
Abstract
Purpose
Examine the long-term association between asthma and mental health conditions in Australian men.
Design
Retrospective cohort study.
Setting
Ten to Men project from four waves (2014–2022).
Subjects
16,021 Australian men (aged ≥ 18 years) at baseline.
Measures
Exposure was self-reported asthma. Outcome measures were depression, anxiety and their comorbidity, assessed through self-reports and validated screening tools. Key covariates included survey year (waves), sociodemographic, lifestyle variables and comorbidities.
Analysis
Chi-square test (χ²) of independence for prevalence analysis and generalised estimating equation models for examining associations between asthma and mental health conditions, adjusting for relevant covariates.
Results
Across survey years, the prevalence of depression ranged from 12.8% to 33.2%, while anxiety ranged from 17.3% to 51.3%. Comorbid depression with anxiety ranged from 11% to 28%, with the highest prevalence reported in 2020. Asthma was significantly associated with higher risks of depression (RR = 1.23, 95% CI: 1.16, 1.30), anxiety (RR = 1.12, 95% CI: 1.05, 1.18), and comorbid depression with anxiety (RR = 1.27, 95% CI: 1.17, 1.38). Significant risk factors included survey year (2020 and 2022), sleep disturbances and being a former or current smoker.
Conclusion
A significant association between asthma and mental health disorders, particularly depression, anxiety, and their comorbidity was identified in Australian men. These highlight the need for an integrated approach to respiratory and mental health care, with particular emphasis on targeted screening and interventions.
Introduction
Chronic respiratory diseases (CRDs) are non-communicable diseases that affect the lungs and respiratory airways, significantly constituting a major public health challenge globally. 1 Chronic obstructive pulmonary disease (COPD) and asthma are the most prevalent CRDs worldwide, and are characterised by symptoms such as increased sputum production, dyspnoea, persistent cough, wheezing, chest tightness and fatigue.1,2 In 2019, CRDs were the third most common cause of mortality, accounting for four million deaths, with 454.6 million cases recorded globally. 3 The burden of CRDs in Australia is concerning, as they accounted for 29% of mortality in 2022, and 7.2% of total disease burden in 2023, with their prevalence threatening to increase in future years due to continuous exposure to risk factors.1,4 Whilst previous studies have mostly reported the impact of CRDs on patients’ physical health, limited attention has been given to their effects on mental health and associated risk factors. 5
Mental health disorders such as depression and anxiety are common comorbidities among individuals living with CRDs. 6 The association between these mental health conditions and CRDs has been described as “two-way”, with increasing evidence suggesting that sleep problems may be a mediating factor due to the shared pathophysiological pathways with depression and CRDs.6–8 This underscores the importance of the Global Initiative for Chronic Obstructive Lung Disease’s recommendation to actively screen for and co-manage psychological comorbidities in persons living with CRDs.7,9 Other health strategies suggested by the Lung Foundation Australia included promoting pulmonary rehabilitation, integrating mental health screening and support services in respiratory care and encouraging lifestyle changes such as smoking cessation, regular physical activity and a healthy diet.10,11 Whilst most of these strategies are currently implemented in clinical settings, the findings from this study will strengthen the rationale for these practices and add in-depth insights that could inform guidelines and policies in managing patients with these conditions. 10
Although depression and anxiety are consistently reported to be more prevalent among females, the scenario among men remains underreported. 12 In the Australian context, previous studies have indicated that CRDs are more common in men, who also exhibit shorter life expectancy at birth, lower rates of health-seeking behaviour and a greater likelihood of experiencing health complications compared to females.1,13,14 Therefore, the present study will focus on male health, aligning with a growing body of research and public health interest in this area. In response to these disparities, the Australian Longitudinal Study on Male Health (Ten to Men) was funded to explore male health, identify key determinants impacting quality of life, and inform policies aimed at improving the health and well-being of Australian men.15,16 In view of the foregoing, this study aims to examine the association between CRDs and mental health disorders (depression and anxiety) among Australian men, using four waves of the Ten to Men data as the primary aim of this study. A secondary aim was to identify the risk factors for depression, anxiety and comorbid depression with anxiety in Australian men living with CRDs. Understanding these relationships is crucial for developing more effective, collaborative care strategies for Australian men living with CRDs, potentially improving both physical and mental health conditions in this population.
Methods
Study Design and Setting
Participants’ Characteristics Across the Study Waves (2014 – 2022)
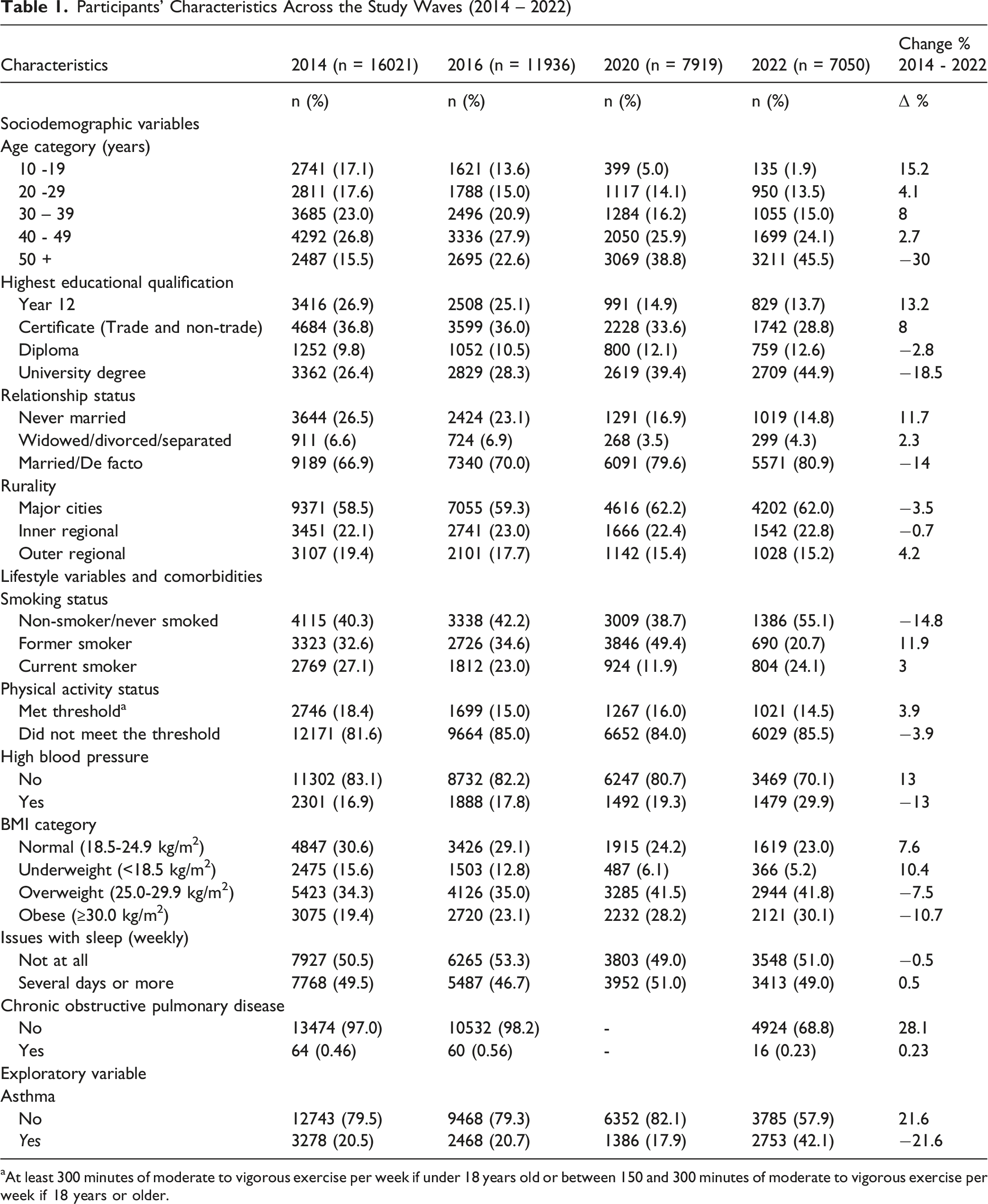
aAt least 300 minutes of moderate to vigorous exercise per week if under 18 years old or between 150 and 300 minutes of moderate to vigorous exercise per week if 18 years or older.
Study Variables
Exposure variable
The exposure variable for this study was self-reported COPD or asthma measures across the four waves of the Ten to Men datasets. In waves 1 and 2, participants were asked, “Has a doctor or other health professional ever told you that you had this condition (lifetime or in the last 12 months): emphysema or chronic obstructive pulmonary disease, chronic bronchitis or asthma?” In waves 3 and 4, participants were asked, “Has a doctor or other health professional ever told you that you had this condition (lifetime or in the last 12 months): asthma or chronic lung disease (other than asthma)? Since emphysema and chronic bronchitis are the two main types of COPD, participants who responded “Yes” to either emphysema or chronic bronchitis were considered to have COPD.
Outcome variables
There were three outcome variables for this study, including depression, anxiety disorders and comorbid depression with anxiety, which are described below.
Depression
Across the four waves, participants were asked, “Has a doctor or other health professional ever told you that you had this condition: depression in your lifetime or in the past 12 months?” They were also asked if they had experienced symptoms or received treatment for depression in the past 12 months. Specific types of depression included major depression/major depressive disorder, postnatal depression (PND), psychotic depression, other types of depression, and depression of unknown type were also assessed for both lifetime and the past 12 months. Participants with a ‘Yes’ response to any of the above questions were regarded as having a major depression. The Ten-to-Men study administered the patient health questionnaire (PHQ-9). The PHQ-9 is a 9-item self-report tool designed to screen for, diagnose and measure the severity of depression in adults, including in primary care settings. It rates symptoms from the past two weeks with scores ranging from 0 to 27. Scoring 10 and above was classified as having moderate to severe depression. 17
Anxiety disorders
Participants were asked if a doctor or other health professional had ever diagnosed them with an anxiety disorder (lifetime or in the past 12 months), “Has a doctor or other health professional ever told you that you had this condition: an anxiety disorder in your lifetime or in the past 12 months?” They were also asked if they had experienced symptoms or received treatment for other anxiety disorders in the past 12 months. Specific anxiety disorders included generalised anxiety disorder (GAD), social anxiety disorder, and other anxiety disorders, as well as anxiety disorders of unknown type. These were similarly assessed for lifetime and the past 12 months. Participants with a ‘Yes’ response to the questions on anxiety (GAD-7 score was used for adults and SPENCE-Anxiety Scale for children) were regarded as having an anxiety disorder. 14 Responses to the self-reported and screening tools were harmonised to determine anxiety.
The PHQ-9 and GAD-7 are widely used and well-validated screening tools with established reliability and validity for assessing depressive and anxiety symptoms in population-based and clinical settings. 17 The PHQ-9 has demonstrated high internal consistency and good sensitivity and specificity for major depressive disorder, 18 while the GAD-7 shows robust psychometric performance for generalised anxiety disorder. 19 The SPENCE Anxiety Scale has similarly demonstrated acceptable reliability and validity in younger populations 20 These instruments are commonly applied in large epidemiological studies, supporting the reliability and comparability of mental health outcomes across study waves.
Comorbid depression with anxiety
Participants who reported ‘Yes’ to the questions on both depression and anxiety disorders or had scores indicative of either of the two conditions, were taken as experiencing both mental health conditions.
Confounding variables
These included the sociodemographic, health, lifestyle and comorbid condition factors based on previously identified evidence. For the demographic factors, these included age 21 categorised into five groups: 10 – 19 years, 20 – 29 years, 30 –39 years, 40 – 49 years, and 50 years and older. The highest level of education2 22 was classified as Year 12 or higher; while rurality 23 was defined based on residence in major cities, inner regional, or outer regional areas. 24 Relationship status 25 was categorised as never married, widowed, divorced, separated, or married/de facto.
Health and lifestyle factors included smoking status 26 classified as never smoked, former smoker, or current smoker. Physical activity levels were determined based on the Australian 27 and the World Health Organisation guidelines, 28 with participants categorised as engaging in adequate or inadequate physical activity. Body mass index (BMI) was treated as a categorical variable with four classifications: normal, underweight, overweight, and obese. 29
Comorbid conditions examined included having diabetes (No/Yes), high blood pressure (No/Yes) and sleep issues (not at all/several days or more). Participants were asked, “Over the last 2 weeks, how often have you been bothered by any of the following problems? Trouble falling asleep, staying asleep or sleeping too much”
Statistical Analysis
Categorical data were summarised as counts and percentages for all sociodemographic, health, lifestyle and comorbid conditions across four waves: Wave 1: 2013 – 2014; Wave 2: 2015 – 2016; Wave 3: 2020 – 2021 and Wave 4: 2022-2023. This was followed by examining the prevalence of depression, anxiety, and comorbid depression and anxiety using the Chi-square test of independence.
Attrition in the Ten to Men study has been shown to depend on observed characteristics such as age, education, employment, rurality, and baseline physical and mental health. These patterns are documented in the Ten to Men technical reports. 16 Since missingness is related to measured factors and these variables were included in the model, the missing-at-random assumption is considered reasonable.16,30 We acknowledge that attrition across waves may introduce selection bias; however, its impact is likely reduced through adjustment for these observed covariates. 16 The Ten to Men study recruited 16021 participants at baseline. Retention across subsequent waves was 75% at Wave 2, 49% at Wave 3, and around 44% by Wave 4. 31
Generalised Estimating Equation (GEE) models were used to analyse the data, allowing for the inclusion of all available observations across study waves. Participants contributed data to the analysis for any wave in which they had complete information on the variables of interest, rather than being excluded entirely due to missing data at other time points. This approach maximises statistical power and reduces potential bias associated with complete-case exclusion, while appropriately accounting for the correlation of repeated measurements within individuals over time. Since missingness in the Ten to Men study is related to measured factors such as age and education, and these variables were included in the GEE models, we applied a missing at random (MAR) assumption, which is considered a robust approach to reducing selection bias. A log link function with a Poisson distribution was specified to directly estimate relative risks (RRs), which are more interpretable than odds ratios for the outcomes of this study. Adjusted RRs and their 95% confidence intervals (CIs) were estimated from the multivariable GEE models.
To examine the association between CRDs and depression, anxiety and comorbid depression with anxiety, a series of GEE models with a log link, exchangeable correlation structure, and robust variance estimation were performed. In the first model (Model 0), the GEE model was used to adjust for sociodemographic factors, including the waves. In the second model (Model 1), sociodemographic factors were added to the health and lifestyle factors, and the GEE model was used to adjust for the association. In the third GEE analysis (Model 2), socio-demographics, health, and lifestyle factors were added to the comorbid conditions. In the last model (Model 3), sociodemographic, health and lifestyle with comorbid conditions factors were added to the main predictor, CRDs. This modelling strategy compared the relationship between each set of confounding variables in examining the association between CRDs and depression, anxiety, and comorbid depression with anxiety.
This study was reported following the guidelines for reporting retrospective cohort studies, Strengthening the Reporting of Observational Studies in Epidemiology (STROBE). 32 All analysis were done using R-software, version 4.2.0 (R Foundation for Statistical Computing, Auckland, New Zealand). Associations were considered statistically significant at P < 0.05 level.
Results
Table 1 summarises participants’ characteristics across the study waves. Over time, the cohort became older and more highly educated, with the proportion of participants holding a university degree increasing from 26.4% in 2014 to 44.9% in 2022. Health risk factors increased across study waves. The prevalence of high blood pressure increased from 16.9% in 2014 to 29.9% in 2022, while obesity rose from 19.4% to 30.1% over the same period. Smoking rates declined modestly, with current smoking decreasing from 27.1% in 2014 to 24.1% in 2022. Physical inactivity remained consistently high, with over 80% of participants not meeting recommended physical activity levels across all waves. Sleep problems were also common, with approximately half of participants reporting sleep issues weekly throughout the study period. Although the Ten to Men data collected information on both asthma and COPD, preliminary analysis revealed a low number of participants diagnosed with COPD. Therefore, subsequent analyses in this study primarily focused on individuals with asthma to ensure robust statistical power and meaningful findings (Table 1).
Prevalence of Mental Health Conditions Among Men with Asthma
Figure 1 shows the prevalence of mental health conditions among men with asthma across the four study waves. There was a significant variation in the prevalence of depression (χ2 = 339.53, P < 0.001), anxiety (χ2 = 946.37, P < 0.001), and comorbid depression with anxiety (χ2 = 273.06, P < 0.001). Depression remained relatively stable between 2014 (30.7%) and 2016 (29.3%), increased to 33.2% in 2020, and then declined to 12.8% in 2022. Anxiety increased markedly from 17.3% in 2014 to 51.3% in 2020, before decreasing to 40.6% in 2022, although remaining higher than pre-2020 levels. Similarly, comorbid depression with anxiety more than tripled, increasing from 9.3% in 2016 to 28.0% in 2020 before declining to 11.4% in 2022. The peak observed in 2020 aligns with the COVID-19 period and likely reflects broader psychosocial disruptions during that time.
33
Age-adjusted prevalence of mental health conditions among Australian men living with asthma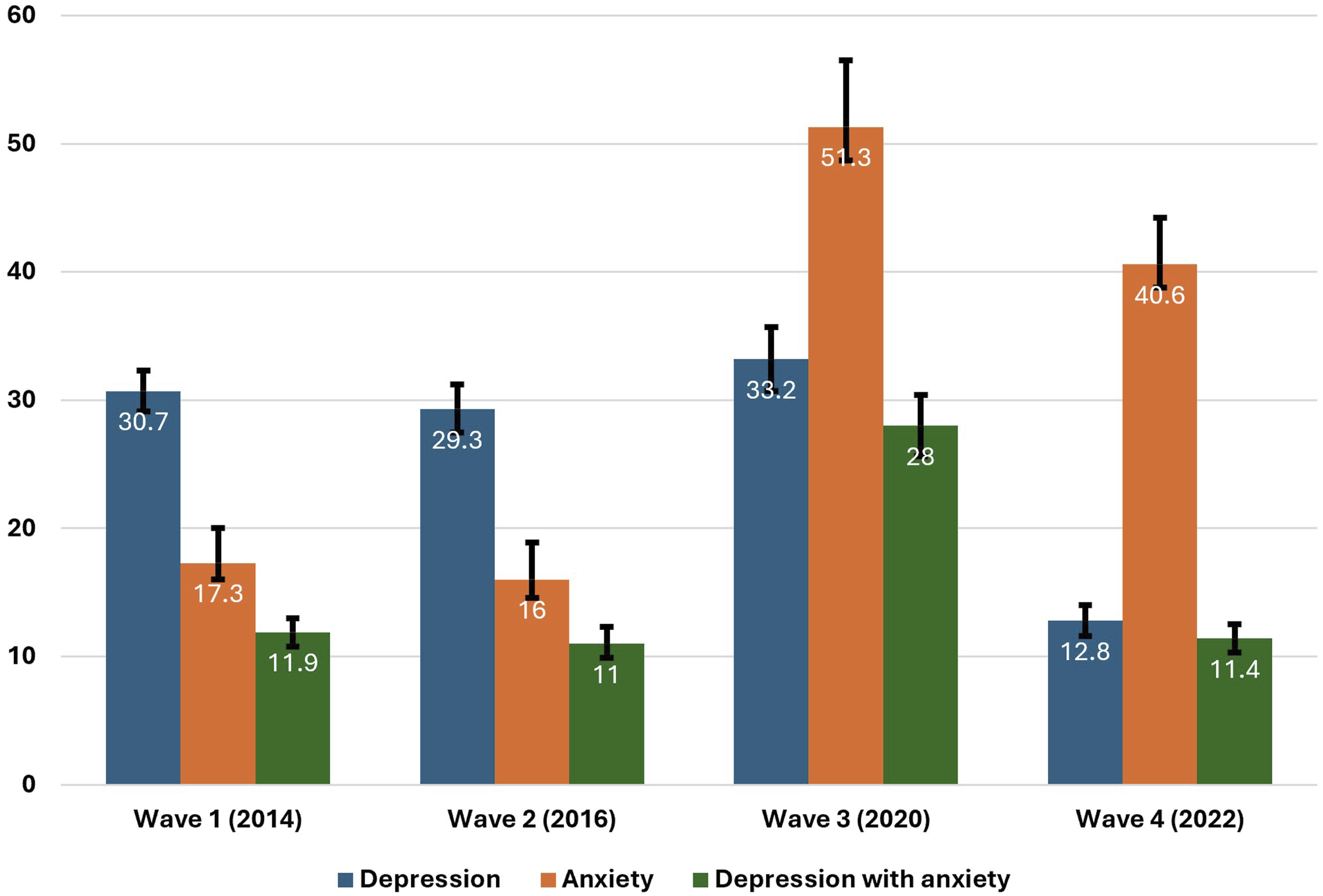
Association Between Asthma and Mental Health Conditions
Association Between Asthma and Depression
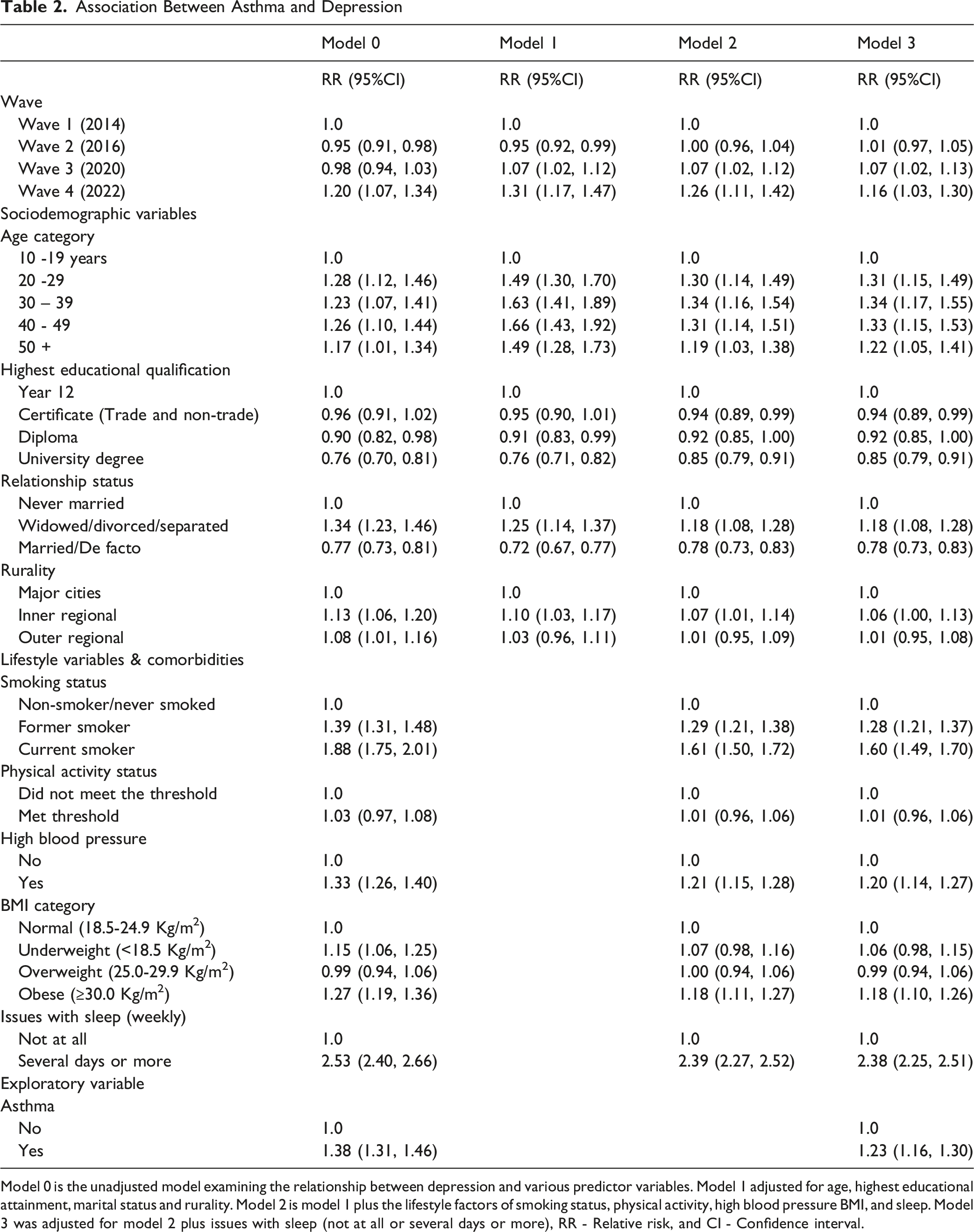
Model 0 is the unadjusted model examining the relationship between depression and various predictor variables. Model 1 adjusted for age, highest educational attainment, marital status and rurality. Model 2 is model 1 plus the lifestyle factors of smoking status, physical activity, high blood pressure BMI, and sleep. Model 3 was adjusted for model 2 plus issues with sleep (not at all or several days or more), RR - Relative risk, and CI - Confidence interval.
Association Between Asthma and Anxiety Disorders
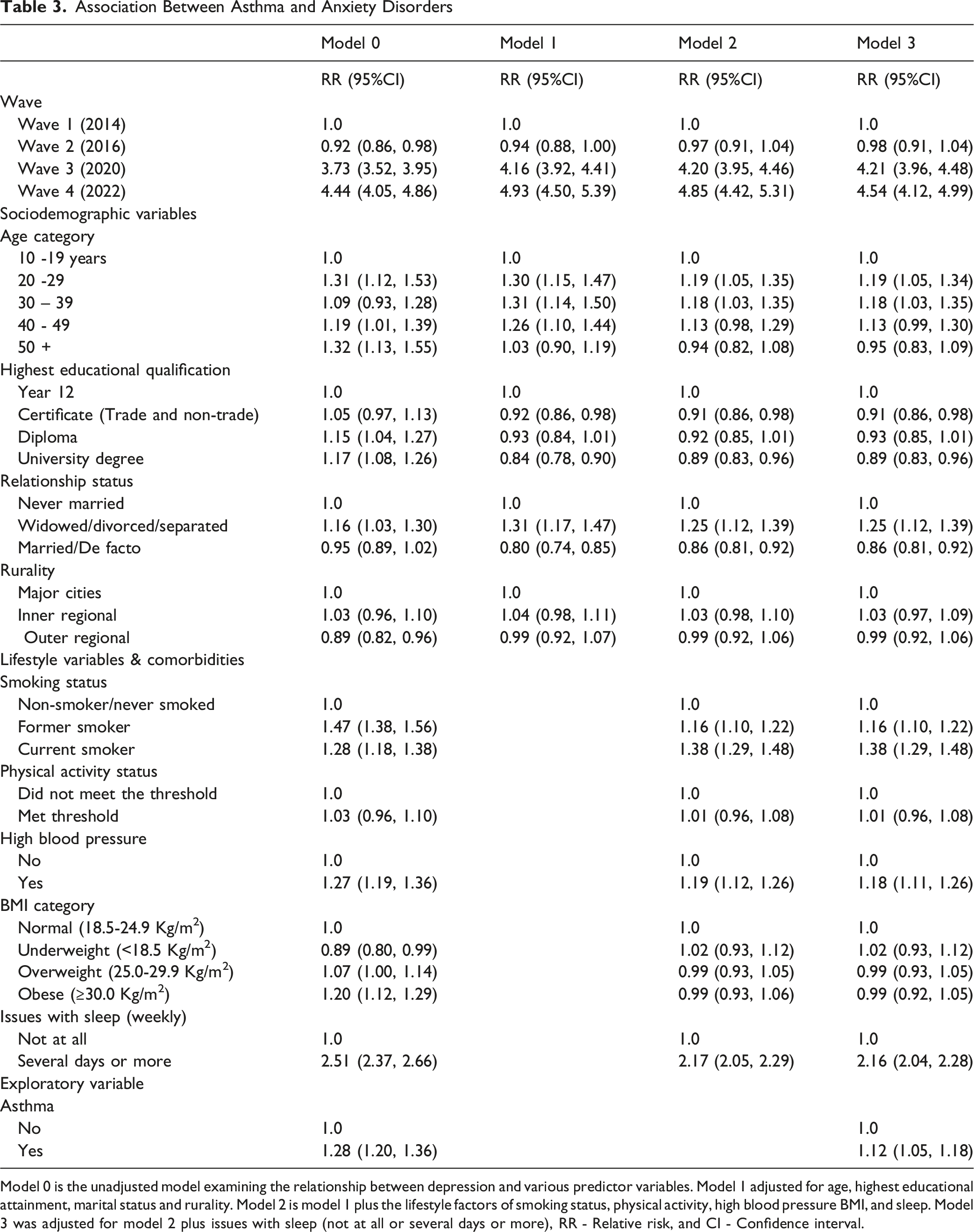
Model 0 is the unadjusted model examining the relationship between depression and various predictor variables. Model 1 adjusted for age, highest educational attainment, marital status and rurality. Model 2 is model 1 plus the lifestyle factors of smoking status, physical activity, high blood pressure BMI, and sleep. Model 3 was adjusted for model 2 plus issues with sleep (not at all or several days or more), RR - Relative risk, and CI - Confidence interval.
Association Between Asthma and Comorbid Depression With Anxiety
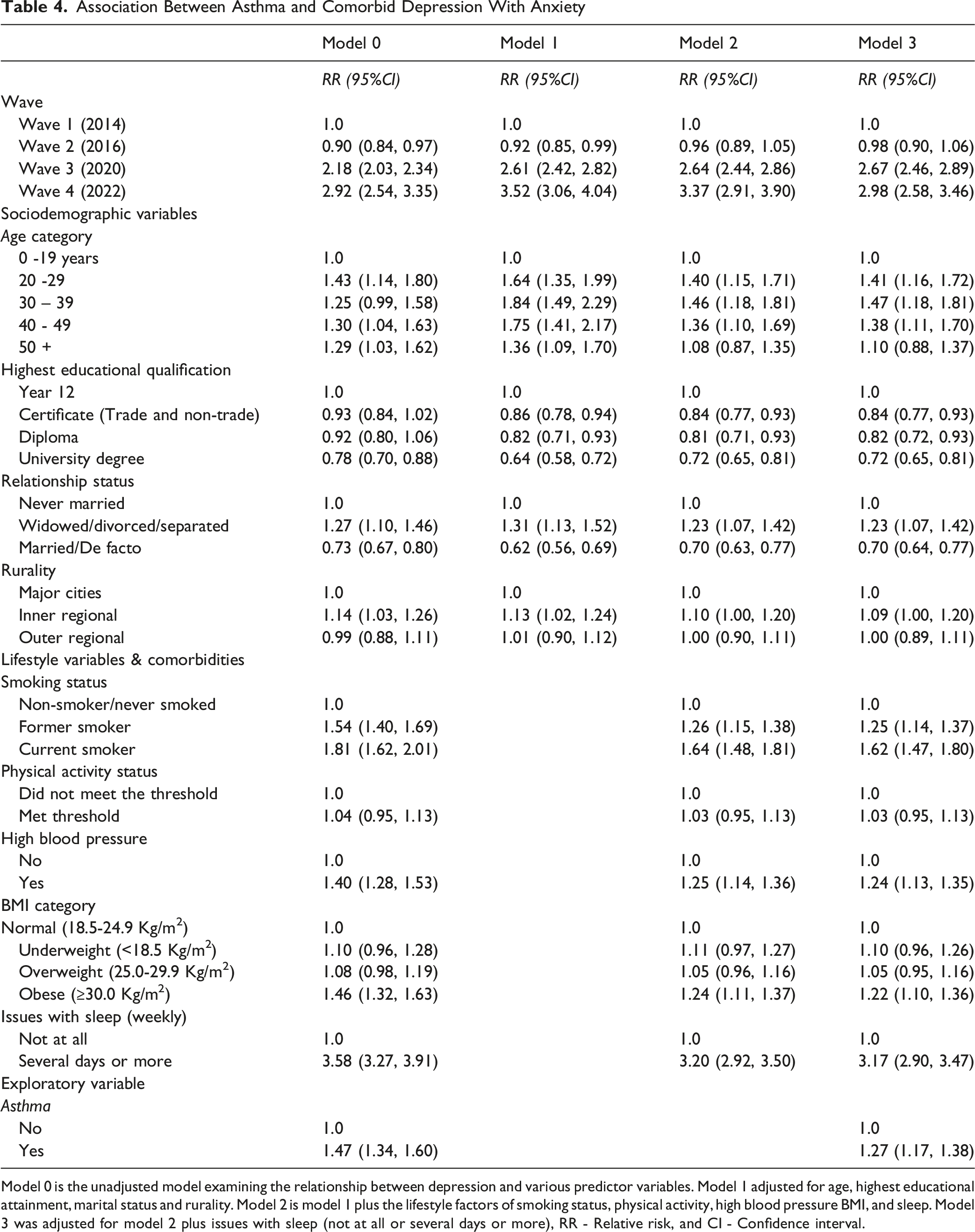
Model 0 is the unadjusted model examining the relationship between depression and various predictor variables. Model 1 adjusted for age, highest educational attainment, marital status and rurality. Model 2 is model 1 plus the lifestyle factors of smoking status, physical activity, high blood pressure BMI, and sleep. Model 3 was adjusted for model 2 plus issues with sleep (not at all or several days or more), RR - Relative risk, and CI - Confidence interval.
Anxiety disorders
Table 3 presents the association between mental health conditions and asthma among Australian men. The risk of developing anxiety disorder was higher (RR = 1.12, 95% CI: 1.05, 1.18) for men with asthma, compared to men without asthma.
Comorbid depression with anxiety
Table 4 presents the association between comorbid depression with anxiety and asthma among Australian men. Similarly, the risk of developing comorbid depression with anxiety was higher (RR = 1.27, 95% CI: 1.17, 1.38) for men living with asthma, compared to men without asthma.
Association between socio-demographic factors, comorbid conditions and mental health conditions in men with asthma
Details of the analysis of risk factors for mental health conditions in Australian men with asthma are displayed in Table S1. Among men with asthma, sleep problems were the strongest risk factor for poor mental health outcomes (Table S1), with risks substantially elevated across depression, anxiety, and comorbid conditions. Smoking was also associated with increased risk, particularly among current smokers. Younger men aged 20-39 years showed greater vulnerability to depression and comorbid depression with anxiety. Full details of these associations are provided in the supplementary material.
Discussion
The study found significant associations between asthma and depression, anxiety, and comorbid depression with anxiety, with comorbidity representing the highest relative burden among the mental health outcomes examined. Whilst the COVID-19 pandemic may have had a significant impact on the prevalence of mental health conditions in this population since 2020, other risk factors identified in this study were younger age, obesity, high blood pressure, sleep issues, and being a past or current smoker. Overall, the current study indicated that Australian men living with asthma are likely to report higher rates of depression, anxiety, and comorbid depression with anxiety, emphasising the importance of integrated healthcare strategies that include ongoing mental health assessments as well as links to mental health support services. Although the longitudinal nature of the data strengthens temporal interpretation, the observational design precludes causal inference, and findings should be interpreted as associations.
The observed surge in mental health conditions among Australian men with asthma in 2020 aligns with broader literature on the psychological impacts of the COVID-19 pandemic, particularly among individuals with pre-existing chronic conditions. 34 Several pandemic-related factors may have contributed to this increased prevalence of these mental health conditions, including prolonged lockdowns, heightened health-related anxiety, social isolation, and economic instability. 35 Furthermore, fear of increased susceptibility to severe COVID-19 outcomes may have intensified anxiety and depression in these individuals, while disruptions to routine healthcare access could have further exacerbated their psychological distress.34,36
The identified significant associations between asthma and mental health disorders in this study corroborate previous studies with developing co-occurring depression with anxiety shown to have the highest risk compared to depression or anxiety.37,38 This comorbidity may reflect shared and overlapping pathways between depression and anxiety. While the current study did not examine underlying biological mechanisms, several hypotheses proposed in the literature may help contextualise these findings. Chronic stress related to symptom burden, disease management, and uncertainty surrounding asthma control may contribute to psychological distress. 39 Additionally, it has been hypothesised that systemic inflammation associated with asthma, often described by the “overspill” theory, may influence neurobiological pathways involved in mood regulation through immune-to-brain signalling. 40 The overspill theory posits that chronic airway inflammation in asthma results in the release of pro-inflammatory cytokines into the bloodstream, which can lead to systemic inflammation. 41 Importantly, these proposed mechanisms remain speculative within the context of the present analysis, as inflammatory markers, hypoxaemia or physiological indicators were not measured. As such, these explanations should be viewed as theoretical frameworks rather than causal pathways supported by the current data.
This study identified younger age (20 - 39 years) as a risk factor for developing depression and comorbid depression with anxiety, with comparable findings reported for only depression in patients with asthma.42,43 This association may be partly explained by challenges related to health literacy, self-management demands and help-seeking behaviours among younger men. 44 These findings underscore the critical need for targeted mental health literacy programs and the integration of accessible, youth-friendly psychological support services within CRD care frameworks, particularly for young men living with asthma. 45 Conversely, being married or in a de facto relationship and having a university degree were identified as protective factors for depression and comorbid depression with anxiety. In people living alone, factors such as physical inactivity, social isolation and lack of emotional support have been identified as risk factors for depression, which are expected to be exacerbated in people with asthma due to persistent fatigue, leading to psychological distress.46,47 The observed association between higher educational attainment and a reduced risk of mental health conditions is consistent with findings from prior research.43,48 Higher education is thought to enhance mental health resilience by promoting greater health literacy, facilitating help-seeking behaviours, and supporting adherence to evidence-based treatment and self-management strategies. 49
Smoking has been widely reported as the leading risk factor for developing asthma, asthma exacerbations and asthma-related mortality.50,51 Whilst most previous studies identified only current smoking as a determinant of depression or anxiety, our study identified both past and current smoking as significant risk factors for depression, anxiety and comorbid depression with anxiety, with current smoking having higher risks for mental health disorders compared to past smoking.52–54 Furthermore, comorbid variables such as high blood pressure, obesity, and sleep disturbances are independently associated with asthma and depression.55,56 Hypertension and obesity are prevalent among individuals with asthma, and their presence may exacerbate physical functional limitations, promote social isolation, and increase psychological distress, thereby contributing to an increased risk of depression and anxiety. 42
Poor sleep quality among individuals with asthma has been linked to factors such as coexisting obstructive sleep apnoea, persistent coughing and nocturnal wheezing, which often intensify during asthma exacerbations. These disturbances can significantly impair sleep continuity and efficiency, contributing to chronic sleep deprivation.57,58 Longitudinal studies have predicted that these could result in emotional dysregulation, increased stress sensitivity, and disruption of neurobiological pathways involved in mood regulation, leading to depression and anxiety.5 59
Limitations and Strengths
A primary limitation of this study is the reliance on self-reported asthma and COPD diagnoses, which lacked objective confirmation through spirometry or medical record review. While this is a common methodology in large epidemiological studies, it may introduce misclassification bias and impact internal validity. Future research should incorporate validated clinical measures to enhance diagnostic accuracy. Nonetheless, it is important to acknowledge that the Ten to Men study is a well-established and nationally representative longitudinal cohort, widely regarded as a credible data source in Australian men’s health research. Another limitation is that the observational nature of the study hinders any definitive causal inferences. Whilst longitudinal data strengthens the inference of directionality, unmeasured confounding factors could still influence both asthma and mental health conditions. The information on the ethnicity of the participants was not reported, which may limit the generalisability of the findings to all Australian men, considering the multi-ethnic diversity of Australia. Despite these limitations, our study leverages a large population-based sample of Australian men, with an eight-year follow-up period. This longitudinal design allows for a more robust assessment of temporal associations between asthma and mental health conditions, including comorbid depression with anxiety, which were sparsely reported by prior studies. Another notable strength is the consideration of a comprehensive set of potential confounders in the analysis, including socio-demographic variables, physical health comorbidities, and lifestyle factors, which enhances the internal validity of the findings.
The large sample size and use of repeated observations across waves provided adequate statistical power to detect the observed associations. However, the low number of COPD cases limited the ability to examine this subgroup, and findings related to respiratory conditions are therefore primarily reflective of asthma.
Conclusion
This study identified an increasing prevalence of depression, anxiety and the comorbidity of both conditions among Australian men with asthma. These findings reaffirm the multifaceted impact of CRDs such as asthma, which is associated with substantial and potentially under-recognised mental health impacts. Policies should prioritise the identification and support of men at increased risk, especially those who are widowed, divorced, or separated; those experiencing sleep disturbances and individuals with a history of smoking. Future interventional research is necessary to evaluate the effectiveness of integrated care models that concurrently address chronic respiratory and psychological health. Tailoring such interventions to the high-risk subgroups identified in this study may enhance their clinical relevance and impact. Men living with CRDs, including asthma, experience higher rates of depression and anxiety, yet mental health screening and promotion are not consistently integrated into routine respiratory care, particularly in community and primary care settings. This study provides longitudinal evidence that asthma is associated with sustained and elevated risks of depression, anxiety, and their comorbidity among Australian men. It identifies sleep disturbances, smoking, obesity, high blood pressure, and relationship status as key modifiable risk factors contributing to poor mental health outcomes. Health promotion practitioners should embed routine mental health screening, sleep health promotion, and smoking cessation strategies into asthma management programs. Gender-responsive, integrated interventions delivered through primary care and pulmonary rehabilitation may improve both mental and respiratory health outcomes.So What?
What is already known on this topic?
What does this article add?
What are the implications for health promotion practice or research?
Supplemental Material
Supplemental Material - Asthma as a Predictor of Depression, Anxiety and Their Comorbidity in Australian Men
Supplemental Material for Asthma as a Predictor of Depression, Anxiety and Their Comorbidity in Australian Men by Nnamdi Mgbemena, Eme E. John, Anayochukwu E. Anyasodor, Kam C. Wong, Tracy MacFarlane, Kingsley Agho, Uchechukwu L. Osuagwu in American Journal of Health Promotion
Footnotes
Acknowledgements
The authors gratefully acknowledge the Australian Institute of Family Studies for managing the Ten to Men: The Australian Longitudinal Study on Male Health data collection and dissemination, and for providing access to the Ten to Men dataset. We thank all the boys and men who participated in the study and generously gave their time to contribute to this important national research resource. The findings and views reported in this paper are those of the authors only and should not be attributed to the Australian Government, the Australian Institute of Family Studies, or the Ten to Men study team.
Ethical Considerations
This study followed the principles of the Declaration of Helsinki for human subjects and received ethical approval from the University of Melbourne Human Research Ethics Committee (HREC 1237897 & 1237376).
Consent to Participate
Participants provided written informed consent prior to their participation. For this study, we obtained approval from the data custodian, Australian Institute of Family Studies, for the use of de-identified data.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.