
Abstract
Purpose
Improving access to low-burden, evidence-based smoking cessation interventions for rural communities is essential. This study evaluated the feasibility and acceptability of a text messaging program for smoking cessation (iQuit Mindfully) in rural and urban Georgia.
Design
Pilot study with randomization to iQuit Mindfully or usual care at each site.
Setting
Urban Atlanta and Rural Georgia.
Sample
60 adults who smoked cigarettes (61.7% female, 41.7% African American, 53.3% with annual household income <$30,000).
Intervention
All participants received nicotine replacement therapy, self-help materials, and Tobacco Quitline referrals. iQuit Mindfully participants also received daily personalized, interactive text message support for quitting smoking.
Measures
Program evaluations and remote exhaled carbon monoxide at 8 and 12 weeks.
Analysis
Descriptive statistics quantified primary feasibility outcomes (engagement, retention, participant ratings) and smoking cessation by condition and rural vs urban site.
Results
Most iQuit Mindfully participants (88.9% overall; 100% rural, 78.6% urban) read most or all text messages. On average, iQuit Mindfully participants found the program helpful (median = 8 on 1-10 scale) and recommended it for others (median = 8). Biochemically verified 7-day abstinence rates were 34.8% among iQuit Mindfully vs 25.0% among usual care at week 8, and 13.6% among iQuit Mindfully vs 8.3% among usual care at week 12.
Conclusion
Mindfulness-based text messaging appears feasible and acceptable for providing accessible smoking cessation support in rural and urban Georgia.
Purpose
Severe tobacco-related adverse health outcomes persist for populations with low socioeconomic status (SES), people living in rural areas, and other under-resourced communities. 1 Adults with low SES exhibit disproportionately high rates of smoking, face significant day-to-day barriers to quitting, have lower access to smoking cessation resources, and are more likely to die from tobacco-related illness.1-5 Rural areas tend to have lower SES, weaker tobacco control policies, and lower healthcare access, contributing to higher smoking prevalence and related mortality.5-7 Rural/urban disparities in cancer incidence trends have widened in recent years. 8 Although most U.S. adults who smoke want to quit, less than 9% quit each year. 2 Quitting success rates are even lower for lower-SES, rural, and African American adults.1,9,10 Improving access to low-burden, evidence-based smoking cessation interventions for these communities is essential. 11
Text messaging interventions could improve smoking cessation among populations with limited treatment access. Systematic reviews and meta-analyses support text messaging interventions for smoking cessation,12,13 although more research is needed to optimize benefits for underserved communities. Texting does not require a smartphone, internet access, or high-speed/capacity data plans. Two-way communication enables people to seek support and receive tailored responses, thereby enhancing perceived social support and accountability.14-17
Mindfulness-based interventions (MBIs) can improve smoking abstinence and lapse recovery,18,19 but numerous barriers have prevented widespread use. MBIs are often resource intensive, involving eight weekly 2.5-hour group sessions led by highly trained facilitators. Individuals with low SES and those from racially and ethnically minoritized backgrounds have been underrepresented in mindfulness research, 20 though growing research supports the promise of MBIs in these populations,21-23 including for smoking cessation.19,24-28 Mindfulness helps people to observe experiences of stress and craving so they can engage in purposeful, adaptive responses instead of automatically reacting by smoking. 29
A mindfulness-based text messaging program (iQuit Mindfully) was developed through iterative feedback from low-SES and predominantly African American adults in urban Atlanta, Georgia. 16 Personalized, interactive text messages provide education and support for practicing mindfulness and quitting smoking. Pilot trial results suggested the program may be particularly useful for adults living in poverty. That is, 23% of participants living in poverty who received the iQuit Mindfully intervention achieved biochemically-confirmed smoking abstinence at end of treatment and 1-month follow-up, compared to 0% of those living in poverty who received in-person-only treatment. 30 The majority of mindfulness research (including iQuit Mindfully pilot work) has focused on urban populations. Given the accessibility and promise of iQuit Mindfully in low-resource communities, this intervention could be impactful in rural settings. The purpose of this study was to evaluate the feasibility and acceptability of iQuit Mindfully in urban Atlanta and rural Georgia.
Methods
Overview
Adults who smoked cigarettes and wanted to quit (N = 60) were recruited in metropolitan Atlanta, Georgia (n = 30) and rural Georgia (n = 30). At each site, participants were randomly assigned to iQuit Mindfully (intervention text messages, nicotine patches and lozenges, self-help materials; n = 20) or usual care (nicotine patches, lozenges, self-help materials; n = 10). Participants in the usual care condition received text message reminders about assessments (ie, links and reminders to take the week 8 and 12 online surveys) rather than intervention messages. Participants completed surveys at baseline, 8 and 12 weeks; biochemical confirmation of smoking at 8 and 12 weeks; and open-ended program evaluations at week 12. The study received Institutional Review Board approval from Georgia State University and through a Reliance agreement for Augusta University.
Participants
Inclusion criteria were: at least 18 years old; currently smokes at least 3 cigarettes per day; motivated to quit within next 30 days; owns a mobile phone with text messaging capacity; and can speak, read, and write in English. Exclusion criteria were: contraindication for nicotine patch or lozenge; current use of tobacco cessation medications; current pregnancy or lactation; or another household member enrolled.
Recruitment, Screening and Enrollment
Urban Atlanta
Flyers were posted at local clinics/community health centers and in downtown Atlanta. Digital flyers were posted on Craigslist and Nextdoor. After telephone or online screening, eligible participants talked by phone with study staff to learn more about the study, ask questions, and provide informed consent. Participants chose to sign consent forms electronically or sign and return paper copies by mail.
Rural Georgia
Using electronic health records, adults who smoked and lived in a rural zip code (defined using the US Census Bureau’s classification 31 ) were identified, and also those with a referral to the Georgia Cancer Center tobacco cessation clinic and who lived in a rural zip code were shared with the study team. Researchers contacted these individuals for screening either by phone or in person if they had a scheduled medical appointment. Participants who enrolled signed consent forms electronically (remote enrollment) or on paper for in-person sessions.
Randomization
Participants were randomly assigned to iQuit Mindfully or usual care using an unequal allocation ratio to allocate fewer participants to usual care32,33 (N = 30 per site, n = 20 iQuit Mindfully, n = 10 usual care). Randomization was computer-generated using Microsoft Excel (RAND function) using the planned 2:1 allocation ratio (intervention:control) and stratified by study site.
Assessments
Participant Characteristics by Urban/Rural Location
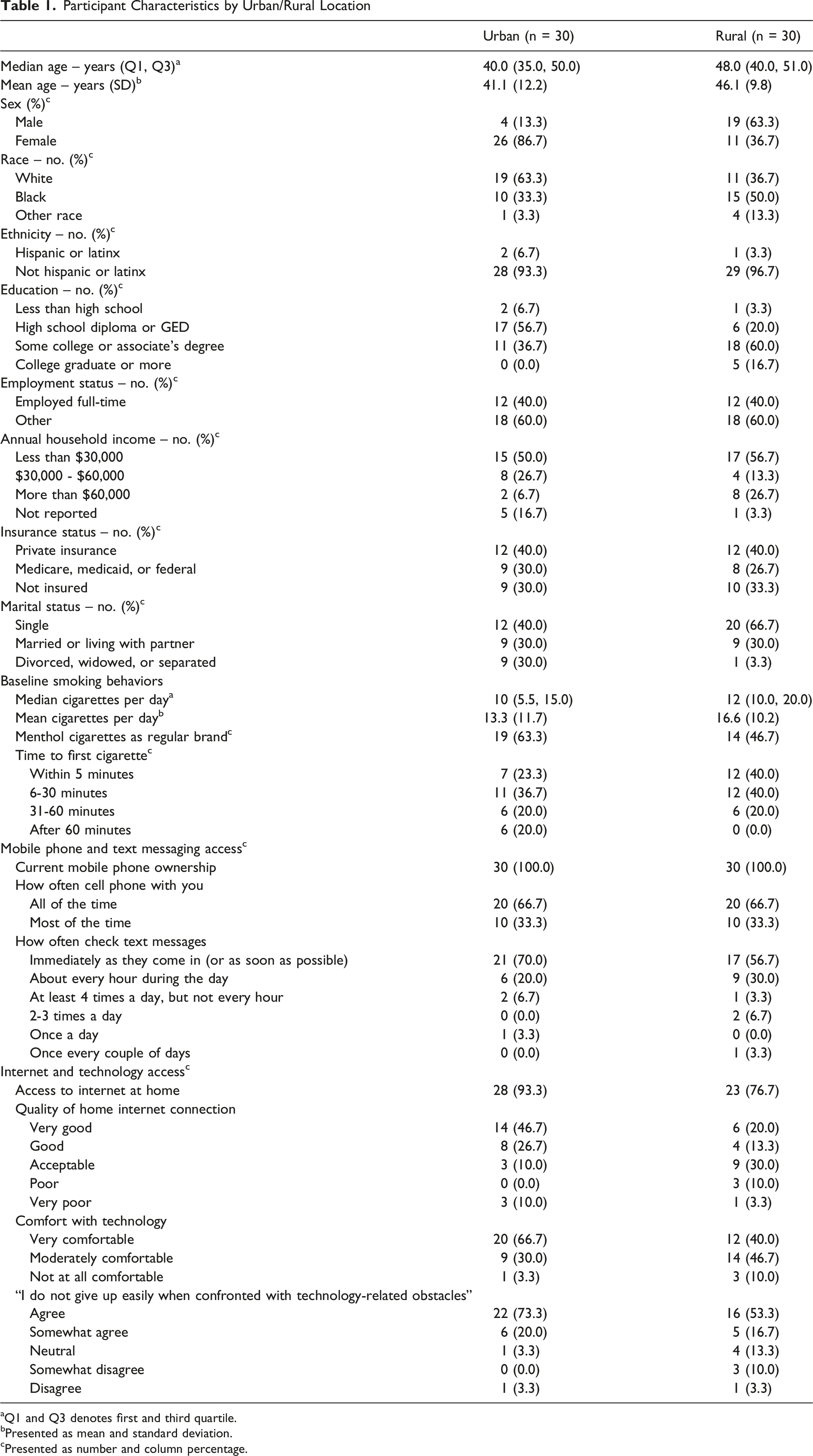
aQ1 and Q3 denotes first and third quartile.
bPresented as mean and standard deviation.
cPresented as number and column percentage.
Participants Characteristics by Intervention Condition
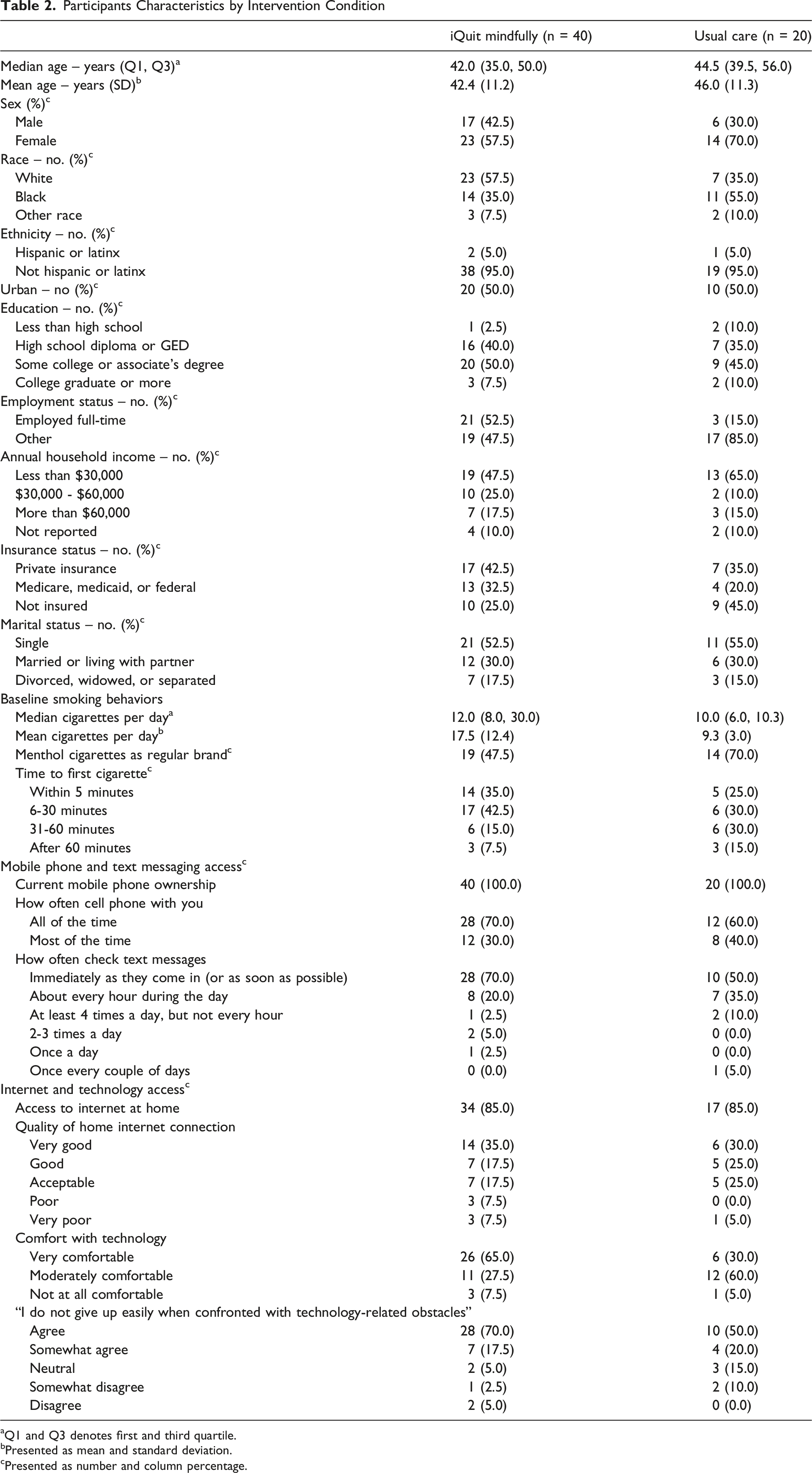
aQ1 and Q3 denotes first and third quartile.
bPresented as mean and standard deviation.
cPresented as number and column percentage.
At weeks 8 and 12, participants were asked, “In the last 7 days, have you smoked even a puff?”. Exhaled carbon monoxide (CO) was assessed with the portable iCO™ Smokerlyzer™. Participants were mailed the device along with handouts with detailed instructions (including pictures) for using it. During week 8 and 12 study visits, research staff reviewed the instructions with participants over the phone. Participants downloaded the app on their Android, iPhone, or tablet for the device to connect via Bluetooth. During the phone call with research staff, participants breathed into the device and clicked “Share results” to immediately email results to the research team. When there were technical issues, staff helped to troubleshoot while on the phone. Seven-day point prevalence abstinence was defined as self-report of no smoking in the past 7 days and exhaled CO<6ppm. Missing data were not coded as smoking because of the potential for severe bias documented in previous studies.34,35
For iQuit Mindfully participants, week 12 program evaluations inquired: “Overall, how helpful were the text messages in getting you to try to quit smoking?” (rated from 1 [not at all helpful] to 10 [extremely helpful]); and “Please select the number that best represents whether you would recommend that other people received the text messages that you received in this program (or similar texts) as a way to help them quit smoking” (rated from 1 [would NOT recommend] to 10 [would DEFINITELY recommend]). They were asked the following open-ended questions: “What did you like the most about the text messages?” “How if at all, did you find the text messages to be helpful?” “What, if anything, did you dislike about the text messages?” and “What recommendations do you have to improve the text messages?”
At week 12, all participants were asked four questions about perceived benefits of the program 17 (each rated from 1 [completely disagree] to 5 [completely agree]): “The program gave me confidence that I can quit smoking,” “The program made me think that it was worthwhile for me to quit,” “The program made me feel that someone cared if I quit,” and “The program made me feel that I knew the right steps to take to quit.”
Financial Compensation
Participants were compensated $40 for the baseline assessment, $10 each for weeks 3 and 5, $40 for week 8, and $50 for week 12. Participants chose mailed Walmart gift cards or electronic gift cards.
Interventions
All participants received: self-help materials (National Cancer Institute “Clearing the Air” 36 ); referral to Tobacco Cessation Quitline; and an 8-week regimen of nicotine patches and lozenges delivered by mail. Patch therapy for participants who smoked >10 cigarettes/day consisted of 4 weeks of 21 mg patches, 2 weeks of 14 mg patches, and 2 weeks of 7 mg patches. Those who smoked 5-10 cigarettes/day received 4 weeks of 14 mg patches and 4 weeks of 7 mg patches. Participants who smoked their first cigarette within 30 minutes of waking received 8 weeks of 4 mg mini lozenges (6-9 lozenges/day). Those who smoked their first cigarette more than 30 minutes after waking received 8 weeks of 2 mg mini lozenges (6-9 lozenges/day).
iQuit Mindfully participants also received text messages for 12 weeks. Mobile Commons, a service that supports implementation of automated SMS applications, sent and received the text messages, which were designed to encourage mindfulness practice (eg, mindful breathing, mindful stretching) and other strategies (eg, removing cues to smoke, eliciting social support). Texts were interactive in that participants answered questions using flow logic (eg, “Good morning, [FirstName], Did you smoke yesterday?”, with a tailored motivational message based on their response), and they could text CRAVE, STRESS, SLIP, or FACT keywords anytime for immediate response. Participants could answer “group poll” questions and later receive a text with the most common responses. Participants could also text keywords to receive a phone call with a short recording of a mindfulness practice. Messages were personalized based on first names, personal reasons for quitting, and amount of money to be saved by quitting. Participants chose their preferred text message frequency and timing and could adjust as needed. They were mailed wallet-sized cards with program information and reminders of text keywords.
Analytic Approach and Benchmarks for Success
The outcomes for this feasibility study, with a priori determined benchmarks for success were: 1) engagement and follow-up rates (we expected ≥75% of iQuit Mindfully participants to read most or all texts and ≥80% of all participants to complete week 12 assessments); and 2) participant ratings (minimum of 7 on 10-point scale for perceived helpfulness of iQuit Mindfully was deemed “acceptable”). While primary outcomes pertain to feasibility and our study was not powered for formal hypothesis testing, we provide descriptive statistics on smoking cessation outcomes at weeks 8 and 12, stratified by treatment condition and rural/urban site. We present the total number and relative frequencies for categorical variables, and either mean (standard deviation) or median (1st and 3rd quartiles) for normal and non-normal continuous variables, respectively. We used SAS software version 9.4 (copyright © 2013 SAS Institute Inc., Cary, NC) for quantitative analyses. For open-ended responses (iQuit Mindfully condition only), descriptive statistics are reported on the number of participants who responded to each item (separately for rural vs urban), and response categories and example quotations are shown.
Results
Participant Characteristics
Most participants were female (61.7%); 41.7% identified as African American and 50% as White. About half (53.3%) reported total annual household income <$30,000. Descriptives by site and condition are shown in Tables 1 and 2 The mean age was 41.1 years (SD = 12.2) for urban participants and 46.1 (SD = 9.8) for rural participants. Although statistical comparisons were not made due to the small sample sizes and exploratory nature of this study, rural participants were more likely to be male (63.3% vs 13.3%) and have a college degree or more (16.7% vs 0.0%). Urban participants were more likely to report being divorced, widowed, or separated (30.0% vs 3.3%) compared to rural participants. Although all participants owned a mobile phone, rural participants checked their text messages less often, were less likely to have internet access at home, rated the quality of their internet connection as worse, and indicated lower comfort with technology, compared to urban participants. At baseline, rural participants tended to smoke more cigarettes per day and smoke sooner upon waking than urban participants. Participants randomly assigned to iQuit Mindfully (vs usual care) were more likely to be male, White, employed full-time, and smoked more cigarettes per day at baseline.
Intervention Acceptability
Comparison of Outcomes Between iQuit Mindfully Intervention and Usual Care Participants
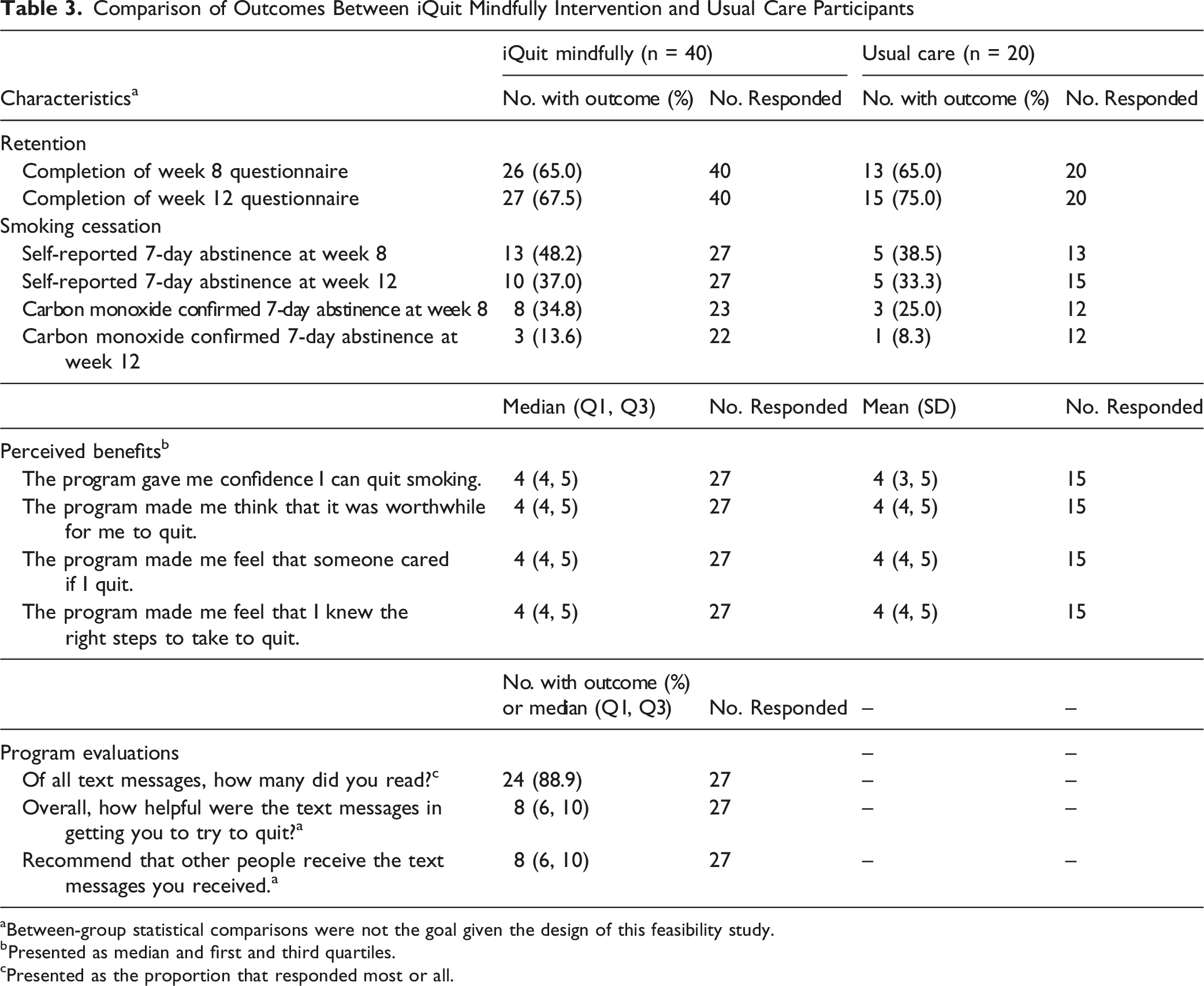
aBetween-group statistical comparisons were not the goal given the design of this feasibility study.
bPresented as median and first and third quartiles.
cPresented as the proportion that responded most or all.
Retention
Benchmarks for success were not met for retention (where we expected at least 80% of participants to complete week 12). Completion of the week 12 questionnaire was 67.5% among iQuit Mindfully participants and 75.0% among usual care (Table 3).
Smoking Cessation
Self-reported 7-day abstinence rates were 48.2% among iQuit Mindfully vs 38.5% among usual care at week 8, and 37.0% among iQuit Mindfully vs 33.3% among usual care at 12 weeks (Table 3). CO-verified 7-day abstinence rates were 34.8% among iQuit Mindfully vs 25.0% among usual care at week 8, and 13.6% among iQuit Mindfully vs 8.3% among usual care at 12 weeks.
Stratification by Rural vs Urban Setting
Comparison of Outcomes Between iQuit Mindfully Intervention and Usual Care Participants, Among 30 Rural Participants
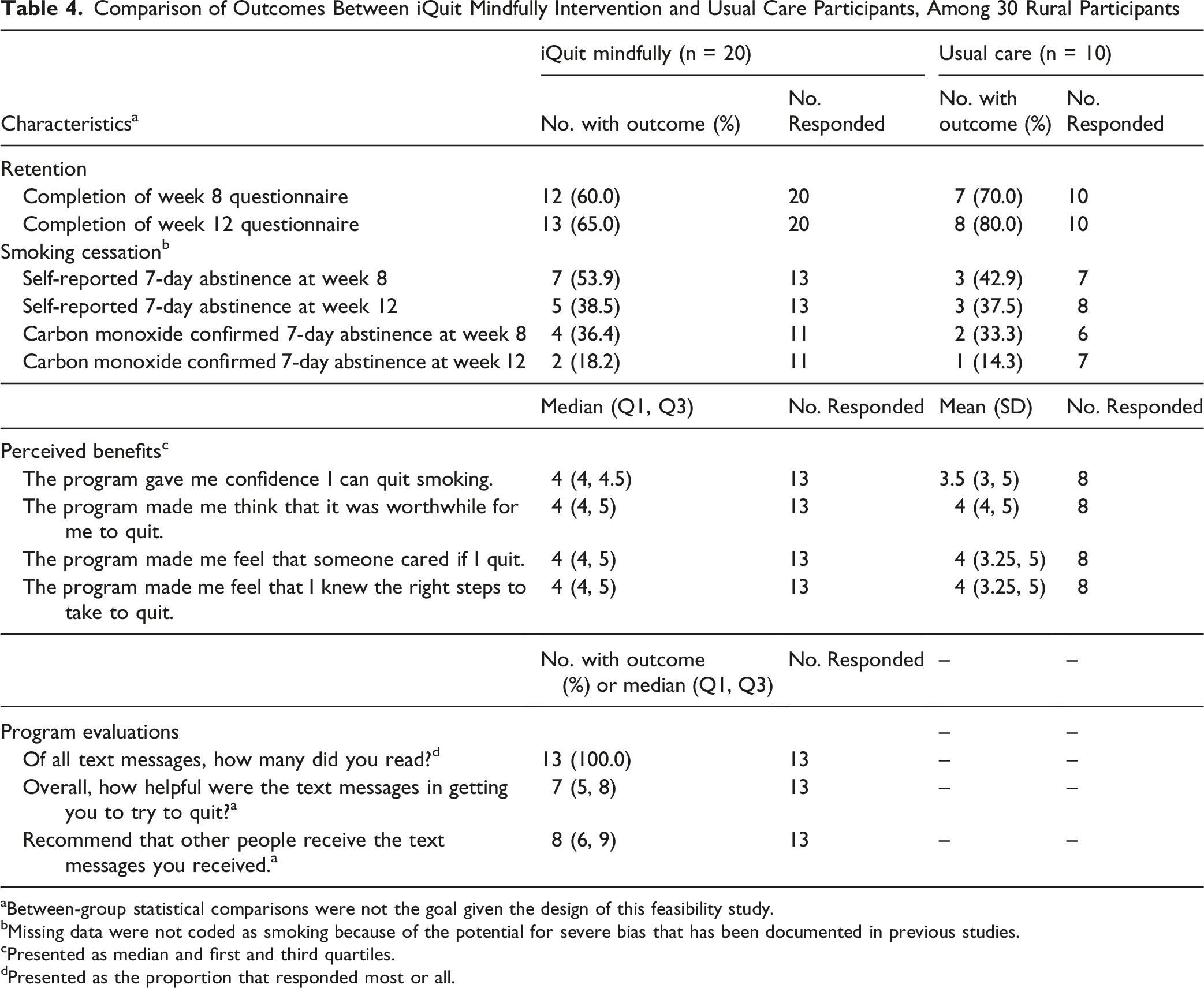
aBetween-group statistical comparisons were not the goal given the design of this feasibility study.
bMissing data were not coded as smoking because of the potential for severe bias that has been documented in previous studies.
cPresented as median and first and third quartiles.
dPresented as the proportion that responded most or all.
Comparison of Outcomes Between iQuit Mindfully Intervention and Usual Care Participants, Among 30 Urban Participants
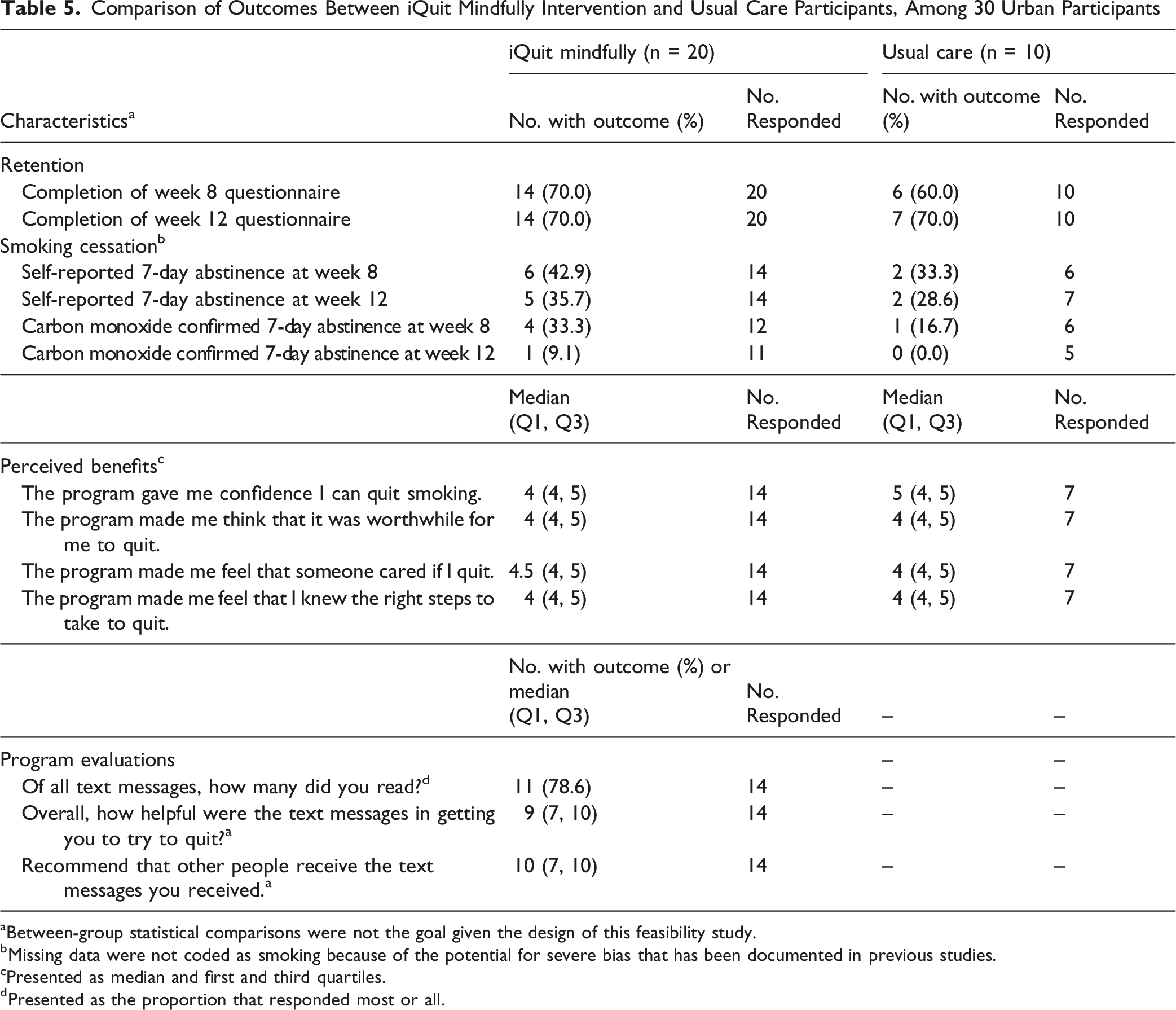
aBetween-group statistical comparisons were not the goal given the design of this feasibility study.
bMissing data were not coded as smoking because of the potential for severe bias that has been documented in previous studies.
cPresented as median and first and third quartiles.
dPresented as the proportion that responded most or all.
Qualitative Findings
When asked what they liked most and what was helpful about the text messages, 19 people (12 urban, 7 rural) responded. Four themes were identified: 1) positive, encouraging tone (eg, “They helped encourage me to quit,” (Urban [U]) “encouraging and uplifting” (Rural [R]); 2) reminders of reasons to quit (eg, “reminders of who I’m quitting for and why” (U); “the constant reminder” (R); 3) mindfulness strategies for coping with stress and cravings (eg, “breathing and count to 10 before you smoke” (U); “learned techniques to use during anxiety” (R); and 4) social support (eg, “It feels like someone is following your progress” (U); “It was nice having a support system outside family” (R).
When asked what they disliked, 10 urban participants responded, with 9 of these being comments like “cannot think of anything” or “none they were great.” Four rural participants responded to the question about dislikes, with one saying that they did not dislike anything, and the three others saying the texts “remind me about smoking” or are too frequent.
When asked about suggestions for improvement, three rural participants responded, with two of those indicating “none” (no suggestions) and the other stating “don’t send any.” Eleven urban participants responded, with six indicating no suggestions. Among the other five, suggestions included more personalization (“be more specific to target individuals”), more picture messages, and that sometimes a call might be needed in addition to texting.
Discussion
This study evaluated the feasibility and acceptability of iQuit Mindfully, a mindfulness-based text messaging intervention for smoking cessation, among adults in urban and rural Georgia. Findings provide preliminary support for the acceptability of the intervention, with strong user engagement, positive perceptions of the text messages, and encouraging trends in smoking cessation outcomes. This project offers insights on both the opportunities and challenges associated with fully remote digital health interventions for smoking cessation in low-SES and rural communities. This work aligns with calls to action for low-burden, accessible interventions to address tobacco use for cancer prevention and control in rural settings.11,37
Across urban and rural sites, iQuit Mindfully participants rated the intervention favorably, exceeding predefined benchmarks. Qualitative feedback illuminated participants’ appreciation for the positive tone, social support, and mindfulness strategies, which is consistent with prior studies of iQuit Mindfully in urban settings.16,38 In a pilot study of another text messaging program to support smoking reduction and cessation among rural older adults (ages 60 and older), participants similarly appreciated the positive reminders, 39 though that intervention did not involve mindfulness. A recent RCT also supported the short-term efficacy of a text messaging intervention for smokeless tobacco cessation in rural communities. 40
Accessibility and comfort with technology are critical for considering implications for digital health equity. 41 The proliferation of digital health interventions has promise for improving population health, but could have unintended consequences of exacerbating worse health outcomes if they are not developed for, evaluated among, and accessible to underserved communities. 41 In rural and other medically underserved areas, text messaging may be more widely accessible than interventions requiring internet access. One study found higher uptake and satisfaction with a text messaging program for home blood pressure monitoring among Black patients with Medicaid or Medicare, compared to using an online patient portal. 42 In our study, rural participants were less likely to have internet access at home, rated their home internet connections as poorer quality, and noted lower comfort levels with technology than urban participants. However, all participants across rural and urban settings said they had their mobile phone with them all or most of the time. Moreover, among iQuit Mindfully participants, 100% of those in rural settings noted reading most or all intervention text messages (versus 78.6% of urban participants). The potential for text messaging as a highly accessible, scalable intervention modality in rural settings is promising. Nevertheless, these programs can be improved through ongoing feedback and community collaboration. In our study, some rural participants expressed concerns about message frequency and repetitiveness—areas that might be addressed through more personalized tailoring. Urban participants suggested enhancements such as adding visuals or incorporating voice calls for additional support.
Although intervention acceptability was strong, benchmarks for retention were not met. Overall, 67.5% of iQuit Mindfully participants completed the 12-week follow-up. While this is below the 80% benchmark, it is more favorable than the 60% retention rate reported in a systematic review of RCTs of mHealth interventions across various cardiovascular diseases. 43 A prior study of iQuit Mindfully that involved in-person interaction reported 89% retention at 12 weeks. 30 It may be that in-person interactions and/or improved strategies for remote engagement are needed. Strategies to build trust and maintain rapport with rural communities include meeting people in person, attending community events, and sending newsletters and personal birthday/holiday cards.44,45 Additional strategies to support retention might include enhanced onboarding, flexible follow-up modality, and structured technical support. Our staged compensation model might also be improved with more escalating incentives for follow-up visits. Although text messaging was well received at both sites, there were issues with remote CO assessment, particularly at the rural site due to limited internet connectivity. A recent review 46 highlighted multiple barriers to collection of remote biomarkers of tobacco use, including usability (eg, challenges using CO monitoring devices), technical issues (eg, problems connecting CO device), and factors related to digital divide (eg, lack of internet service), with a call to action for user-centered design methods to advance health in underserved populations. Ongoing work is needed to address these issues, both to provide personalized motivation and to support rigorous data collection in underserved communities.
While this study was not powered to detect significant differences in smoking cessation, findings suggest promising trends. The iQuit Mindfully group demonstrated higher self-reported and biochemically verified abstinence rates at both 8 and 12 weeks compared to usual care. Biochemically confirmed abstinence rates of 34.8% and 13.6% in the iQuit Mindfully group at weeks 8 and 12, respectively, are favorable compared to less than 9% of people who successfully quit in the general U.S. population, 2 recognizing that success rates are typically lower in rural and low-SES populations.1,9 Ongoing work is needed to support long-term smoking cessation success. As suggested by some participants, more personalization, varied content, and additional support (eg, phone call or in-person visit) might help to promote long-term abstinence.
Several limitations warrant consideration. First, the small sample size limits generalizability and precludes formal efficacy testing. Second, retention was suboptimal, highlighting the need to improve participant engagement strategies. Strategies to enhance retention and biochemical confirmation in future trials might include in-person onboarding and study visits, more check-in appointments for technical support, and alternative remote biochemical verification strategies that do not require internet access (eg, saliva samples to assess cotinine). Third, self-selection bias may have favored individuals already motivated to quit smoking, potentially inflating acceptability ratings. Fourth, randomization was conducted without blocking within site, which may have contributed to baseline imbalances observed between study conditions, and allocation concealment was not maintained. Future trials might implement blocked/stratified randomization and alternative biochemical verification. However, this study is strengthened by its focus on an underserved population, randomization within both rural and urban settings, and use of both quantitative and qualitative data to assess acceptability. Scalable and accessible interventions like iQuit Mindfully have the potential to expand the reach of evidence-based smoking cessation support. This study provides the groundwork for a full-scale randomized controlled trial to examine efficacy and whether rurality moderates treatment outcomes. If supported in larger trials, this intervention could be integrated into broader public health efforts and adapted for use within community settings or rural telehealth platforms. Rural communities have lower access to smoking cessation resources and are more likely to die from tobacco-related illness. A mindfulness-based text messaging program (iQuit Mindfully) shows promise for smoking cessation but has not been tested in rural settings. Evidence supporting the acceptability and feasibility of iQuit Mindfully for predominantly low-socioeconomic status adults in urban and rural Georgia, in addition to promising biochemically verified smoking cessation outcomes. Mindfulness-based text messaging is a promising low-burden, evidence-based intervention for smoking cessation. This highly accessible and cost-effective modality could be implemented for health promotion in rural and other underserved communitiesSo What?
What is Already Known on This Topic?
What Does This Article Add?
What are the Implications for Health Promotion Practice or Research?
Footnotes
Author Note
Authors’ affiliations are listed based on the institutions where the work was conducted. Since completing the research, Dr Cherell Cottrell Daniels moved to Health Choice Network; Dr Justin X. Moore moved to the University of Kentucky College of Medicine; and Ms. Angelique B. Willis moved to Michigan State University.
Acknowledgements
We are deeply grateful to the study participants for their valuable contributions to this project, as well as to the following team members who assisted with data collection and study coordination: Sharrill Bell, MPH, Fonda Doby, MPA, Gina Hopf, BSN, RN; Matthew Humphries, MS, CCRP, Jackie Luong, MPH, Kaylee Martin, Josephine Mhende, DrPH, MPH, Sarah Moore, Ayeesha Sayyad, MPH, and Marsha Wright, MPH.
Ethical Considerations
This study received Institutional Review Board approval from Georgia State University and through a Reliance agreement for Augusta University.
Consent to Participate
All participants provided informed consent which was documented by their signature either electronically or on paper.
Author Contributions
CAS and MST designed the study, acquired funding, and oversaw data collection, analysis, interpretation, and manuscript development. CAS, MST, LM, and JXM collaborated on original draft preparation. AB, CAS, and MST provided project administration. JXM conducted statistical analyses. AB, CCD, and ABW collected and managed data. All authors reviewed and edited the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Augusta University and Georgia State University Seed Award Program for Collaborative Clinical & Translational Research, awarded to Dr Claire Spears and Dr Martha Tingen. The content is solely the responsibility of the authors and does not necessarily represent the official views of Augusta University or Georgia State University.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, or publication of this article.
Data Availability Statement
Deidentified participant data will be made available upon reasonable request from the corresponding author.