaviors Based on the Information-Motivation-Behavioral Skills Model: An Integrated Individual and Dyadic Mediation Analysis
Supplemental material for Associations of Knowledge and Skills With Preconception Health Behaviors Based on the Information-Motivation-Behavioral Skills Model: An Integrated Individual and Dyadic Mediation Analysis by Ruyu Sun, PhD, Lu Li, Xin Xu and Hanqian Wang in American Journal of Health Promotion
Footnotes
Acknowledgements
We sincerely thank all the investigators for their diligent efforts in collecting data for this study.
Ethical Considerations
The study protocol was reviewed and approved by two Institutional Review Boards: School of Public Health (ZGL202303-6) and the Women’s Hospital, School of Medicine (IRB-20230245-R) at Zhejiang University.
Consent to Participate
Electronic informed consent was obtained from all participants prior to their involvement in the study.
Consent for Publication
Participants provided electronic consent for the publication of their data as part of this research.
Authors Contributions
Ruyu Sun: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Visualization, Writing – original draft. Lu Li: Conceptualization, Funding acquisition, Methodology, Project administration, Resources, Writing – review & editing. Xin Xu: Methodology, Writing – review & editing. Hanqian Wang: Methodology, Writing – review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Social Science Fund of China [grant numbers 21BGL235].
Declaration of Conflicting Interests
The authors have no relevant financial or non-financial interests to disclose.
Data Availability Statement
The data and materials used in this study are available upon reasonable request to ensure transparency and reproducibility.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.