
Abstract
Background:
Neonatal weight loss is universally recognized, yet poorly understood. Limited professional consensus exists on the definition of lower limit of safe weight loss.
Objective:
Our aim was to assess the extent of neonatal weight loss and its association with selected clinical variables in a population of healthy term infants cared for using a specific protocol on weight loss.
Methods:
We retrospectively considered 1003 infants consecutively admitted to the regular nursery of the Institute for Maternal and Child Health “Burlo Garofolo” (Trieste, Italy). We studied the relationship of selected variables with neonatal weight loss recorded during the hospital stay. We also analyzed all readmissions in the first month of life as a result of weight loss and its complications.
Results:
We observed a mean absolute weight loss of 228 g ± 83g, and a mean percent weight loss of 6.7% ± 2.2%. Weight loss ≥ 10% and > 12% were 6% and 0.3%, respectively. In multivariate logistic regression, cesarean section, hot season, any formula feeding, and jaundice not requiring phototherapy were independently associated with neonatal weight loss ≥ 8%. Conversely, low gestational age status was associated with lower weight loss. Readmission within the first month of life because of dehydration occurred in 0.3% of infants.
Conclusions:
Breastfeeding, compared to formula feeding, may not be a risk factor for greater early neonatal weight loss, at least in contexts in which weight is routinely monitored, breastfeeding is repeatedly assessed and appropriately supported, and careful supplementation is prescribed to limit and promptly treat excess weight loss and its related complications.
Well Established
It is widely recognized that most newborns will lose weight in the first days after birth. However, definitions of average normal weight loss and maximum safe weight loss are not yet well established.
Newly Expressed
In a context in which postnatal weight is routinely monitored, breastfeeding is assessed and supported, and supplementation cautiously prescribed, breastfeeding appears not to be associated with weight loss, which is instead associated with formula feeding, cesarean section, and jaundice.
Background
Neonatal weight loss is universally recognized, yet poorly understood. 1 Limited professional consensus exists on the definition of both the average normal weight loss and the lower limit of safe weight loss. This lack of consensus does not assist health workers in maternity wards in combining breastfeeding promotion with the prevention of weight loss complicated by hypernatremic dehydration.
In fact, dehydration and hyperbilirubinemia as well as their serious consequences (hypernatremic dehydration and kernicterus) are more common in breastfed infants, possibly as a result of inadequate breastfeeding.2,3 Consequently, health care services should adopt strategies to reduce the risk of severe complications in exclusively breastfed infants. As support and advice to the breastfeeding mother might not be enough, weight monitoring has been commonly used to indirectly assess the adequacy of feeding and the eventual need for supplementation of the breastfed infant with formula or expressed breast milk. 4
The aim of this study was to assess the extent of neonatal weight loss and its association with selected variables in a population of healthy term infants cared for using a specific protocol on weight loss. In our analyses, we adopted a birth weight loss of 8%, 5 although 10% is also commonly indicated by authoritative sources of the literature.6-9
Methods
In a retrospective cohort study, we reviewed hospital records of 1003 healthy term neonates consecutively admitted to the regular nursery of the Institute for Maternal and Child Health – IRCCS “Burlo Garofolo” (Trieste, Italy) from January 1-August 15, 2007. Our institute is a level 3 maternity hospital with 1850 deliveries per year and a well-established practice of rooming-in since the late 1970s. We analyzed clinical records regarding readmissions within the first month of life resulting from weight loss and its complications. We explored the relationship of common clinical variables with neonatal weight loss recorded during the hospital stay. Variables studied were: type of feeding (breastfeeding versus formula feeding), season (cold season from January-March; mid-season, April and May; hot season from June-August), type of delivery (vaginal vs cesarean section [CS]), birth weight, jaundice treated and not treated with phototherapy, length of hospital stay, hypernatremia (> 150 mEq/L), and hypoglycemia (blood glucose < 45 mg/dL). With regard to weight, we considered: (a) weight at birth, (b) weight at hospital discharge, and (c) maximum weight loss (both in absolute and percentage terms) reached at any time during the hospital stay. Every day between 8-10 AM, all infants were weighed naked, with an electronic scale, by a nurse, regardless of the feeding pattern.
According to the WHO definition, 10 we initially classified feeding practices into exclusive breastfeeding (EBF), predominant breastfeeding (PBF), complementary feeding (CF), and no breastfeeding (NBF). For the analysis, however, we combined EBF and PBF into breastfeeding (BF) and CF and NBF into formula feeding (FF). The feeding status of newborn infants was routinely categorized by the neonatologist at the discharge visit based on a review of the medical records from birth through hospital discharge.
In our population, mainly composed of Caucasians, we defined jaundice as obvious yellow color of the skin detected by nurses and/or pediatricians, followed by a test of bilirubin serum level. Jaundice was then defined as clinically relevant if serum bilirubin concentrations were high enough to require phototherapy, according to the 2004 American Academy of Pediatrics graphs. 11 In all infants with a weight loss > 10% or with a weight loss between 8%-10% and “not looking well,” we measured serum sodium concentrations. Hypernatremia was defined as serum sodium concentration > 150 mEq/L. Blood glucose was checked only if clinical signs and/or risk factors were present (birthweight < 10th percentile, infants of mothers with diabetes). In infants at risk of hypoglycemia, blood glucose tests were carried out at 1, 6, and 12 hours of life. Neonatal hypoglycemia was defined as serum glucose level < 45 mg/dL, regardless of gestational age and postnatal age. A neonate was considered as small for gestational age (SGA) if she/he was below the 10th percentile based on our reference curves. 12
Neonatal Weight Loss Protocol
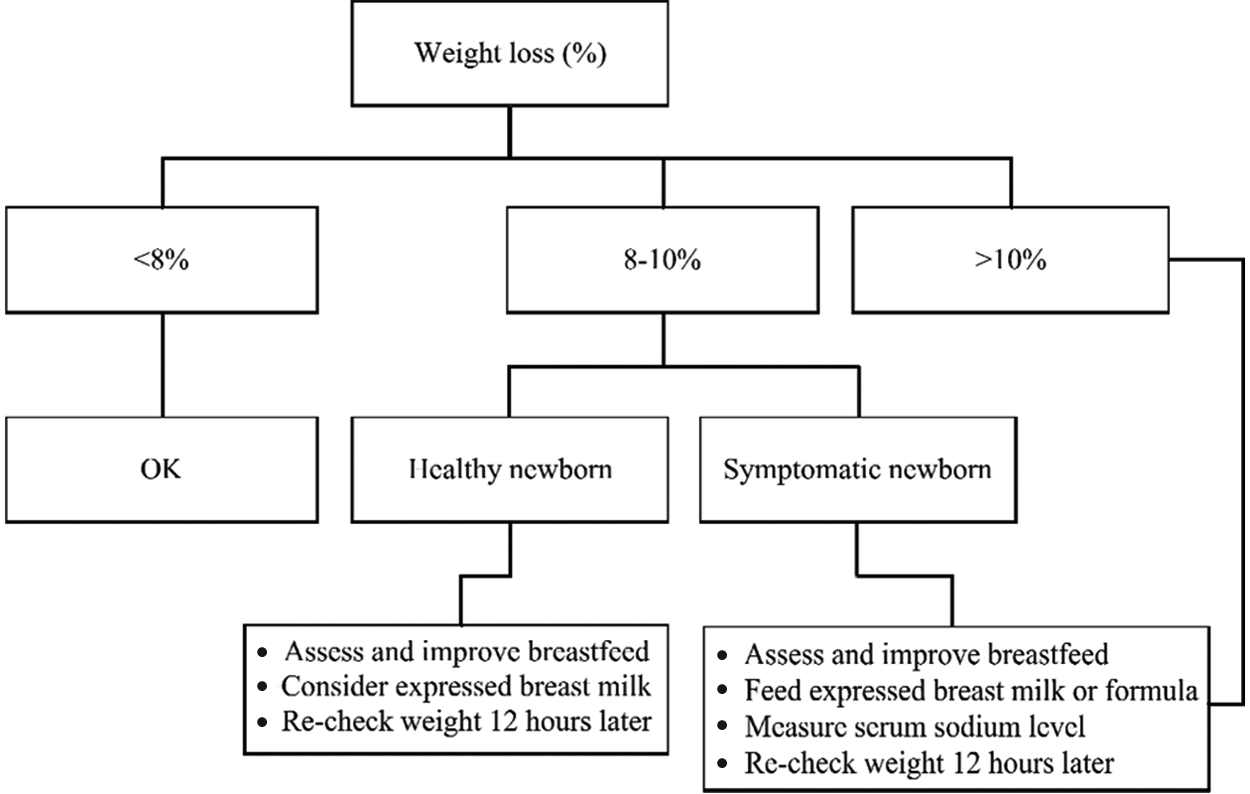
In order to monitor neonatal weight loss in the first days of life, a specific protocol has been applied since 2004 to all neonates during hospitalization (Figure). This protocol suggests different interventions according to: (a) the percentage of weight loss; (b) the infant’s physical examination; and (c) evaluation of breastfeeding, including the onset of lactation (lactogenesis II).
Clinical Management According to the Extent of Neonatal Weight Loss
Thus, in the assessment of weight loss and to identify appropriate interventions, we considered the following:
Effective breastfeeding: All breastfeeding mother-infant pairs were evaluated (primarily by nurses) during hospitalization, in order to promptly identify problems and intervene. First, nurses evaluated possible maternal problems and capability to respond to the infant feeding demands. Second, the following items were assessed: achievement of lactogenesis II (the onset of copious milk volume), breast and nipple morphology before and after a feed, latch-on, and newborn and mother position during breastfeeding sessions.
Weight loss >– 8%: Eight percent has been indicated by Livingstone and colleagues as the safest upper limit, excluding concurrent hypernatremic dehydration, as infants losing < 8% usually have natremia ≤ 145 mEq/L. 5 During the hospital stay, all infants were weighed at least once daily. On any given day, when clinically indicated, a second weight check was performed and recorded. If neonatal weight loss was ≥ 8%, extra support during the feeds was provided and special attention was paid to assess the oral cavity (palate, tongue tie) and ability to suckle. Serum sodium concentration was measured in infants with (1) a weight loss ≥ 10 % and (2) an 8%-10% weight loss with either clinical signs of dehydration or “not looking well.” Such infants were given supplemental feeds of expressed breast milk and/or formula, and weight was reassessed after 12 hours.
Discharge and Follow-up Policy
Healthy infants were routinely discharged from the hospital at a postnatal age ≥ 36 hours, according to the recommendations of the American Academy of Pediatrics.13,14 Babies with a neonatal weight loss > 10% were not considered for discharge until they regained enough weight to fall below 10% weight loss. A weight check of discharged infants was scheduled within 2-4 days after discharge, 15 and was carried out either at the hospital outpatient clinic by a registered nurse or at the health districts of the Trieste province, by a midwife. A hospital-based post-discharge weight check was scheduled for some infants depending on: (a) extent of in-hospital weight loss, (b) uncertainty of breastfeeding, and (c) need for jaundice reassessment.
Statistical Analysis
Continuous data were reported as means and standard deviations if normally distributed (according to the skewness and kurtosis joint test) or as medians and interquartile ranges if not distributed normally. Weight loss was analyzed as both a continuous and a dichotomous variable (≥ 8% or < 8%). Bivariate relations were evaluated by the t test, Mann-Whitney nonparametric test, or χ2 test, depending on the nature of the variables. Multivariate logistic regression was used to study the association between weight loss ≥ 8% (outcome) and all covariates. In the saturated model, variables associated with the outcome of P >.1 were excluded from the final regression model. Results are presented as adjusted odds ratios (OR). All data management and analyses were done using the SPSS package, version 11.5 (SPSS Inc. Chicago, IL, USA. 2002), and Stata/IC, version 11.2 for Windows (StataCorp LP. College Station, TX, USA. 2009).
Results
Demographic and selected clinical data of our study population are summarized in Table 1.
General Features of the Study Population (N = 1003)
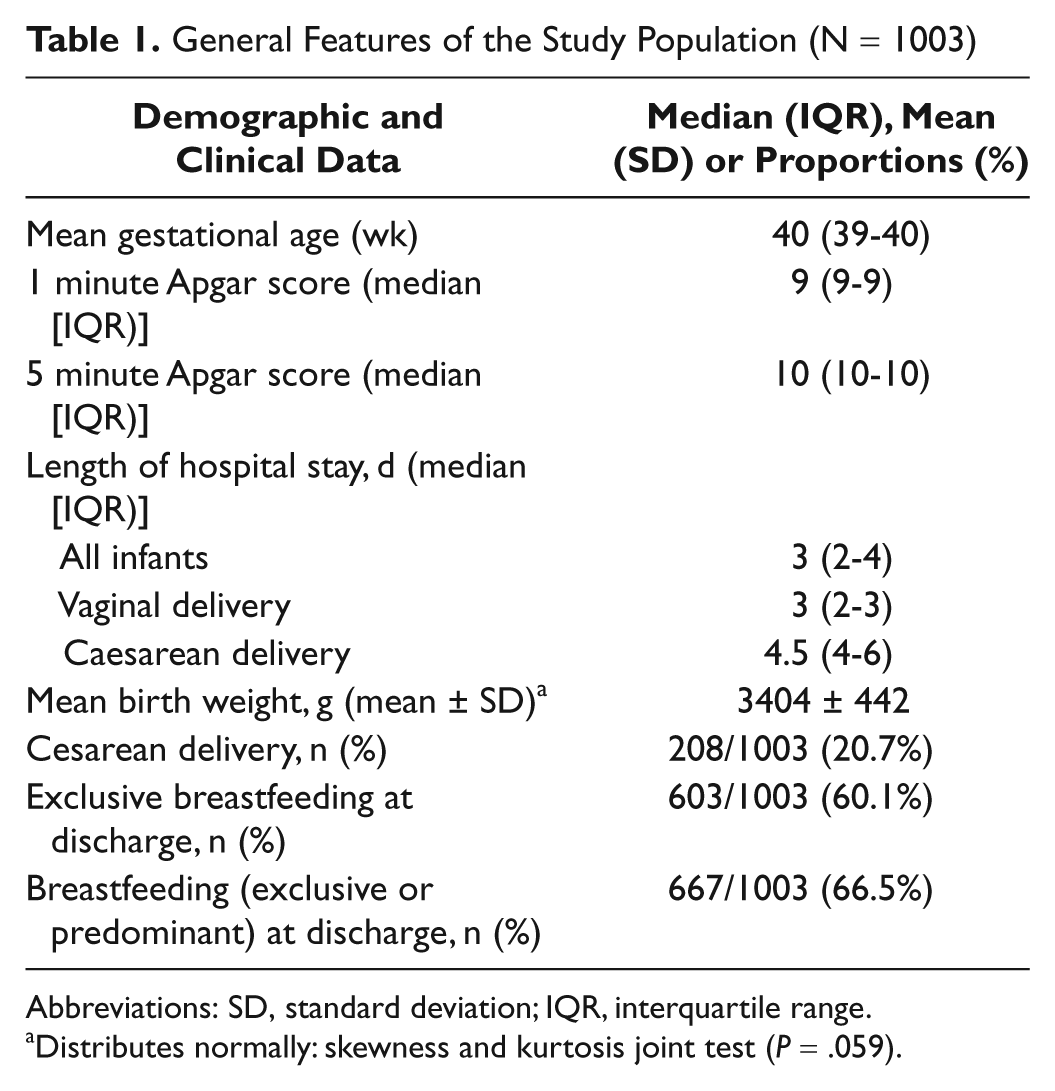
Abbreviations: SD, standard deviation; IQR, interquartile range.
Distributes normally: skewness and kurtosis joint test (P = .059).
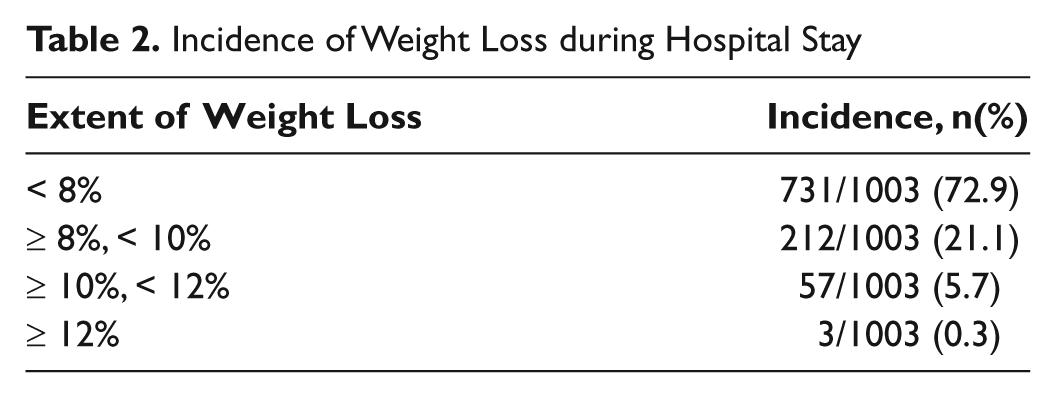
Weight loss distributed normally (joint skewness/kurtosis test for normality: P = .8). We observed a mean weight loss of 228 ± 83 g, with a mean percentage weight loss of 6.7% ± 2.2%. In our population, the rates of weight loss between 10% and 12% and ≥ 12% were 6% and 0.3%, respectively (Table 2). During the hospital stay, weight loss ranged between 0%-13.2%.
Incidence of Weight Loss during Hospital Stay
Mean weight loss was significantly higher in FF infants (255 ± 93 g or 7.5% ± 2.4%) if compared with BF infants (215 ± 73 g or 6.3% ± 2.0%; P < .001). During the cold months, the incidence of weight loss ≥ 8% was significantly lower than in the hot months: 23% (88/383) versus 32% (110/347; P = .008). In the midseason, such incidence was not significantly different than in the cold season: 27% (74/273; P = .23). Cesarean section was associated with a higher neonatal weight loss if compared with vaginal delivery: 254 ± 89 g (or 7.6% ± 2.2%) versus 222 ± 80 g (or 6.4% ± 2.1%; P < .001). A weight loss ≥ 8% affected 23% of infants delivered vaginally versus 45% of those born by CS (P < .001).
With regard to jaundice, 59 infants needed phototherapy (5.9% of the total sample). The mean bilirubin serum concentration of jaundiced infants requiring phototherapy was 16.9 mg/dL. Upon bivariate analysis, no difference in weight loss ≥ 8% was found between jaundiced infants requiring or not requiring phototherapy (32% vs 38%; P = .4).
Fifty-one out of 1003 (5%) infants were SGA. Weight loss ≥ 8% was reported in 12% of SGA infants versus 28% of non-SGA infants (P = .01).
In our infants, high serum sodium concentration before hospital discharge was a rare event: serum Na levels > 145 mEq/L were reported in 60/1003 infants (6%), but only 2 had serum Na levels > 150 mEq/L, and none had a serum Na concentration > 155 mEq/L. All cases of hypernatremia occurred in infants with a weight loss ≥ 8%.
Blood glucose was measured in 268 infants (26.7%). Hypoglycemia unrelated to weight loss, as it occurred before weight loss, was detected in 40 babies (4% of the population) in the first 24 hours of life: 38 infants had moderate hypoglycemia (25-45 mg/dL), and 2 (0.2% of the population) had severe hypoglycemia (< 25 mg/dL). Thirty out of 40 (75%) hypoglycemic infants had a weight loss < 8%, 9 had a weight loss of 8%-10% (22.5%), and 1 had a weight loss > 10% (2.5%). Weight loss distribution in hypoglycemic infants was almost identical to the distribution in the general population.
Re-hospitalization within the first month of life occurred in 2.7% of infants (27/1003). Seventeen out of 27 (1.7% of the whole population) were admitted for jaundice requiring phototherapy; the remaining 10 (1% of the whole population) were admitted because of excessive weight loss with dehydration, but only 3 presented with hypernatremia. The highest serum Na concentration found was 156 mEq/L.
In multivariate logistic regression, 5 variables were independently associated with neonatal weight loss ≥ 8% before discharge: (1) delivery by CS versus vaginal; (2) hot season versus cold season; (3) any FF versus EBF or PBF; (4) jaundice not requiring phototherapy versus no jaundice; and (5) appropriate and large for gestational age versus SGA (Table 3). Hypernatremia was not included in the multivariate logistic regression, as the hypernatremic infants were all in the weight loss ≥ 8% group. Sex of the child, hypoglycemia, birth weight, and gestational age were not included in the final multivariate analysis, as they were associated with weight loss ≥ 8% with a P > .1.
Multivariate Analysis of Factors Possibly Influencing Neonatal Weight Loss (N = 1003)
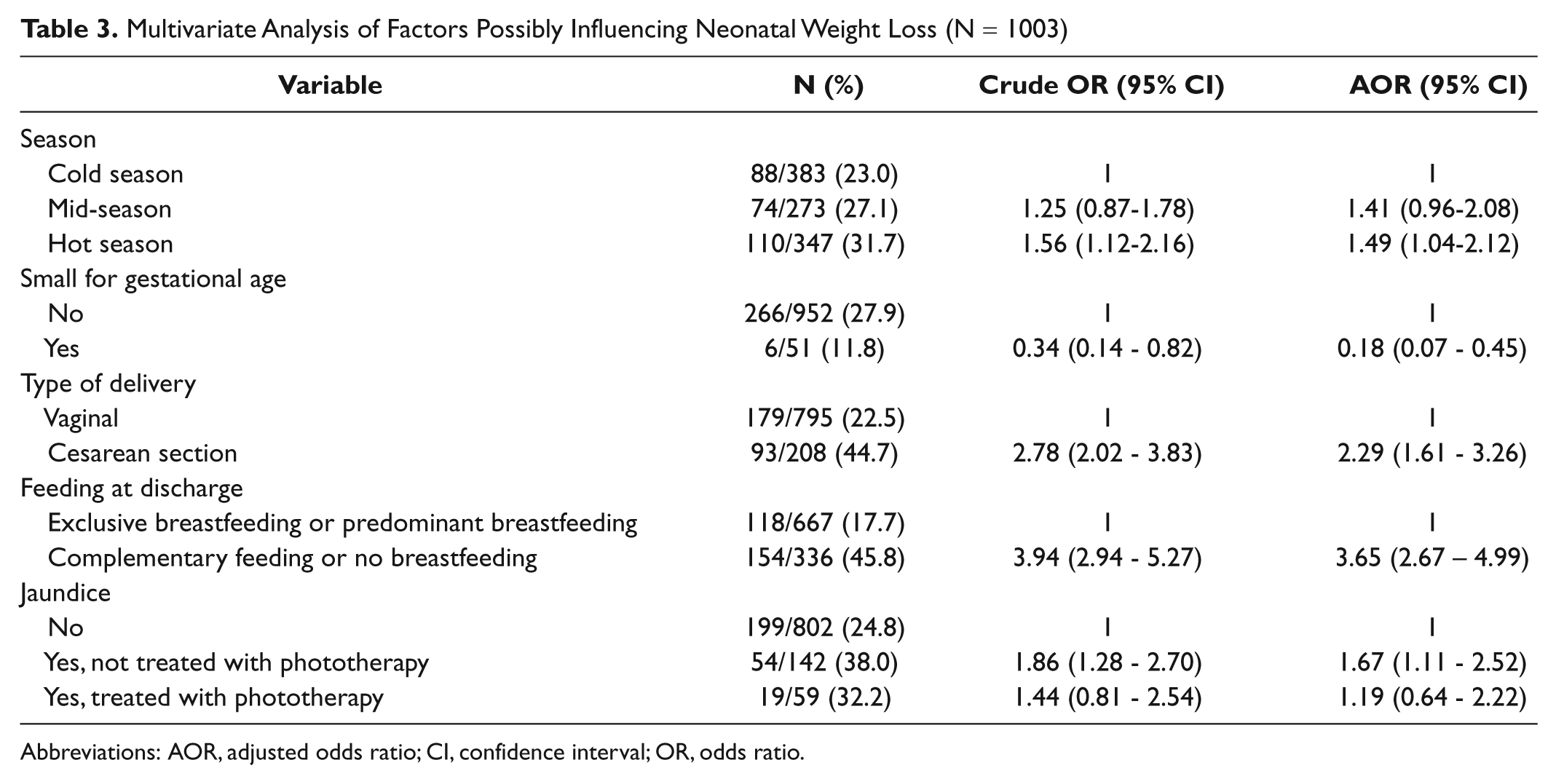
Abbreviations: AOR, adjusted odds ratio; CI, confidence interval; OR, odds ratio.
Considering the possibility that CS caused infants to lose weight and, for this reason, infants were changed to FF, we carried out a multivariate logistic regression with the same variables as in Table 3, but restricting only to vaginal deliveries. Results are presented in Table 4. There is no relevant change in the adjusted ORs and in the confidence intervals with respect to Table 3.
Multivariate Analysis of Factors Possibly Influencing Neonatal Weight Loss, Restricted to Vaginal Deliveries (n = 795)
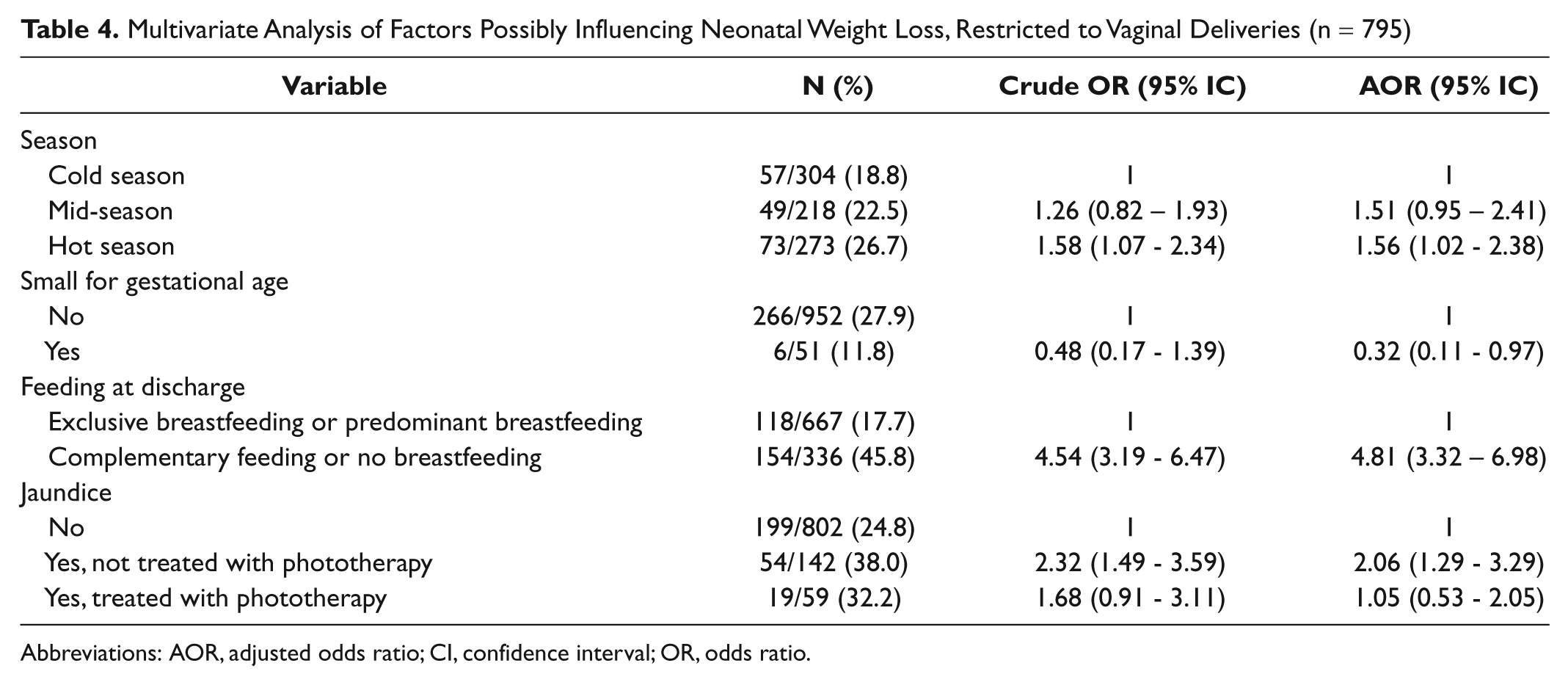
Abbreviations: AOR, adjusted odds ratio; CI, confidence interval; OR, odds ratio.
Discussion
Our data suggest that breastfeeding could be associated with a weight loss lower than that reported for formula-fed newborns, contradicting a concept widely accepted by health care staff experience and knowledge.16-23 In our infant population weight loss in the FF was higher than in the BF group (7.5% vs 6.3%). All16-23 but one 24 previous study documented higher mean weight loss in breastfed than in formula-fed infants (Table 5). In such studies, mean neonatal weight loss in breastfed infants ranged from 5.5%-7.4% and in formula-fed infants, from 2.4%-4.9%.16,21 This variability may be the consequence of different feeding protocols and practices. Considering that exclusively breastfed babies depend on the volume of breast milk after lactogenesis II and may lose more weight during the first days after birth, the association between weight loss and FF is probably because infants with greater weight loss are more likely to receive formula supplements.
Neonatal Weight Loss: Data from the Literature
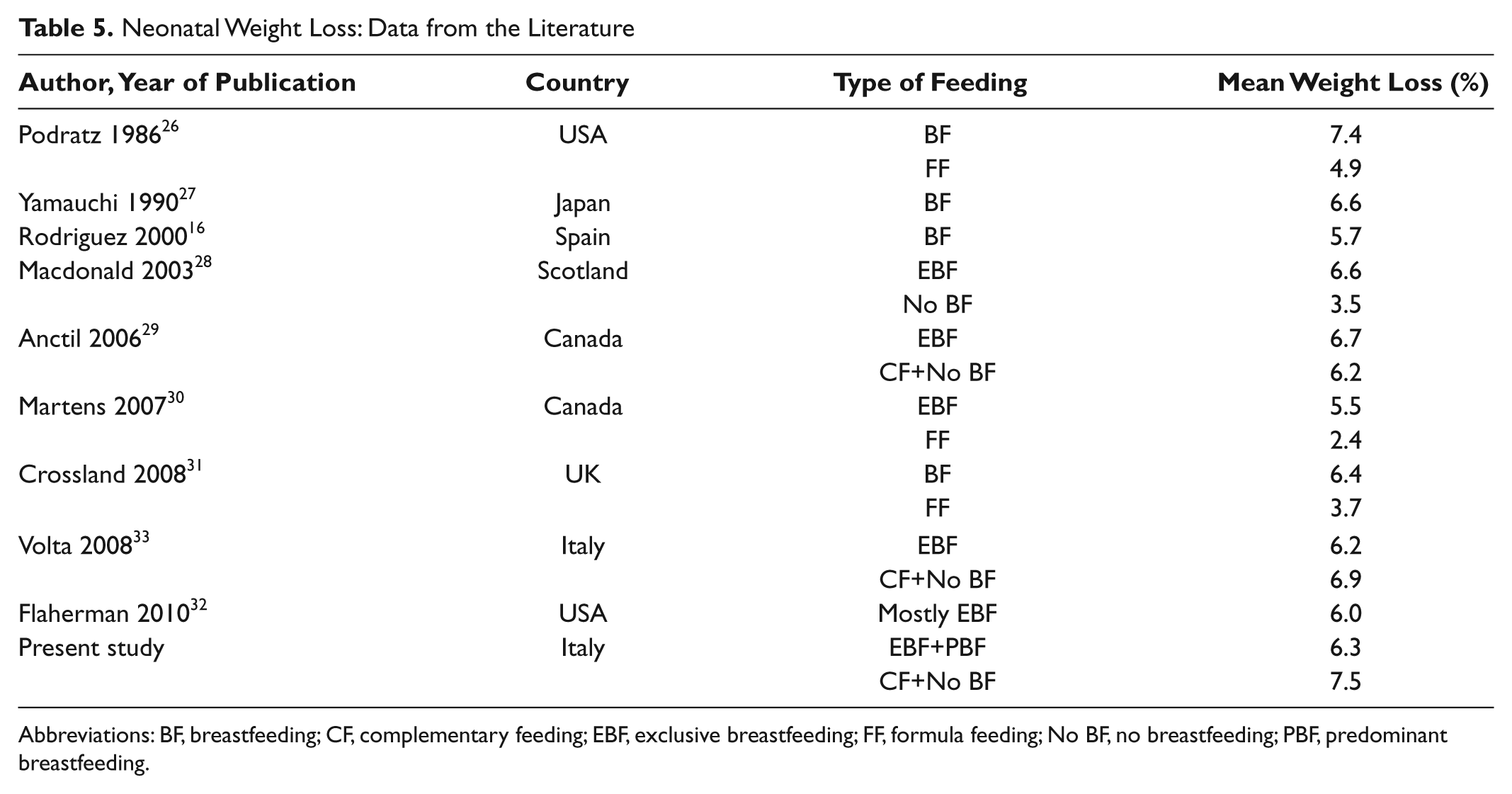
Abbreviations: BF, breastfeeding; CF, complementary feeding; EBF, exclusive breastfeeding; FF, formula feeding; No BF, no breastfeeding; PBF, predominant breastfeeding.
It is surprising that the documentation of a phenomenon that affects the entire human population is relatively limited in the scientific literature. The weight loss observed in the early days after childbirth depends on changes in body composition, mainly a loss of total body water and fat in a proportion of weight loss of approximately 80% and 20%, respectively.18,25 As recently demonstrated, greater weight loss after birth could also result from positive maternal intrapartum fluid balance and fetal volume expansion. 26 We found a mean percentage neonatal weight loss of 6.7% and an association of increased weight loss with non-SGA status, FF, CS, hot season, and jaundice.
In our infants, being SGA seemed to be a protective factor against weight loss. This association may simply be explained by greater attention paid, by health professionals and mothers, to the feeding of this category of neonates, deemed at increased risk of hypoglycemia.27,28 Our results are probably a result of a more liberal policy in breast milk substitutes applied to SGA infants. Limited scientific literature specifically addresses the relationship between weight/age ratio and neonatal weight loss. 29
In agreement with other authors,30,31 we demonstrated that neonatal weight loss, apart from diet, is associated with type of delivery. Suboptimal feeding after CS may lead to greater weight loss. In fact, despite efforts to promote a “natural” CS 32 and a specific breastfeeding education program, 33 CS still adversely affects both initiation34-36 and duration of breastfeeding,34,37 especially after an emergency procedure. 38 Lower breastfeeding rates may be a result of maternal impairments after surgery. Additional factors involved may be limited effective compensatory aid by health professionals and delay in feeding after birth. 39 The latter is independently associated with breastfeeding failure. 40
Our study also shows that in the hot season, infants tend to lose more weight. Our maternity ward is provided with air conditioning; nevertheless, some mothers prefer to switch it off. We did not record data on the hydration status of mothers in the maternity ward, and therefore we cannot infer that greater weight loss in the hot season is associated with a poorer maternal hydration status. Although supported by common sense, our finding is not in agreement with the scientific literature.41,42 In his review paper, Sachdev documented that, based on breast milk intakes, urine output, and urinary specific gravity or osmolarity, breastfed infants do not need fluid supplementation. 43 However, this finding does not imply that weight loss should be identical in the hot and in the cold seasons, as long as weight loss remains within “normal,” acceptable limits.
In accordance with previous studies, our data show that jaundiced infants lose more weight than non-jaundiced infants.44-46 However, need for phototherapy does not significantly alter weight loss, possibly because of a wider use of breast milk supplements. In our study, we found no significant difference in the proportion of weight loss ≥ 8% between those subjected to phototherapy (33%; 20/61) and not subjected (27%; 252/942; P = .30), even if this finding might be partially a result of the insufficient size of the sample. The hypothesis that jaundiced neonates might lose more weight secondarily to altered sucking behavior has been rejected by Alexander and Roberts, 47 as bilirubin levels showed no correlation with milk consumption. Although a recent report underlines that breastfed newborns have higher rates of significant hyperbilirubinemia, 48 there is sufficient consensus that jaundice does not appear to be associated with breastfeeding per se, but with increased weight loss in dehydrated breastfed newborns. 46
In the present study, we recorded the maximum neonatal weight loss measured during the hospital stay. We have documented that only a minority of neonates lose ≥ 10% birth weight. In clinical practice, some uncertainty exists concerning the definition of the upper limit of safe weight loss in neonates. According to main reference textbooks,6-9 an infant should not lose more than 7%-12% of birth weight. Ten percent is the most frequently cited upper normal percentage limit of neonatal weight loss. However, the reported percentage of infants with a weight loss > 10% varies considerably, ranging from less than 1% to 12%.49,50 These differences are likely to result from variables that are difficult to control, such as characteristics of the mother-baby dyad, breastfeeding management, hospital feeding protocols, and attitudes and skills of health care workers in maternity wards. Dewey reports that excessive weight loss is generally associated with suboptimal breastfeeding and is influenced by many factors such as primiparity, long duration of labor, use of medications, CS, neonatal conditions at birth, delayed onset of lactation, and infant feeding behavior on the first day of life. 50
Hospital-based as well as community-based health services of Trieste province recommend and support EBF for the first 6 months of life. In 2007, the rate of EBF at the average age of 17 weeks in Trieste province was 52%. 51
We believe that breastfeeding support prior to lactogenesis II and during the very first weeks of lactation, careful monitoring of infant weight loss, and following a strict weight loss protocol as part of the infant feeding policy led to low rates of: (a) weight loss ≥ 8% (27%) and in particular, ≥ 10% (6%); (b) hypernatremia before discharge (0.2%); and (c) admission for hypernatremia (0.3%).
Hypernatremia is the most feared complication of neonatal weight loss, and its incidence reported in the literature appears to be increasing as a consequence of the promotion of exclusive breastfeeding.52-56 Our data on readmissions for dehydration after discharge are in line with data available in the literature.57-60
Our study has obvious limitations. First, we studied a limited number of variables related to weight loss, which hinders the value of multivariate analysis. In particular, we did not control for relevant maternal factors, both clinical—such as body mass index 61 and intrapartum fluid balance 26 —and sociodemographic. Second, as this was a retrospective cohort study, we have not been able to establish direct causation between some of the variables considered and weight loss as outcome; that is, the decision to formula feed might be made after weight loss occurs, thereby generating a problem of reverse causality, with weight loss being the potential cause of FF and not vice versa. Third, regarding the use of a weight loss protocol, previous studies were designed as audit and re-audit studies following the implementation of guidelines.60,62,63 We did not make any comparison with a control group before and after the implementation of our neonatal weight loss protocol, and consequently we cannot attribute any proven clinical effectiveness to our protocol. Nevertheless, we evaluated some clinically meaningful neonatal outcomes and compared our results with those available in the scientific literature. In our study, hypernatremia (a serum Na level > 150 mEq/l) appeared to be a rare event both during the first days of life (0.2%) and after discharge (0.3%). Moreover, the rate of re-hospitalization for dehydration after birth appears to be rather low (1%). Finally, we realize Risk Ratios would be more appropriate than ORs for incidence measures such as weight loss ≥ 8%, which is not a rate outcome. However, both the problem of temporality already mentioned and the use of the logistic regression made us opt for reporting the ORs.
Conclusion
In conclusion, breastfeeding is not necessarily a risk factor for higher early neonatal weight loss, as previously documented in the scientific literature. The promotion and support of breastfeeding is compatible with other good neonatological practices, including postnatal monitoring, breastfeeding assessment, and careful formula supplementation.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The study was approved by the Research Commission of the IRCCS “Burlo Garofolo,” Trieste, and funded by the grant RC 18/09 of the same Institute.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.