
Abstract
Purpose
This study explored the types of health-related goals, the strategies employed, and challenges experienced by Latina caregivers of children with intellectual and developmental disabilities (IDD).
Design
This study focuses on exploratory data on goal setting obtained through qualitative observations and documentation of the intervention arm from a two-site RCT.
Setting & Sample
Twenty-six Latina caregivers were recruited and assigned to receive the intervention across 2 sites—Texas and Illinois.
Intervention
A 10-session culturally tailored health promotion intervention was delivered to participants by promotoras addressing caregivers’ wellness, physical activity, healthy eating, and navigating the environment and decision-making. Goal setting was incorporated throughout the intervention. Promotoras worked closely with participants to develop action plans and provided support as needed.
Measure
To analyze qualitative data, we used a deductive analytical approach based on transcript discussions and early data extraction. Qualitative data were categorized into types of goals, strategies used, subcategories, and barriers encountered.
Results
Twenty caregivers identified a total of 68 goals; 61.7% were achieved or in progress. Health promotion strategies included engaging in physical activity, changing nutrition/eating habits, participating in wellness activities, and using reminders. Caregivers experienced stress, feeling overwhelmed, and a lack of support.
Conclusion
This study has some limitations, which are fully discussed. Despite the challenges they experienced, caregivers achieved or reported progress towards most of their goals.
Introduction
Goal setting is a behavioral strategy that supports the identification and pursuit of specific behaviors an individual may wish to adopt or modify. As a behavior change technique, goal setting has been implemented across diverse populations and behavioral domains and is recognized as a key strategy in health-related interventions.1–5 Grounded in self-efficacy theory, 6 health education programs that incorporate goal setting can effectively enhance engagement in the targeted behaviors and ultimately improve health outcomes.7,8
Goal setting strategies have been used to promote health behaviors among marginalized populations, including people with disabilities. 9 For example, goal setting strategies have been implemented to optimize physical functioning among children with cerebral palsy 10 ; promote self-efficacy among children with special needs, and promote health behaviors among Latinx.9,11 In addition to individual-level interventions, some studies have focused on goal setting within the family context. Research indicates that health promotion interventions incorporating parent-focused goal setting can produce positive outcomes for both parents and children.12,13 However, relatively few studies have specifically examined goal setting as an intervention strategy for Latinx families. One pilot study used goal setting as part of a home-based intervention to improve parental practices related to diet and nutrition and identified multiple individual, interpersonal, and environmental barriers to goal achievement, including personal motivation, the child’s temperament and interests, schedule, and financial constraints. 14 Another pilot intervention with Latina caregivers of children with intellectual and developmental disabilities (IDD) found that caregivers expressed satisfaction with the use of goal setting and acknowledged various challenges while pursuing and achieving many of their goals (e.g., time constraint, work demand, and lack of motivation). 9
As demonstrated by previous research, merely setting a goal does not guarantee meaningful behavior changes.8,10 Some individuals and families may struggle to identify suitable and attainable goals, whereas others may struggle to translate goals into action.10,15 Despite substantive research on goal setting, several systematic reviews have emphasized the need to better understand the specific behavioral change processes that facilitate goal attainment as well as the barriers individuals and families encounter in pursuing their goals.3,15 Greater attention to these issues is especially important when working with underserved populations facing structural and contextual challenges.
One such population is Latinx families of children with disabilities, who often face greater levels of socioeconomic, cultural, and structural barriers due to intersectional difficulties related to their immigrant, racial/ethnic minoritized, and disability backgrounds.16–18 They are also at an increased risk for poor physical and mental health outcomes. 17 For the purposes of this paper, we use the term Latinx as a gender-neutral term to refer to the broader population, and Latina when referring specifically to the female primary caregiver. Latina caregivers of children with disabilities often report high levels of stress due to the complex demands of raising a child with developmental disabilities. Latinx families of children with disabilities have unique cultural beliefs and practices regarding behaviors related to health and caring for a child with disability. 18 For example, studies reported that Latina caregivers of children with disabilities face high levels of stigma and social isolation, which may negatively impact their help-seeking and other health-related behaviors.19,20 Latina caregivers tend to prioritize their child and family’s needs over their own. 19 Latina caregivers also reported unique patterns of parenting strategies related to diet and physical activity for their children with disabilities. 18 A deeper understanding of their experiences with goal setting (e.g., what works, what supports are needed, and what barriers they face) is necessary to design and refine health promotion interventions that integrate goal setting.
This study aims to explore the processes of goal setting in the context of a health promotion intervention as experienced by Latina caregivers, with a focus on the experiential and contextual aspects of goal setting. As such, this study aims to qualitatively assess the types of goals, strategies utilized, and barriers experienced among Latinx families of children with IDD. Specifically, we will answer the following research questions: (1) What types of health-related goals are identified by Latina caregivers of children with IDD? (2) What specific strategies do Latina caregivers use to achieve their goals? (3) What challenges do Latina caregivers face when making progress toward their goals?
No hypotheses were proposed for these research questions, given the study’s qualitative and exploratory nature.
Methods
Study Background and Intervention Description
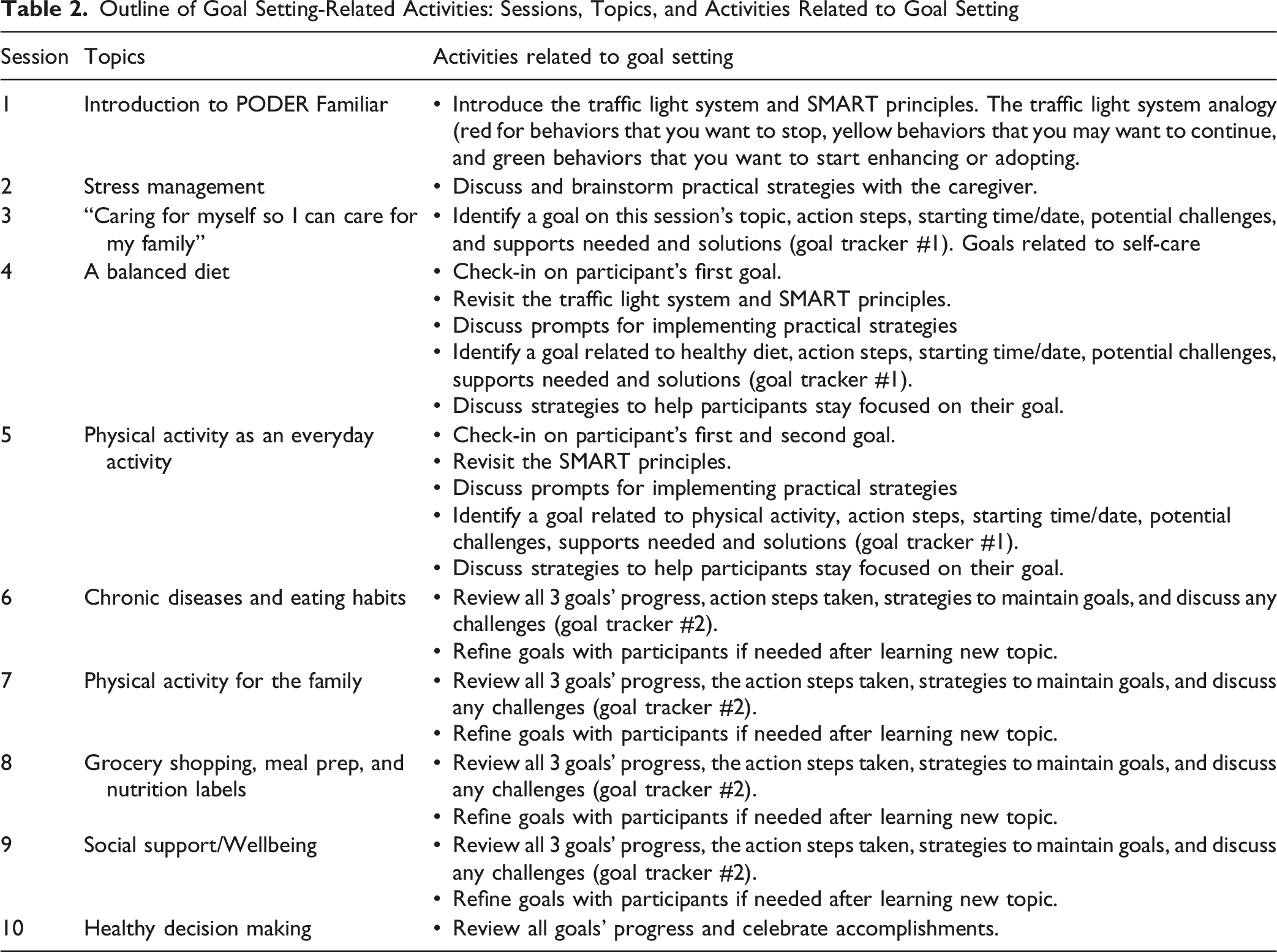
Based on prior research conducted by the investigators, we developed PODER Familiar, a culturally tailored health intervention aimed at enhancing the health and well-being of Latinx families of children with IDD. 21 The research team recruited and systematically trained the promotoras, who were themselves Latina caregivers of children with IDD, to deliver the intervention. PODER Familiar consisted of ten sessions covering 4 main topics: caregiver wellness (e.g., managing stress, caring for oneself, social support, seeking help), engagement in physical activity (e.g., the relationship between exercise/physical activity and health, strategies for enhancing physical activity), healthy eating habits and nutrition (e.g., role of healthy eating, why it is important, strategies for a balanced meal), as well as navigating the environment and decision-making (e.g., grocery shopping, home and community environment, establishing routines, strategies). Each session included learning objectives, content knowledge, stories about families of children with disabilities, strategies, and practical questions.
Promotoras were trained to deliver the intervention via videoconferencing software—Zoom —and to provide participants with ongoing support and troubleshooting. The intervention integrated 2 evidence-based programs, Caring for Myself and Familias Saludables, both of which had components to promote the health and well-being of Latinx families of children with disabilities.22–24: The combined new intervention was pilot-tested before the implementation of the design described below. 21 Throughout the intervention development and pilot testing, ongoing feedback from a community advisory board and the promotoras was incorporated to inform the final intervention and the randomized control trial (RCT) protocol. The intervention PODER Familiar’s primary outcomes focused on the health and well-being of the caregiver and the child with IDD. Yet goal setting, explored in this study, was incorporated throughout.
Study Design
The overarching aim of the goal setting data collection was to examine the types of goals and behavioral strategies that participants identified and implemented throughout the health promotion program, as well as the barriers they encountered in pursuing their goals. This study focuses exclusively on exploratory data related to goal setting obtained through qualitative observations and documentations of the intervention arm from a two-site RCT. While we also examined several primary health and well-being outcomes, which we reported in a separate manuscript about the RCT [manuscript under preparation]. Participants were randomly assigned to the intervention or control arm using a sequential method (e.g., if the first participant was randomly assigned to the intervention arm by coin toss, then the next would be assigned to the control arm). The RCT study was conducted in Texas and Illinois between 2024 and 2025. Twenty-six Latina caregivers (out of 55 in total) were assigned to the intervention arm to receive the intervention led by a trained promotora. Participants would start the intervention once they were assigned to the intervention arm. To measure fidelity, all individual sessions between Latina caregivers and the promotoras were recorded. The 10-session intervention was typically delivered once a week and completed within 10 weeks. However, occasionally, a session could be canceled due to unforeseen family circumstances or illness. When this occurred, the promotora would reschedule and follow up with the participant during the following week. Most participants completed the 10-session intervention within 3-4 months. Participants in the control arm did not receive the intervention and thus did not complete any intervention activities related to goal setting or goal setting data collection.
Participants
Participants were recruited through community partner agencies or via social media. Potential participants contacted the research staff if they were interested in the study. During the initial contact, research staff asked eligibility screening questions. Individuals who met the following eligibility criteria were then invited to participate in the study: self-identified as female adults (aged 18 or older), of Latin American heritage, and a primary caregiver of a child (aged 6-17 years) with autism, Down syndrome, and/or intellectual disability. Of the 26 eligible Latina caregivers assigned to the intervention arm, 6 did not report any qualitative data related to their goal setting activities, nor did they report on goal attainment. Three of the 6 participants withdrew from the study before completing the intervention due to insufficient time or changes in their work schedules. The other 3 participants left their goal setting sheets blank and expressed no interest in working on goals. Setting goals was not a requisite to continue in the study. We compared demographic characteristics and found no significant differences between participants who did and those who did not complete goal setting and related activities. As such, the final study sample consisted of N = 20 Latina caregivers who provided valid data on goal setting and activities related to goal attainment.
On average, Latina caregivers were 41.8 years old. Most caregivers had, some college or more education (60%), were employed/self-employed (60%), married/partnered (70%), born outside of the U.S. (60%), had a health insurance of any kind (69%), did not own a home (60%), and reported a household income of $35,000 or less (69%). Latina caregivers also reported that their children were all born in the U.S. and had a mean age of 10.5 years. Ninety percent (n = 18) reported that their child had autism as the primary diagnosis, whereas the remaining 10% (n = 2) had Down syndrome or another developmental disability. Although the majority of the caregivers had a child with autism, we will continue to refer to the population of interest as children with IDD, as this is how we advertised and recruited for the study. No separate demographic analysis was done to explore if there were any differences between the 18 caregivers of children with ASD and the 2 who had other disabilities.
Demographic Characteristics of Participants
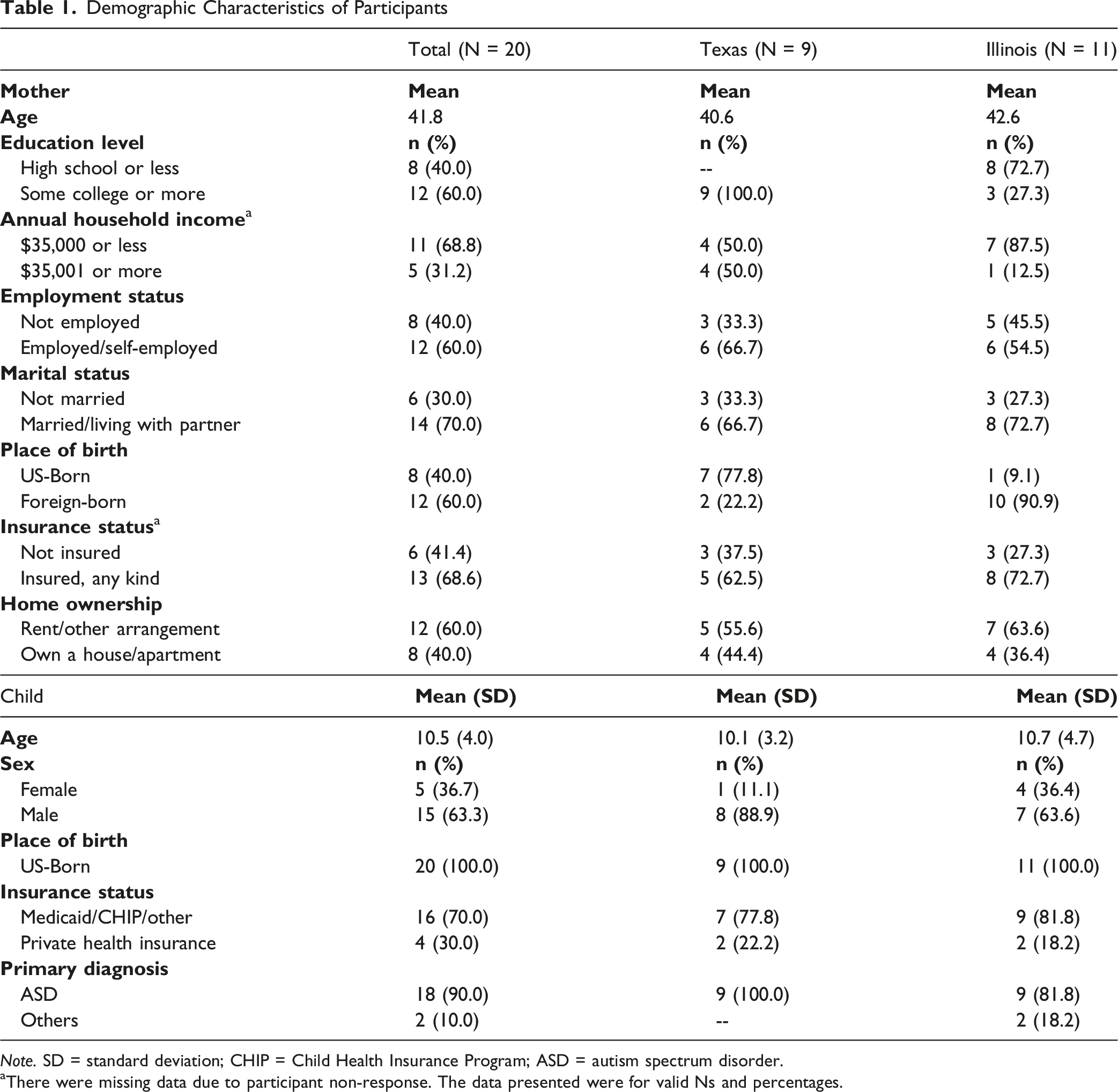
Note. SD = standard deviation; CHIP = Child Health Insurance Program; ASD = autism spectrum disorder.
aThere were missing data due to participant non-response. The data presented were for valid Ns and percentages.
Goal Setting Procedure and Data Collection
Outline of Goal Setting-Related Activities: Sessions, Topics, and Activities Related to Goal Setting
Data Extraction and Content Analysis
All individual sessions were recorded and transcribed verbatim in the language in which they were conducted (English or Spanish) using Sonix, an online transcription software. To prepare for data analysis, the first and second authors, both of whom hold PhD degrees with substantial qualitative research experience, developed a codebook based on the 2 goal trackers in the curriculum (See Supplemental Material). The goal trackers included items such as the types of health-related goals identified by caregivers, the strategies used to make progress on these goals, and the challenges/barriers experienced by caregivers. We trained 3 bilingual research staff members (one doctoral-level and 2 master’s-level students) to become familiar with the PODER Familiar curriculum manual, goal setting protocol, and the charting and tracking procedures for data extraction. They extracted all data relevant to goal setting from the transcripts and reviewed the corresponding video recordings when additional contextual detail was needed.
Once data extraction was completed, the research staff analyzed the original language (English or Spanish) transcripts using agreed-upon categories from the codebook, including study site, goal mentioned in session, target of the goal (caregiver/child/family), type of goal (physical health; nutrition/eating habits/diet; mental health/well-being; or other), goal description, strategies to engage or maintain goals, goal progress or achievement, whether challenges were identified (yes/no/not applicable), and type of challenges. Exemplary quotes with corresponding transcript timestamps were noted. Based on the prior established codebook, a deductive content analysis was conducted. 25 Qualitative data were categorized into categories and subcategories based on the types of goals, strategies used to achieve them, and challenges encountered. This preliminary analysis yielded main categories and subcategories related to actions taken and challenges experienced. Based on this initial analysis, the codebook was refined to include definitions of main categories and subcategories. Three bilingual researchers individually coded the data according to the codebook. Discrepancies were discussed and resolved collaboratively, and codebook adjustments were made as necessary. To assess intercoder reliability in classifying strategies, goal types, and challenges experienced, 25% (n = 5) of the 20 cases were randomly selected, yielding 80% intercoder agreement. Coding discrepancies were resolved through discussion with one of the project’s bilingual co-principal investigators. All analyses were conducted using Microsoft Word and Excel.
The research team had no prior relationship with study participants, and the participants did not know about the researchers prior to the study. All research staff involved in the data analysis received extensive training and supervision, both of which helped minimize bias. Methodological integrity was ensured by applying the fidelity principle outlined by Levitt and colleagues 26 and by including relevant elements as stated in the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist (See Supplemental Material). 27
All goal setting and goal-status data were self-reported. A goal was rated as met if the caregiver reported completing it, particularly for goals with clearly defined start and end points (e.g., scheduling a medical physical exam and attending the appointment or registering and participating in a self-care training session). Goals were rated as in progress if the caregiver reported consistent engagement in the selected strategies during at least 2 of 4 intervention sessions. For example, a caregiver who set a goal of taking 15 minutes each morning for herself to practice a deep-breathing relaxation routine and reported engaging in this routine at least 2 of the last 4 weeks was considered to have the goal in progress. A goal was classified as dropped if the caregiver reported that she was no longer working towards it or had decided it was no longer a priority. A goal was classified as postponed or showing inconsistent progress if the caregiver expressed interest in continuing but reported barriers such as limited time, illness, or other competing demands. Inconsistent progress meant engagement in the selected behavioral strategy for fewer than 2 weeks within a 4-week period. All data was self-reported. Throughout the intervention, when participants shared that a goal had been met or was in progress, the promotora congratulated them and inquired about ways to sustain the goal. When participants shared challenges that hindered their progress, the promotora engaged in problem-solving, offered support, modeled behaviors, pointed to resources and/or strategies in the toolkit, or encouraged them to seek support from family members and/or professionals.
Results
Results are presented according to the research questions, with findings reported as percentages alongside qualitative categories. Participant quotes are presented in the tables.
Types of Health-Related Goals Identified by Latina Caregivers of Children With IDD
Twenty caregivers set a total of 68 goals, averaging 3.4 goals per participant (range: 2-5). Of these, 67.6% (n = 46) were self-oriented, focusing on Latina caregivers’ own wellness, nutrition, and physical activity. The remaining goals were either child-focused (16.1%; n = 11) or family-oriented (16.1%; n = 11).
Of the self-oriented goals (n = 46), 45.6% focused on overall mental wellness, 32.6% on physical activity, and 15% on improving nutrition habits and meal routines. About 7 percent included other types of goals, such as enrolling in a class. Most child-oriented goals focus on improving the child’s nutrition and meal routines. Similarly, family-oriented goals focused mostly on increasing engagement in physical activity and improving nutrition habits and routines. Only one wellness goal was identified for the family.
Overall, 61.7% of the goals were met or in progress. Examples of goals that were met included obtaining a medical physical health exam (for a caregiver who had not had one in several years) and completing a specific training course. Goals that were in progress included behaviors such as walking the dog for 30 minutes each day of the week, exercising at the gym twice per week for at least 45 minutes, and avoiding purchasing soda during the family’s weekly grocery shopping. Of the 68 goals, 5.8% were dropped, and 30.8% were either postponed or demonstrated inconsistent progress. Most of these goals pertained to the caregiver’s mental wellness, including strategies for managing stress. The most common reasons for postponing or demonstrating inconsistent progress included lack of time and competing caregiving demands.
Specific Strategies Caregivers Used to Achieve Their Goals
Main Strategies, Subcategories, and Illustrative Quotes (N = 20)
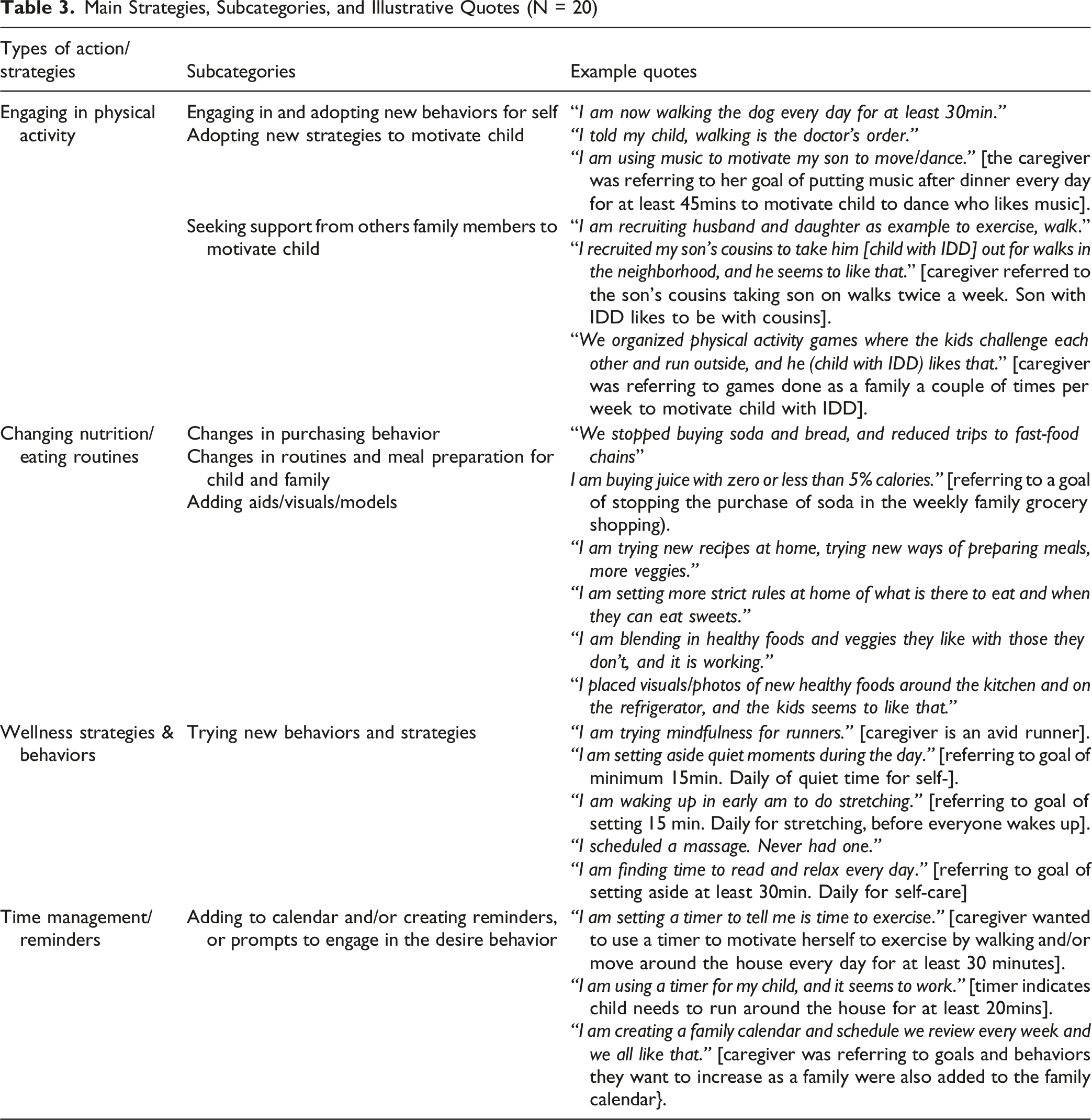
Strategy 1: Engaging in Physical Activity-Related Behaviors
Two subcategories were identified: engaging in and adopting new behaviors, and seeking support to help children with disabilities participate in physical activity.
Engaging in and adopting new behaviors. Examples included going to the park with friends once a week to walk for 45 minutes, walking the dog every day, going to the gym twice a week, and dancing and playing at home with music every night, among other activities. One caregiver, an avid runner, began training for a marathon as part of her effort to increase physical activity.
Seeking support from others. This subcategory targeted the child and family goals, including seeking support from others to encourage physical activity in the child with IDD and family members. Support came from the child’s father, cousins, and siblings, who helped model and promote activities such as walking, playing, and dancing. None of the caregivers’ self-targeted goals included seeking support from others as a strategy for pursuing them.
Strategy 2: Changing Nutrition Routines and Eating Habits
Three subcategories were identified: changes in purchasing behaviors, changes in meal preparation and routines, and the use of visuals and other aids to support goals.
Changes in purchasing behavior. Caregivers adjusted their shopping habits to support healthier eating, including reducing or eliminating purchases of high-sodium items at the grocery store and reducing visits to fast-food restaurants. They also chose to buy healthier options, such as juices with no added sugar or less than 5% sugar, and purchase a variety of seasonal vegetables.
Changes in meal preparation and routines. Caregivers employed targeted strategies to enhance meal quality and variety, such as trying new recipes (some provided by the promotora or from the intervention manual or toolkit provided to participants). Other strategies included blending vegetables that the child with IDD and family liked with those they did not (eg, in smoothies).
Adding visuals, modeling, and other aids. This subcategory focused on strategies aimed at the child with IDD and the family. Caregivers placed visual aids—such as charts or reminders—in common areas or on the refrigerator, to promote healthy habits. They also modeled desirable behaviors by positioning themselves or their spouses as role models for their children.
Strategy 3: Wellness Strategies and Behaviors
This strategy focused on wellness behaviors targeting the caregiver, a topic discussed in 4 of the ten sessions of the intervention. This included emphasizing the importance of managing their own stress, anxiety, and overall well-being. The primary subcategory was trying new behaviors and strategies. These included engaging in mindfulness exercises to promote relaxation, learning relaxation techniques, setting aside 10-15 minutes in the early morning for deep breathing, performing daily light stretching for 15 minutes, carving out 30 minutes of daily reading time, and scheduling and attending medical appointments for their own health needs. No wellness or well-being goals were reported for the child.
Strategy 4: Time Management and Reminders to Engage in Desired Behaviors
One strategy that emerged across different types of goals was the use of time management to support engagement in desired goals. Participants shared adding goal-related strategies and activities to a calendar and/or creating reminders or prompts around the house. This strategy was applied to goals set for the caregiver, child, and family, and included creating a shared family calendar, adding goals and action steps to a personal calendar indicating type of activity, time, duration, and frequency; developing a family schedule incorporating both healthy meals and physical activity goals, and setting timers as reminders.
Challenges in Making Progress Towards Goals
Types of Challenges Experienced by Participants and Illustrative Quotes (N = 20)
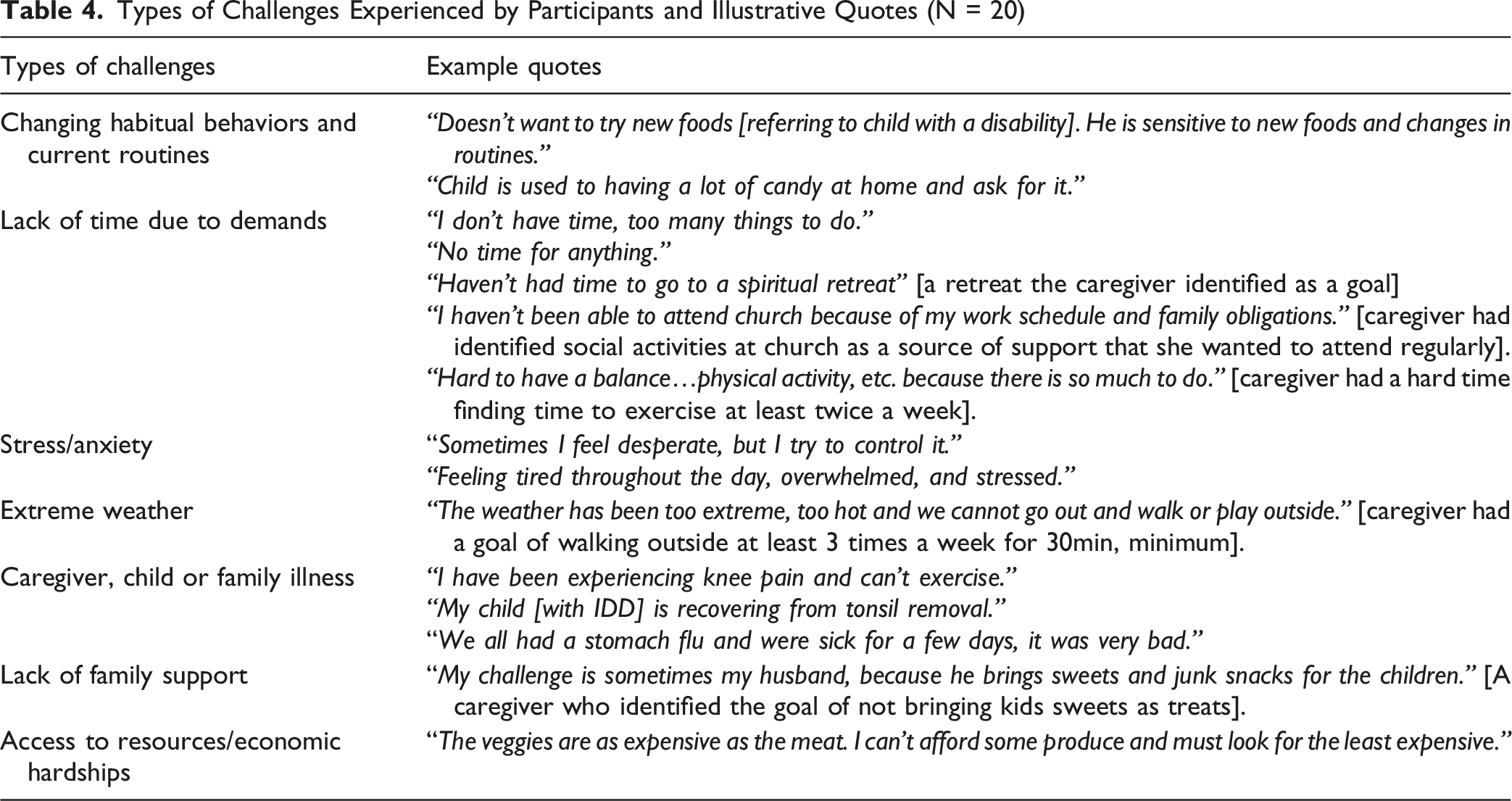
Challenge 1: Changing Habitual Behaviors and Routines
Fourteen Latina caregivers reported challenges in changing behaviors and routines, including adapting to new meal preparation, trying new foods, or engaging in new activities. Participants emphasized that changes were difficult for their children, noting that alterations to meals, routines, or schedules were often refused/resisted. Nine participants mentioned the child’s disability as one of the reasons why changing routines/habits was difficult. Two participants specifically mentioned the child’s sensory issues as a challenge in trying new foods or engaging in new routines.
Challenge 2: Lack of Time due to Current Demands
The lack of time was a common concern. Nine participants described being stretched thin by current demands, including caring for a child with special needs, household chores, attending regular appointments, and meeting the needs of their other children. Due to a lack of time, they did not prioritize their own health or their well-being.
Challenge 3: Stress and Anxiety
Nine participants mentioned feeling overwhelmed, stressed, and anxious as the biggest challenges they experienced. This was attributed to overwhelming demands and a lack of support. Two participants reported experiencing panic attacks due to high stress levels, and one required hospitalization.
Challenge 4: Extreme Weather
This category primarily emerged in relation to physical activity and wellness-related goals. Nine participants mentioned experiencing extreme heat or cold as a barrier. Given that the study spanned 8 months, participants in Texas experienced extreme summer heat. In contrast, those in Illinois experienced severe winter cold, which limited their ability to engage in physical activity.
Challenge 5: Caregiver or Child Illness
Nine participants experienced illness, were recovering from surgery, or had a child or other family member sick, which limited their ability to work on their goals. Examples included the whole family having stomach flu, a caregiver experiencing knee pain, recovering from surgery, and a child undergoing a tonsillectomy.
Challenge 6: Lack of Family Support
Nine participants mentioned a lack of support from a family member as a barrier to making progress towards their goals. Four mentioned a lack of support from their spouse; examples included the child’s father bringing home sweets or other unhealthy snacks after the caregiver had communicated the goal of reducing sweets as special treats to the child.
Challenge 7: Limited Access to Resources
Two participants reported difficulty purchasing healthy food for their families due to financial hardships, noting that they often had to choose the least expensive foods and couldn’t afford fresh produce. One other participant mentioned not having the resources or support to cover childcare, which would enable her to care for herself and work on her wellness goals.
Throughout the intervention, when participants shared that a goal had been met or was in progress, the promotora congratulated them and inquired about ways to sustain the goal. When participants shared challenges that hindered their progress, the promotora engaged in problem-solving, offered support, modeled behaviors, pointed to resources and/or strategies in the toolkit, or encouraged them to seek support from family members and/or professionals.
Discussion
This is one of the few studies exploring health-related goal setting by Latina caregivers of children with IDD, as well as strategies and barriers related to achieving their goals. Twenty Latina caregivers of children with IDD completed the goal setting activities with promotora support while enrolled in the PODER Familiar intervention. Most of the 68 goals identified by participants were met or in progress. Notably, most goals were self-oriented, while smaller subsets focused on the child or were family-oriented.
Latina caregivers of individuals with disabilities tend to prioritize family responsibilities over their own needs, partly due to the influence of Latinx cultural concepts such as marianismo and familismo (e.g., loyalty to family). 28 This shift, in which participants selected more self-care goals than family or child goals, may have resulted from the intervention’s emphasis on participants caring for themselves to care for their families. Our findings show that family demands can be an essential impediment to self-care for Latina caregivers of children with IDD. Therefore, health interventions for this population must not only encourage caregivers to prioritize self-oriented goals but also provide specific strategies to achieve them. In a previous study involving Latina mothers, participants called for structured support in creating and pursuing realistic health-related goals that take into account their individual needs and preferences, as well as their family and cultural context. 29 To this end, PODER Familiar employed a structured, family-centered approach where the curriculum and the trained promotoras explicitly encouraged caregivers to prioritize self-care. PODER Familiar also included a toolkit of tangible strategies that caregivers could use to pursue their self-care goals. One session of the intervention was dedicated to helping the caregiver identify sources of social support and strategize how to tap into them to facilitate their goals as an essential coping strategy.
Support from the promotoras could have been an important factor in achieving goals in this sample. Previous research supports the effectiveness of promotores in assisting Latinx adults to improve their health behaviors by developing SMART goals. 30 However, in this study, not all caregiver goals followed the SMART guiding principles, suggesting that promotoras may need more training in this area. Despite this, the role of promotoras in supporting caregiver goals was critical. Latina caregivers tend to derive informational and emotional support from other women in their social network. Promotoras provided informational and emotional support and served as facilitators throughout the PODER Familiar intervention. Their shared cultural backgrounds, caregiving experiences, and peer leadership likely enhance participation and fidelity, as Latina caregivers may have perceived the promotora as a role model and someone they can connect with. Studies have consistently shown that the promotora model is a culturally grounded mechanism for bridging social, linguistic, and structural gaps in health interventions.30,31 Promotoras can facilitate behavioral change through personalized goal setting, collaborative problem-solving, and consistent monitoring, even when participants face individual, family, and structural barriers. 30
Furthermore, participants reported both internal and external barriers related to tangible (financial resources), intangible (eg, time), and psychosocial (eg, stress and social support) resources. Similar barriers, such as time constraints, stress, and competing obligations, were reported in a nutrition-focused intervention with Latina caregivers of children without disabilities. 14 Many caregivers in our study described limited time and high caregiving demands as their primary challenges, reflecting the realities of caring for a child with disabilities and the structural and role-related barriers limiting caregivers’ ability to pursue personal wellness and well-being. They also identified barriers that are unique to families of children with IDD, such as the child’s food sensitivities and reactivity to any changes in routines. These barriers often co-occurred with limited resources and low family/social support. These individual, family, and contextual factors reflect broader social determinants of health that disproportionally impact families of children with disabilities, especially those of immigrant backgrounds.19,30 Health interventions aiming at individual-level behavior change alone may have limited impact unless accompanied by policy/systemic changes addressing accessibility to resources and other structural barriers. According to one systematic review of behavior change strategies among Latina women, successful techniques targeted goal setting and problem-solving at the individual level, partner support and child-related obligations at the interpersonal level, and access to safe, weather-independent physical activity resources at the environmental level. 32
The negative impact of these challenges/barriers was partially reflected by the fact that most goals postponed or dropped by Latina caregivers while participating in the PODER Familiar intervention were wellness goals for themselves. Even though 4 of the ten curriculum sessions emphasized the importance of caring for themselves to care for their child and family, this may reflect cultural expectations of self-sacrifice associated with being a Latina caregiver. 31 Given the lack of support and time/resource constraints, Latina caregivers might have to postpone or drop these wellness goals, and instead, prioritize the more urgent, day-to-day care needs of their child and other family members. 19 Most Latina caregivers completed the PODER Familiar intervention in 3-4 months. As such, it was also possible that Latina caregivers did not have enough time to implement their goals while being enrolled in the intervention.
Despite these challenges/barriers, most participants demonstrated progress and/or achieved at least one of their personal wellness goals. The PODER Familiar intervention’s goal setting components, strategies, and interactive curriculum provided a structured and motivational way for Latina caregivers to engage in behaviors and routines that promote their health and well-being. Monitoring and recognizing small successes with a promotora throughout the PODER Familiar intervention may also have reinforced positive feedback loops, which in turn incentivized goal attainment. Aligned with current literature on behavioral change and maintenance, setting goals related to daily routines/habits and the home environment reduces difficulty/complexity and increases commitment and determination.3,5
Limitations
Several study limitations should be acknowledged. First, qualitative data collected and analyzed were from Latina caregivers enrolled in the PODER Familiar RCT intervention arm only. This may limit the generalizability of our findings, as they lack a comparison with participants from a control arm. Second, we did not document participants’ prior exposure to therapy and rehabilitation services, which might have exposed caregivers to goal setting strategies before they participated in this study. Third, goal setting and attainment data were extracted from self-reported progress conveyed to promotoras throughout the intervention. Although we systematically reviewed the transcripts and recordings to enhance accuracy, social desirability may have influenced caregivers’ reports of goal setting and attainment. For example, caregivers may be subject to social desirability bias and inadvertently report positive changes when asked by the promotoras. The lack of follow-up assessments is another limitation. We don’t know whether the reported goal attainment and progress were sustained over time, and whether participants continue working on their goals without prompting from the promotora. Future research should include independent follow-up or behavioral observations to triangulate findings.
Implications for Future Research and Practice
Given the exploratory nature of this study, future research in this area is essential. Future research may include a control arm that identifies goals but receives no intervention curriculum or prompts from promotoras. Furthermore, future research may include at least a 6-month follow-up assessment to evaluate the long-term impact of goal setting strategies and extend the intervention beyond 3-4 months, as this may not be sufficient to sustain behavior change. Future research should incorporate some of the challenges identified in this study as points for discussion throughout the curriculum. Engaging in problem-solving with the promotora about anticipated challenges may better prepare the caregiver to address them as they arise. Finally, future research should focus on exploring goal setting strategies for specific populations. For instance, the majority of caregivers in this study had a child diagnosed with autism spectrum disorders (ASD). Although this study’s recruitment process included children with IDD, we don’t know if the challenges caregivers experience pursuing their goal might differ according to the child’s diagnosis.
In terms of implications for practice, a substantial body of literature indicates that Latina caregivers of children with disabilities experience various stressors associated with raising a child with special needs.19,23 Community and school programs should take into account the challenges identified by caregivers in this study to address the needs of this growing population. Specifically, community-based programs could prioritize offering respite care, allowing caregivers time to focus on their self-care, while also providing additional supports to help address their broader needs. Future practice efforts might also consider expanding the role of promotoras, who serve as trusted community liaisons and a support system for families.
Conclusions
Despite the limitations, this study explores the type of goals, strategies, and barriers expressed by caregivers of children with disabilities. The findings provide valuable insights into the challenges Latina caregivers face when intentionally working to enhance their health and well-being, and that of their children with IDD and their families. Future efforts should further incorporate goal setting and behavioral change strategies into interventions designed to support Latinx families of children with disabilities.
Takeaways
• Latina caregivers of children with disabilities identified several goals to enhance their health and well-being and were successful in achieving or making progress toward the majority of them. • Latina caregivers used several strategies to help them achieve goals, including seeking support, changing nutrition routines and eating habits, changing meal preparation routines, and using prompts and reminders. • Participants experienced several barriers to achieving their goals that could inform the design of future interventions designed to support caregivers of children with disabilities. • There is a need to develop practical interventions to support the health and well-being of caregivers of children with intellectual and developmental disabilities.
Supplemental Material
Supplemental Material - Promoting Health Behaviors Among Latina Caregivers of Children With Intellectual and Developmental Disabilities Through Goal Setting
Supplemental Material for Promoting Health Behaviors Among Latina Caregivers of Children With Intellectual and Developmental Disabilities Through Goal Setting by Yolanda Suarez-Balcazar, Amy Pei-Lung Yu, Weiwen Zeng, Mansha Mirza, Claudia Castillo Ayala, Christopher L. Shepperd, Tana Holt, Deborah Parra-Medina, Pei-Chiang Lee, and Sandy Magaña in American Journal of Health Promotion
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The contents of this research project were developed under a grant from the United States Department of Health and Human Services, Administration for Community Living (ACL), National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR) Grant #90DPHF0005-01-00 (P.I. Sandy Magaña). However, those contexts do not necessarily represent the policy of the Department of Health and Human Services (DHHS), and you should not assume endorsement by the federal government.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.