
Abstract
Purpose
To examine how adults respond to real-world health videos that vary in credibility.
Design
Randomized, within-subjects online experiment.
Setting
Online U.S. survey.
Sample
179 adults recruited from an online panel.
Intervention
Participants viewed one misleading and one evidence-based health video, in randomized order.
Measures
Before viewing, participants reported trust in traditional and social media. After each video, they rated perceived information credibility (PIC) and perceived source credibility (PSC), relevance, and behavioral intention to adopt the recommended behavior. Demographic data were also collected.
Analysis
Paired-samples t-tests and hierarchical linear regressions examined responses to evidence-based vs misleading videos and associations among the variables.
Results
The evidence-based video was rated higher for relevance (t (178) = −4.93, P < .001), PSC (t (178) = −11.36, P < .001), PIC (t (178) = −10.61, P < .001), and intention (t (178) = 5.73, P < .001). For both videos, PSC and relevance were positively associated with intention. Trust in traditional media was related to higher PSC (b = .43, P < .001) and PIC (b = .35, P < .001) of the evidence-based content, whereas trust in social media was related to higher PSC (b = .46, P < .001) and PIC (b = .33, P = .022) of the misleading content. Higher education was associated with a better ability to distinguish between the PSC and PIC of the two videos (ps < .01).
Conclusions
Findings highlight psychological and contextual factors shaping engagement with online health information and the importance of speaker credibility and platform trust in promoting informed health decision-making.
Keywords
Purpose
The dissemination of health misinformation on social media and video-sharing platforms poses a significant threat to public health. 1 Beyond clinical consequences, this phenomenon raises concerns for public understanding of science, as many rely on digital platforms to form opinions about scientific and medical issues. Misinformation can undermine trust in evidence-based recommendations, 2 reduce adherence to preventive behaviors, 3 and promote the adoption of unproven or harmful techniques (eg, using vitamin supplements to prevent viral infection). 4 Despite rising attention and regulation, health misinformation continues to thrive in digital environments where engagement metrics like views and shares often take precedence over accuracy.5,6 One particularly understudied area concerns how individuals process and respond to health misinformation in short-form video format, especially in comparison to credible, evidence-based content. Unlike text-based misinformation, videos integrate audiovisual cues, storytelling, and personal connection presence, 7 all of which may influence perceived credibility and behavioral intentions.8–10 These dynamics complicate efforts to strengthen public discernment between accurate science and pseudo-scientific claims. Yet experimental research comparing individual-level responses to real-world misleading vs evidence-based health videos remains limited. This gap is especially salient given that short-form platforms like TikTok and YouTube are among the most common sources of health information for the public.8,11,12
Theoretical models of credibility 13 suggest that both information credibility and source credibility play key roles in how information is evaluated. These perceptions, in turn, shape behavioral intentions, particularly when audiences lack prior knowledge or motivation to critically evaluate the content. Drawing from the Elaboration Likelihood Model (ELM), 14 individuals under low-involvement conditions often rely on heuristic cues—such as the speaker’s delivery fluency—rather than engaging in systematic processing of message content. This reliance on superficial cues may exacerbate the spread of health misinformation and distort laypeople’s perceptions of scientific validity. 15
Prior work also underscores the role of digital health literacy,16,17 including the ability to access, interpret, and critically evaluate online health information. Factors such as general trust in media and educational attainment may moderate individuals’ capacity to differentiate between accurate and misleading content. 18 However, few studies have examined how these factors operate when people are exposed to both misleading and evidence-based health information in naturalistic video formats—a growing source of informal science communication. 19
This study presents a randomized, within-subjects online experiment conducted with a U.S. national adult sample. Each participant viewed one misleading and one evidence-based health video, presented in random order. We examined how perceived information credibility, source credibility, and information relevance predicted participants’ intentions to adopt the behaviors being recommended in each video. We also assessed whether general trust in social and traditional media predicted perceived credibility and explored which characteristics (eg, education) were associated with individuals’ ability to differentiate between low- and high-credibility content. By examining individual responses to real-world video content, this study contributes to ongoing conversations about the mechanisms that support—or hinder—the public’s ability to recognize credible scientific information in an increasingly crowded and contested media environment.
Methods
Sample
We conducted an online survey and recruited a national sample of adults aged 18 and older living in the United States using Prolific, a sample service platform that enables timely online recruitment with numerous features ensuring high-quality data. 20 We monitored recruitment during data collection to approximate balance across key demographic categories, including age and gender, and to promote heterogeneity in race and ethnicity in our sample. Participants were enrolled from March-April 2024. The study was approved by the university’s IRB.
Design
After providing informed consent, participants were asked about their general perceptions regarding health information. They were then presented with two health-related videos: one intended to be misleading and one evidence-based (described below). Following each video, participants rated their perceptions of the information, the source (ie, the speaker in the video), and their intention to adopt the behavior described in the video. Afterwards, we assessed health and media literacy and collected sociodemographic information, including education level, race/ethnicity, age, and gender. At the end of the survey, participants were debriefed and informed that there was no evidence to support the statements made in the misleading video.
Videos
Both videos were from TikTok and had received more than 250K views. 1 We selected high-reach real-world videos to prioritize ecological validity and to reflect the types of short-form health information that people commonly encounter online. Each video lasted approximately 1 min and was embedded into the survey so that additional video content (eg, the channel name of the content creator, likes, and comments) was not visible. This method was used to reduce the influence of platform-level heuristic cues and ensure participants’ evaluations remained focused on the video content and the speaker. In each video, a man (appearing to be aged under 40, with a light complexion) spoke directly to the camera about a health topic and had a tone that was friendly but not overly animated. The misleading video promoted neck stretches to “reset” the vagus nerve. The idea of “resetting your nervous system” was considered misleading because it suggests a quick, definitive fix for nervous system dysregulation, while scientific evidence indicates that regulation necessitates experiential learning encompassing multiple personalized states (eg, mapping out the personal need emotionally and physically).21,22 Another reason for selecting this as our misleading video was that it did not involve an immediately dangerous health recommendation. The evidence-based video provided information on the flu vaccine, supported by CDC sources, to demonstrate the prevalence of the flu and the effectiveness of the flu shot in that particular year. Video order was randomized across participants to minimize the effect of message order bias. Directly after each video, participants were asked a question about the video content to verify that they had watched the video.
Measures
General Trust in Sources of Health Information
Before exposure to the videos, participants rated their trust in health information from various sources on a scale from 1 (“not at all”) to 5 (“completely”). An index was created by averaging trust ratings across six social media platforms: “Facebook,” “Instagram,” “Snapchat,” “TikTok,” “Twitch,” “Twitter (now X),” “Reddit,” and “YouTube” (M = 1.78, SD = .63). Trust ratings for four traditional media outlets were averaged to form an index: “Traditional Newspapers and Magazines,” “Television News,” “News websites (eg, ABC News, New York Times, Fox News),” and “Newsletters” (M = 2.43, SD = .80).
General Means of Acquiring Health Information
Prior to the videos, we posed a set of four hypothetical scenarios to participants, each followed by an open-ended question. Two scenarios were aimed at assessing how participants passively acquired health information; these scenarios described a new global health event (eg, a new disease spreading across the globe) and participants were asked “how would you be most likely to hear or learn about this?” Two other scenarios measured how participants actively sought out health information; these scenarios described a new personal health event (eg, noticing a new mole) and participants were asked “what would you do to learn more about it?”
Perceived Information Credibility (PIC)
The measurement of PIC was adapted from Appelman and Sundar’s 23 three-item credibility scale. Following each video, participants were asked to indicate, on a 5-point Likert scale, the extent to which each video was “credible,” “authentic,” and “believable.” To create an index, we averaged scores (misleading: Cronbach’s ⍺ = .92; evidence-based: Cronbach’s ⍺ = .91).
Perceived Source Credibility (PSC)
Adapted from Nekmat et al., 24 PSC was measured with six items using a 5-point Likert scale (eg, “I think the person in the video is reliable.”). To create an index, we averaged scores (misleading: Cronbach’s ⍺ = .96; evidence-based: Cronbach’s ⍺ = .96).
Perceived Information Relevance (PIR)
Adapted from Lee and Kim, 25 PIR was measured with three items on a 5-point Likert scale. To create an index, we averaged scores (misleading: Cronbach’s ⍺ = .93; evidence-based: Cronbach’s ⍺ = .91).
Differentiation Scores
We computed within-subject difference scores for PIC and PSC. These scores were calculated by subtracting participants’ responses to the misleading video from their responses to the evidence-based video, such that higher scores reflected relatively more favorable evaluations of the evidence-based vs the misleading content. Unlike the PIC and PSC scores on their own (which can indicate, in part, general levels of trust for any type of health video), these differentiation scores indicate a person’s ability to distinguish credible from misleading health content.
Behavioral Intention to Adopt
Following each video, we asked participants about their intention to use the technique described in the video over the next 12 months, using a 5-point Likert Scale (misleading: M = 2.43, SD = 1.42; evidence-based: M = 3.37, SD = 1.52).
Literacy
Health literacy was assessed using items adapted from Chinn and McCarthy 26 to evaluate functional, communicative, and critical health literacy, with all items on a 3-point scale (1 = rarely, 2 = sometimes, 3 = often). Media literacy was measured using items adapted from Koc and Barut 27 to assess functional consumption and critical consumption, with all items rated on a 5-point scale (1 = strongly disagree, 5 = strongly agree).
Sociodemographic Variables
Participants also reported their age (in years), race/ethnicity, highest level of education, and gender identity.
Attention Checks
We included two attention check questions at different points in our survey. The first question was an “instructional manipulation check” type question, in which participants are explicitly instructed to answer a question in a certain way. The second attention check question was a “nonsensical items” type question, in which only one response can be justified as objectively correct.
Data Analysis
Analyses began with descriptive statistics to characterize the sample. For the open-ended questions on acquiring health information, two investigators developed codes based on an initial review of responses, then applied the coding scheme to code all responses independently. Coders met periodically with a senior investigator to resolve discrepancies and identify new codes as necessary.
We next conducted a series of within-subjects paired-sample t-tests to compare participants’ responses to the evidence-based vs misleading health videos on four key outcomes: PIR, PSC, PIC, and behavioral intention. We then conducted hierarchical linear regression analyses to examine how participants’ perceptions of the videos influenced their behavioral intentions to adopt the behaviors depicted in the video (H1) and whether general trust in social media and traditional media predicted perceptions of the videos (H2). All models controlled for age, gender, education level, and video order. Assumptions of normality, homoscedasticity, linearity, independence of errors, and absence of outliers were checked and met before performing the analyses. To address RQ1, we conducted linear regressions to analyze whether health and media literacy and individual characteristics (ie, education level, gender identity, and age) predicted participants’ ability to differentiate between evidence-based and misleading videos using the differentiation scores. To enhance statistical robustness, 95% confidence intervals were generated using 5000 bootstrap samples.
Results
Descriptive Statistics
Demographic Characteristics of Participants (N = 179)
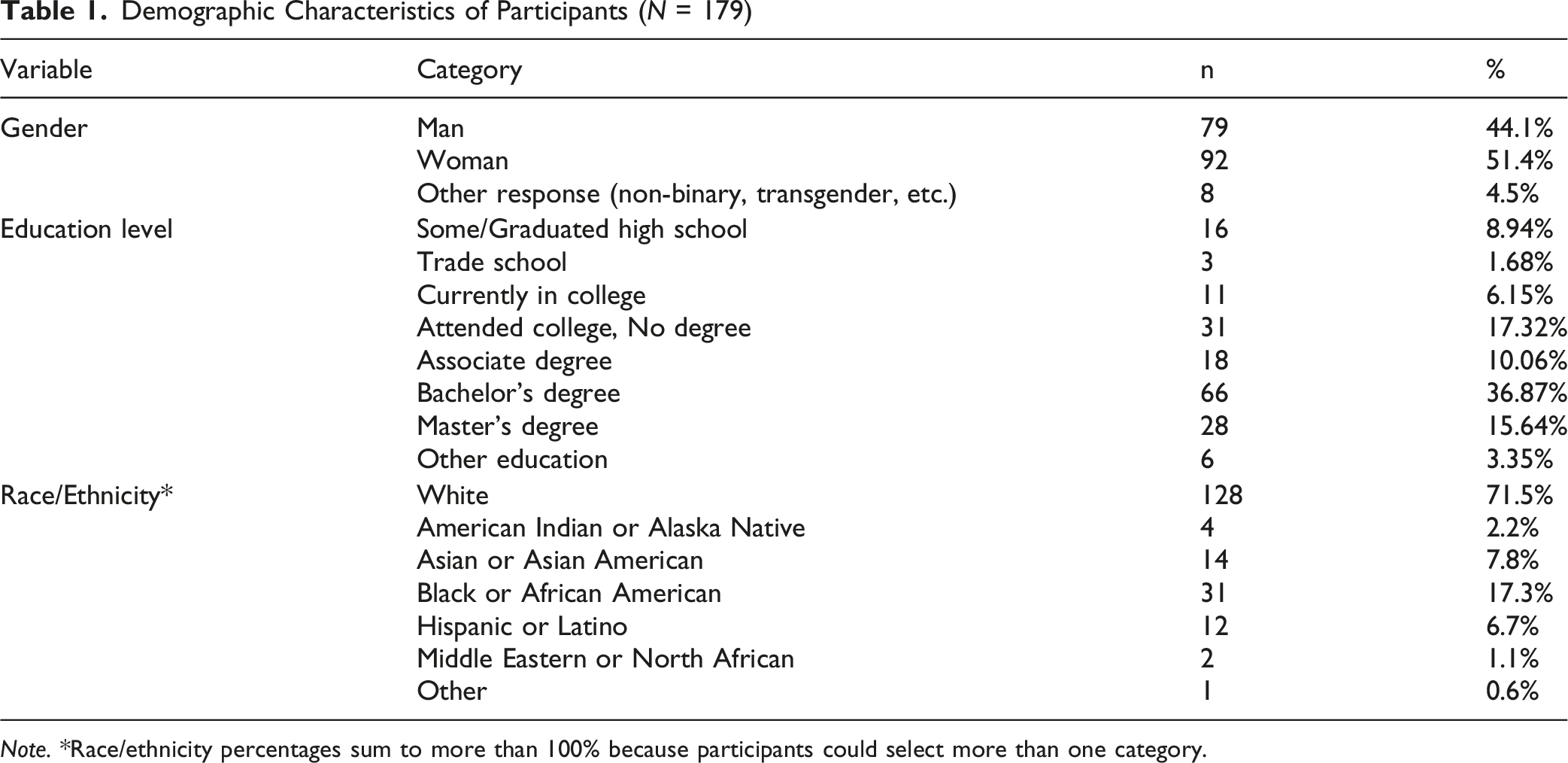
Note. *Race/ethnicity percentages sum to more than 100% because participants could select more than one category.
Although not designed for formal analysis, the coded open-ended responses offer a contextual window into participants’ everyday information-seeking habits and underlying assumptions about trustworthy sources. For the passive health information scenarios (eg, learning about a new disease), the majority of participants reported they would learn from a social media platform. For example: “I would most likely hear about it through Instagram or TikTok. Those types of crowds are very quick to spread information.” For the active health information scenarios (eg, a new mole), many participants described consulting a health professional; however, using an online source of information was the most frequent response. For example: “WebMD would be a good result for a generic type of pain.”
Regarding PIR, participants rated the evidence-based video (M = 3.58, SD = 1.04) significantly higher than the misleading video (M = 2.99, SD = 1.24), t(178) = −4.93, P < .001, Cohen’s d = −.37, 95% CI [−.82, −.35]. Likewise, for PSC, the evidence-based video (M = 3.44, SD = 0.94) was rated significantly higher than misinformation video (M = 2.46, SD = 1.00), t(178) = −11.36, P < .001, Cohen’s d = −.85, 95% CI [−1.15, −.81]. Finally, for PIC, the evidence-based video (M = 3.73, SD = .94) was also rated significantly higher than the misleading video (M = 2.62, SD = 1.09), t(178) = - 10.61, P < .001, Cohen’s d = −.79, 95% CI [−1.31, −.91]. These findings indicate that participants consistently perceived the evidence-based video as more credible, relevant, and trustworthy compared to the misleading video.
In terms of intentions to use the behavior described in the video, the evidence-based video (M = 3.37, SD = 1.52) received significantly higher ratings than the misinformation video (M = 2.43, SD = 1.42), t (178) = 5.73, P < .001, Cohen’s d = .43, 95% CI [.63, 1.25], indicating a stronger intention to engage in the evidence-based behavior.
Predicting Intentions From Perceptions (H1)
Hierarchical Regression Predicting Behavioral Intentions From Perceptions of the Videos
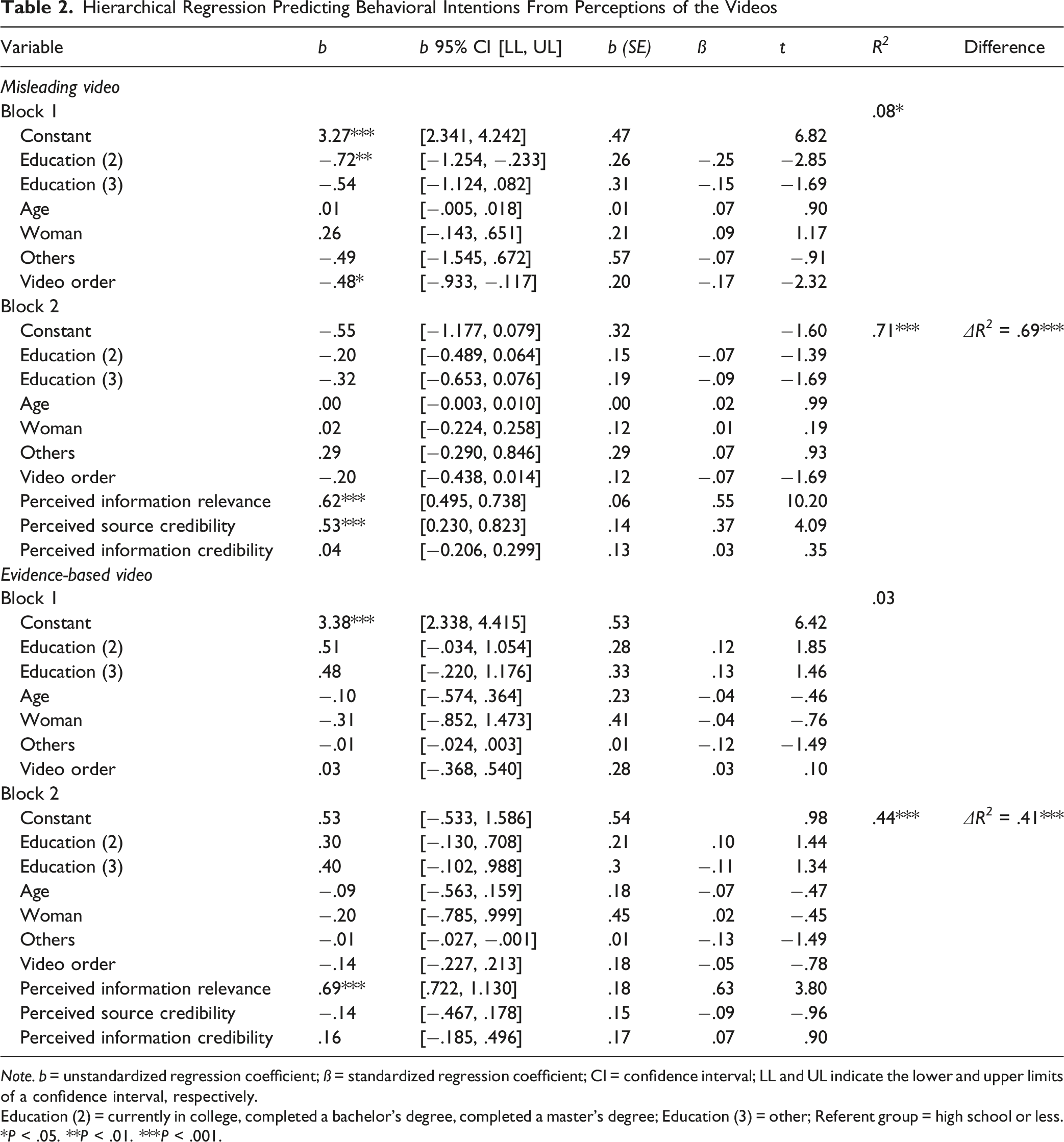
Note. b = unstandardized regression coefficient; ß = standardized regression coefficient; CI = confidence interval; LL and UL indicate the lower and upper limits of a confidence interval, respectively.
Education (2) = currently in college, completed a bachelor’s degree, completed a master’s degree; Education (3) = other; Referent group = high school or less.
*P < .05. **P < .01. ***P < .001.
In our analyses with the evidence-based video, demographic variables did not significantly predict behavior intention, R 2 = .03, F (6, 172) = .92, P = .48. Adding perceptions significantly improved the model, F-change (3, 169) = 41.35, P < .001, with the full model explaining 44% of the variance in intention (ΔR 2 = .41). Among the predictors, PIR was a significant positive predictor (b = .69, 95% CI [.722, 1.130], P < .001), while PSC (b = −.14, 95% CI [−.467, .178], P = .38) and PIC (b = .16, 95% CI [−.185, .496], P = .37) were not significant.
Influence of Trust in Sources of Health Information on Perceptions (H2)
Hierarchical Regression Predicting Perceived Source Credibility and Perceived Information Credibility From Trust in Sources of Health Information
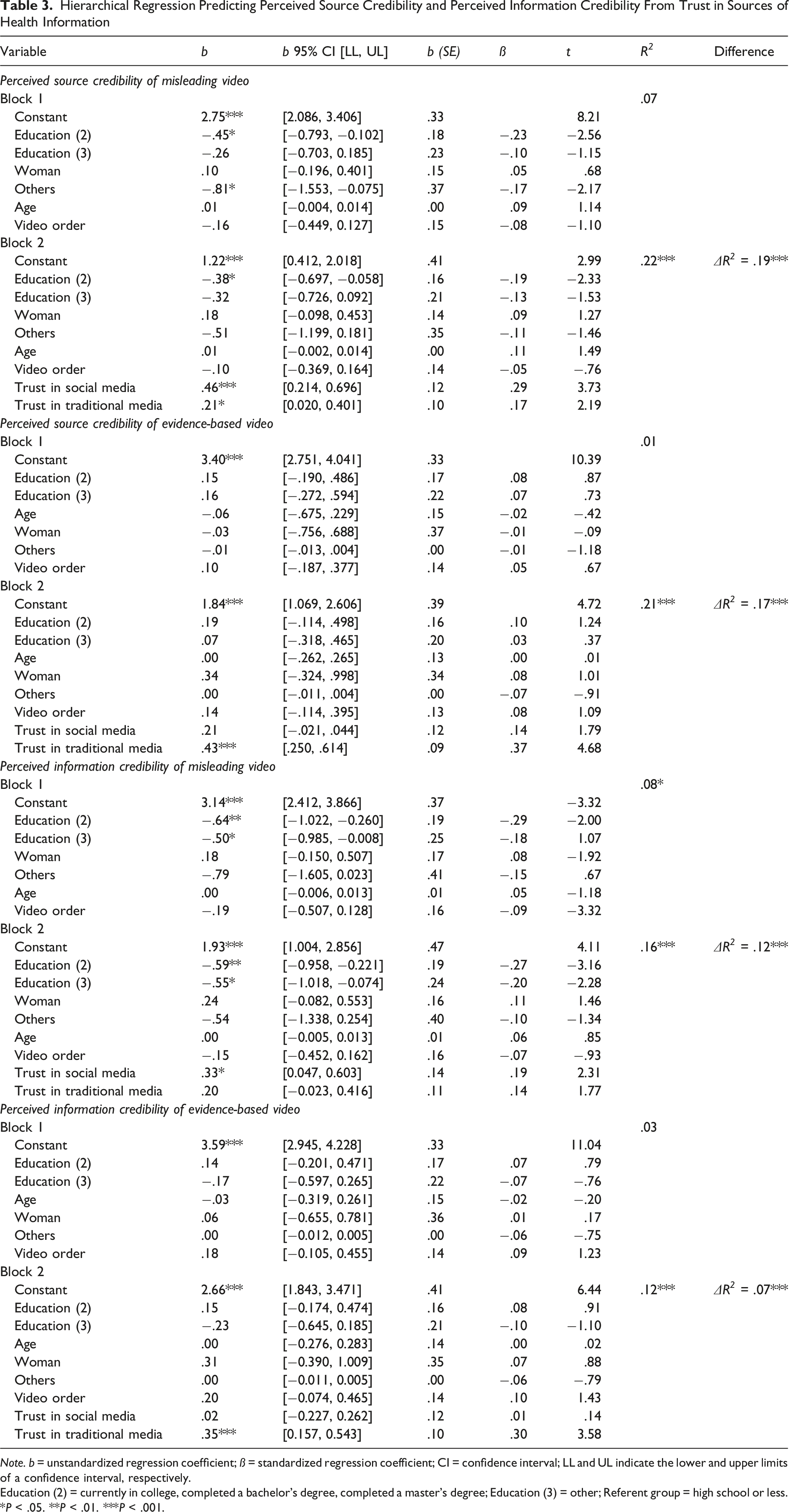
Note. b = unstandardized regression coefficient; ß = standardized regression coefficient; CI = confidence interval; LL and UL indicate the lower and upper limits of a confidence interval, respectively.
Education (2) = currently in college, completed a bachelor’s degree, completed a master’s degree; Education (3) = other; Referent group = high school or less.
*P < .05. **P < .01. ***P < .001.
PIC. For the misleading video, demographic variables explained a small but significant proportion of variance, R 2 = .08, F (6, 172) = 2.56, P = .021. Adding trust significantly improved the model, F-change (2, 170) = 7.75, P < .001, with the full model explaining 12% of the variance in PIC (ΔR 2 = .12). Trust in social media was a significant positive predictor (b = .33, 95% CI [0.047, 0.603], P = .022), while trust in traditional media was not significant (b = .20, 95% CI [−0.023, 0.416], P = .079). For the evidence-based video, demographic variables did not significantly predict perceptions, R 2 = .03, F (6, 172) = .82, P = .556. Adding trust also significantly improved the model, F-change (2, 170) = 8.44, P < .001, with the full model explaining 7% of the variance in PIC (ΔR 2 = .07). Trust in traditional media was a significant positive predictor (b = .35, 95% CI [0.157, 0.543], P < .001), while trust in social media was not significant (b = .02, 95% CI [−0.227, 0.262], P = .888).
Perceptions of Evidence-Based vs Misleading Videos (RQ1)
Multivariable Associations Between Health/Media Literacy, Individual Characteristics, and Credibility Difference Scores (Where Higher Scores Indicate Greater Perceived Credibility for the Evidence-Based Video Compared to the Misleading Video)
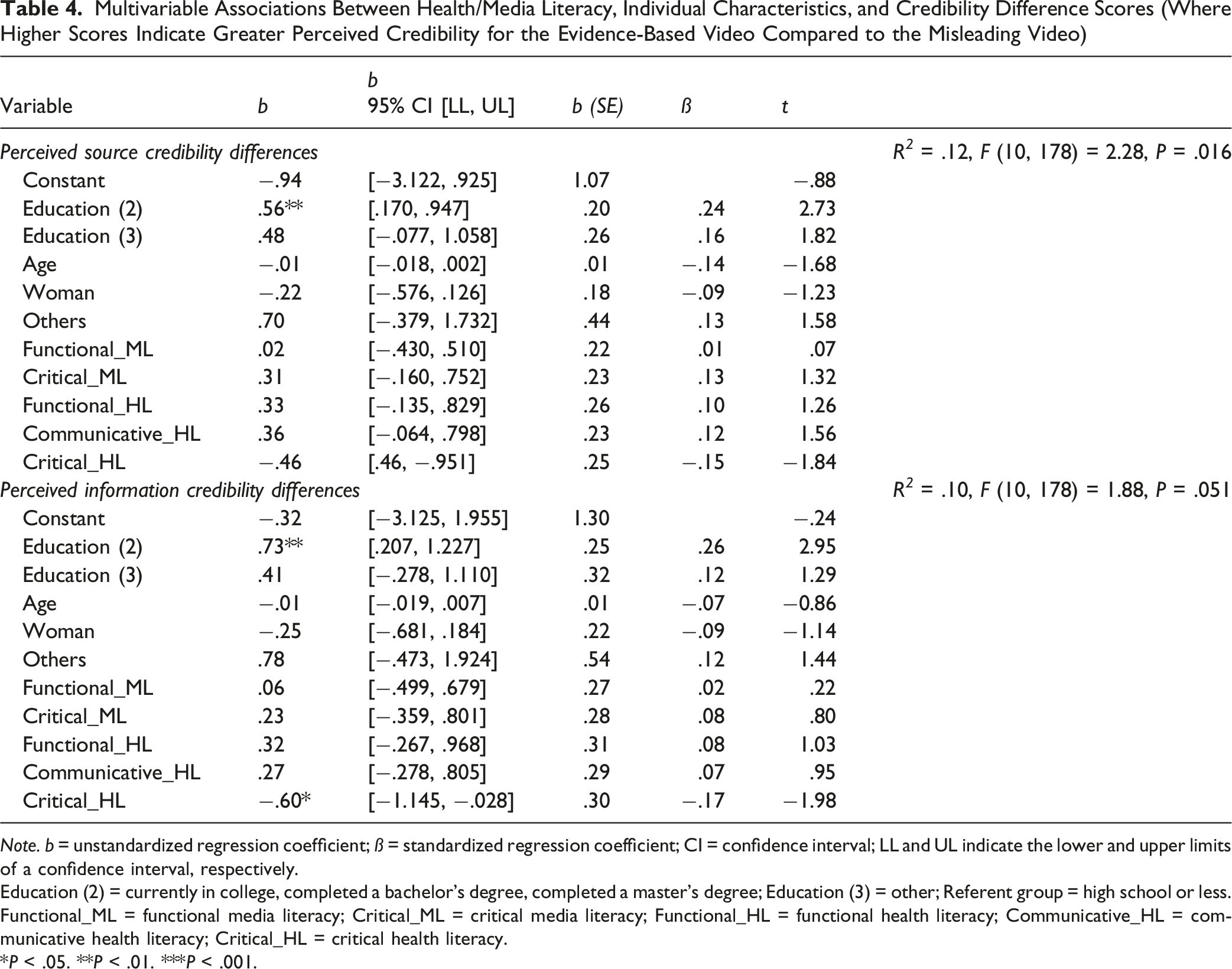
Note. b = unstandardized regression coefficient; ß = standardized regression coefficient; CI = confidence interval; LL and UL indicate the lower and upper limits of a confidence interval, respectively.
Education (2) = currently in college, completed a bachelor’s degree, completed a master’s degree; Education (3) = other; Referent group = high school or less.
Functional_ML = functional media literacy; Critical_ML = critical media literacy; Functional_HL = functional health literacy; Communicative_HL = communicative health literacy; Critical_HL = critical health literacy.
*P < .05. **P < .01. ***P < .001.
In contrast, age, gender identity, and both media literacy subscales—functional and critical—were not significant predictors of either differentiation outcome (ps > .10). Similarly, functional and communicative health literacy were not significantly associated with PSC or PIC differentiation. Critical health literacy, however, was negatively associated with PIC differentiation (b = −.60, 95% CI [−1.145, −.028], P = .049), suggesting that people who self-reported higher critical health literacy were worse at distinguishing evidence-based vs misleading video content.
Discussion
This study provides empirical evidence on how adults in the U.S. evaluate and respond to real-world health-related videos that differ in credibility. We found that participants expressed stronger behavioral intentions to adopt the evidence-based recommendations. These patterns suggest that minimal cues in short-form digital content, such as messenger presentation, may shape health-related decisions. Importantly, general trust in media was associated with participants’ credibility perceptions, and higher educational attainment was associated with individuals’ ability to distinguish between misleading and credible video content.
Our findings contribute to theoretical models of credibility and persuasion in digital contexts. Consistent with the literature on information credibility,13,28 participants were more likely to form intentions aligned with videos they judged as personally relevant and sourced from credible messengers. PSC was found to be a stronger statistical predictor of behavioral intention than information credibility alone, especially for misleading content. This indicates that in video-based formats, the speaker’s characteristics, such as perceived expertise, are particularly influential. This aligns with previous research showing that audiovisual cues and perceived authenticity can outweigh factual content when heuristic processing occurs in practice.29,30
As reflected in participants’ open-ended responses, there is high trust and reliance on online sources for acquiring health information, both passively and actively. Our findings also underscore the continued relevance of media trust in shaping the public’s evaluations of health content. Trust in traditional media was positively associated with the perceived credibility of evidence-based content, whereas trust in social media was more closely linked to the perceived credibility of the misleading video. These patterns suggest that different forms of media trust may reflect distinct orientations toward institutional knowledge vs decentralized, peer-driven information networks.31,32 As science communication increasingly occurs in online and hybrid spaces, understanding these divergent trust profiles becomes essential for anticipating how different audiences respond to public health messages.
Concerningly, we found that our scales of health and media literacy were not related to people’s abilities to distinguish between evidence-based and misleading content. Thus, self-report measures are likely not a valid measure of a person’s ability to identify health misinformation. This finding aligns with political misinformation research, 33 showing that individuals are not good judges of their own ability to recognize political misinformation (eg, news headlines invented for the research study) when they encounter it. Researchers in this field have recommended using more skills-based assessment tools. 34
The finding that participants with higher educational attainment were more likely to distinguish between evidence-based and misleading content may reflect differences in exposure to analytical thinking and scientific reasoning. Individuals with college or graduate-level education may have had more opportunities to develop skills in logic, evidence evaluation, and critical interpretation of information—skills that are essential for identifying subtle credibility cues in multimedia formats. This pattern reveals educational disparity and suggests analytical reasoning skills as a potential target for future interventions to help more people evaluate online health content’s trustworthiness.
Our results suggest that enhancing source transparency and personal relevance in science communication may be linked to public engagement with credible health content. However, even within our national sample, the perceived credibility of the misleading video was fairly high for some individuals, suggesting that stylistic presentation, speaker fluency, or narrative appeal may continue to influence perceptions, regardless of factual accuracy. This highlights a key challenge for digital platforms and science communicators: aligning surface features of media—tone, clarity, production value—with the integrity of its evidence, in accessible formats for diverse publics. From an applied health promotion perspective, health promoters may learn from wellness-oriented videos about how to make their videos more persuasive.
Several limitations of this study warrant attention. First, although our sample was diverse in age and education, it was limited to U.S.-based adults recruited via an online platform. Replication in other sociocultural contexts is necessary to evaluate the generalizability of findings. Second, some participants may have previously encountered one or both videos, which could introduce internal validity concerns. Additionally, the two videos varied in their topics (flu vaccine vs vagus nerve), so differences in perceived relevance and behavioral intention may partly reflect baseline topic interest or preexisting perceptions. Accordingly, we interpret differences between videos cautiously and avoid attributing them solely to evidentiary support. Given our goal of examining responses to authentic, high-reach content, we chose to prioritize higher ecological validity, at the tradeoff of lower internal validity. Future studies may consider creating their own health (mis)information videos, in order to achieve higher internal validity by more tightly controlling for extraneous factors such as message topic. Finally, the outcome measure of behavioral intention was self-reported. Future research should examine actual behavioral outcomes over time or incorporate physiological or observational metrics to complement self-report data. For instance, studies could incorporate simple behavioral indicators like clicking a link for more information or engaging in verification behaviors.
In conclusion, this study advances understanding of how individuals evaluate competing health messages in digital environments. By analyzing naturalistic video content within a randomized experimental design, we offer insight into the psychological and contextual mechanisms—credibility, relevance, and media trust—that shape public discernment. For the field of public understanding of science, our findings underscore the need to integrate media design, communicator credibility, and audience trust dynamics into effective digital health communication strategies. Understanding how people evaluate and react to online health information is essential for effective health promotion in digital platforms. These findings emphasize the importance for health professionals to incorporate credible messengers, trusted platforms, and audience-focused message design to enhance public engagement with accurate health content.So What
Footnotes
Ethical Considerations
This project was reviewed and approved by an Institutional Review Board.
Consent to Participate
Informed consent was obtained from all individual participants included in the study through an agreement embedded in the survey questionnaire.
Author Contributions
Tong Lin, PhD: Conceptualization, Methodology, Formal analysis, Writing – original draft, Writing – review & editing. Dylan D. Wagner, PhD: Conceptualization, Funding acquisition, Methodology, Writing – review & editing. Daphine Choy: Conceptualization, Methodology, Writing – review & editing. Chelsie Hartman: Conceptualization, Methodology, Writing – review & editing. Abigail Henck: Conceptualization, Methodology, Writing – review & editing. Juliette A. Louer: Conceptualization, Methodology, Writing – review & editing. Laine O’Shaughnessy: Conceptualization, Methodology, Writing – review & editing. Megan E. Roberts, PhD: Conceptualization, Funding acquisition, Methodology, Supervision, Writing – review & editing. All authors approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by a Seed Grant from The Ohio State University Office of Undergraduate Education.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data will be made available on request.