
Abstract
Purpose
This study explores how social support and social norms influence Black and Hispanic adults’ experience in a weight management program, and if this varies based on race, ethnicity, and gender.
Approach
Semi-structured interviews and egocentric social network assessments.
Setting
Single primary care site in New York City.
Participants
Twenty Black and Hispanic adults in a weight management program.
Method
Interviews explored social influences on weight loss and differences based on demographics. Network composition and functions were characterized through social network analyses.
Results
Participants favored informational and tangible support to achieve health goals, through shared experiences and assistance, but felt social gatherings and unhealthy dietary norms undermined behavior change. Females described emotional strain, weight stigma, and the burden of balancing multiple social roles, whereas males emphasized health-related motivations and cultural dietary challenges. Among 276 network members identified, females tended to disclose program participation to friends, while males tended to disclose participation to people that provided them with health advice. Variability in social influence types and sources was primarily associated with gender, not race or ethnicity.
Conclusions
Social influences potentially play an important role in Black and Hispanic adults’ engagement in a weight management program, with notable gender differences. Incorporating social network members to facilitate specific forms of support and overcome unique social pressures may enhance the effectiveness of weight loss interventions.
Purpose
The prevalence of obesity in the United States (US) has continued to rise for several decades, particularly for certain racial and ethnic groups. 1 Non-Hispanic Black and Hispanic adults remain disproportionately affected by obesity compared to non-Hispanic White (NHW) adults, with a prevalence of 47.6%, 44.8%, and 37.9%, respectively. 2 Disparities also vary considerably by gender: among women, the prevalence of obesity is highest among those that are non-Hispanic Black (56.1%, vs 38.8% among NHW), but among men, the prevalence is highest among those that are Hispanic (41.2%, vs 36.9% among NHW). 2
Social networks, the social connections between people, 3 influence dietary choices and physical activity.4-6 A recent systematic review of interventions leveraging social networks to influence these health behaviors found that they improved several health outcomes. 7 However, only 1 of 37 identified interventions focused on weight reduction, while 2 focused on dietary outcomes and 2 on physical activity.7,8 The scarcity of social network interventions focusing on weight-related behaviors may be because key questions remain about which people and social processes should be the focus of such network interventions. Addressing these research gaps is of critical importance to intervening on obesity, particularly in high-prevalence populations.
Social network strategies that are integrated into weight management programs may need to be tailored for different types of network structures (eg, network size), network composition (eg, prevalence of family vs friends), and network functions (eg, social support). Social network features vary considerably by race, ethnicity, and gender. Specifically, Black adults often name fewer social network members, defined as meaningful social contacts, than NHW adults, while Hispanic adults name more network members including more extended family members. 9 Both Hispanic and non-Hispanic Black adults often have a higher proportion of family members relative to friends, alongside more frequent interactions and exchanges of social support.9,10 The kinds of social support offered in networks also vary by race and ethnicity. Following abnormal mammogram findings, the networks of Hispanic adults provided emotional support (encouragement), while those of NHW individuals provided informational and tangible support (facilitating follow up). 11 Social network characteristics also vary by gender: women generally maintain larger and less family-centered social networks, 12 and their social networks are typically more emotionally engaged than those of men.13,14 Despite these variations, little research has investigated the social networks of non-Hispanic Black and Hispanic men and women engaged in weight management programs. Advice-seeking and discussions about health are particularly critical for enhancing focused risk communication and encouraging behavioral lifestyle changes,15,16 yet few studies have described the interactions and social processes within these specific networks that facilitate and obstruct weight-behaviors.
This study employed qualitative and quantitative methods to explore how social processes influencing weight management may differ across race, ethnicity, and gender. Specifically, among non-Hispanic Black and Hispanic adults engaged in a weight management program, this study explored (1) social support and social norms influencing adoption and adherence to behavior change, and (2) characteristics of their social networks, including network members they disclose their program participation to and provide them with health advice.
Approach
This mixed methods study represents phase 1 of a randomized control trial. 17 The study was informed by social network theory, which elucidates the role of social relationships and social structure in transmitting information, channeling interpersonal influence, and enabling attitudinal or behavioral change. 18 Semi-structured interviews explored social relationships’ influences on attempts to lose weight, accounting for gender and racial or ethnic-based experiential differences. Additionally, personal (or egocentric) social network analysis explored the composition of participants’ social networks. 19 Data was integrated to develop an intervention focusing on leveraging the positive influence of social contacts, and mitigating their negative influences, to promote weight loss behaviors. The current report follows the Consolidated Criteria for Reporting Qualitative Research (COREQ) (Supplemental Table).20,21 Ethical approval to conduct the research was obtained from the BRANY Institutional Review Board (# 23-08-702-380).
Setting
Study participants were recruited 1/2024-6/2024 from a primary care-based weight management practice in an urban academic medical center. 22
Participants
Eligible participants had a body mass index ≥30 kg/m2, self-identified as Black or Hispanic, spoke English or Spanish, and participated in the program for ≥6 months. Anyone with an advanced medical illness or diagnosis impairing capacity to consent was excluded. Eligible individuals were invited to the study via postal mail, telephone, and email messages. Interested participants received a study information sheet before the study team received informed consent. Supplemental Figure presents the exclusion cascade. Demographic and clinical characteristics were abstracted from electronic health record (EHR), including: age, sex assigned at birth, self-identified ethnicity, race, marital status, preferred language, body mass index, and number of visits attended while enrolled in the program.
Method
Data Collection
Qualitative Interviews
Twenty individual interviews were conducted in person or via Zoom by an experienced member of the study team. Interviews lasted <60 min. Enrollment continued until thematic saturation was reached. 23 A semi-structured interview guide explored (1) social network influences on weight loss and (2) contrasting influences on weight loss for men and women.
Social Network Data
Personal social networks were assessed as part of the semi-structured interview using a standard name generator and questions about named network members.
19
Participants were prompted to name ≤15 meaningful social contacts, eliciting a sample of social contacts that have been established to reliably capture variability in the structure and composition of social networks. Participants responded to questions about the characteristics of each named social contact,
24
including:
Analysis Strategies
Qualitative Analysis
Interviews were transcribed verbatim using the audio-to-text feature in Microsoft Word. Original recordings and transcriptions were cross-referenced for accuracy and deidentified. Data was managed and analyzed using MaxQda 24. Deductive coding leveraged prominent models of social support and social network theory. Coding of social support and undermining aimed to capture 4 well-established forms of social support: (1) informational support, transmitting information; (2) tangible support, providing resources, including time, money, or labor; (3) emotional support, providing empathy or comfort, and (4) esteem support, acting to alter someone’s self-confidence and sense of self-worth. 25 Gender norms and influences beyond social network support and undermining were coded inductively as they emerged. Transcripts were coded by 2 of 3 independent coders. New codes and categories were added to a codebook iteratively. The principal investigator debriefed regularly with the coders to review codes and reconcile discrepancies. After all transcripts were analyzed, codes were collated into potential categories by 2 coders independently. Potential themes were discussed and reworked with the additional involvement of study authors until key themes were generated. Names for themes and sub-themes were agreed upon by all authors and presented with illustrative quotes.
Quantitative Analysis of Participant and Personal Social Network Data
Baseline characteristics of study participants are presented using frequencies and percentages for categorical variables and median and interquartile range (IQR) for continuous variables. Participants’ personal social network data were analyzed using R, SAS, and Stata. Network size was defined as the total number of social network members listed by each participant. Proportions of each participant’s network were calculated: (1) who had a particular relationship category, (2) whom the participant had contact with once a day, (3) to whom the participant had disclosed the program (reflecting emotional and esteem support), and (4) whom the individual viewed as health advisors (reflecting tangible and informational support). Descriptive statistics report the mean, standard deviation, and range of each characteristic across the study sample, and for sub-groups of study participants (male, female, Hispanic, Black). Visualizations of participants’ personal networks were generated using R. Because this study did not measure social networks among the named network members (ie, who knows whom), it was not possible to compute some network structure characteristics, such as network density.
Analyses of the personal social network were also conducted at the dyad level (ie, focused on each study participant-network member pair). Frequency of the social role (eg, family, friend) for network members with each role (disclosed to, health advice) were reported for all participants, and for the same participant sub-groups of interest. Dyad-level associations between network members to whom program participation was disclosed, and those who were health advisors, were also explored. Pearson correlation coefficients were used to assess the strength and significance of the association between 2 dyadic variables: “disclosed the program to” and “health advisor.”
Results
Of the 20 index participants, 65% were female, 40% identified as Hispanic, and 60% identified as Black with a median age of 53.5 years across all index participants. Male participants were overall younger than females (47 years vs 55 years of age). Half of the participants had never been married (50%). Participants overall median BMI was 35.9 kg/m2 with male participants having a higher median BMI in comparison to females (41.9 vs 33.3 kg/m2).
Social Support and Social Norms - Qualitative Findings
Most differences in social support and norms emerged between genders rather than self–identified racial or ethnic grouping. For each theme, commonalities between genders are presented, then differences.
Social Network Influences on Weight Management
Social Support Facilitators to Weight Management
Facilitators to weight loss emerging among all genders included esteem, informational, and tangible support from their social networks. They received informational and esteem support by sharing weight-loss experiences with network members, including having friends and family who struggled with weight loss themselves, but who offered encouragement to lose weight, set joint weight behavior goals (eg, “cutting out soda and increasing water intake”), and shared different types of foods. Tangible support (also from family and friends) included receiving assistance with shopping for and preparing food, and mutually engaging in physical activity, including walking, sharing exercise routines, and bonding through joint experiences. Tangible support through non-weight related tasks, including running errands, helped make time to focus on weight loss activities.
Females felt that non-weight related emotional support from friends (eg, shared experiences like attending concerts) substituted emotional eating. They received esteem support from others modeling weight behaviors: one was inspired to implement healthy habits by their son’s health journey, while others were influenced by family members to adopt vegetarian or vegan diets. No social network social support facilitators emerged uniquely among males.
Social Support Challenges to Weight Management
Participants described social undermining, primarily through unhealthy dietary norms influencing their dietary choices. Social experiences, including dining out, often increased exposure and temptations to unhealthy options. They often felt pressured to make unhealthy food choices to fit in with family, accommodating the preferences of others, particularly of children, for fast food and takeout.
Females also discussed receiving unwanted and uninvited informational, emotional, and esteem support, as well as direct and indirect undermining. Several described frustration with their mothers expressing concerns about their weight, their bodies and what they ate. Others described childhood experiences with weight-related comments intended as support or more direct critiques, which impacted their adult relationship with food. Beyond family members, uninvited comments about weight were perceived as upsetting and frustrating, and even specific tones and word choices used when talking about weight could be hurtful. They mentioned being hyperaware of inflections, micro-expressions, annoying comments, negative people, others being blunt, and cultural terms like “gorda” or “gordita”. They also described how family members unintentionally undermined their goals, stating physical activity was interrupted by kids complaining or not mutually engaging in exercise. Males described receiving undermining esteem and tangible support, by feeling pressured to eat unhealthy foods to fit in and relying on partners or family members for food.
Beyond Social Support: Other Social Influences on Weight Management
Behaviors
Participants expressed that, generally, men eat more while women are limit how much they eat. Males felt men frequently have jobs that are more physically demanding.
Biology
Females felt weight loss is easier and faster for men than for women, and that hormonal fluctuations affected their physique. Males explained that genetics and age can affect body size, shape, and metabolism.
Body Image
Females felt they were more conscious and critical of body image and appearance than men. They emphasized the relationship between body image and dressing, including how the body affects the way women dress, how dressing can affect body image (eg, “when sizes are not available”), and how dressing can be used to change body image (eg, “girdles”, “body shapers”). Males felt they also felt pressure to be attractive but were not vocal about it. Black males, specifically, discussed how stereotypes impacted self-image: “Black men are often perceived as big and aggressive”. Males felt women may seek to lose weight to “maintain her husband’s attraction”.
Culture
Participants noted cultural variations in beauty standards for women, but felt they were “tougher” for women than men. Females felt cultural pressures to prepare and accept food, and, in some cases, to undergo surgery to achieve a certain appearance. Males described cultural variations in perspectives on body shapes/sizes. One explained that some cultures prioritize male body shapes associated with physical labor, while another mentioned: “African-Americans may have a higher prevalence of larger body sizes compared to other cultures.” Males also explained that culture, alcohol intake, and eating habits are related to each other. One male stated: “Late-night eating is also a cultural influence, with some cultures, like the Caribbean, eating before and after parties where alcohol is consumed.”
Motivation
Participants felt women are primarily motivated by social pressures to lose weight. Females, but not males, mentioned that professional help could be beneficial to losing weight. Males were motivated to lose weight by goals to improve their health.
Societal Expectations
Participants felt there were “double standards” related to weight, with women being judged more harshly and feeling more societal pressure to lose weight. Females felt many societal pressures placed on them: “Women are expected to do it all, take care of the family, work, and look pretty at the same time”. Females, exclusively, discussed the stigma associated with being overweight: “Fat shaming is prevalent in society.” Males discussed societal stereotypes, including body “prejudices associated with certain body types, particularly for black men”, and noted that social media promotes certain body shapes or sizes.
Stress
Females explained that people, particularly women, sometimes “eat their stress away”, and mentioned specific stressors, like relationships and school/work: “Men may not have as much stress as women and may rely on their partners to handle it”.
Structural Influences
Several environmental cues posed challenges to losing weight, including the lack of healthy options at restaurants and the large serving sizes. Females mentioned financial limitations to food access and expressed frustration with wasting money on food that is not eaten.
Quantitative Findings
Social Network Characteristics
Characteristics of Social Network Members (n = 276) Nominated by Index Participants (n = 20) Stratified by Gender
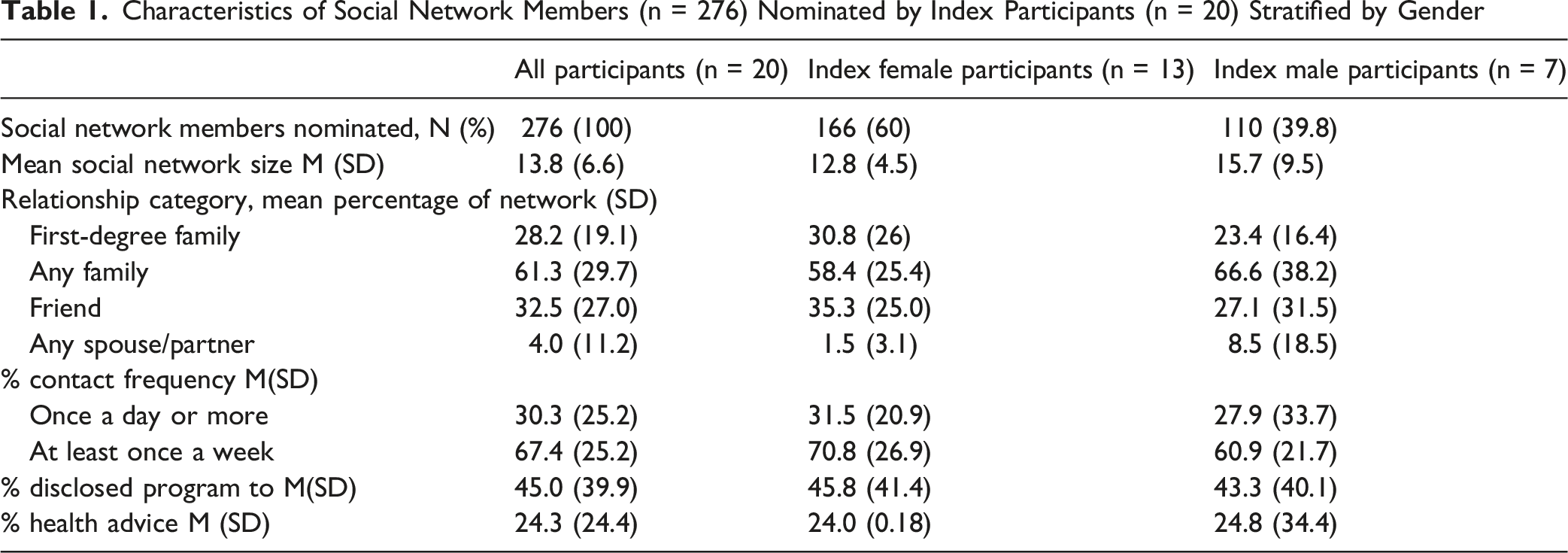
Social network characteristics of female and male participants were similar. Males tended to have a larger proportion of family, and smaller proportion of friends in their networks, compared to females. Females trended toward having frequent contact with a greater proportion of their network, compared to males. However, considering subgroup size, trends may not be robust.
Network Members to Whom the Program Was Disclosed and Who Were Health Advisors
Participants reported having disclosed their participation in a weight loss program to less than half (45.0%) of their network. About one-quarter (24.3%) were people whose health advice mattered to them. Personal network characteristics for each of the 20 study participants are visualized in Figure 1. Visualizations of participant personal networks displaying network members whom: (a) the participant had disclosed their weight loss program participation, and (b) whose health advice mattered to them. Personal networks are displayed starting with those with the lowest percentage of network members with a given feature through to those with the highest percentage. Black nodes = participant; grey nodes = social network member; orange nodes = network member to whom the participant disclosed their weight loss program participation; red nodes = network member whose health advice mattered to them. (a) Program disclosure, (b) Health advisor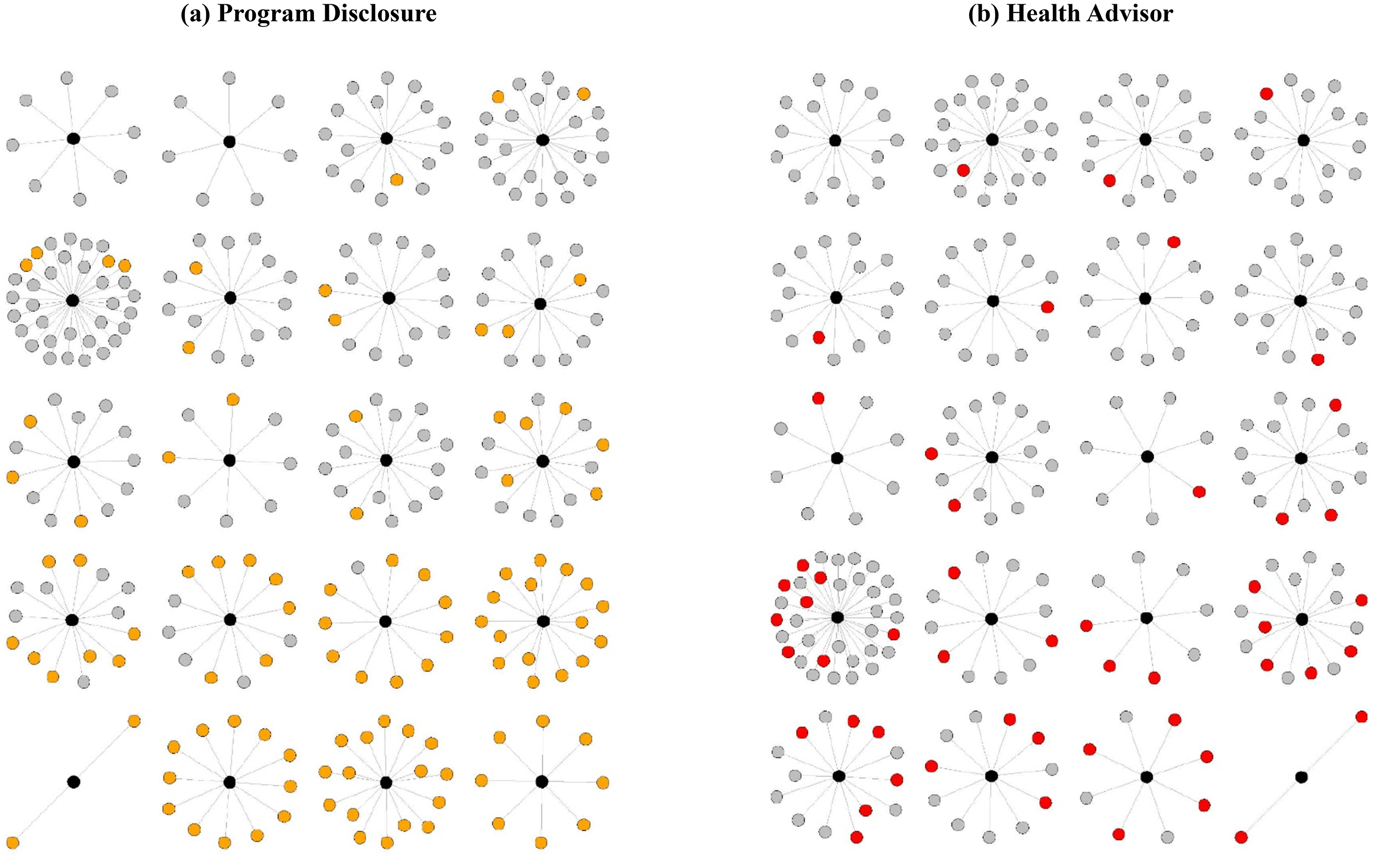
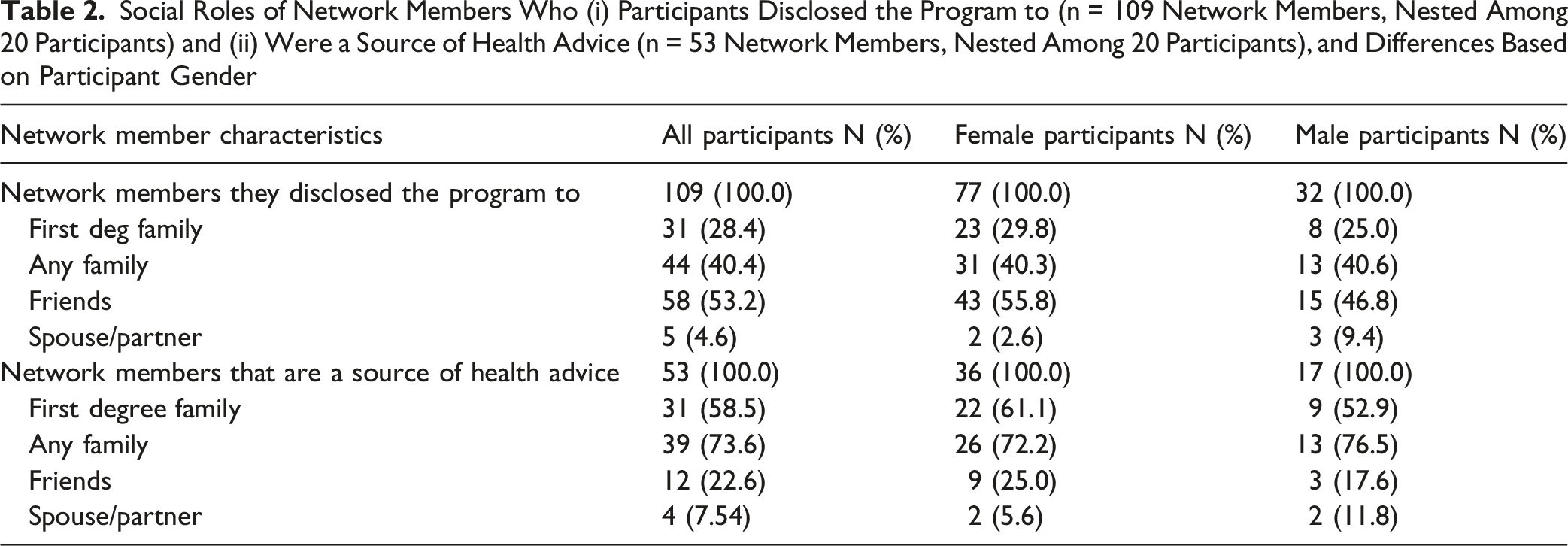
Social Roles of Network Members Who (i) Participants Disclosed the Program to (n = 109 Network Members, Nested Among 20 Participants) and (ii) Were a Source of Health Advice (n = 53 Network Members, Nested Among 20 Participants), and Differences Based on Participant Gender
Finally, there was overlap in dyads to whom participants disclosed their program participation and those identified as health advisors, so-called “multiplex” relationships (Figure 2). Among all participants, this overlap was modest (r = 0.28, P < .01), indicating a small positive association. However, this pattern differed by gender: the correlation was moderate among males (r = 0.44, P < .01), but weaker, though still significant, among females (r = 0.18, P = .01). This indicates that males had a stronger tendency to disclose their program participation to same people they viewed as health advisors, while females were more likely to disclose to people who were not health advisers. Associations were consistent across racial and ethnic groups, with similar positive correlations observed among both Black (r = 0.28, P < .01) and Hispanic participants (r = 0.30, P < .01). Illustration of a personal social network of one fictious participant (black node), their social network members (grey nodes), and the extent to which these social relationships entail specific functions: (a) weight loss program disclosure, and (b) health advice. Across all participant-network member pairs (dyads), if these 2 types of relationships (a) and (b) consistently co-occur in the same dyads the correlation in the relationships will be strong, but if the relationships rarely co-occur in the same dyads the relationship correlation will be weak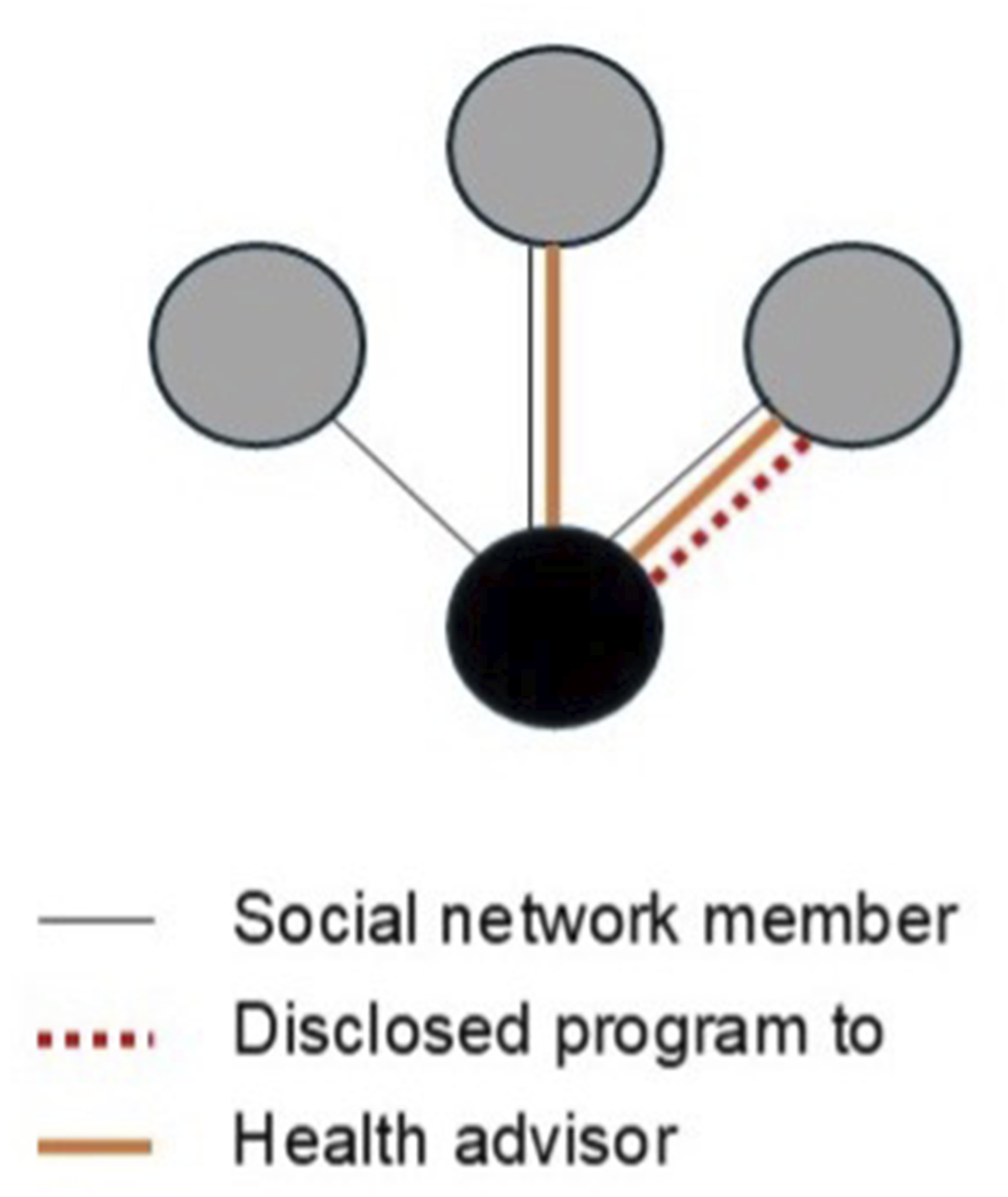
Integrated with qualitative findings, these patterns suggest differences in how social networks are engaged. Women’s reports of unsolicited support, weight stigma, and heightened sensitivity to weight-related commentary may help explain both the overall tendency to disclose program participation to fewer than half of network members and the weaker overlap between disclosure and health advisory ties among females. Women may selectively disclose health behaviors to avoid judgment or emotional burden. Additionally, balancing caregiving, social expectations, and personal health may contribute to a mismatch between emotionally supportive relationships and those from whom health advice is sought, resulting in a fragmentation of support functions across their networks.
Discussion
This mixed-methods study of non-Hispanic Black and Hispanic adults engaged in a weight management program highlights the gendered nature of social influences on weight-related behaviors. Informational and tangible support were valued, while unhealthy dietary norms within social settings often undermined behavior change. Women, however, described greater exposure to emotional burden, unsolicited support, and weight stigma, reflecting broader social expectations that shaped their experiences. Integration of qualitative and network findings suggests that these lived experiences are reflected in measurable social network patterns. Gender differences in disclosure and health advisory roles suggest adaptive strategies for managing stigma, social expectations, and role-related strain may emerge within social networks.
Prior research demonstrates that social support, social pressure, and social norms influence obesity-related behaviors, 26 but the current study provides additional insight into how these processes differ by gender among Black and Hispanic adults with obesity. Although about a quarter of social network members provided participants with useful health advice, the qualitative interviews highlighted that males did not receive emotional support from their social networks. Prior research suggests men are less likely to exchange emotional support.14,27 Females emphasized the benefits of emotional support and the stress associated with unsolicited or undermining interactions. Women may experience greater social strain within their networks, potentially due to larger and more socially engaged networks or more frequent and emotionally intensive interactions. 28 Regardless, interventions for weight management should aim to address these stressors.
Females tended to have more friends and frequent contact within their networks. When interpreted alongside the qualitative findings, these patterns suggest that women’s networks may be broader but also more socially complex, increasing exposure to both supportive and undermining interactions. Although both males and females demonstrated a positive association between program disclosure and health advisory ties, this relationship was notably weaker among females. In contrast, the stronger overlap observed among males may indicate more functionally consolidated networks, where individuals who are trusted sources of advice are also those with whom health behaviors are shared. Together, these findings suggest that differences in network structure may reflect adaptive strategies for managing social risk and support within gendered social contexts.
More broadly, integrating the qualitative and network findings highlights how lived social experiences are reflected in measurable network configurations. The observed partial disconnect between disclosure and advisory ties suggests that not all supportive relationships are perceived as safe or appropriate for health-related discussions. These dynamics underscore the importance of considering both the structure of social networks and the roles of social network members when designing network-informed interventions. Multiplex ties may represent efficient targets for intervention, particularly among men where these roles are more closely aligned. Among women, interventions may benefit from engaging different network members for distinct functions, such as leveraging friends for disclosure and emotional support, and family members or partners for informational or tangible support. The prominence of friend-based disclosure and family-based advising further suggests that aligning intervention strategies with naturally occurring support roles may enhance effectiveness.
Notably, these findings should be interpreted cautiously. Dyadic observations are nested within individuals, and the number of male participants was small. Correlation estimates, especially those stratified by gender, may be sensitive to the influence of a limited number of participants or network ties. These findings are therefore best understood as hypothesis-generating and illustrative of potential patterns, rather than definitive estimates of association.
Weight management interventions should consider the intersectionality of identities, particularly how cultural and gender norms shape social interactions. Engaging partners or close ties in interventions may offer meaningful benefits, particularly for facilitating shared behavior change within households. A survey of over 253 experienced lifestyle coaches found that 83% had delivered interventions to partners, suggesting that dyadic models are both acceptable and commonly implemented. 29 Participation in partnered lifestyle interventions has been associated with improved outcomes among men, including a 4-fold increase in the odds of achieving ≥5% weight loss compared with those participating alone. 30 This approach may not be equally beneficial to all. We found women described substantial emotional burden and role strain, consistent with evidence that women often provide more social support than they receive. 28 This imbalance may help explain why partnership-based effects have not been observed among women in prior studies: female partners often facilitate household behavior change without experiencing equivalent benefit themselves. Together, these findings suggest that dyadic approaches hold promise, but require adaptation to ensure they do not inadvertently increase burden on women and instead equitably support their needs within the context of gendered social roles.
Limitations
This study has several limitations. Participants were recruited from a single academically-affiliated site. Gender was based on sex assigned at birth, and gender-related findings reflect participants’ reported experiences rather than formally measured constructs. Comparisons of themes across gender were based on qualitative interpretation, not quantitatively tested. Social network data relied on participant self-report, subject to recall and social desirability bias. Network nominations were limited to 15 people, potentially biasing network members enumerated. These factors may influence network characteristics computed and observed overlap between social roles. Quantitative network analysis was not designed to assess whether specific network members systematically provided specific types of support; future work with larger samples could better examine these patterns. The egocentric network design and modest sample size (n = 20) limit statistical inference. Although 276 network members were identified, dyadic observations are not independent and are nested within participants. Correlation estimates may be unstable, especially for male participants, where smaller sample sizes may amplify variability. Findings should be interpreted as exploratory and hypothesis-generating rather than definitive.
Conclusion
This mixed-methods study of non-Hispanic Black and Hispanic adults engaged in a weight management program highlights the complex nature of social influences on weight-related behaviors. Informational and tangible support were widely valued, while unhealthy dietary norms within social settings often undermined behavior change; women, in particular, described greater exposure to emotional burden, unsolicited support, and weight stigma, reflecting broader social expectations that shape engagement with their networks. Integration of qualitative and network findings suggests that these lived experiences are reflected in how individuals structure and engage their social relationships, with specific network features including multiplex ties, friend-based disclosure, and family-based advisory roles emerging as actionable targets for intervention. Multiplex ties may offer opportunities to align support functions within single relationships, while differences in how disclosure and advice-seeking occur across relationship types highlight the need to tailor strategies to distinct network roles, and based on some unique needs and social contexts of females and males. Despite their promising influence on dietary choices and physical activity, social network interventions have not been leveraged to address racial disparities in obesity. Key questions remain about which people and social processes should be the focus of such interventions. Non-Hispanic Black and Hispanic adults in weight loss interventions appreciate receiving informational and tangible social support, but social norms related to weight and weight behaviors can often undermine behavior change, particularly for women. Men and women may also differ in whom within their social networks they seek health advise from. Findings underscore the importance of developing network-informed interventions that intentionally engage key person-specific social network members, enhance supportive interactions, and mitigate social barriers to sustained behavior change.So What? (Implications for Health Promotion Practitioners and Researchers)
What is Already Known on This Topic?
What Does This Article Add?
What Are the Implications for Health Promotion Practice or Research?
Supplemental Material
Supplemental Material - Opportunities for Leveraging Social Networks in Behavioral Lifestyle Interventions for Black and Hispanic Adults With Obesity: A Mixed Methods Approach
Supplemental Material for Opportunities for Leveraging Social Networks in Behavioral Lifestyle Interventions for Black and Hispanic Adults With Obesity: A Mixed Methods Approach by Christopher J. Gonzalez, Natasha Wasim, Anika Lewis, Mussarat Nahid, Kayla de la Haye, and Erica Phillips in American Journal of Health Promotion
Footnotes
Ethical Considerations
Obtained from the BRANY Institutional Review Board (# 23-08-702-380).
Author Contributions
CJG, KH, EP contributed to the conceptualization and analysis of the study, and writing of the original draft. NW, JC, AL and MN contributed to the analysis and writing-review and editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication is supported by the National Institute of Diabetes Digestive and Kidney Diseases of the National Institutes of Health under Award Number R01DK135949 (EP) and Award number K23 DK139410-01A1 (CJG). Research reported is also supported by the National Center for Advancing Translational Sciences of the National Institutes of Health under Award Number UL1TR002384. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
De-identified data from this study are not available in a public archive. De-identified data from this study will be made available (as allowable according to institutional IRB standards) by emailing the corresponding author. Materials used to conduct the study are not publicly available.
Availability of Analytic Code
Analytic code used to conduct the analyses presented in this study are not available in a public archive. They may be available by emailing the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.