
Abstract
Purpose
To evaluate short-term outcomes of a six-month clinic-based produce prescription program on food security, dietary behaviors, and health indicators.
Design
Non-experimental pre–post pilot evaluation using quantitative methods.
Setting
Clinic-based food pharmacy.
Sample
62 adults enrolled between June 2024 and April 2025; all identified as food insecure and diagnosed with at least one diet-related chronic condition.
Intervention
Participants received biweekly free produce for six-months.
Measures
USDA 6-item food security module, self-reported daily fruit/vegetable servings, self-reported health status, and continuous BMI.
Analysis
Generalized estimating equations, adjusted for demographic characteristics, were used to assess changes over time.
Results
Food security improved significantly; participation was associated with greater odds of improved food security (aOR = 0.484, P = 0.005). Fruit intake increased by 0.65 servings/day (β = 0.645, P < 0.001) and vegetable intake by 0.60 servings/day (β = 0.597, P < 0.001). Odds of reporting better health status also rose (OR = 1.85, P = 0.020). BMI change was nonsignificant (P = 0.239).
Conclusion
Clinic-based produce prescriptions may reduce food insecurity and improve diet and perceived health in high-risk patients. Limitations include a small sample size, a single site, self-reported data, and the absence of a control group.
Purpose
Approximately 14.3% of U.S. households experience food insecurity, a social condition of limited or uncertain access to adequate food. 1 Individuals facing food insecurity tend to consume more nutrient-poor food and fewer fruits, vegetables, and other healthy foods 2 ; thus, increasing the risk for negative diet-related chronic health conditions (eg, hypertension, hyperlipidemia, diabetes, obesity) and mental health issues.3-10 Correspondingly, food-insecure individuals with diet-related chronic conditions have significantly higher health care expenditures, with increased emergency department visits and hospitalization, and a 46% greater odds of becoming a high-cost health care user.11-13 Moreover, health care utilization increases as food insecurity levels rise. 14
Food-as-medicine programs aim to address the association among food insecurity, diet quality, and diet-related chronic conditions by formally integrating food-based nutritional interventions into clinical settings to prevent these conditions among patients experiencing food insecurity.15,16 For example, food-as-medicine produce prescription interventions are typically geared for patients experiencing food insecurity who have also been diagnosed with at least one diet-related chronic condition (eg, prediabetes, type 2 diabetes, hypertension, obesity) who can still shop, prepare, and cook their own meals. 16 Eligible patients receive a “prescription” (ie, recommendation) from a physician and/or allied health professional to obtain healthy produce at low or no cost (eg, vouchers, coupons) through produce prescription redemption sites (eg, local farmers market, food bank, food pharmacy).16,17 A growing body of evidence suggests that food-as-medicine programs may improve food security, fruit and/or vegetable consumption, and food literacy; however, findings are mixed regarding the impact on blood pressure, BMI, HbA1c, and cholesterol.2,18-23 Most recently, a 2023 microsimulation model estimated that, over a lifetime, produce prescription programs could prevent cardiovascular disease events, increase quality-adjusted life-years, and save billions in healthcare costs. 24
Although emerging evidence is promising, additional evaluations are needed to support scalable implementation within health systems. The purpose of the current pilot evaluation is to assess the preliminary short-term outcomes of a six-month
Methods
Design
The pilot evaluation employed a non-experimental pre-post design and used quantitative methods to explore preliminary short-term outcomes of a 6-month clinic-based produce prescription program on food security, dietary behaviors, and health indicators. As a program evaluation, the activity in this pilot qualified for exemption from IRB review under the U.S. DHHS regulations at 45 CFR 46.104(d), specifically Exemption Category 5, which applies to “research and demonstration projects designed to study, evaluate, improve, or otherwise examine public benefit or service programs. 26 ”.
Intervention
The TampaWell Food Pharmacy (TW FoodRx) is a produce prescription program developed and implemented by the Tampa General Hospital (TGH) Health Park Specialty Clinic and TampaWell, a partnership between TGH and the City of Tampa, with the overall goal of reducing chronic illness and supporting the city’s most at-risk residents by addressing social determinants of health. Patients are referred to the TW FoodRx program by their primary care provider if they have been identified at risk for food insecurity via the Hunger Vital Sign screening tool 27 and are diagnosed with at least one diet-related chronic condition (ie, prediabetes, diabetes, hypertension, obesity). Upon enrollment, patients can “shop” at the TW FoodRx once every two weeks for six months and choose four fruits, six vegetables, and other food items, including grains, proteins, and spices. No formal nutrition counseling was provided; however, pharmacy staff included a registered dietitian who offered informal guidance on produce use upon request. Attendance data was not available for this evaluation, limiting dose quantification.
Sample
Participants in the current pilot evaluation included patients enrolled at TW Food Rx from June 2024 to April 2025. Inclusion criteria included: (1) enrolled between June 2024 and April 2025, (2) first-time participant, (3) over the age of 18, and (4) completed both the baseline assessment and the six-month post assessment. Participant intervention onboarding occurred in person with a pharmacy staff member at the start of the first visit to the food pharmacy. During onboarding, each participant consented to participate in the program and completed the intake survey (ie, baseline assessment) on an iPad. The survey was repeated using the same collection methods at the start of the participants’ final visit at the conclusion of the six-month intervention period (ie, six-month post-assessment). During the evaluation period, 128 participants enrolled in the program, and 62 completed both baseline and six-month assessments and were included in the analysis.
Measures
Demographics
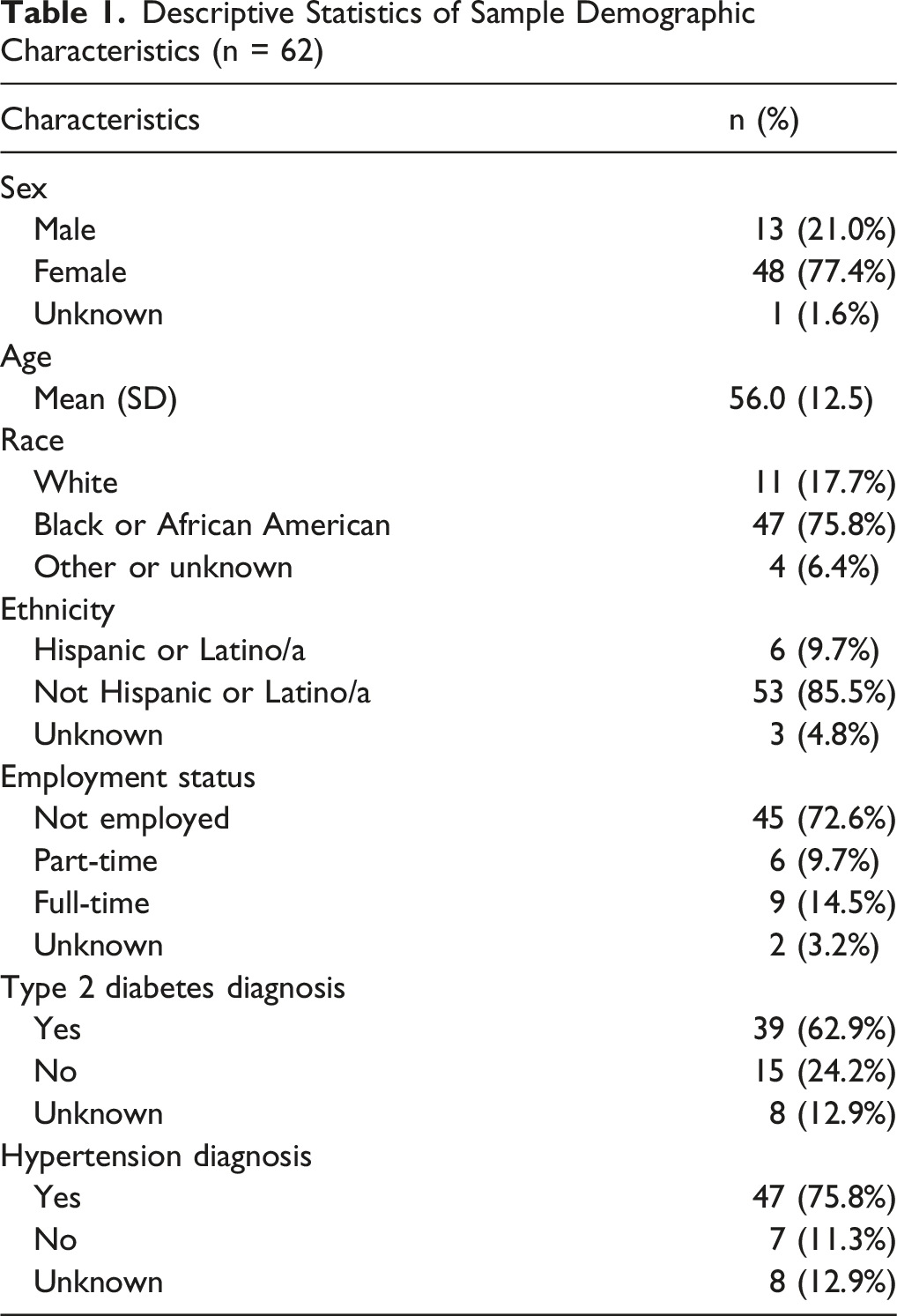
Demographic information collected at baseline included self-reported sex, age, race, ethnicity, employment status, and chronic disease status. Sex was categorized as male, female, or intersex. Age was measured as continuous years. Race was categorized as White, Black or African American, Asian, or another/unknown race. Ethnicity was categorized as Hispanic/Latino/a or not Hispanic/Latino/a. Employment was measured as working part-time (ie, 29 hours a week or less), full-time (ie, over 29 hours per week), or not employed. Regarding chronic disease status, each patient was asked if they had been diagnosed with Type 2 Diabetes, with response options being yes or no, and if they had been diagnosed with Hypertension, with response options being yes or no. Participants were allowed to skip any demographic items they did not wish to report.
Food Security
Food security was assessed using the six-item short form of the U.S. Department of Agriculture (USDA) Household Food Security Survey Module.28,29 Responses were required for all six items on both the baseline and post-assessments. The six-item version is adapted from the 18-item USDA Household Food Security Survey Module, which is widely considered reliable and accurate for measuring food security levels. 28 The six-item short form uses a subset of items from the 18-item scale and has also demonstrated adequate reliability. 29 The scale includes questions on whether, due to limited resources, patients worried food would run out, experienced food not lasting, were unable to afford balanced meals, or reduced the size or frequency of meals. All items asked patients to reflect on the past 30 days. Two items asked patients to rate how often: (1) The food that I bought just didn’t last, and I didn’t have money to get more, and (2) I couldn’t afford to eat balanced meals. Response options were “often”, “sometimes”, and “never”. Responses of “often” or “sometimes” were considered affirmative responses. Three items had yes/no response options. These include: (3) did you ever eat less than you felt you should because there wasn’t enough money for food?, (4) were you ever hungry but didn’t eat because there wasn’t enough money for food?, and (5) did you ever cut the size of your meals or skip meals because there wasn’t enough money for food? Responses of “yes” were considered affirmative responses. Lastly, if the patient responded yes to item five, they were asked to rate how often they cut the size of their meals or skipped meals with response options of “only 1 or 2 days”, “some days but not every day”, and “almost every day”. Responses of “some days but not every day” and “almost every day” were considered affirmative responses. A sum score was created as the total number of affirmative responses, ranging from 0 to 6, with lower scores indicating greater food security. Per USDA scoring guidelines, the sum score was categorized into high or marginal food security (0-1), low food security (2-4), or very low food security (5-6), yielding a categorical food security variable in which lower scores indicate higher food security. 28
Dietary Behaviors
Dietary behaviors were assessed using self-reported daily fruit and vegetable consumption. At each assessment, patients were asked, “On average, how many servings of fruits do you eat each day?” and “On average, how many servings of vegetables do you eat each day?” Per program guidelines, a serving was defined as approximately one cup of raw or cooked vegetables or one medium piece of fruit. Responses were required for both items on both the baseline and post-assessments. Participants selected from a continuous integer response scale ranging from zero servings to six or more servings. Responses were used to generate continuous variables representing the average daily number of fruit servings and the average daily number of vegetable servings.
General Health Status
An adapted item from the CDC Health Related Quality of Life (HRQOL-4) core module was employed to assess general health status. 30 Patients were asked, “How would you describe your current health status?” Responses were on a four-point scale and included “poor”, “fair”, “good”, and “excellent.” A categorical health status indicator was generated, with higher scores indicating better self-reported general health status.
Body Mass Index (BMI)
Participants’ self-reported height (in feet and inches) and weight (in pounds) were used to calculate continuous body mass index. Responses were not required for these items.
Analysis
Analyses were conducted using IBM SPSS Statistics Software 27.0. Descriptive statistics were used to summarize demographic characteristics and outcome variables. To evaluate changes in outcomes from baseline to post-intervention, bivariate pre–post analyses were conducted to assess within-participant change over time. Paired sample t-tests were used to evaluate changes in continuous outcomes, including BMI, daily fruit consumption, and daily vegetable consumption, and Wilcoxon signed-rank tests were used for ordinal outcomes, including food security level and general health status. Next, generalized estimating equations (GEE) were employed to account for the repeated measures within subjects over time. In addition to time (pre vs post), adjusted models included sex, age, race, and ethnicity as covariates to control for potential confounding by demographic characteristics. Covariates were measured at baseline and treated as time-invariant. A cumulative logit link function with a multinomial distribution was used for each ordinal outcome and a normal distribution with an identity link function was used for a linear model of each continuous outcome. Each model included time (pre vs post) as the primary predictor to assess the intervention’s effect and demographic characteristics as covariates. GEE models were specified as: g(μⱼ) = β0 + β1·Timeⱼ + β2·Ageᵢ + β3·Sexᵢ + β4·Raceᵢ + β5·Ethnicityᵢ; where g(μᵢⱼ) is the link function appropriate for the outcome (ie, identity for continuous, cumulative logit for ordinal), μᵢⱼ is the expected value of the outcome, and β1 represents the adjusted effect of time (post vs pre). Model fit and parameter estimates were evaluated using robust standard errors. Statistical significance was set at P < 0.05. Including covariates did not alter the magnitude or statistical significance of the time effects, and the covariates were not independently associated with outcomes. Accordingly, results are presented as adjusted time estimates.
Missing data was managed based on variable types. For each demographic characteristic, the reported descriptive statistics include an unknown category for those who did not respond to the item. For the outcome variables, descriptive statistics and model estimates were limited to those with available data. As food security and dietary behaviors were both required, there was no missing data, and all 62 participants were included in the analysis of these outcomes. However, three participants did not report their general health status, and two participants did not provide the information needed to generate body mass index scores, resulting in a total sample size for analysis of 59 participants and 60 participants, respectively, for analyses of the health indicators.
Results
Demographics
Descriptive Statistics of Sample Demographic Characteristics (n = 62)
Food Security
Baseline and Post-Intervention Outcomes (n = 62)
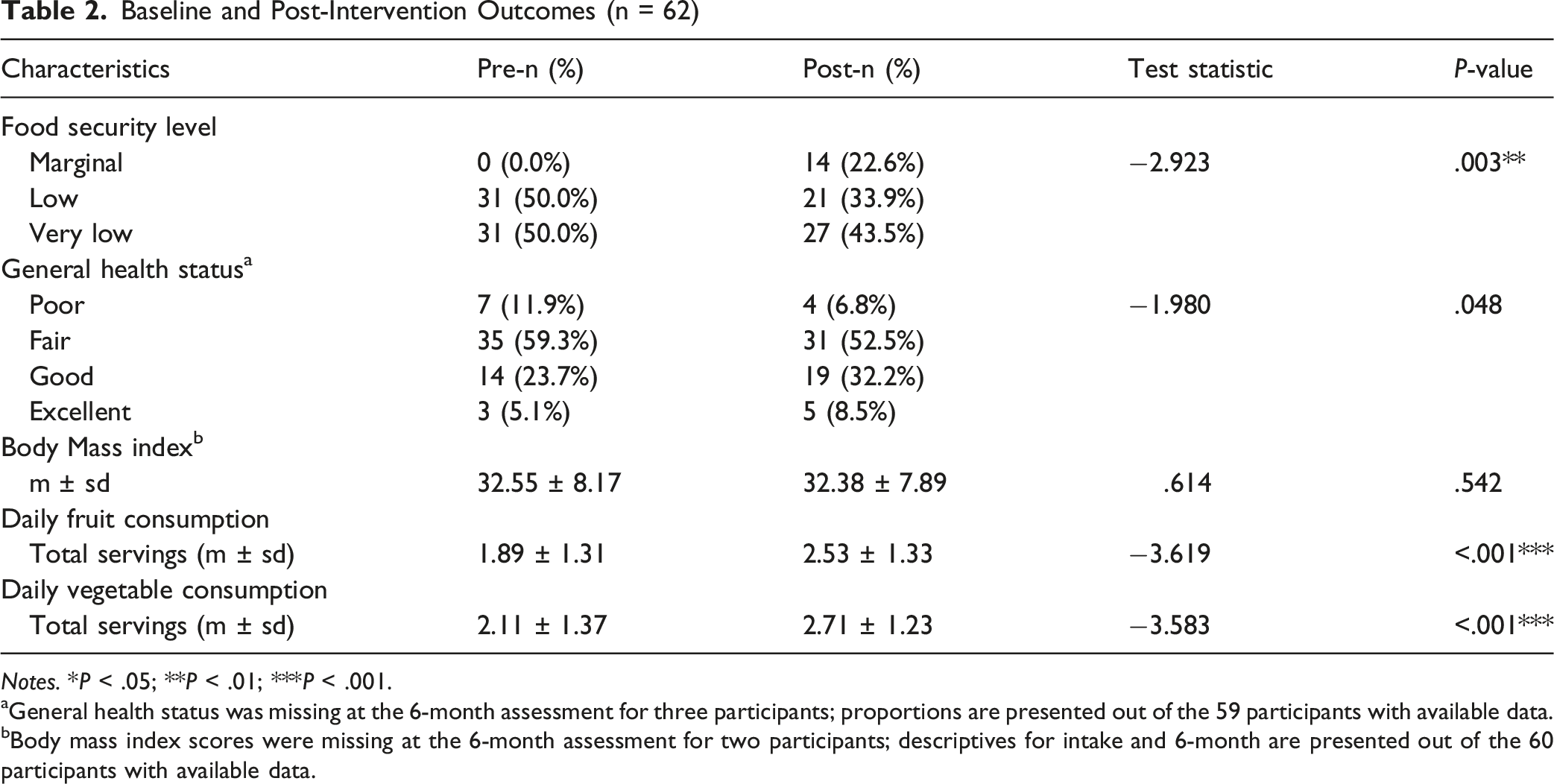
Notes. *P < .05; **P < .01; ***P < .001.
aGeneral health status was missing at the 6-month assessment for three participants; proportions are presented out of the 59 participants with available data.
bBody mass index scores were missing at the 6-month assessment for two participants; descriptives for intake and 6-month are presented out of the 60 participants with available data.
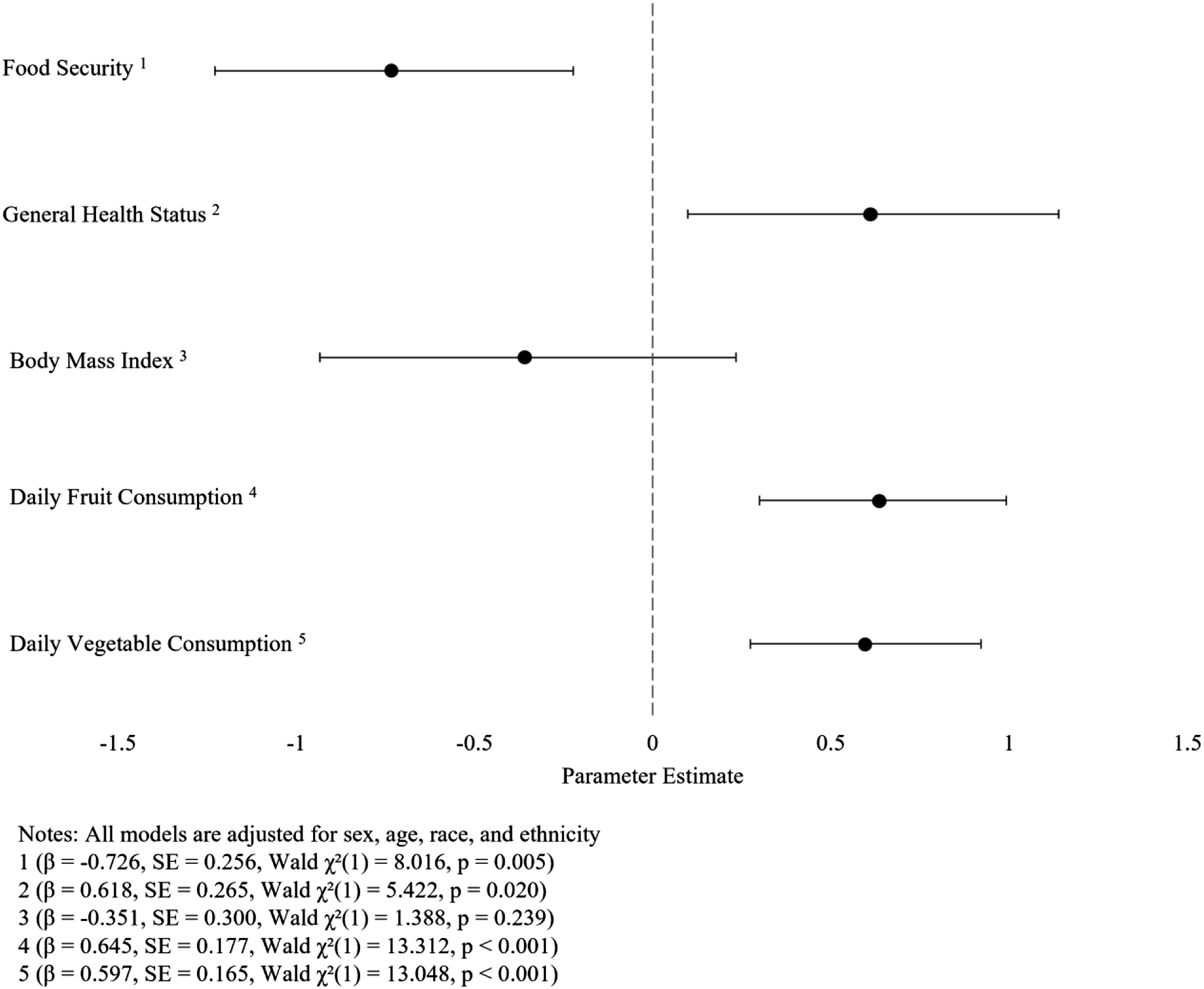
Parameter estimates and 95% confidence intervals from generalized estimating equation models of change in intervention outcomes over time
Dietary Behavior
At pre-intervention, participants reported consuming an average of 1.89 (SD = 1.31) servings of fruits and 2.11 (SD = 1.37) servings of vegetables daily. At post-intervention, participants reported 2.53 (SD = 1.33) servings of fruits and 2.71 (SD = 1.23) servings of vegetables daily. Paired sample t-tests revealed statistically significant increases in both daily fruit and vegetable consumption between baseline and six-month follow-up (Table 2). Mean daily fruit intake increased by 0.65 servings per day (t = −3.619, P < 0.001), and mean daily vegetable intake increased by 0.60 servings per day (t = −3.583, P < 0.001). These improvements were corroborated by adjusted GEE analyses, which showed significant intervention effects on both fruit (β = 0.645, SE = 0.177, P < 0.001) and vegetable (β = 0.597, SE = 0.165, P < 0.001) consumption, indicating increased daily intake following participation (Figure 1).
Health Indicators
Regarding self-reported general health status, at baseline, 11.9% (n = 7) reported to be in poor health, 59.3% (n = 35) in fair health, 23.7% (n = 14) in good health, and 5.1% (n = 3) in excellent health. At post-intervention, a higher proportion of participants reported being in good or excellent health. More specifically, 6.8% (n = 4) reported being in poor health, 53.5% (n = 32) in fair health, 32.2% (n = 19) in good health, and 8.5% (n = 5) in excellent health. At baseline, the mean BMI was 32.67 (SD = 8.10), and post-intervention, the mean was 32.38 (SD = 7.89). Wilcoxon signed-rank testing indicated a significant improvement in general health status over time (Z = −1.980, P = 0.048), with a greater proportion of participants reporting good or excellent health at six months than at baseline (Table 2). In contrast, paired samples t-test results showed no statistically significant change in body mass index from baseline to post-intervention (t = 0.614, P = 0.542). Consistent with bivariate findings, adjusted GEE models demonstrated a significant improvement in health status over time (β = 0.618, SE = 0.264, P = 0.020), corresponding to an increase in the odds of reporting a higher health status category (aOR = 1.85, 95% CI: 1.10-3.12, see Figure 1). No significant intervention effect on body mass index was observed (β = −0.351, SE = 0.300, P = 0.239).
Discussion
While food-as-medicine programs seek to mitigate the relationship between food insecurity, poor diet quality, and diet-related chronic conditions through the integration of nutrition interventions within clinical settings, further empirical evidence is needed to confirm their effectiveness. The current pilot evaluation of a clinic-based produce prescription program demonstrated significant improvements in food security and dietary behaviors among adults experiencing food insecurity and diet-related chronic conditions.
The observed increase in the odds of becoming more food secure is notable and consistent with previous evaluations of produce prescription programs, which reported reductions in food insecurity ranging from one-third to over 90% among participants.23,31 Although only 22.6% of participants achieved marginal food security, this shift suggests that targeted programs can begin to disrupt cycles of food scarcity within a short period (six months), reinforcing the potential for healthcare-linked food access interventions to address structural barriers.
The observed increase in fruit and vegetable consumption, while modest, is clinically relevant given the strong evidence noting even modest improvements in diet quality can reduce cardiometabolic risk, particularly in populations with high rates of diabetes and hypertension. 32 Current U.S. Dietary Guidelines recommend adults consume at least 4-5 servings of fruits and vegetables daily (approximately 2 cups of fruit and 2.5 cups of vegetables) to support optimal health. 33 In this evaluation, participants’ combined intake increased from an average of 4.0 servings to 5.2 servings per day, approaching—but not fully meeting—these recommendations. This suggests that produce prescription programs may help close the gap between actual and recommended intake, particularly among food-insecure populations who face structural barriers to healthy eating.
While prior studies have shown that produce prescription programs can improve dietary patterns,2,23 the current evaluation findings extend this evidence by demonstrating improvements in perceived health status. Improvements in self-reported health status further underscore the potential of food-as-medicine interventions to enhance perceived well-being, even in the absence of significant changes in BMI. This pattern is consistent with previous evaluations reporting that short-term interventions often yield behavioral and psychosocial benefits before measurable changes in weight or metabolic markers occur.20,21 Further, the lack of BMI change may reflect the relatively short duration of the program, reliance on self-reported measures, and the complexity of weight regulation, which is influenced by multiple factors beyond fruit and vegetable intake. This is supported by research indicating that weight-related outcomes often require longer intervention periods. 34
FoodRx programs represent a scalable, patient-centered approach that can complement clinical care for chronic disease management. Given the disproportionate burden of food insecurity among racial and ethnic minority populations, such interventions also have implications for health equity. Findings align with prior research demonstrating that food insecurity and poor diet quality are significant drivers of chronic disease and that interventions targeting these social determinants may represent a practical strategy for mitigating these risks.3-10,23,31 By integrating food access into clinical practice, food-as-medicine programs move beyond education to tangible support, bridging the gap between clinical care and community resources. This approach is particularly relevant as social determinants of health account for a substantial proportion of health outcomes and addressing these factors is essential to reducing disparities. 35 As such, implications for practice and policy are significant. Healthcare systems and payers should consider integrating food-as-medicine programs into routine care for patients with diet-related chronic conditions. Policymakers can support these efforts by expanding reimbursement mechanisms and incentivizing partnerships that address food insecurity.
Several limitations should be considered when interpreting these findings. The small sample size and single-site setting limit generalizability, and all data were self-reported, introducing potential reporting and social desirability bias. For example, self-reported general health status may be influenced by participants’ awareness of receiving program support and should not be interpreted as equivalent to clinical disease improvement. Additionally, the non-experimental design lacked a control group, limiting the ability to attribute observed changes solely to program participation. Moreover, this evaluation included only participants who completed both the baseline and the six-month assessments. Referral data, reasons for non-enrollment, and detailed program attendance were not available, limiting the ability to assess participant flow, attrition prior to baseline, or intervention dose. As a result, selection bias cannot be ruled out, as outcomes may reflect the experiences of participants who were more engaged or able to complete the program. Future research should employ larger samples, longer follow-up periods, and controlled designs to confirm these findings and examine long-term sustainability, cost-effectiveness, and integration with other lifestyle interventions. Future analysis should incorporate comprehensive referral tracking, retention metrics, and utilization data to more fully characterize program reach, engagement, and implementation fidelity. Qualitative studies are also needed to explore participant experiences and inform program refinement.
In conclusion, this pilot evaluation provides preliminary evidence that clinic-based produce prescription programs can reduce food insecurity and improve dietary behaviors and perceived health among patients with chronic conditions. These findings contribute to the growing body of evidence supporting food-as-medicine initiatives and highlight the need for continued investment in interventions that address the root causes of diet-related chronic disease.
So What?
What is Already Known on This Topic?
Food insecurity and poor diet are major contributors to chronic disease. Produce prescription programs have emerged as a promising strategy to improve access to healthy foods and support dietary behavior change, with prior studies showing improvements in fruit and vegetable intake and reductions in food insecurity.
What Does This Article Add?
This pilot evaluation demonstrates that a clinic-based Food Rx produce prescription programs may increase fruit and vegetable consumption, improve perceived health status, and improve food security within six months. These findings provide evidence from a real-world healthcare setting and highlight the potential to integrate food access interventions into routine care.
What Are the Implications for Health Promotion Practice or Research?
Health promotion practitioners should consider food-as-medicine programs as scalable strategies to address social determinants of health. Researchers should explore long-term outcomes, cost-effectiveness, and implementation models to inform policy and expand access to vulnerable populations.
Footnotes
Acknowledgements
We would like to thank Rachel Hoyer, Assistant Director of Community Wellness, and Jenise Carr, Community Garden and Food Pharmacy Manager, at Tampa General Hospital for their support in facilitating the evaluation.
Ethical Considerations
This project was a program evaluation. The activity qualified for exemption from IRB review under the U.S. DHHS regulations at 45 CFR 46.104(d), specifically Exemption Category 5, which applies to “research and demonstration projects designed to study, evaluate, improve, or otherwise examine public benefit or service programs.”
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data may be requested by the corresponding author, Dr. Bleck (