
Abstract
Purpose
Trust is a critical part of patient-provider relationships and has been shown to improve patient outcomes, including increased utilization of preventative services and greater adherence to medications. However, few studies have examined health care provider trust (HCPT) among older sexual minority men (SMM) and its association with healthcare avoidance.
Design
Cross-sectional secondary data analysis.
Setting/Sample: Baseline data from the MACS/WIHS Combined Cohort Study’s Stigma and Non-Communicable Disease Syndemic Sub-Study (N = 997).
Methods
Multiple linear and multivariable logistic regression models were conducted to estimate associations between HCPT and past-year healthcare avoidance.
Results
Participants had a mean age of 59 years (SD = 13.3); 64% were White, 30% Black, and 5% identified as other races. Fifty-six percent were living with HIV. HCPT was lower among Black SMM (b = −2.23; 95% CI = −4.46, 0.00) and was positively associated with multiple income groups and having 1 (b = 3.80; 95% CI = 1.49, 6.11), 2 (b = 2.96; 95% CI = 0.67, 5.25), and 3 (b = 3.03; 95% CI = 0.53, 5.53) chronic health conditions. Past-year healthcare avoidance was inversely associated with HCPT (aOR = 0.95; 95% CI = 0.94, 0.97) and age (age 26-45 years vs 65-75 years, aOR = 0.26; 95% CI = 0.11, 0.58).
Conclusion
This work demonstrates various associations between healthcare provider trust and sociodemographic and health factors. Furthermore, lower HCPT was associated with a higher likelihood of avoiding medical care, indicating the importance of provider trust for accessing health services.
Introduction
For many older sexual and gender minority (SGM) adults, seeking and accessing health services can engender trepidation, given past stigmatizing and discriminatory experiences in healthcare environments.1-3 Many older SGM adults had such experiences during a time when identifying as a SGM was seen by society as “wrong, unhealthy, and illegal”. 4 While the recent creation of SGM-specific centers and spaces have provided services and support, these past encounters may affect how aging SGM, and the larger SGM population, access and utilize health services.
Given that the healthcare system is built on cis-heteronormative standards, older SGM individuals are more likely to not disclose their sexual orientation and/or gender identity and conceal health information from healthcare providers due to mistrust and anticipatory and experienced discrimination.4-6 These experiences have also led many older SGM adults to not seek care or to avoid the healthcare system. 4 These disparities are further exacerbated for racially diverse older SGM adults, particularly older Black SGM adults who report higher incidences of discrimination and stigma in healthcare settings 7 and often struggle with finding services tailored to their needs.8,9 For many Black individuals (SGM and non-SGM), issues with the healthcare system stem from well-documented historical mistreatment from healthcare providers resulting in deep-rooted medical mistrust.10-14
However, for some older SGM adults, hesitancy in utilizing health services has declined as they age as they have discovered ways to facilitate use of health services. A MetLife study that investigated the lives of lesbian and gay (LG) older adults noted that while many LG older adults discussed how being LG made aging more difficult, their sexual identity also helped prepare them for aging. Participants noted that due to experiencing challenges or issues that were related to their sexual orientation and/or gender identity they developed greater self-reliance, became more knowledgeable and informed about legal/financial matters, had prior experiences with handling serious health issues, and knew how to create stronger support systems. 15 Studies examining health service utilization among majority White older SGM adults have found that older age is positively associated with comfort in disclosing sexual orientation with a primary healthcare provider and discussing health issues related to one’s sexual orientation. 16 More specifically, older gay men (majority White, residing in the Southwest US) have identified several factors contributing positively to care-seeking, including the increased availability of gay doctors, providers that are SGM friendly, patient-provider trust, and overall comfort interacting with healthcare providers and staff. 1
Prior research has shown that trust is a critical aspect of patient-provider relationships. Patient trust can predict factors such as utilization of preventative services, adherence to medication or treatment plan, and continued use of services. 17 Trust can be seen as a defining characteristic of one’s relationship with healthcare providers and professionals and is reflected in a commitment to an ongoing relationship. Having less trust has been associated with being more likely to report a service was not provided, less satisfaction with care, and less likelihood of adherence to the treatment plan and reporting symptom improvement. 18 For some older SGM adults, having identity-affirming providers is associated with greater use of preventative services and improvement in the management of mental health conditions. 19 Additionally, trust has been linked to healthcare avoidance, such that the likelihood of avoiding healthcare is associated with lower trust in healthcare providers.20-22
The basis for this work comes from the conceptual model of medical care avoidance that Taber and colleagues developed. 22 Their conceptual model demonstrates four major components to why individuals avoid medical care, with physician factors falling under the component of “unfavorable evaluations of seeking medical care.” Physician factors that were listed included interpersonal concerns with a “general mistrust of doctors” being a top factor. 22 Given this background, it is important to explore further the role that healthcare provider trust may have as one ages and when they access health services. Utilizing data from the Stigma and Non-Communicable Syndemic Sub-study of the MACS/WIHS Combined Cohort Study (MWCCS), we aimed to characterize HCPT in this data and estimate its association with healthcare avoidance. We hypothesized that HCPT would be inversely associated with healthcare avoidance. Few studies have investigated healthcare provider trust in older sexual minority men; these results will provide insight into the potential relationship that healthcare provider trust has with age and healthcare avoidance in older SMM.
Methods
Study Design
Data for this study came from the Stigma and Non-Communicable Syndemic Sub-Study of the MACS/WIHS Combined Cohort Study (MWCCS). The MWCCS is a longitudinal observational cohort study that examines the health and well-being of individuals living with HIV and a socio-demographically matched comparison group without HIV. 23 The purpose of this sub-study is to examine risk and protective factors related to non-communicable disease incidence, prevalence, and control. More detailed information and study protocol procedures are available elsewhere. 24 For this current work, data utilized were drawn from baseline survey data collected between July 2023 to March 2025. At the time this study was conducted, a total of 997 eligible (at least 18 years old) MWCCS participants were enrolled into this sub-study from participating sites in Baltimore, MD/Washington, D.C.; Miami, FL; Pittsburgh, PA; Chicago, IL; Birmingham, AL; Jackson, MS; and Los Angeles, CA. The sub-study staff at each participating site contacted eligible MWCCS participants and invited them to participate in the sub-study. The sub-study relies on a single IRB of record (Advarra protocol number 00068335). 24
Measures
Healthcare Provider Trust (HCPT) Scale Score
Healthcare provider trust was assessed using the validated Health Care Relationship Trust Scale. 25 This is a 15-item scale (α = 0.92) that aims to measure patient trust in healthcare providers and was developed with a sample of individuals who were living with HIV. As an example, this scale includes questions such as, “How often does your main healthcare provider talk over your head?”; “How often does your main healthcare provider discuss options and choices with you before healthcare decisions are made?”; “My healthcare provider is committed to providing the best care possible.” Responses to these and the remaining scale questions range from 0 (none of the time) to 4 (all the time). To create a scale score, some items were reversed coded and then the score of each item was summed with a total possible score ranging from 0 to 60. A higher score indicates greater collaborative trust. 25 The reliability of this scale with this sample was 0.93. The HCPT scale score was utilized as a continuous variable for analysis as the developers of the scale did not provided validated cut off points that would allow this scale to be categorized.25,26
Healthcare Avoidance
Participants were asked “Was there a time in the past 12 months when you did not seek medical care even when you thought you should?” Responses to these questions were coded to yes (1) and no (0).27,28
Demographics
Age was categorized into groups of “26 to 45 years old,” “46 to 64 years old,” “65 to 75 years old,” and “76+ years old.” Gender was dichotomized into “cisgender man” and “transgender/non-binary man.” Race was categorized into White, Black, and another race due to small sample sizes. Hispanic ethnicity was coded to yes (1) and no (0). HIV status was coded to “living with HIV” (1) and “not living with HIV” (0). Income was categorized as “less than $6,000,” “$6001 to $12,000” “$12,001 to $18,000,” $18,001 to $24,000,” $24,001 to $30,000,” “30,001 to $36,000,” “36,001 to $75,000,” “75,001 to $100,000,” “$100,001 to $150,00,” “$150,001 to $200,000,” and “more than $200,000.” Health insurance was coded as yes (1) and no (0).
Non-Communicable Disease Burden
Participants were asked if a doctor or other healthcare provider had told them they had high cholesterol, high blood pressure, and diabetes. Each of these questions was coded to yes (1) and no (0). A non-communicable disease count variable was created and categorized into “no conditions,” “one condition,” “two conditions,” and “three conditions.” This count variable was utilized in statistical analysis.
Statistical Analysis
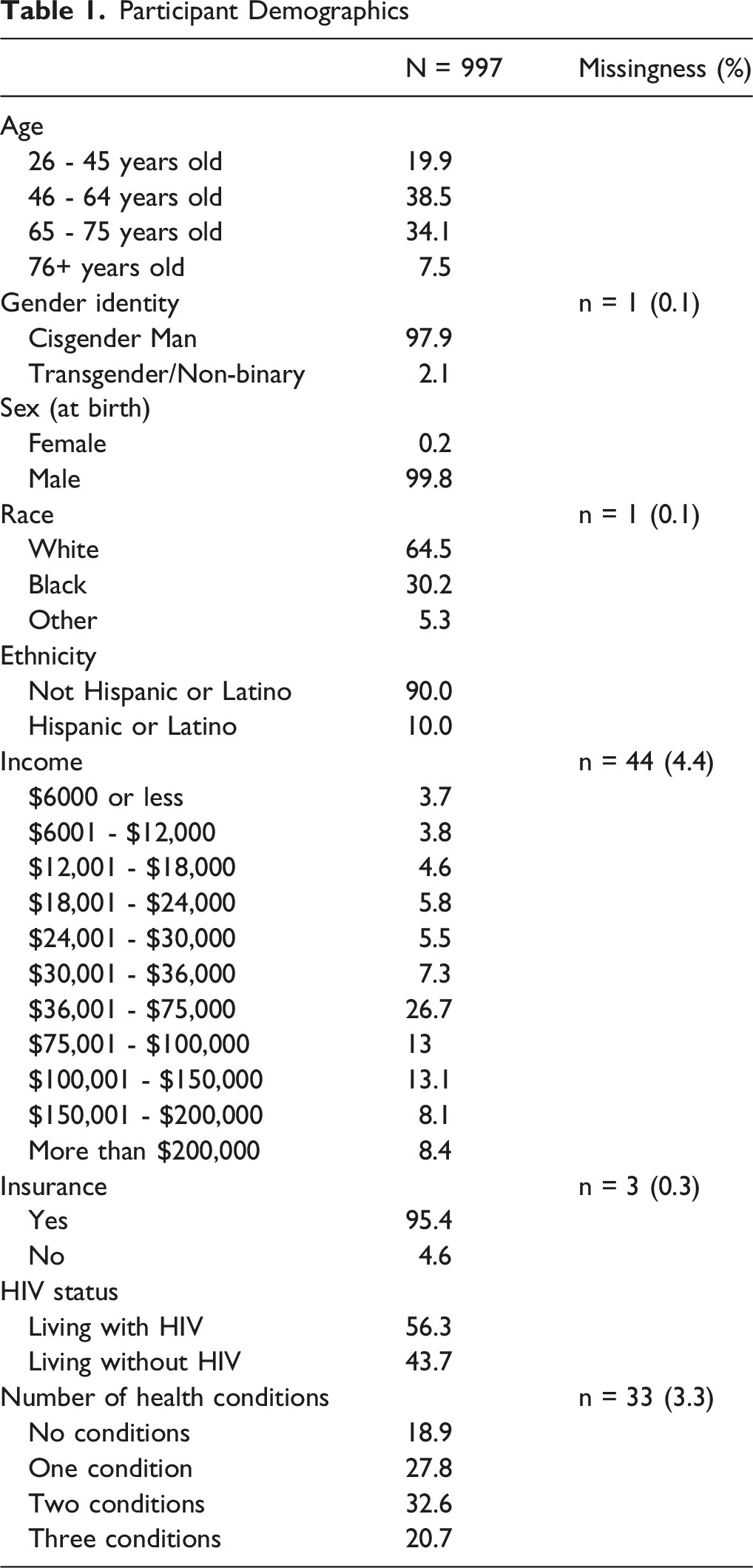
Participant Demographics
Results
Sample Demographics
The total sample size was 997 participants. Sample demographics are shown in Table 1. Mean age for the sample was 59.3yrs (SD = 13.3) with 38% of the sample in the age group of “46 – 64 years old.” Most participants identified as cisgender men (98%) and White (64%). Twenty-six percent had an income of $36,001 to $75,000. Fifty-six percent of respondents were living with HIV and 33% were managing two non-communicable health conditions (ie, high cholesterol, high blood pressure, and/or diabetes) (Table 1).
Healthcare Provider Trust (HCPT)
Multivariable Linear Regression for Healthcare Provider Trust
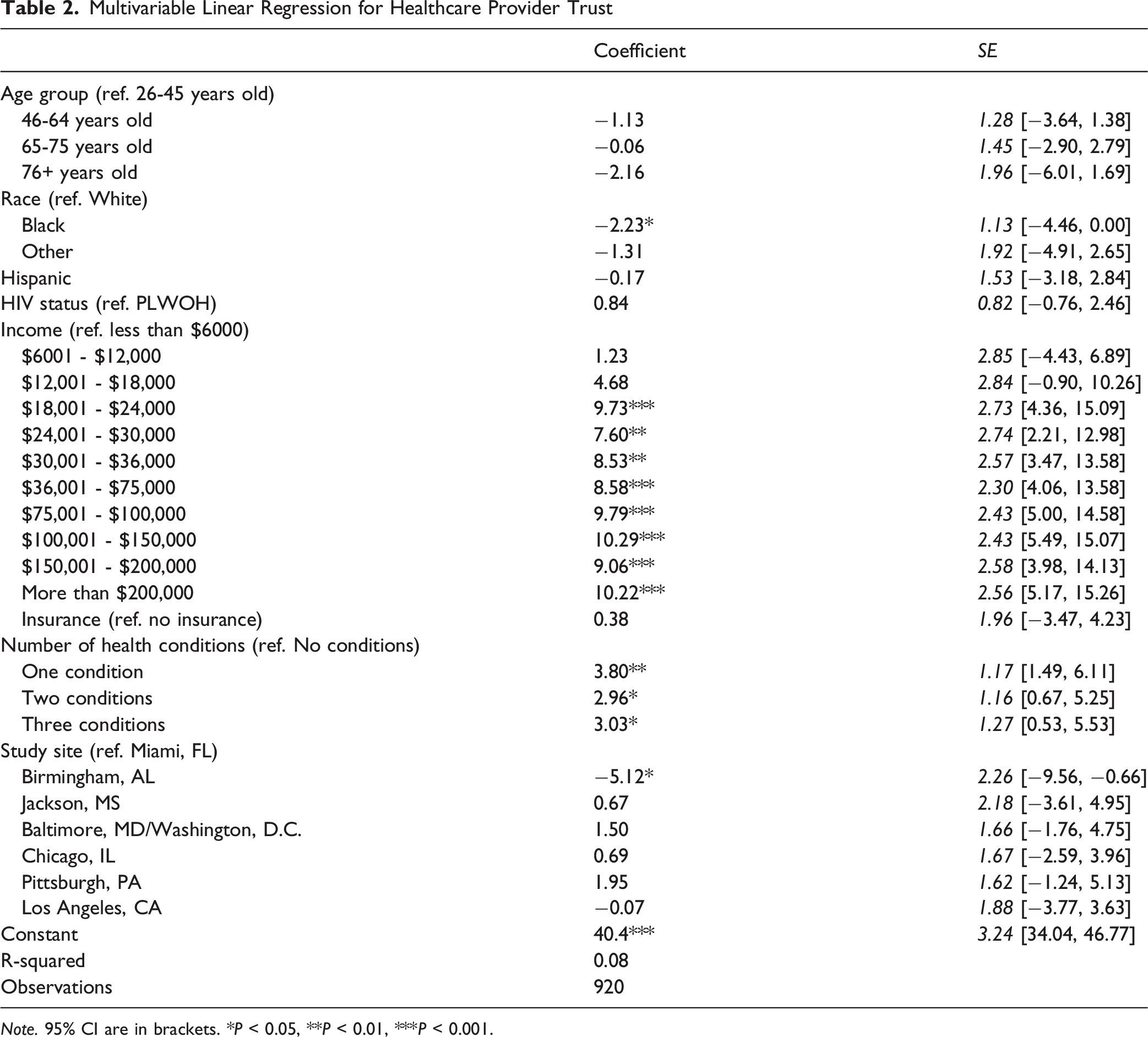
Note. 95% CI are in brackets. *P < 0.05, **P < 0.01, ***P < 0.001.
Healthcare Provider Trust and Healthcare Avoidance
Logistic Regression for Healthcare Avoidance in the Last 12 Months
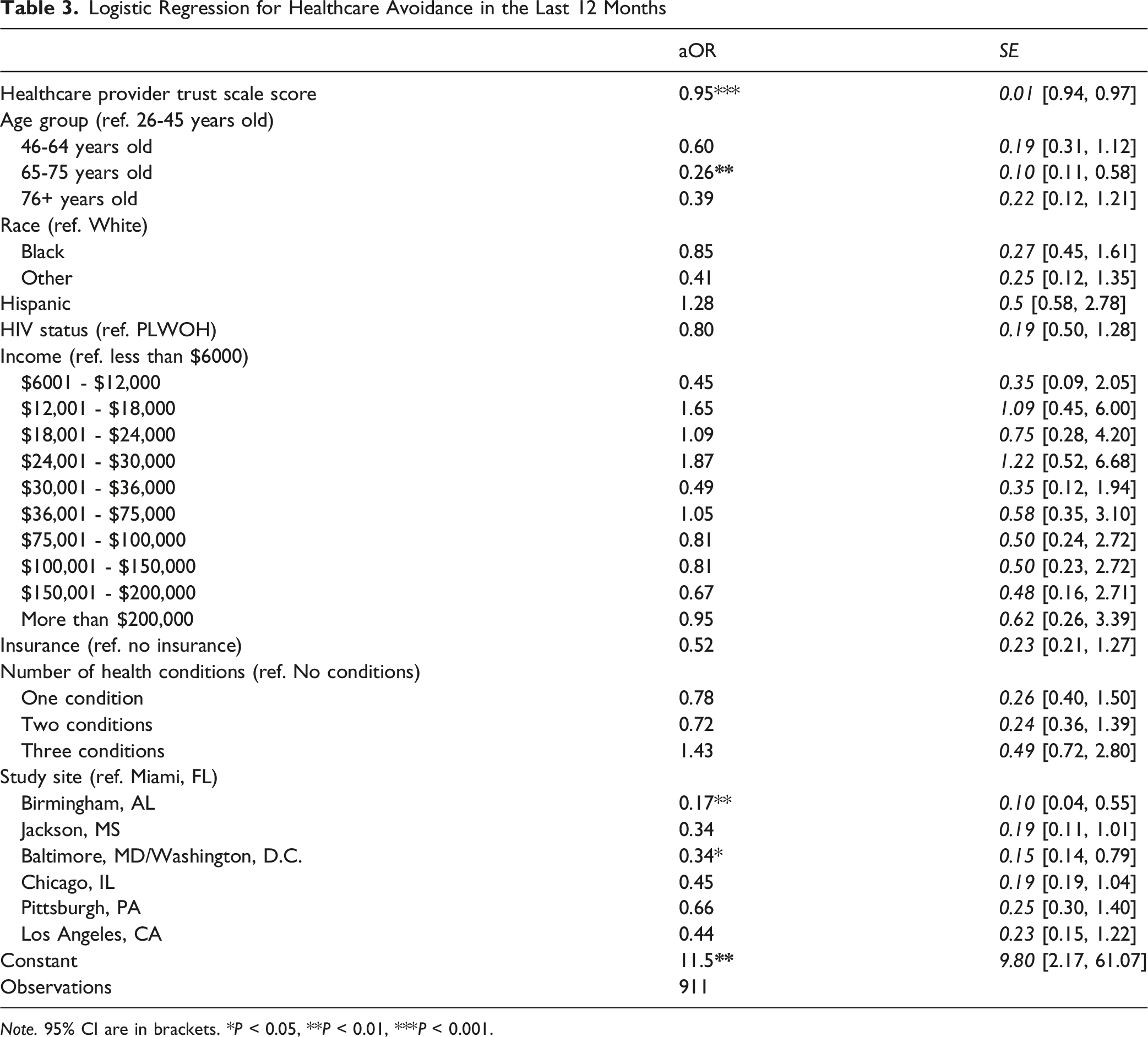
Note. 95% CI are in brackets. *P < 0.05, **P < 0.01, ***P < 0.001.
Discussion
In this cross-sectional analysis of data from the MWCCS Stigma and Non-Communicable Syndemic Sub-study, we found that Black SMM had a lower HCPT and HCPT was positively correlated with income and number of health conditions (not including HIV) but was not correlated with age. We also found that people with higher HCPT were less likely to have avoided healthcare in the past year, adding to the growing area of research focused on health equity and SGM aging. It is important to note that we found these outcomes amongst a mixed HIV serostatus group, which highlights that having healthcare provider trust and not avoiding healthcare are important for both groups, particularly for participants in this study.
Our finding of racial differences in healthcare provider trust aligns with previous work indicating that, regardless of age, racially marginalized people report and experience discrimination in the healthcare system and have medical mistrust at higher rates.5,16,31 These outcomes are also prevalent among those living with HIV. Haile and colleagues (2011) examined the effect of stigma on older, Black SMM living with HIV in New York City; many participants discussed the intense level of stigmatization they experienced in medical institutions when trying to manage chronic conditions. In learning to navigate these spaces, they had to adhere to the knowing their place to be tolerated and to receive services. They recognized that as Black SMM, they are low within the hierarchy of who society has deemed worthy of care and support. 32 Along with outcomes of the current work, previous findings highlight the lasting impact that discrimination and negative healthcare experiences can have on the individual, and that as individuals age and have developed a level of adeptness to meet their needs, they will continue to navigate these structural levels of discrimination and oppression.
Those who reported their annual income was $18,000 or more were more likely to report greater trust in healthcare providers. Research on utilization of health services has shown that individuals who have a higher socioeconomic status or a higher household income are more likely to access healthcare. 33 Furthermore, greater income may provide some individuals with agency to choose their healthcare provider, which could enhance the potential to develop rapport and a long-standing relationship or switch providers until a suitable one is found. Lai and colleagues (2024) found that among young SMM, greater trust in physicians was more common among those who had no difficulty in paying for health services. 34 Among older SMM in this study, having a higher income along with health insurance coverage potentially provides the opportunity for one to engage with a healthcare provider who gains their trust. To adequately assess the role of income in healthcare, research should aim to address what types of healthcare related behaviors do individuals partake in depending on income levels and ways that HCPs can be trained to provide equitable care regardless of income and/or discuss cost saving options.
In this study, SMM living with any number of noncommunicable health conditions were more likely to report greater healthcare provider trust. This may have arisen as most participants were recruited from the MWCCS, a large, longitudinal study following the health and well-being of people living with and without HIV. Loeb and colleagues (2025) found that older gay men found it easier to seek out healthcare when looking for a provider specializing in their healthcare needs, such as HIV prevention and treatment. Some individuals who are living with HIV and/or managing other health conditions can be consistent with their healthcare and frequently interact with providers thus leading to a higher level of trust.
In addition to the above correlates of healthcare provider trust, another significant finding of our study was that trust was inversely associated with healthcare avoidance. This finding is consistent with other studies demonstrating that mistrust is associated with healthcare avoidance in rural populations, 35 older-age people,20,36 and willingness to use mental health services among Black people. 37 Our findings add to this literature by showing that having a higher healthcare provider trust reduces the likelihood of avoiding healthcare for some older, mostly White SMM. Developing and maintaining trust with patients is a key factor that can lead to consistent positive health outcomes. Prior work has shown that a critical part of patient-provider trust and the patient-provider relationship overall is engagement in shared-decision making.38-42 A strategy that providers can implement to strengthen trust is including patients in the decision-making process. Patients who feel their providers care about their concerns, answer their questions, and are receptive to information provided to them are more likely to trust their provider, develop a long-standing relationship with them, and feel the most comfortable when having to interact with their healthcare provider.1,43,44
Furthermore, our findings along with prior work highlight the need to understand the association between provider trust and healthcare avoidance from an intersectional perspective as well. Future work should be aimed at how provider trust and healthcare avoidance are associated for individuals who experience intersecting levels of oppression and stigma. The implications from this work would allow healthcare interventions and policies, particularly at the structural level, to be developed that can adequately address the needs of a diverse population.
While age was not a predictor of healthcare provider trust, it was associated with healthcare avoidance. Those in the 65-75 years old group had a lower likelihood of avoiding healthcare in the last 12 months. Romanelli and colleagues (2024) found that when measuring health care access among mainly White midlife to older LGBTQ adults, individuals who were men and aged 66+ reported higher healthcare access scores. 45 It is possible that for some LGBTQ adults, the ability to access and utilize healthcare is not an issue. Also, more than half of the participants in this study are living with HIV and/or other chronic conditions which might be preventing them from avoiding healthcare.
Lastly, we did find some study site differences in respect to healthcare provider trust and healthcare avoidance. Compared to participants at the Miami, FL site, those at the Birmingham, AL site were more likely to report having lower healthcare provider trust yet had lower odds of having avoided healthcare in the last 12 months. A similar outcome was found for participants at the Baltimore, MD/Washington, D.C. site with those participants having lower odds of avoiding healthcare in the last 12 months compared to the Miami, FL site. Some potential explanations for these differences could be due to: 1) the location of the MACS/WIHS clinics, 2) many of the participants that are enrolled in the MACS/WIHS also seek and access health services at other places, and 3) the avoidance of healthcare in the last 12 months could have been for any health service, not just HIV care or primary care.
Limitations
The data utilized for this study was specificized to SMM aged 35+, limiting the assessment of HCPT in younger SMM and others within the larger SGM population. To date, the HCPT scale has not been utilized with individuals in the SGM population, thus we are unable to compare the scores of these participants to prior work. The MACS/WIHS Combined Cohort Study collects data from specific geographic locations which limit our ability to state these findings are generalizable to all sexual minority men. This sample is not racially and ethnically diverse to investigate additional demographic differences that are present as it pertains to HCPT and accessing healthcare. Additionally, this data comes from a larger project 24 that aims to assess the full scope of these issues from an intersectional lens. Furthermore, the healthcare avoidance question only inquired about avoiding health within the last 12 months and some participants may have had experiences of healthcare avoidance longer than 12 months ago. We did not assess the reasons for avoiding healthcare given that only 12% of participants had reported avoiding healthcare in the last 12 months. The income variable is limited given that we did not have household size for participants.
Conclusion
The outcomes from this study highlight the association between sociodemographic and health factors on trust in healthcare providers. While factors such as racism were negatively associated with healthcare provider trust, income and managing non-communicable health conditions positively affected healthcare provider trust. Findings also illustrated the positive relationship between healthcare provider trust and the utilization of health services. However, this work further highlights the continued racial inequities that exist in relation to engaging in the healthcare system. Interventions aimed at addressing these inequities should focus on developing mechanisms that can improve how healthcare providers are trained to provide equitable and trustworthy care. Prior work has shown that healthcare provider trust has been associated with patient’s adherence to treatment plans, utilization of health services, and satisfaction with care. The current work demonstrates how for sexual minority men, healthcare provider trust is associated with several sociodemographic and systemic factors. This study provides evidence that for sexual minority men, past-year healthcare avoidance is inversely associated with healthcare provider trust and age. Further research is needed to explore how healthcare provider trust may change overtime for sexual minority men. From a health promotion perspective, these findings elucidate the role that healthcare provider trust can have on one’s access of health services. Health promotion strategies should focus on healthcare providers developing practices that are aimed at building a high level of trust with their patients.So What?
What is Already Known on This Topic?
What Does This Article Add?
What are the Implications for Health Promotion Practice or Research?
Footnotes
Acknowledgements
Data in this manuscript were collected by the MACS/WIHS Combined Cohort Study (MWCCS). The contents of this publication are solely the responsibility of the authors and do not represent the official views of the National Institutes of Health (NIH). MWCCS (Principal Investigators): Atlanta CRS (Cecile Lahiri, Anandi Sheth, and Gina Wingood), U01-HL146241; Baltimore CRS (Todd Brown and Joseph Margolick), U01-HL146201; Bronx CRS (David Hanna and Anjali Sharma), U01-HL146204; Brooklyn CRS (Deborah Gustafson and Tracey Wilson), U01-HL146202; Data Analysis and Coordination Center (Gypsyamber D’Souza, Stephen Gange and Elizabeth Topper), U01-HL146193; Chicago-Cook County CRS (Mardge Cohen, Audrey French, and Ryan Ross), U01-HL146245; Chicago-Northwestern CRS (Steven Wolinsky, Frank Palella, and Valentina Stosor), U01-HL146240; Northern California CRS (Bradley Aouizerat, Jennifer Price, and Phyllis Tien), U01-HL146242; Los Angeles CRS (Roger Detels and Matthew Mimiaga), U01-HL146333; Metropolitan Washington CRS (Seble Kassaye and Daniel Merenstein), U01-HL146205; Miami CRS (Maria Alcaide, Claudia Martinez, and Deborah Jones), U01-HL146203; Pittsburgh CRS (Jeremy Martinson and Charles Rinaldo), U01-HL146208; UAB-MS CRS (Mirjam-Colette Kempf, James B. Brock, and Emily Levitan), U01-HL146192; UNC CRS (M. Bradley Drummond and Michelle Floris-Moore), U01-HL146194. The MWCCS is funded primarily by the National Heart, Lung, and Blood Institute (NHLBI), with additional co-funding from the Eunice Kennedy Shriver National Institute of Child Health & Human Development (NICHD), National Institute on Aging (NIA), National Institute of Dental & Craniofacial Research (NIDCR), National Institute of Allergy and Infectious Diseases (NIAID), National Institute of Neurological Disorders and Stroke (NINDS), National Institute of Mental Health (NIMH), National Institute on Drug Abuse (NIDA), National Institute of Nursing Research (NINR), National Cancer Institute (NCI), National Institute on Alcohol Abuse and Alcoholism (NIAAA), National Institute on Deafness and Other Communication Disorders (NIDCD), National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), National Institute on Minority Health and Health Disparities (NIMHD), and in coordination and alignment with the research priorities of the National Institutes of Health, Office of AIDS Research (OAR). MWCCS data collection is also supported by UL1-TR000004 (UCSF CTSA), UL1-TR003098 (JHU ICTR), UL1-TR001881 (UCLA CTSI), P30-AI-050409 (Atlanta CFAR), P30-AI-073961 (Miami CFAR), P30-AI-050410 (UNC CFAR), P30-AI-027767 (UAB CFAR), P30-AI-124414 (ERC-CFAR), P30-MH-116867 (Miami CHARM), UL1-TR001409 (DC CTSA), KL2-TR001432 (DC CTSA), and TL1-TR001431 (DC CTSA). The authors gratefully acknowledge the contributions of the study participants and dedication of the staff at the MWCCS sites.
Ethical Considerations
Data for this study relies on a single IRB of record granted by Advarra (Advarra protocol number 00068335).
Consent to Participate
Participants were provided with written or verbal informed consent dependent on method of recruitment into the study.
Author Contributions
Conceptualization: M.S. (lead), M.P., M.R.F. Data curation: S.H., M.S. Formal analysis: M.S. (lead), M.R.F. Funding acquisition: M.R.F Methodology: M.S. (lead), M.R.F. Visualization: M.S. Writing – original draft: M.S. (lead), M.R.F. Writing – review and editing: All authors.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Heart, Lung, and Blood Institute (R01HL160326; PI: Mackey R. Friedman).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are not publicly available as data collection is still occurring for the larger, funded study.