
Abstract
Background:
Australia has high rates of breastfeeding initiation, with a consistent decline over the first year. Furthermore, there is a growing trend of maternal employment and rising numbers of children enrolled in different types of child care services, both of which can have a negative impact on breastfeeding.
Objectives:
To provide evidence to better inform implementation of breastfeeding-friendly strategies in child care settings, this study examined breastfeeding policy and practice in child care centers in metropolitan Adelaide.
Methods:
The paper reports on a survey sent to 292 child care centers in metropolitan Adelaide in 2010. The survey collected information on center location and type, number of enrolled children under age 2, and number of breastfed babies. The survey also included questions about breastfeeding facilities and support, breastfeeding policies, staff training, and barriers to and recommendations to enhance breastfeeding support in child care centers.
Results:
Of the 62 completed returned surveys (21% response rate), 43 centers (69.4%) reported that they currently have children who receive breast milk at the center; however, in most centers, the total number of breastfed children was reported to be between 1 and 4; 76% reported that the center was supportive of exclusive breastfeeding for 6 months; and 80.6% had statements on breastfeeding as part of their food and nutrition policies or guidelines. Furthermore, 64.5% reported there was no formal or informal training for staff on breastfeeding support, but 50% reported that staff members do provide breastfeeding advice to mothers of children in their center.
Conclusions:
Despite some strategies in place to support breastfeeding, there are no standards on breastfeeding policies, practices, and training in child care settings. Therefore, the extent and scope of such support depend on parental request and the perceptions and attitudes of child care center staff toward breastfeeding.
Well Established
Australia has a growing trend of maternal employment and rising numbers of children enrolled in different types of child care services. There is little evidence on the scope of breastfeeding support in child care settings in Australia.
Newly Expressed
Despite some strategies to support mothers, there are no standards on breastfeeding policies and practices in child care settings. This paper suggests that the lack of breastfeeding-specific policies, lack of staff training on breastfeeding, and factors external to child care that influence parents’ choice of infant feeding are key barriers that need to be addressed in order to move toward breastfeeding-friendly child care centers.
Background
Breastfeeding supports normal growth and development, and it has a positive impact on child health over the lifetime. Breastfeeding also contributes to the health of mothers and enhances the economic well-being of society.1-4 In Australia, breastfeeding practice lags behind the national and international recommendations. The Australian National Health and Medical Research Council recommends exclusive breastfeeding for 6 months and continued breastfeeding for at least 12 months. 5 The World Health Organization recommends 6 months of exclusive breastfeeding and continued breastfeeding to 2 years and beyond. 6 Although 96% of Australian mothers initiate breastfeeding, rates decline significantly, with only 15% exclusively breastfeeding to 5 months (less than 6 months), and around 60% and 18% of infants receive any breast milk at 6 and 13-18 months, respectively. 7 These figures show that although initiation rates of breastfeeding meet the Australian National Health and Medical Research Council dietary guideline, the targets of exclusive breastfeeding for 6 months and continued breastfeeding for at least 12 months are not being achieved, which suggests policy and practice could better support, promote, and protect breastfeeding. 8
There are several factors constraining the continuation of breastfeeding in the context of industrialized countries. Studies suggest that return to work and consequent separation from the baby are associated with lower rates of breastfeeding.9,10 In Australia, there is a growing trend for maternal employment, 11 and thus, a higher percentage of enrollment in child care services. 12 Between 1996 and 2005, the percentage of Australian children aged 0-5 enrolled in different types of child care services increased from 13% to 24%, and by 2008, 35%–50% of children aged 1-4 years were enrolled in child care centers.11,12 Of children under 1 year old, 6% were in long day care, that is services that operate at least 10 hours a day Monday-Friday (17,000 children), compared with 25% of 1-year-olds (74,000) and 41% of 2-year-olds (110,000). 12 Therefore, the provision of support for breastfeeding in child care settings seems vital in encouraging mothers to continue breastfeeding while working. The Australian National Breastfeeding Strategy also places an emphasis on breastfeeding-friendly environments, including child care and the workplace, to empower mothers to continue breastfeeding. 13
Although child care settings provide an important opportunity for breastfeeding promotion, there is little evidence on the scope of breastfeeding support in child care settings to inform policy development and resource allocation to move toward breastfeeding-friendly child care centers. 14 This study examined breastfeeding policy and practice support in child care centers in metropolitan Adelaide (the capital city of the state of South Australia, with a total population of 1.65 million) to provide evidence to better inform implementation of breastfeeding-friendly strategies in child care settings.
Methods
The study employed mixed methodology by gathering qualitative and quantitative data from child care centers. The study had 2 phases. In phase 1, face-to-face interviews were conducted with 15 child care center directors or child care workers. This phase collected information on policy support, breastfeeding practices, staff training on breastfeeding, and barriers to promoting breastfeeding. The results of phase 1 are published elsewhere. 15 The second phase consisted of a survey of all long day care centers in metropolitan Adelaide. This paper presents the findings of phase 2, the child care survey.
A list of Adelaide metropolitan child care centers was compiled from sources including the South Australian Department of Education, the National Childcare Accreditation Council, and the Community-based Childcare Centres Association, supplemented by a thorough search of the South Australian business telephone directory (Yellow Pages). Information collated included the name, telephone number, and postal and email address of each center. The initial list contained 315 child care centers. An online survey (using SurveyMonkey) was emailed to 241 centers for which an email address was available. Hard copies of the survey were posted to 74 centers whose email addresses were not available from online sources. An alert of “failure to deliver” was received for 28 center email addresses, so a hardcopy of the survey was sent to their street address. Of the 102 surveys posted, 23 were returned to sender because of an invalid address. The survey was therefore considered received by 292 child care centers in metropolitan Adelaide. Two reminders via email and post (at 2-week intervals) were sent to centers that did not respond to the initial invitation.
The questionnaire was developed based on the key themes and issues that emerged from the individual interviews in phase 1. The survey included questions under these domains: (a) breastfeeding facilities and support (eg, physical space, staff training on breastfeeding, and breastfeeding advice); (b) breastfeeding policies, including main policy areas, communication of policies with staff and parents, and policy review; (c) barriers to support breastfeeding; and (d) recommendations to enhance breastfeeding support. The questionnaire included yes/no questions as well as questions with the option to select multiple items that applied to their center. Comment boxes were placed after each question to allow participants to comment on specific issues not covered by the questions. The survey also collected information on child care center location and type (private, non-for-profit, community-based), number of children enrolled under 2 years old, and the number of children receiving breast milk in the center. The survey was composed of 26 questions.
Categorical survey responses were imported into SPSS (version 15.0, SPSS Inc, Chicago, Illinois, USA, 2006) and analyzed using descriptive statistics. The first author conducted the analysis, and all authors had access to and reviewed the data analysis. Open-text responses were imported into NVivo (version 9, QSR International, Melbourne, Australia, 2010) and analyzed thematically to identify and describe data in more detail. 16 The first and third authors independently coded the texts using the categories used in the questionnaire and linked the texts to the survey questions. The open-text responses were generally a further clarification of current practices. Nevertheless, the codes from 3 team members were discussed in project meetings until an agreement was reached.
The study received ethics approval by the Flinders University Social and Behavioural Human Research Ethics Committee.
Results
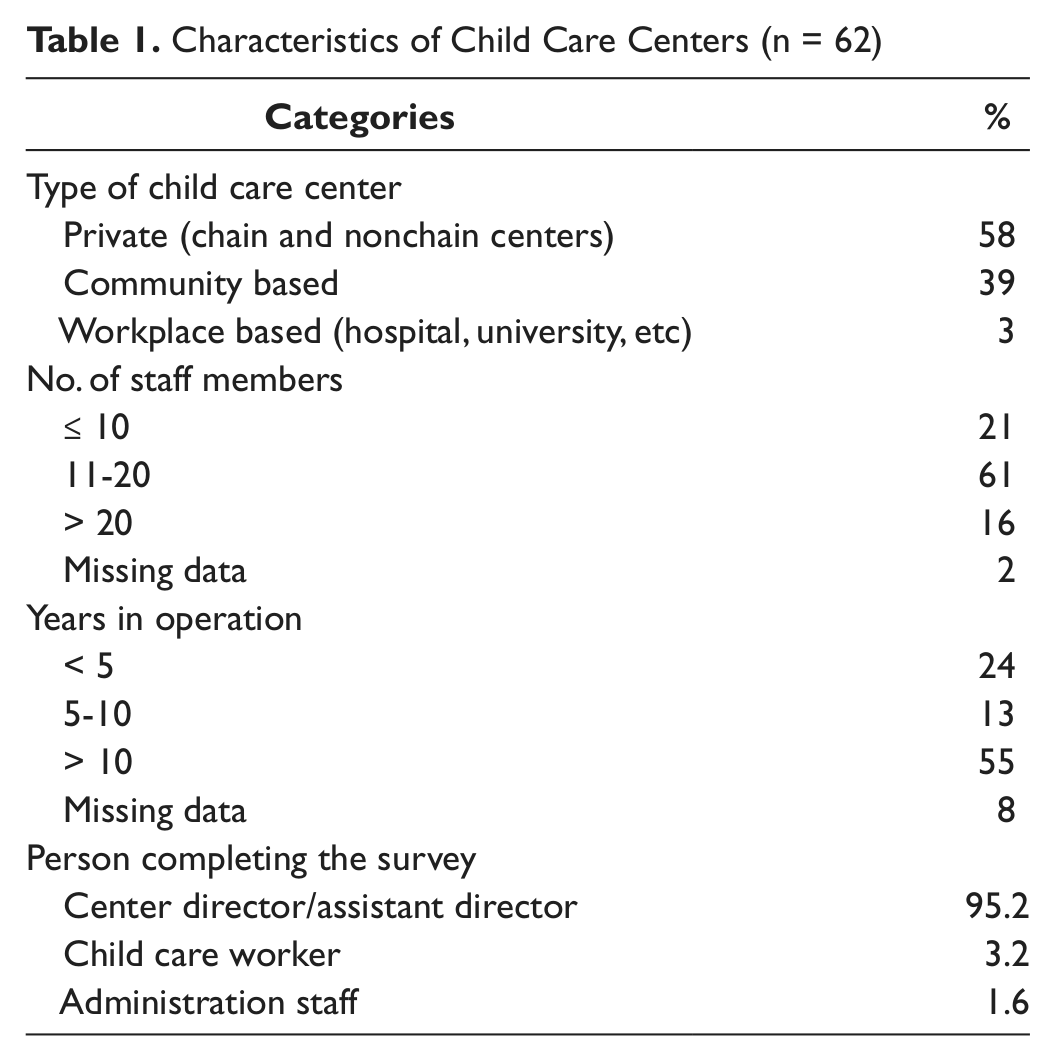
Of the total 292 child care centers that received the invitation to participate, 62 centers completed the survey (27 paper and 35 online), a response rate of 21.2%. Table 1 shows the characteristics of the centers that participated. Forty-three centers (69.4%) reported that they currently have children who receive breast milk, either as expressed breast milk in a bottle or cup, by mothers visiting the center to breastfeed, or a combination of both of these ways, although in most centers the total number of breastfed children was reported to be between 1 and 4. This number did not include children, particularly older babies and toddlers, who were breastfed only at home and so did not receive any breast milk at the center.
Characteristics of Child Care Centers (n = 62)
Survey results are reported in 5 key areas: (a) breastfeeding policies and policy areas; (b) breastfeeding support; (c) staff training and practice of breastfeeding support; (d) barriers to supporting breastfeeding; and (e) recommendations to improve breastfeeding support in child care settings.
Breastfeeding-Specific Policies
The majority of participating centers (50/62; 80.6%) reported having statements on breastfeeding as part of their food and nutrition policies or guidelines. Ten respondents reported having no policy statement regarding breastfeeding, and 2 did not answer the question. The main policy areas reported were storage and heating of expressed breast milk (75.8%), encouraging breastfeeding (62.9%), providing breastfeeding information and advice to parents (33.9%), and staff training on breastfeeding (11.3%).
In most centers, policies, including breastfeeding policies, have been reviewed and/or updated on a regular basis (64% at least once a year, 24.5% once in 1-5 years, and 11% had ongoing review). Seventy percent stated that breastfeeding-related policies are available to prospective parents or at child enrollment. More than 90% of child care centers had strategies in place to communicate new policies/policy changes with parents and staff; the vast majority used center newsletters, staff meetings, and flyers in child pockets and/or notice boards.
Breastfeeding Support
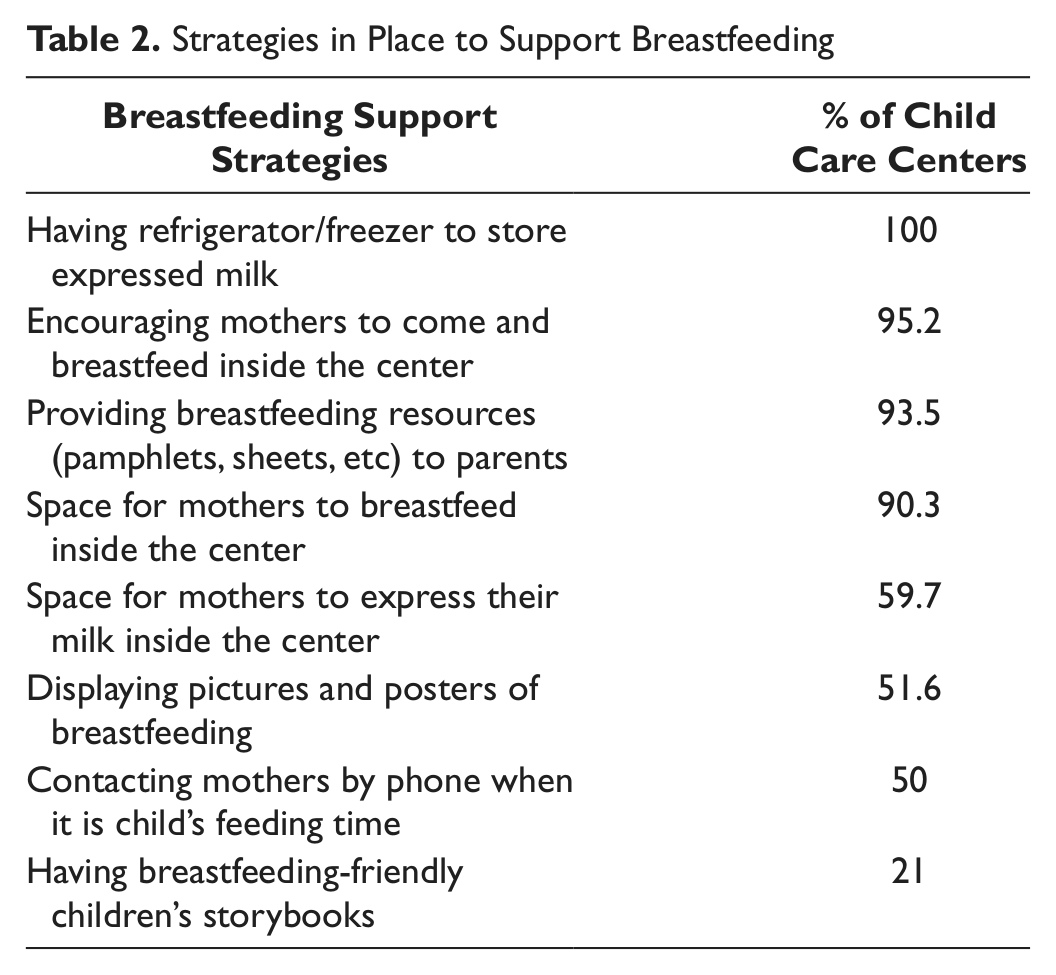
Of all centers participating in the survey, 76% reported that they are supportive of exclusive breastfeeding for 6 months. However, the importance of parents’ choice on infant feeding, and the role of child care centers in supporting parents’ choice (breast or formula feed), were key issues raised by a large number of centers. Low numbers of children under 6 months old who are enrolled in the center and early cessation of breastfeeding (before enrollment in child care) were issues frequently cited as main factors decreasing demand for breastfeeding support in child care settings. In the open-text responses, there was a sense of hesitation to promote breastfeeding as optimal, and respondents suggested that centers should strive to be impartial about infant nutrition and health promotion messages of “breast is best,” with the ethos to support parental choice and not impart judgment. Such responses included: “We promote it [breastfeeding] but do not judge our families on their choices”; “Mums are supported and respected of their choice to [breast] feed or use formula”; and “It is a parent’s choice. We give information on breastfeeding and bottle feeding.” However, the centers did report having strategies in place to support parents who chose to continue breastfeeding, for example by providing a physical space for mothers who wish to come and breastfeed in the center. Table 2 demonstrates the most common ways that breastfeeding was supported within the surveyed centers.
Strategies in Place to Support Breastfeeding
Staff Training and Practice of Breastfeeding Support
Although some centers (30%) provided staff training in breastfeeding support, most did not. Forty respondents (64.5%) reported that there was no formal or informal training on breastfeeding for current or new staff responsible for infant care to enable them to provide appropriate information and support to mothers to continue breastfeeding. This result links well with the finding that only 11.3% of centers included staff training on breastfeeding support in their policies. In response to this question, some respondents (30%) justified their responses, stating that many staff members have child care qualifications that include a component on breastfeeding support and many others have personal experience as a mother. There was a sense that advice was offered only by the trained staff, but all staff could provide pamphlets or refer to other community resources upon parental request. Such responses included: “Most staff have completed child care training, which briefly looks at breastfeeding, but no further training is done here”; “Staff have information but are not trained”; and “Written information is available if staff are interested in it.”
Although only 30% of centers provide staff training in breastfeeding support, 50% reported that their staff provides breastfeeding advice and support to mothers of children in the center if required. Open-text explanations of this issue included: “Staff who have [their own] children do talk to parents about breastfeeding, but it is informal, and we suggest they [parents] talk to their doctor,” and they do so “to the best of their ability” and “if requested.” Many responses related to the provision of a referral or pamphlets of relevant information available in the center. One respondent explained, “Sometimes they want advice re: balance of ‘bottle versus breast,’” which needs more knowledge of the area to provide appropriate advice.
Barriers to Breastfeeding Support
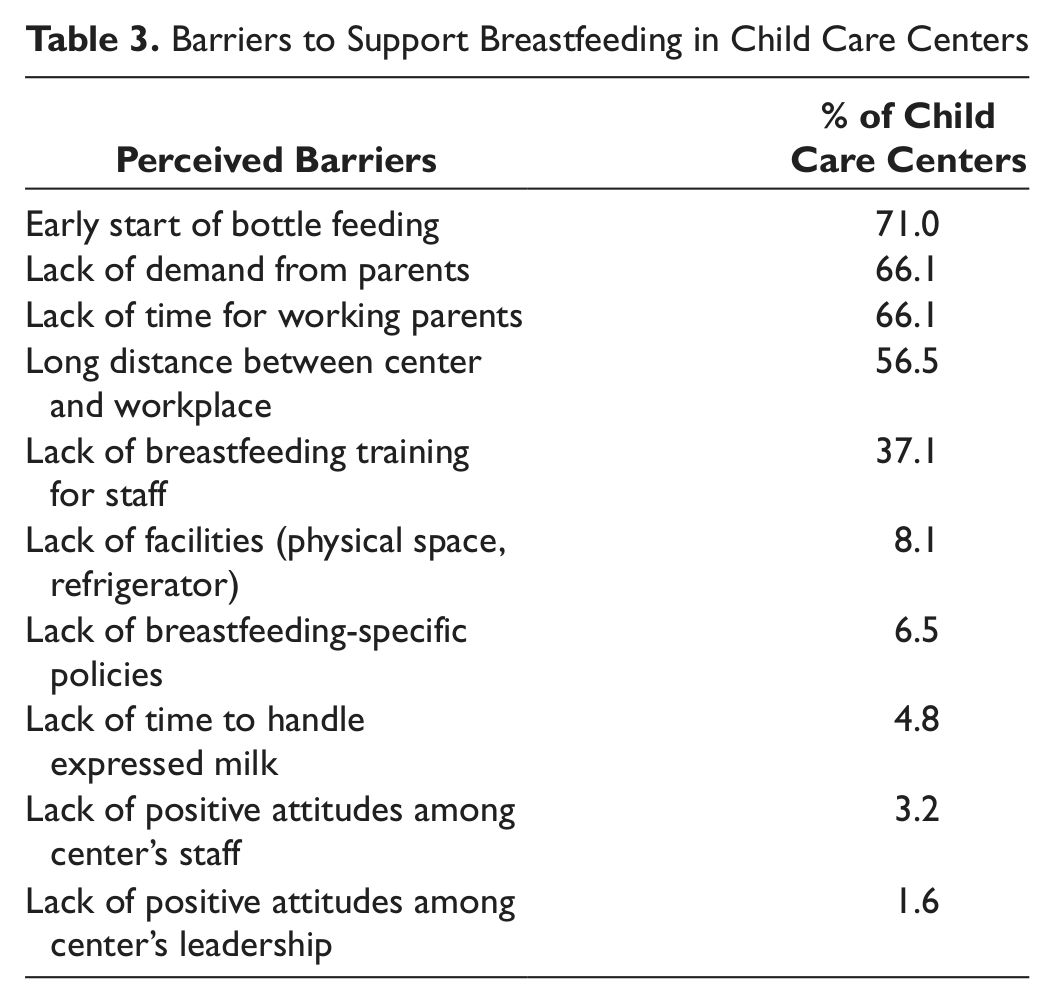
Table 3 demonstrates the most common barriers in child care centers to supporting breastfeeding that were identified in the survey. Most responses put a high priority on external factors that affect mothers’ decisions on infant feeding and in turn lead to poor demand for breastfeeding support in child care centers. The 2 primary areas of concern were related to societal support for breastfeeding and maternal employment. The limited breastfeeding support in child care centers was seen principally as a reflection of societal attitudes and workplace policies, rather than child care centers’ policies. For example, the lack of support from workplaces and long distance between workplace and child care was reported as a reason that mothers prefer formula or expressed breast milk in a bottle rather than coming to the center for breastfeeding. Lack of staff training for breastfeeding was also rated high as a barrier. Lack of facilities such as physical space, and procedural/technical factors of expressing and storing breast milk rated low as barriers.
Barriers to Support Breastfeeding in Child Care Centers
Recommendations to Improve Breastfeeding Support in Child Care Centers
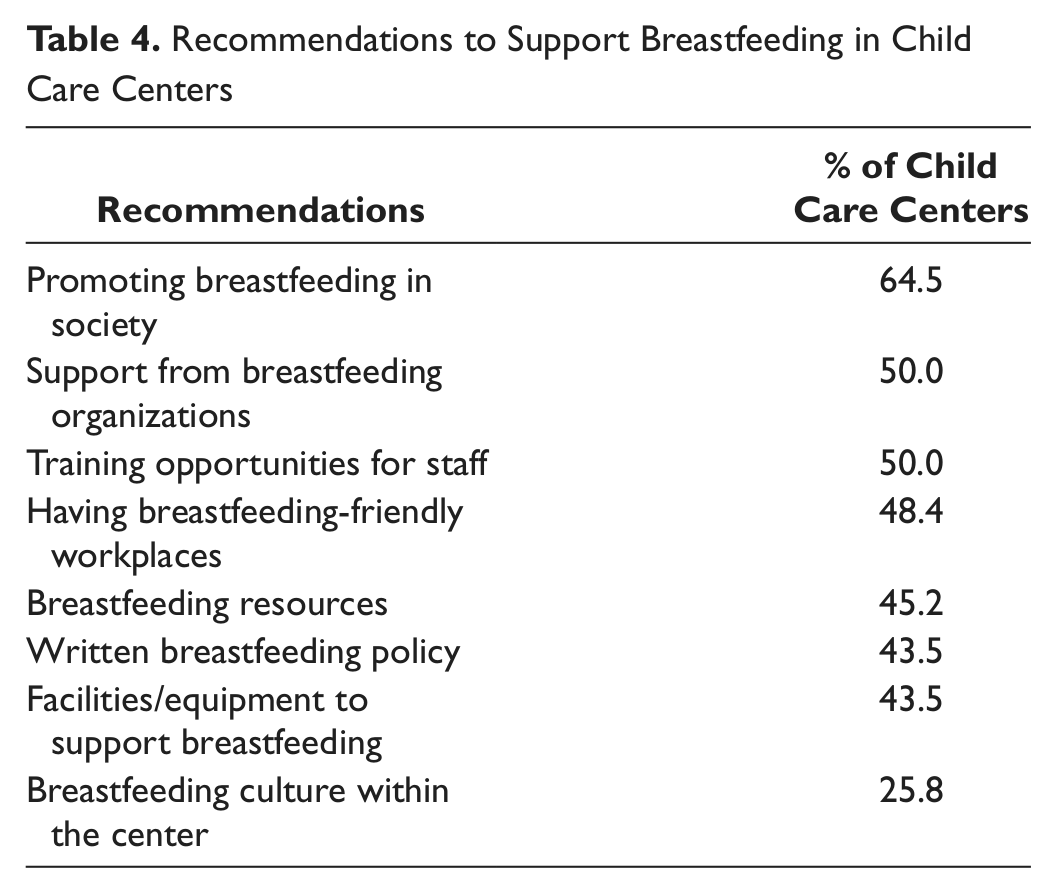
When asked about ways in which breastfeeding could be better supported in child care centers, most centers placed an emphasis on the role of public health interventions to improve breastfeeding culture in the whole of society. Table 4 shows the interventions that respondents felt would best support breastfeeding in child care centers. These responses reflect the belief that child care centers have no active role in breastfeeding promotion, but rather just followed parental requests. Almost 26% of centers reported that improving breastfeeding culture in the whole society is a useful strategy for improved breastfeeding practice in child care centers.
Recommendations to Support Breastfeeding in Child Care Centers
Although respondents described the sense of pressure that parents experience over feeding choice, they also commented on decreasing demand for breastfeeding in child care centers. This decreasing demand was attributed to 2 primary reasons; the first was the older age of children entering child care (most often over 6 months), and the practice of combined formula and breastfeeding whereby women provide formula for child care and breastfeed when at home. Many responses were made about combined formula and breastfeeding, such as: “Some parents are still breastfeeding but only after care, they will give the child a [breast]feed before they leave [home]and when they get back [home],” and “We have 5 parents who breastfeed exclusively at home and never at Center (ie, AM and PM feed).”
Discussion
The findings of the survey reported in this paper are consistent with those of phase 1 of the research, 15 which involved in-depth interviews with center directors or child care workers. Although we acknowledge that the survey was developed from the findings of phase 1, this study adds further evidence and complements the previous findings from a broader cohort of child care centers in the same geographical area. This survey has further highlighted that few child care centers have a written policy specific to breastfeeding, but rather they subsume breastfeeding within broader policies on nutrition and safe handling of expressed breast milk.
The majority of participating centers reported that they were supportive of breastfeeding, and they provided for storage of breast milk, space for mothers to breastfeed or express, and resources such as pamphlets and posters promoting breastfeeding. However, it is interesting to note the free-text comments that the demand from mothers to practice breastfeeding while their child is in care is reduced. Many open-text responses reported that mothers choose to feed their children by bottle feeding of expressed breast milk and/or formula in the child care center and breastfeeding at home. Given that 69.4% of respondents reported that they currently have children receiving breast milk at the center, it leads us to question why women are not breastfeeding in the centers. The reason may be related to the distance between the child care center and the mothers’ residence or workplace, women’s comfort of feeding in that environment, or the needed frequency of breastfeeding depending on the child’s age. However, it was noted in phase 1 of the study that it was common practice for staff to recommend that parents introduce feeding expressed breast milk in a bottle prior to commencing child care. 15 Indeed, 71% of the survey respondents considered the early start of formula feeding to be the biggest barrier to supporting breastfeeding in child care centers.
The findings of this survey further demonstrate that child care centers support breastfeeding in a more passive than active way. As with phase 1 of the study, most respondents identified attitudes and facilities within their center that are supportive of breastfeeding. At the same time, they reinforced parental choice and a need for centers to make an equally inclusive and supportive environment for breastfeeding and nonbreastfeeding families alike. Therefore, most centers and staff do not actively promote breastfeeding but simply support it when parents require it. Respondents described the societal pressures on mothers to breastfeed and a strong sense that it was not their place to advise families on infant feeding methods and thereby add another source of societal pressure. This perspective is reinforced by the lack of staff training in support of breastfeeding. Given the high number of centers with children receiving breast milk, it seems reasonable to expect staff to have some education and training in supporting breastfeeding, rather than relying on personal experience or anecdotal information. This is an area in which support for breastfeeding in child care centers could be improved, and such an improvement may lead to productive collaborations with breastfeeding peer support groups and professionals such as lactation consultants.
The social expectations and lack of support around breastfeeding were considered a significant barrier to supporting breastfeeding in child care centers. Respondents felt strongly that breastfeeding practice in child care centers will be improved by addressing societal factors that affect mothers’ decision on breastfeeding.
A mother’s return to work and a child’s commencement of child care are 2 known events that currently result in a decline of breastfeeding. Addressing these issues is particularly important with the rising number of Australian mothers returning to work after having a child, and the increasing demand for child care services. If we are to achieve the goals set out in the Australian National Breastfeeding Strategy, 13 ways are needed to enable continuation of breastfeeding through these events.
Study Limitations
This study aimed to examine policy and practices that support breastfeeding in child care centers in metropolitan Adelaide. The low response rate (21.2%) for this survey limits the generalizability of the findings, however we did achieve a good variation of center types and sizes participating. Furthermore, we recognize the potential bias in the sample, as centers supportive of breastfeeding may have been more inclined to respond to our survey than those centers that do not actively support breastfeeding. Considering the low levels of active breastfeeding support reported among respondents who went to the effort to participate in this survey, it could be expected that breastfeeding support would be even lower if the survey had included those who were less interested in responding to a breastfeeding study. Finally, this study included only the long day care center. Study of other forms of child care, such as family day care and occasional care, are important in providing comprehensive understanding of breastfeeding support in all child care settings. Despite these limitations, this study, the first work of its kind in Australia, provides new information to inform future research and practice to promote breastfeeding-friendly child care environments.
Conclusion
Despite some strategies in place to support mothers to continue breastfeeding, there are no national standards on breastfeeding policies and practices in child care settings. Therefore, the extent and scope of practices in supporting breastfeeding depend on parental request and the perceptions and attitudes of child care center staff toward breastfeeding. Breastfeeding needs to be actively promoted and supported within child care settings through policy, practice, and training strategies to address the increasing need of Australian mothers who return to work after childbirth.
Footnotes
Acknowledgements
The authors acknowledge the participation of child care centers who accepted to complete the survey and provide us information about their breastfeeding policies and support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was made possible by a grant from the Faculty of Health Sciences, Flinders University.