
Abstract
Purpose
To examine the use of pharmacotherapy and behavioral cessation methods among U.S. adolescents who vape nicotine.
Design
Cross-sectional Analysis of Wave 7 data From the Population Assessment of Tobacco and Health Study.
Setting
United States.
Sample
Adolescents aged 12-17 years (N = 1181) who reported past-year nicotine vaping.
Measures
Self-reported use of cessation methods (apps, nicotine replacement therapy [NRT], cessation medications) and past-year quit attempts.
Analysis
Descriptive statistics and weighted logistic regression models using STATA 18.0, with significance set at alpha <0.05.
Results
Overall, 10.6% of adolescents reported using any cessation therapy, with NRTs being the most commonly used cessation method (4.4%), while medications (i.e., Varenicline or Bupropion) were the least commonly used method (3.3%). Adolescents with higher nicotine dependence (wanting to vape within 30 minutes of waking) (aOR: 2.83; 95% CI: 1.49, 5.36) and those planning to quit within 12 months (aOR: 1.88; 95% CI: 1.10, 3.20) had higher odds of using any cessation therapy. Among racial ethnic groups, Hispanic adolescents (vs. non-Hispanic White; aOR: 0.46, 95% CI: 0.25, 0.86) had lower odds of reporting any cessation therapy.
Conclusion
Among U.S. youth who vape e-cigarettes, about 1 in 10 self-reported using any cessation aid. This low utilization rate suggests a need for tailored and equitable cessation interventions.
Keywords
Purpose
E-cigarettes are the most widely used tobacco product among U.S. adolescents. In 2024, over 1.5 million adolescents reported nicotine vaping, with lifetime prevalence ranging from 9.6% in 8th grade to 21% in 12th grade. 1 Initiating nicotine use during adolescence is especially concerning given the unique vulnerability of the developing adolescent brain, neural networks, and the increased risk of long-term nicotine dependence. 2
While two recent clinical trials have demonstrated that pharmacotherapy 3 and behavioral therapy 4 are efficacious for nicotine vaping cessation in adolescents in clinical trial settings, the real-world applicability of these approaches remains unclear. National survey data also show that most adolescents try to quit unassisted, 5 showing a disconnect between evidence-based interventions and actual cessation behaviors. Importantly, data is sparse on which cessation methods, including pharmacotherapy, are being used by adolescents who vape nicotine. Because no pharmacotherapy is currently FDA-approved for adolescent vaping cessation, meaning any such use is off-label, it is crucial to understand which methods adolescents use in practice. The current study addresses this gap by examining the use of pharmacotherapy and behavioral cessation methods among U.S. adolescents. Identifying which cessation methods adolescents use in practice can inform efforts to tailor and scale cessation resources to support adolescents who vape nicotine.
Methods
Design
We conducted a cross-sectional analysis of the Population Assessment of Tobacco and Health (PATH) Study Wave 7 (2022-2023; N = 10,834), a longitudinal survey conducted across U.S. States and the District of Columbia. The Westat Institutional Review Board approved the Study, and parental consent with youth assent was obtained before study procedures. 6
Sample
The study population was restricted to adolescents (12-17 years) with complete responses on study variables (n = 1181) who had vaped nicotine in the past year.
Measures
We assessed past-year cessation methods: i. past-year use of an app on a tablet/computer/smartphone to help quit nicotine vaping (also called ‘app-based’ methods), ii. Past year use of Nicotine Replacement Therapy (NRTs) to quit vaping, iii. Past year use of cessation medications (i.e., Varenicline or Bupropion) to quit vaping; and iv. any past year use of vaping cessation therapy (NRTs or medications or app-based behavioral therapy). The methods were grouped as cessation aids (i.e., NRTs or medications or app-based behavioral therapy) consistent with cessation treatment frameworks. Additionally, the past-year use of NRTs and cessation medications was assessed regardless of whether participants indicated a past year quit attempt (“tried to completely stop using electronic nicotine products”), recognizing that some adolescents might have used these methods to reduce rather than fully quit nicotine vaping. The app-based method, by contrast, was assessed only among adolescents who reported a quit attempt. As a secondary measure, we examined cessation methods among individuals who reported a nicotine vaping quit attempt (yes/no) in the past year. The definition of measures and wording of survey questions are provided in Appendix Table 1. Cessation methods were drawn from different assessments in the PATH Youth instrument: the NRT and cessation-medication items were administered to all past-year tobacco users, whereas the app-based behavioral item was administered only to established (past-30-day, non-light) past-year electronic nicotine product users who reported a past-12-month attempt to completely stop e-cigarette use. The composite “any cessation therapy” outcome therefore combines items with differing denominators and groups pharmacological (NRT, cessation medications) and behavioral (app-based) aids that are heterogeneous in mechanism and evidence base. We therefore report each method separately (app-based methods, NRTs and/or cessation methods), and in a sensitivity analysis, the composite excluding the app-based item.
Analysis
Descriptive associations between adolescent characteristics and cessation methods were tested using Rao-Scott chi-square tests. Additional analysis was conducted examining cessation methods used among adolescents who made quit attempts in the past year. Multivariable logistic regression models controlled for age, sex, race/ethnicity, annual household income, current cigarette smoking, current vaping, vaping frequency, time to wanting nicotine vaping after waking, and readiness to quit vaping. Time to first vape after waking was included as a proxy for nicotine dependence, consistent with validated youth e-cigarette dependence measures.7–10 Analysis incorporated the PATH weighting procedures to account for the complex survey design and was conducted between April-November 2025 using Stata (18.0), with the significance level set at α = 0.05. Given the low prevalence of each individual method, we used the composite as the primary outcome. In disaggregated analyses, we modeled pharmacotherapy-based methods (NRT or cessation medications), adjusting for all main-model covariates, and modeled the app-based method separately, adjusting only for time to first vape and readiness to quit because of sparse cells (Appendix Tables). Missing responses were <10% and reported by variable in the Appendix.
Results
Cessation Methods Among Adolescents who Vaped Nicotine in the Past Year in the 2022/2023 PATH Study
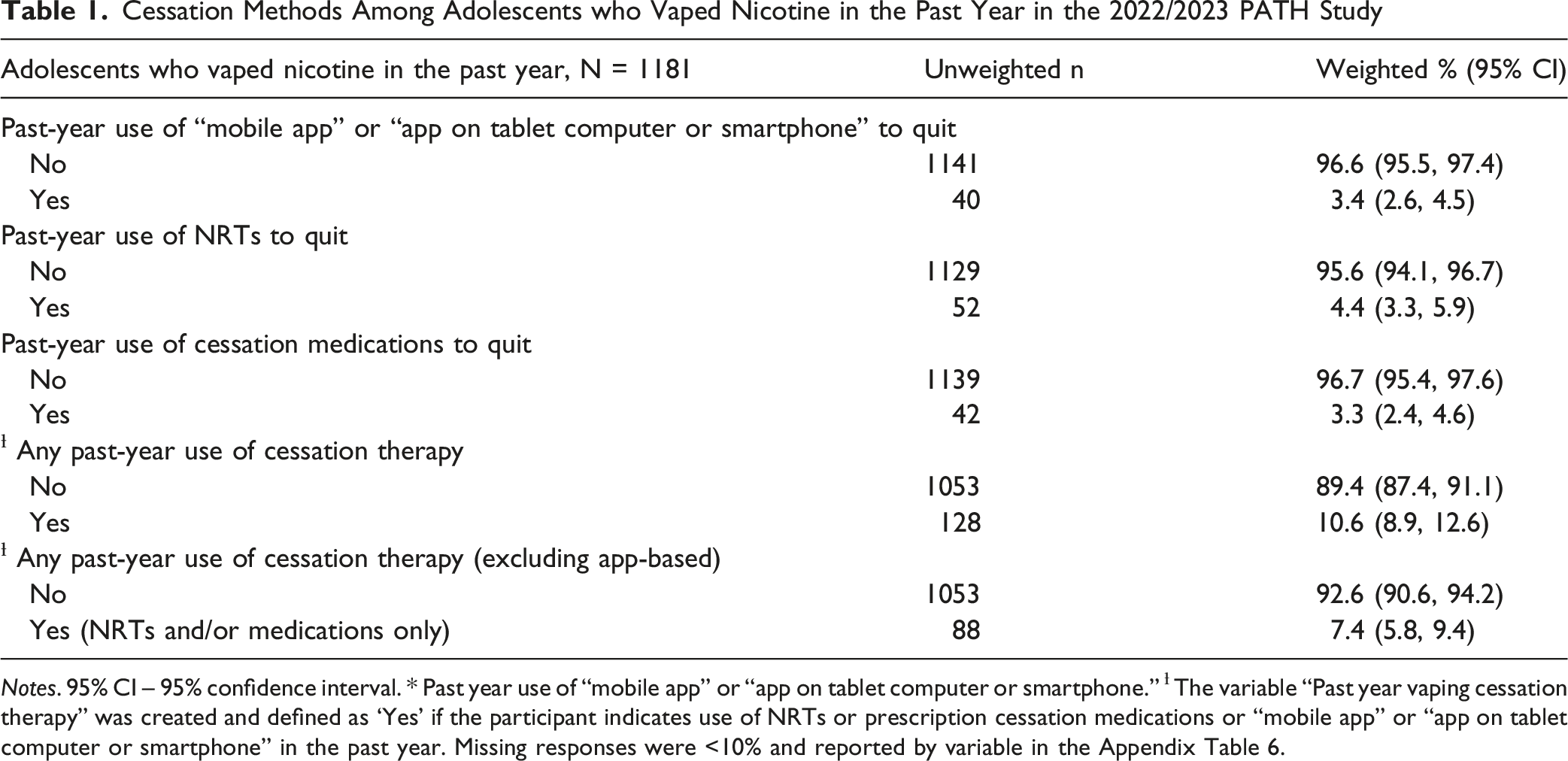
Notes. 95% CI – 95% confidence interval. * Past year use of “mobile app” or “app on tablet computer or smartphone.” ƚ The variable “Past year vaping cessation therapy” was created and defined as ‘Yes’ if the participant indicates use of NRTs or prescription cessation medications or “mobile app” or “app on tablet computer or smartphone” in the past year. Missing responses were <10% and reported by variable in the Appendix Table 6.
Adolescents who reported wanting to vape within 30 minutes of waking (aOR: 2.83; 95% CI: 1.49, 5.36) had higher odds of using any cessation therapy compared to those who reported wanting to vape more than 1 hour of waking. Similarly, adolescents who were planning to quit in the next 12 months (aOR: 1.88; 95% CI: 1.10, 3.20) had higher odds of any cessation therapy compared to those who were not planning to quit. Adolescents who identified as Hispanic had lower odds (aOR: 0.46, 95% CI: 0.25, 0.85) of reporting any cessation treatment compared to non-Hispanic White adolescents. We did not detect significant associations for other demographic or behavioral factors. Given the sparse cells and limited power, these are interpreted as inconclusive rather than as evidence of no association (Appendix Table 2).
Among adolescents who made a quit attempt in the past year, 21.5% used at least one cessation therapy in that year, and 78.5% that did not use any cessation therapy (Appendix Table 3).
In disaggregated models, the two cessation modalities showed distinct correlates. For pharmacotherapy-based methods (NRT or cessation medications; Appendix Table 4), wanting to vape within 30 minutes of waking was associated with higher odds of use in both unadjusted (OR 4.45, 95% CI 2.16, 9.18) and adjusted (aOR 3.06, 95% CI 1.93, 4.85) models, whereas planning to quit within 12 months was not significantly associated with pharmacotherapy use (Appendix Table 4). For app-based use (Appendix Table 5), shorter time to first vape after waking and planning to quit within 12 months were each associated with higher odds of use, with the 30-minute-to-1-hour dependence category (aOR 2.47, 95% CI 1.05, 5.79) and planning to quit within 12 months (aOR 9.70, 95% CI 3.87, 24.31) remaining significant, while the strongest dependence category (<30 minutes) was attenuated and no longer significant (aOR 3.59, 95% CI 0.95, 13.54). (Appendix Table 5).
Discussion
These exploratory findings show that about 1 in 10 U.S. adolescents who vape nicotine use cessation aids. Those who reported higher nicotine dependence and readiness to quit had higher odds of using any cessation therapy, while Hispanic adolescents had lower odds of reporting any cessation therapy.
The results showing low use of NRTs and cessation medications among adolescents in the same year they made a vaping quit attempt, suggest a disconnect between available interventions and actual youth behavior. Additionally, the use of these cessation tools even among adolescents who did not indicate a ‘quit’ attempt suggests some youth may be using these therapies for other reasons (e.g., limiting their vaping frequencies) 11 rather than completely quitting, as demonstrated in other studies with adults. 12 Low use may also reflect the cost of these products and adolescents’ reluctance to disclose vaping to parents or clinicians, which constrains access to prescription-based cessation options. In the U.S., most cessation medications are not FDA-approved for adolescents, and this regulatory context likely contributes to the low utilization and may limit clinician prescribing. Because PATH does not capture how these cessation aids were obtained, we cannot determine whether the reported medication use reflects clinician prescribing or informal access. Therefore, findings should be interpreted cautiously. Additionally, prior research shows that unassisted quitting (“cold turkey” quitting) remains a predominant real-world cessation strategy among adolescents 5 and should be considered when interpreting the low uptake of cessation aids observed in this study. A recent systematic review and meta-analysis synthesizing vaping cessation interventions provides broader evidence that behavioral and pharmacologic approaches show promise for youth, 13 underscoring the need for more accessible and youth-oriented cessation resources with messaging that could potentially enhance readiness to quit.
Our findings also suggest that nicotine dependence and readiness to quit were associated with higher odds of using cessation aids. 14 Cessation therapists could optimize the delivery of behavioral therapy and pharmacotherapy by leveraging information on readiness to quit and nicotine dependence severity for tailored interventions, thereby enhancing success. Furthermore, the observed lower odds of cessation therapy use among Hispanic compared to non-Hispanic White adolescents likely reflects a complex interplay of cultural, linguistic, structural, and access factors. Potential mechanisms include limited availability of culturally appropriate services, language barriers, immigration-related concerns, lower healthcare engagement, and family-based decision-making norms. Because the models did not include contextual variables or interaction terms, the mechanisms underlying this disparity cannot be isolated, and these findings should be interpreted cautiously and treated as hypothesis-generating. This warrants further investigation and targeted public health strategies to ensure equitable support.
This study has some limitations. First, the cross-sectional design does not allow for causal inference. Second, the self-reported data may be subject to recall bias. Third, the low prevalence of cessation therapy use produced sparse cells for several variables, limiting statistical power to detect significant associations; as a result, null findings should be interpreted as inconclusive rather than evidence of effect. Fourth, because the app-based item was assessed only among established users who reported a quit attempt and app use, the composite outcome is likely underestimated and may be subject to misclassification. These prevalence estimates should be interpreted as lower bounds, and app use among adolescents who reduced rather than fully quit could not be captured. Because the composite groups have modalities of differing mechanisms and evidence base, it should be read as a marker of any aided cessation effort rather than of a single, uniform intervention. Fifth, although time to first vape after waking was adapted from recent youth vaping studies, which support its use, it may not robustly capture e-cigarette dependence, and the overall sample size and sparse cells precluded the use of more detailed PATH dependence indicators. Sixth, data were collected in 2022-2023, and the adolescent nicotine landscape, including product types, emerging cessation tools, and regulatory and legislative actions, is evolving rapidly; current patterns of cessation-aid use may differ from those observed here. Finally, there may be residual confounders such as parental involvement and healthcare access, which were not accounted for in the analysis.
Overall, these findings highlight the need for youth-oriented vaping cessation interventions. Tailoring accessible, culturally responsive cessation support that integrates both behavioral and pharmacotherapeutic components14,15 may improve the use of cessation therapies among adolescents who vape nicotine, reduce nicotine dependence and advance health equity. Most adolescents who use nicotine products attempt to quit without assistance and data is sparse on their use of cessation methods, particularly pharmacotherapy. This study uses nationally representative data to show that very few adolescents who vape nicotine use cessation therapy, with 10.6% reporting any cessation therapy. It also identifies predictors of treatment use. Findings highlight the need for targeted and appropriate cessation interventions that address readiness to quit and cultural barriers. For practice, school-based health centers and pediatric clinics can incorporate brief cessation counseling and provide guidance on evidence-based tools. Community health workers, school counselors, and youth-serving organizations can help address cultural and language barriers, particularly for Hispanic youth, through tailored outreach and navigation support. Public health agencies can also improve implementation by expanding low-cost access to NRTs and promoting youth-friendly app-based behavioral tools.SO What?
What is Already Known on This Topic?
What Does This Article Add?
What Are The Implications for Health Promotion Practice or Research?
Supplemental Material
Supplemental Material - Pharmacotherapy and Behavioral Cessation Methods Used by Adolescents Who Vape Nicotine
Supplemental Material for Pharmacotherapy and Behavioral Cessation Methods Used by Adolescents Who Vape Nicotine by Olufemi Erinoso, Wei Li, Ebbie Kalan, Olatokunbo Osibogun in American Journal of Health Promotion.
Footnotes
Ethical Considerations
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.