
Abstract
Background:
Infant formula marketing, either directly to consumers or through health care providers, may influence women’s breastfeeding intentions, initiation, and duration. However, little is known about the impact of different types of media marketing on infant feeding intentions and behavior.
Objective:
This study investigated whether different types of recalled prenatal media marketing exposure to formula and breastfeeding information are related to breastfeeding intentions and behavior.
Methods:
Data were from the Infant Feeding Practices Study II, a longitudinal study from pregnancy through the infants’ first year. Sample sizes ranged from 1384 to 2530. Negative binomial, logistic regression, and survival models were used to examine associations between recalled prenatal exposure to formula or breastfeeding information and breastfeeding intentions and behavior.
Results:
Exposure to infant formula information from print media was associated with shorter intended duration of exclusive breastfeeding, and formula information from websites was related to lower odds of both intended and actual initiation. Exposure to breastfeeding information from websites was related to higher odds of both intended and actual initiation and longer intended duration of any breastfeeding. Breastfeeding information from print media was associated with longer duration of any breastfeeding, but information from broadcast media was associated with shorter duration of any breastfeeding.
Conclusion:
Mothers who recall exposure to formula information from print or websites are more likely to intend to use formula or to intend to use formula earlier and are less likely to initiate breastfeeding than mothers who do not recall seeing such information.
Keywords
Well Established
Infant formula is marketed directly to consumers through the media and promotions, including coupons and free samples. It is also marketed through the medical community. Infant formula marketing has been shown to influence infant feeding decisions and breastfeeding success.
Newly Expressed
Mothers who recalled exposure to formula information were more likely to intend to use formula or use it earlier—either intending not to initiate breastfeeding or intending a shorter duration of exclusive breastfeeding—and less likely to actually initiate breastfeeding.
Background
Infant formula marketing, either through the medical community or directly to consumers, has been shown to influence women’s decisions on whether to breastfeed or formula feed their newborn children.1,2 The World Health Organization’s International Code of Marketing of Breast-milk Substitutes 3 calls for no marketing of infant formula to the public, but the United States (US) has not adopted this code. While many studies show the ubiquity of marketing formula through the medical community in the United States and its effects on breastfeeding initiation and duration, little systematic research has been done to measure exposure to infant formula media marketing or its effects on infant feeding practices.4,5 Although some evidence suggests that mass media advertising of infant formula has increased recently, its extent is more difficult to quantify than the extent of marketing through the medical community because of data proprietary issues. 5 A report from the Government Accountability Office stated that the annual number of television (TV) and print ads for infant formula in the United States increased from about 7000 in 1999 to over 10 000 in 2004, while annual advertising expenditures grew from an estimated $29 million to over $46 million for domestic formula companies during the corresponding years. 5
We hypothesized that formula media marketing exposure is associated with a lower likelihood of intended and actual initiation and shorter intended and actual breastfeeding duration. We expected breastfeeding media marketing to have the opposite effects. We developed our hypotheses based on the theory of reasoned action and the theory of planned behavior 6 and tested associations between self-reported exposure to media marketing of infant formula and breastfeeding and breastfeeding intentions, initiation, and duration. These theories emphasize the importance of behavioral intentions and that subjective norms (formed by opinions of important people around an individual) can directly influence intentions and behaviors. 6
Methods
This study uses data from the Infant Feeding Practices Study II (IFPS II) to analyze infant formula media marketing exposure. Because formula media marketing can take the form of information pieces in addition to advertisements, we did not distinguish advertisements from other forms of information, although we controlled for other forms of marketing, including marketing through the medical community and providing samples directly to mothers. We included breastfeeding media marketing in our analysis because breastfeeding and formula information frequently appear together,1,7 and each may affect response to the other.
Study Population
The IFPS II is a longitudinal survey of women from late pregnancy through their infant’s first year of life conducted by the US Food and Drug Administration (FDA) and the Centers for Disease Control and Prevention between 2005 and 2007. The sample was drawn from a nationally distributed but not representative consumer opinion panel, resulting in a sample size of about 3000 mothers aged 18 and older for postnatal data. Questionnaires were mailed once prenatally and 10 times over the first year postpartum; 94% of the postnatal sample returned at least 2 questionnaires. The sample was limited to healthy mothers with healthy term or near-term singleton infants, and it overrepresents older, White, middle income, and higher educated mothers. Detailed methods and sample criteria are given in Fein et al. 8 The study was approved under expedited review by the institutional review board of the US Food and Drug Administration, Silver Spring, Maryland.
Dependent Variables
Intended breastfeeding duration
Intended duration of exclusive breastfeeding was based on when mothers expected to first feed food besides breast milk. The original categories were in ranges; we used the midpoints (rounded to the nearest integer to enable negative binomial modeling) of each category to estimate months of intended breastfeeding. In Table 1, these were converted to weeks for comparison with actual behavior. Intended duration of any breastfeeding was based on the question, “How old do you think your baby will be when you completely stop breastfeeding?”
Descriptive Statistics of Mothers’ Characteristics and Other Variables Used in the Models a
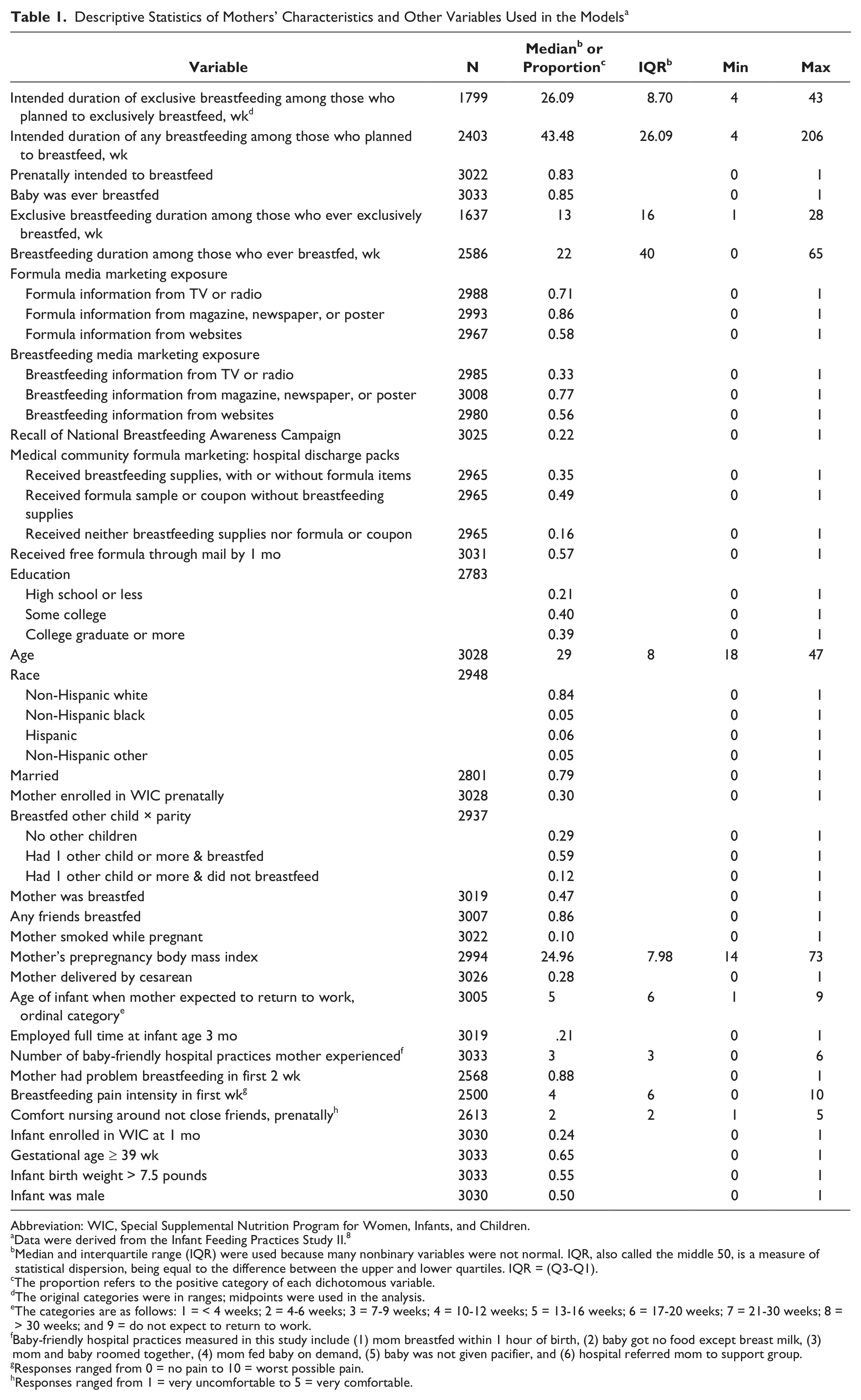
Abbreviation: WIC, Special Supplemental Nutrition Program for Women, Infants, and Children.
Data were derived from the Infant Feeding Practices Study II.
Median and interquartile range (IQR) were used because many nonbinary variables were not normal. IQR, also called the middle 50, is a measure of statistical dispersion, being equal to the difference between the upper and lower quartiles. IQR = (Q3-Q1).
The proportion refers to the positive category of each dichotomous variable.
The original categories were in ranges; midpoints were used in the analysis.
The categories are as follows: 1 = < 4 weeks; 2 = 4-6 weeks; 3 = 7-9 weeks; 4 = 10-12 weeks; 5 = 13-16 weeks; 6 = 17-20 weeks; 7 = 21-30 weeks; 8 = > 30 weeks; and 9 = do not expect to return to work.
Baby-friendly hospital practices measured in this study include (1) mom breastfed within 1 hour of birth, (2) baby got no food except breast milk, (3) mom and baby roomed together, (4) mom fed baby on demand, (5) baby was not given pacifier, and (6) hospital referred mom to support group.
Responses ranged from 0 = no pain to 10 = worst possible pain.
Responses ranged from 1 = very uncomfortable to 5 = very comfortable.
Breastfeeding initiation
Breastfeeding initiation is a dichotomous variable where 1 means “Baby was ever breastfed.”
Breastfeeding duration
Our measure of any breastfeeding duration was constructed from a question asking how old the baby was when the mother completely stopped breastfeeding and pumping milk. If the mother did not answer the question, duration was estimated as the midpoint of infant ages on the questionnaire when she last indicated she was breastfeeding and the first questionnaire on which she indicated that she was not breastfeeding. If the mother was breastfeeding on the last questionnaire she returned, duration is censored at the infant age on the last questionnaire. Because the study ended at about infant age 12 months, the measure is actually breastfeeding duration within the first year.
We defined exclusive breastfeeding duration to measure this behavior after hospital discharge; infants who were given formula in the hospital but were exclusively breastfed after discharge were considered exclusively breastfed. Duration of exclusive breastfeeding was the midpoint of the infant age when the mother last reported feeding the infant only breast milk and the age when the mother first reported that she was not exclusively breastfeeding. If the mother was exclusively breastfeeding on the last questionnaire she returned, exclusive breastfeeding duration is censored at the infant age on the last questionnaire. Exclusive breastfeeding is recommended only for the first 6 months of life, 9 and nearly all mothers introduced solid foods by 6 months 10 ; therefore, we measured exclusive breastfeeding only through 28 weeks (6.5 months). Exclusive breastfeeding durations longer than 28 weeks (about 4% or 65 mothers reported exclusive breastfeeding over 28 weeks) were set to 28 weeks.
Focus Variables
Infant formula and breastfeeding media marketing exposure
Our measures of exposure to media marketing are based on mother’s recall of having seen certain information and therefore measure both exposure and attention to the information. The prenatal questionnaire, completed at an average gestation age of 30.6 weeks, asked mothers whether they had recently heard about infant formula and about breastfeeding from various media sources without distinguishing advertisements from information pieces or defining recently. The responses were grouped into 3 pairs of dichotomous variables each for formula and for breastfeeding, where 1 means that respondents reported recent exposure to marketing from TV or radio; from magazines, newspapers, or posters; or from the Internet. An additional variable was awareness of the National Breastfeeding Awareness Campaign (NBAC), 11 which ran concurrently with the prenatal data collection; 1 means the respondent was aware of an NBAC ad, including the radio ads.
Covariates
Covariates were selected based on the literature, especially previous publications from this dataset,10,12-15 and the theories of reasoned action and planned behavior. 6 These covariates included demographic and economic characteristics of mothers,10,12,14-16 employment,12-17 hospital experience,12,18 Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) enrollment, 10 previous breastfeeding experience,14,19 feelings toward breastfeeding,12,13,17,20,21 breastfeeding difficulties, 17 maternal smoking,12,14,17 and influence of people around the mother.12,14,22 Marketing through the medical community was measured by whether breastfeeding supplies, formula samples, or coupons were included in a gift pack received from the hospital or birth center. It was coded into the following mutually exclusive categories: received breastfeeding supplies with or without formula items, received formula samples or coupons only, and received no gift pack. Hospital experience was measured by the number of baby-friendly hospital practices 23 the mother experienced, of those available in the data: breastfed within 1 hour of birth, baby got no food except breast milk, mother and baby roomed together, mother fed baby on demand, baby was not given a pacifier, and the hospital referred the mother to a support group. 12
Additionally, several covariates measured the supportiveness toward breastfeeding of the mother’s social networks, because our theory indicated that we should include such variables: whether the mother was breastfed, whether she had friends who had breastfed, and her level of embarrassment about breastfeeding. Other covariates are listed in Table 1. Each multivariate analysis includes a slightly different set of covariates, as listed in the footnote of each table, because some variables likely to influence breastfeeding duration had not occurred when intentions or initiation were measured.
Statistical Analyses
We used SAS 9.2 to conduct all analyses. We analyzed both bivariate associations (without controlling for any covariates) and multivariate models between media marketing exposure and each of the intended and actual breastfeeding behaviors. We used negative binomial models for the intended duration variables because they were not normally distributed, even after various transformations. The negative binomial is more appropriate than a Poisson approach here because our sample variance was not equal to the sample mean. We have some right censoring (mothers either did not complete all the questionnaires or they breastfed longer than the period we measured) with both of our breastfeeding duration variables; therefore, we used Cox Proportional Hazards models for the actual duration variables. A Cox Proportional Hazards model is a type of survival model that can account for censored data and is robust and makes no parametric assumptions concerning the nature or shape of the underlying survival distributions. 24 All independent variables were non-time-dependent covariates. Both the negative binomial and survival model results were exponentiated so that all results are interpreted as either expected ratios of durations or hazard ratios. Because hazard ratios 24 represent the risk of breastfeeding cessation rather than continuation, hazard ratios of less than 1 indicate a reduced risk of breastfeeding cessation and thus increased breastfeeding duration. Similarly, hazard ratios greater than 1 indicate an increased risk of breastfeeding cessation and therefore decreased breastfeeding duration. To reduce confusion, we interpret the inverse of hazard ratios in the Results section to indicate the association with breastfeeding duration rather than cessation.
Results
Almost all breastfeeding duration variables were not normally distributed; medians and interquartile ranges were used instead of the means and standard deviations. The median intended duration of exclusive breastfeeding (26 weeks) nearly met the recommended 28 weeks, but the median intended any breastfeeding duration (43.5 weeks) was shorter than the recommended minimal 52 weeks. 9 In this sample, 83% of mothers intended to initiate breastfeeding and 85% actually did so. The median actual duration of exclusive (13 weeks) and any (22 weeks) breastfeeding was much shorter than intended, measured among those who initiated each behavior.
More women reported exposure to formula than to breastfeeding information from each type of media except the Internet, which showed about the same percentage exposed to both topics. The most common media exposure was printed materials for both formula and breastfeeding information. About 22% of mothers were aware of an advertisement from the NBAC. More than half of mothers also received free formula by mail. Other sample characteristics are shown in Table 1.
Bivariate associations between formula and breastfeeding marketing measures and intended and actual breastfeeding are shown in Table 2. None of the media marketing exposure measures was significantly related to intended exclusive breastfeeding duration. Formula information exposure from TV or radio was associated with shorter exclusive breastfeeding duration, but exposure to formula media marketing from websites was associated with longer intended any breastfeeding and higher odds of intended and actual breastfeeding initiation. Exposure to formula media marketing from print was also positively associated with higher odds of intended breastfeeding initiation. Breastfeeding media exposures displayed many resemblances to formula exposures among all the significant bivariate relationships but were also associated with duration of any breastfeeding: Breastfeeding information exposure from TV or radio was associated with shorter exclusive and any breastfeeding duration, and exposure from print or websites was positively associated with intending to breastfeed and actual initiation and longer duration of any breastfeeding. Recalling an advertisement from the NBAC was significantly associated with shorter duration of any breastfeeding (Table 2), but not with other breastfeeding measures.
Bivariate Associations between Each Media Marketing Exposure Variable and the Breastfeeding Measures a
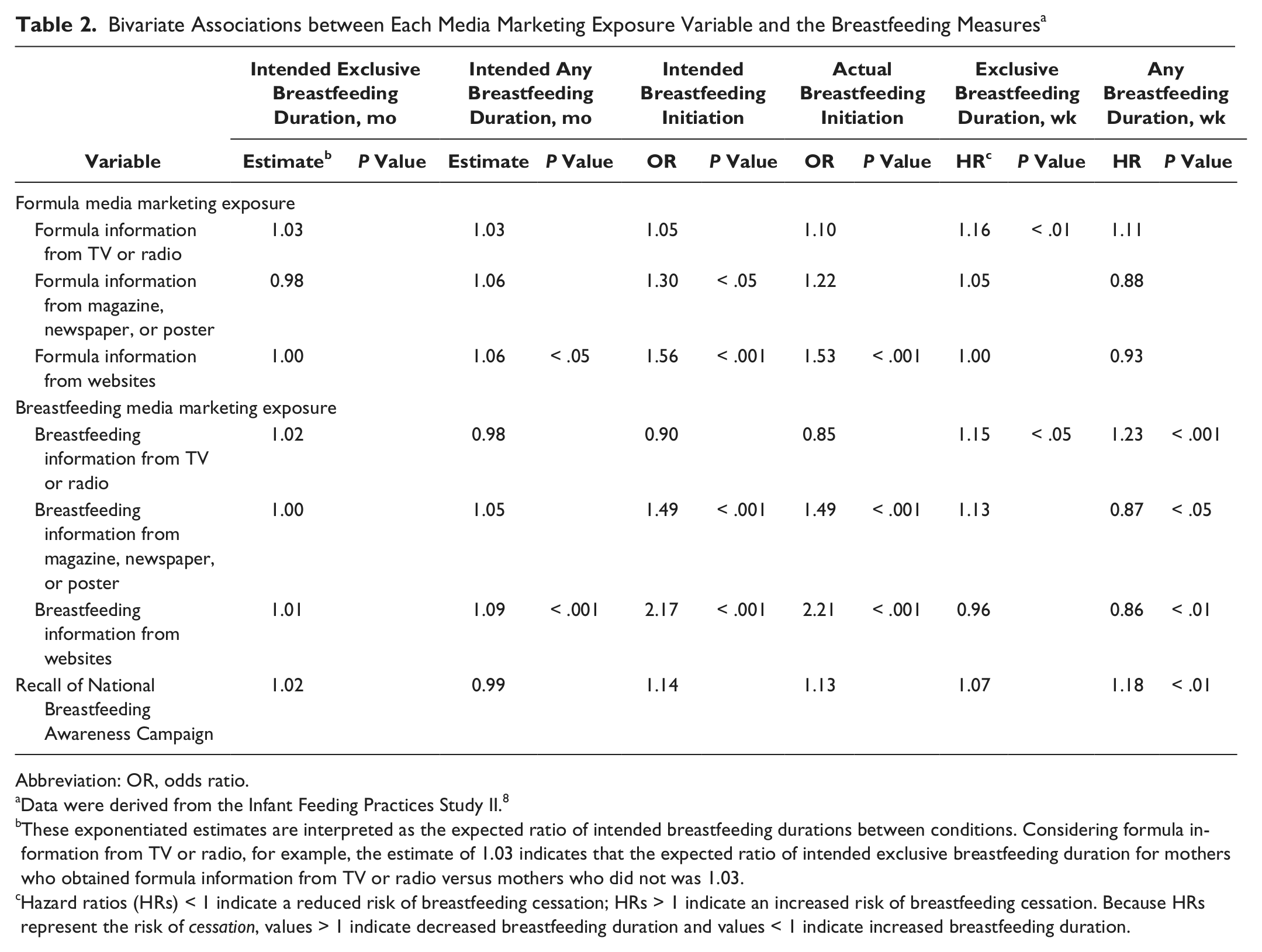
Abbreviation: OR, odds ratio.
Data were derived from the Infant Feeding Practices Study II. 8
These exponentiated estimates are interpreted as the expected ratio of intended breastfeeding durations between conditions. Considering formula information from TV or radio, for example, the estimate of 1.03 indicates that the expected ratio of intended exclusive breastfeeding duration for mothers who obtained formula information from TV or radio versus mothers who did not was 1.03.
Hazard ratios (HRs) < 1 indicate a reduced risk of breastfeeding cessation; HRs > 1 indicate an increased risk of breastfeeding cessation. Because HRs represent the risk of cessation, values > 1 indicate decreased breastfeeding duration and values < 1 indicate increased breastfeeding duration.
Table 3 displays multivariate negative binomial regression results between exposure to formula and breastfeeding media marketing and intended duration of exclusive and any breastfeeding, after adjusting for other marketing variables and the covariates. We found only 2 significant associations. Formula information from printed materials was negatively associated with intended duration of exclusive breastfeeding, and exposure to breastfeeding information from websites was positively associated with intended duration of any breastfeeding. The estimates are expected ratios of duration for mothers who did and did not report exposure to each type of information. For example, the expected ratio of intended exclusive breastfeeding duration for mothers who obtained formula information from print materials versus mothers who did not was .92, which means that exposure to formula information from printed materials was associated with shorter intended exclusive breastfeeding duration (Table 3).
Negative Binomial Estimates (Exponentiated) for Intended Exclusive and Any Breastfeeding Duration among Mothers who Intended to Breastfeed as a Function of Media Marketing Exposure a
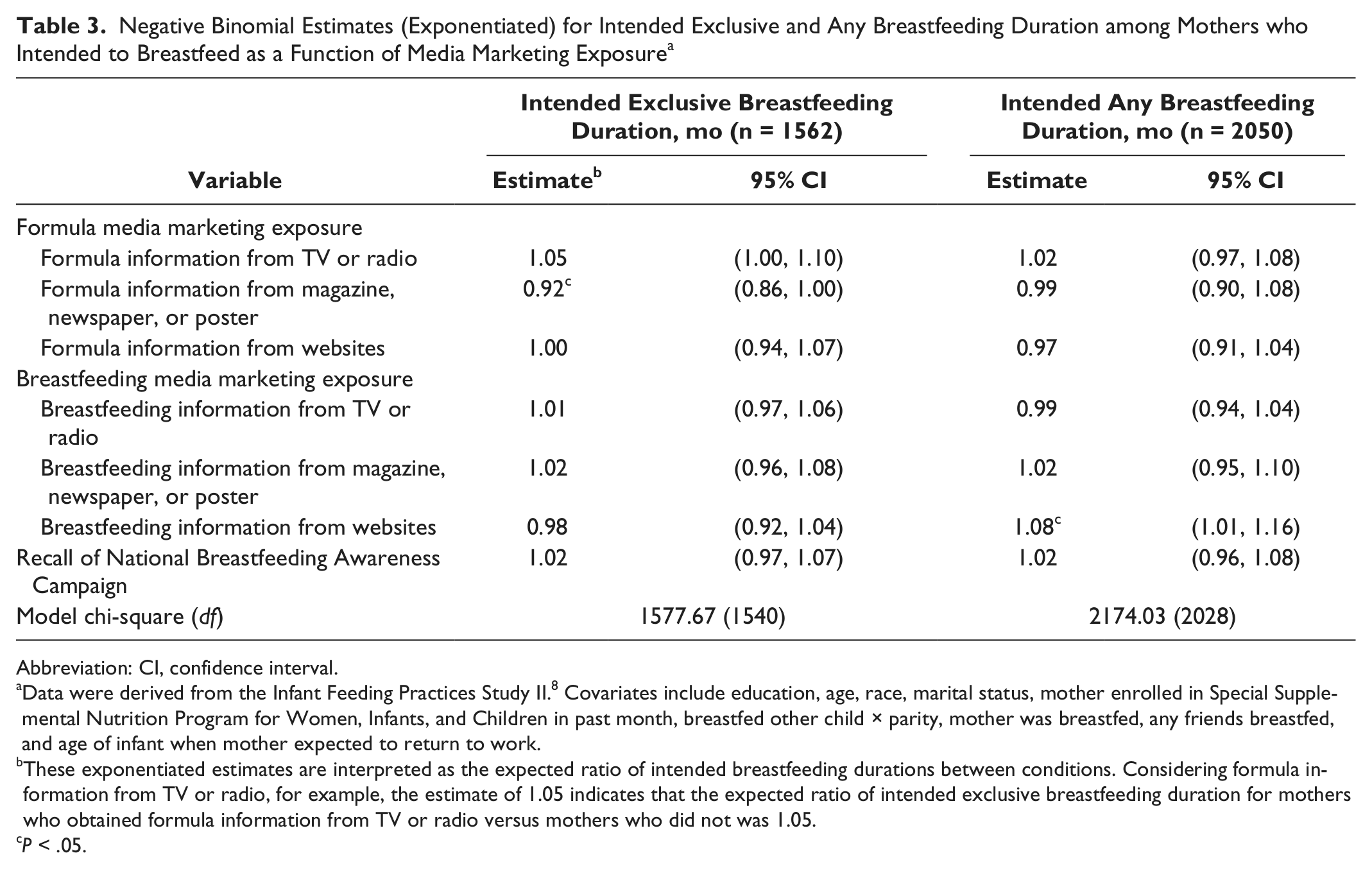
Abbreviation: CI, confidence interval.
Data were derived from the Infant Feeding Practices Study II.8 Covariates include education, age, race, marital status, mother enrolled in Special Supplemental Nutrition Program for Women, Infants, and Children in past month, breastfed other child × parity, mother was breastfed, any friends breastfed, and age of infant when mother expected to return to work.
These exponentiated estimates are interpreted as the expected ratio of intended breastfeeding durations between conditions. Considering formula information from TV or radio, for example, the estimate of 1.05 indicates that the expected ratio of intended exclusive breastfeeding duration for mothers who obtained formula information from TV or radio versus mothers who did not was 1.05.
P < .05.
The multivariate logistic regression model results between formula and breastfeeding marketing exposure and intended and actual breastfeeding initiation are shown in Table 4. Controlling for other variables in the model, both formula and breastfeeding information from websites stood out as significant, though in opposite directions: The odds of intended breastfeeding initiation among mothers who received formula information from websites were .62 times (or 38%) lower than those of mothers who did not; for mothers who received breastfeeding information from websites, the comparable odds were 2.58 times (or 158%) higher. For actual breastfeeding initiation, the odds were .65 times (or 35%) lower among mothers who received formula information from websites versus those who did not and 2.35 times (or 135%) higher for mothers who received breastfeeding information from websites (Table 4).
Logistic Regression Models for Intended and Actual Breastfeeding Initiation as a Function of Media Marketing and Mother and Infants’ Characteristics a
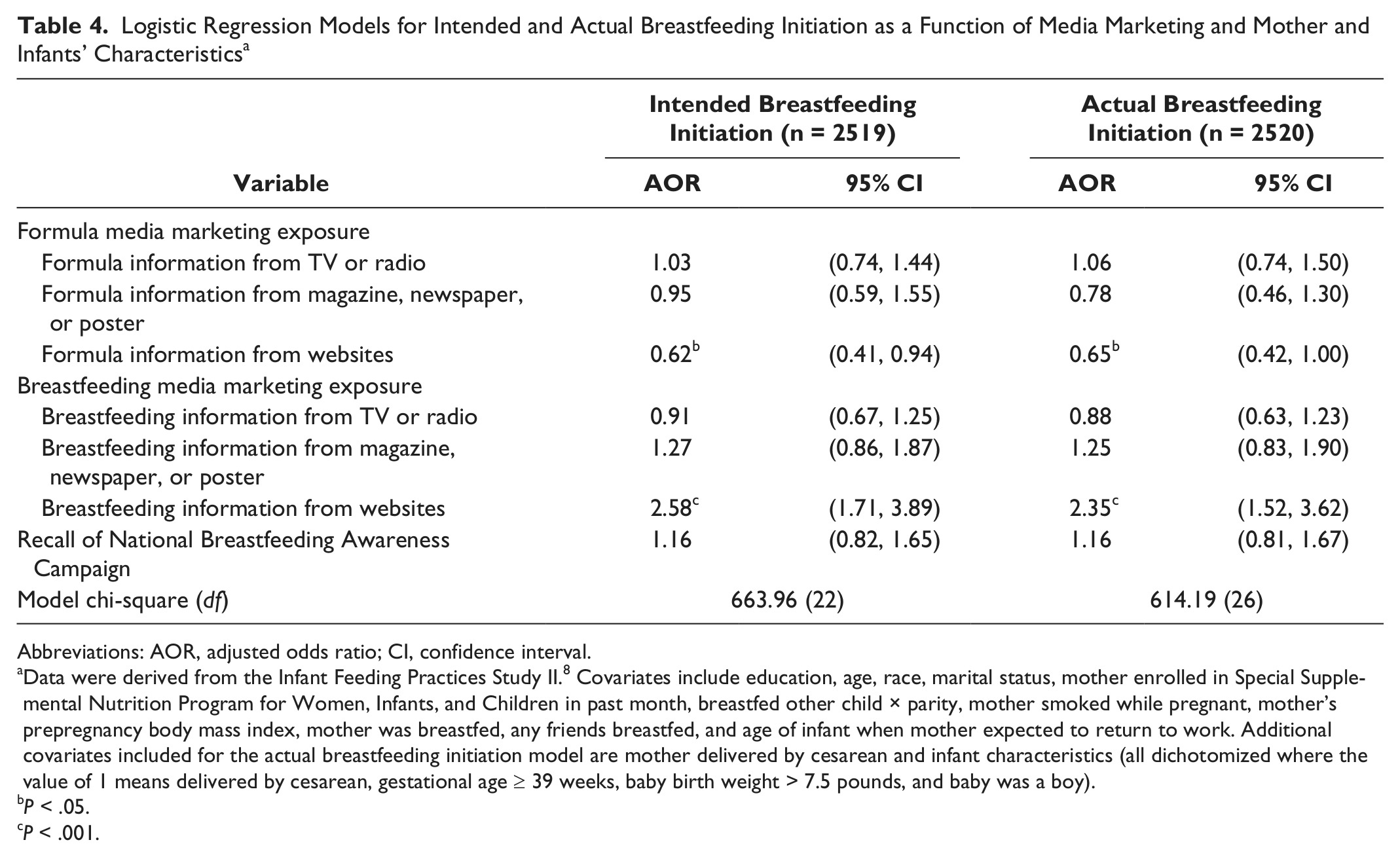
Abbreviations: AOR, adjusted odds ratio; CI, confidence interval.
Data were derived from the Infant Feeding Practices Study II.8 Covariates include education, age, race, marital status, mother enrolled in Special Supplemental Nutrition Program for Women, Infants, and Children in past month, breastfed other child × parity, mother smoked while pregnant, mother’s prepregnancy body mass index, mother was breastfed, any friends breastfed, and age of infant when mother expected to return to work. Additional covariates included for the actual breastfeeding initiation model are mother delivered by cesarean and infant characteristics (all dichotomized where the value of 1 means delivered by cesarean, gestational age ≥ 39 weeks, baby birth weight > 7.5 pounds, and baby was a boy).
P < .05.
P < .001.
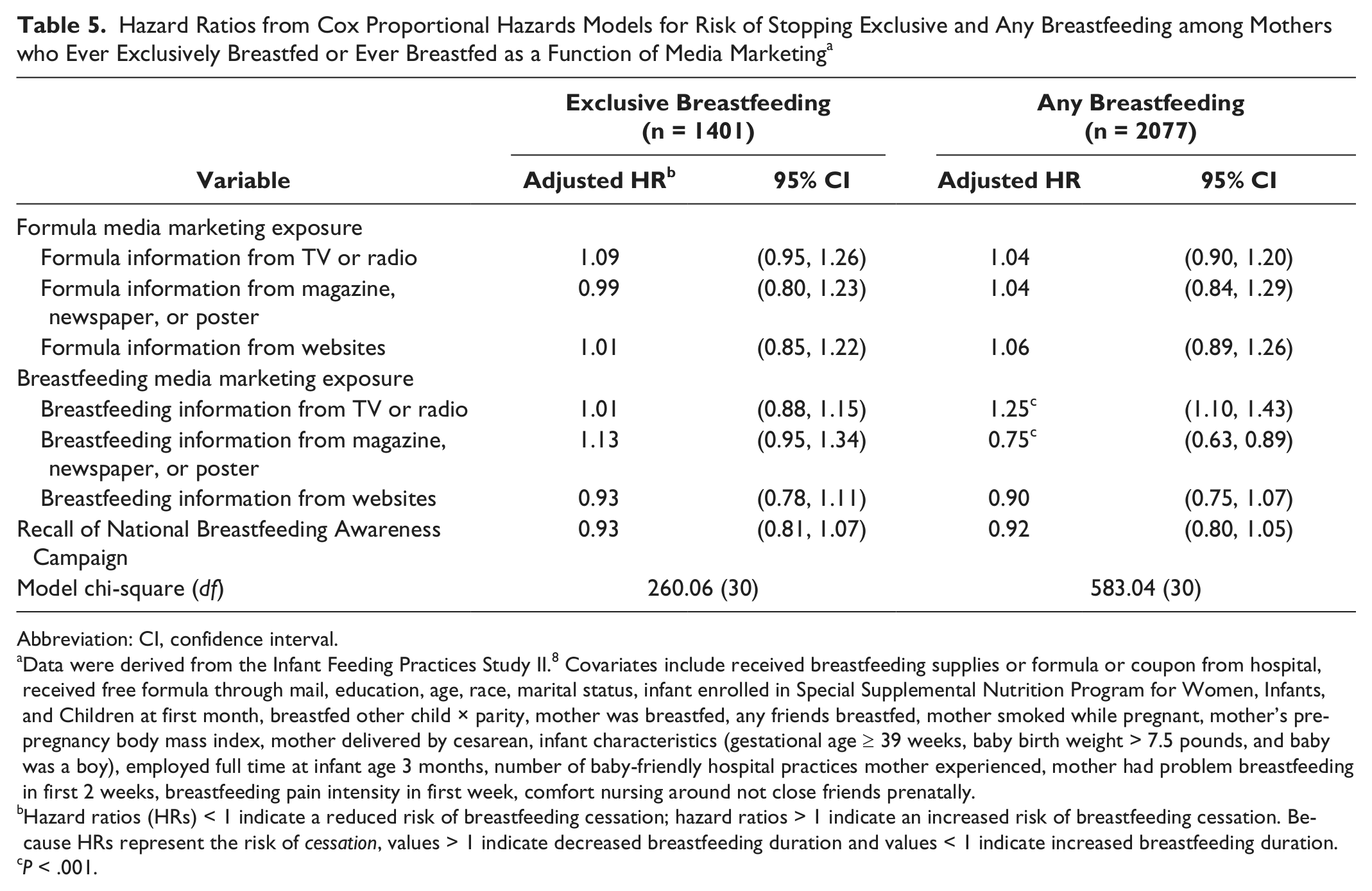
Table 5 displays the multivariate survival models between the formula and breastfeeding marketing measures and actual duration of exclusive and any breastfeeding. Because hazard ratios model the risk of cessation, ratios greater than 1 indicate greater risk of cessation and therefore shorter duration, while ratios less than 1 indicate reduced risk and longer duration. After controlling for other measures of marketing exposure and the covariates, only 2 of the bivariate significant associations remained. Mothers who received breastfeeding information from TV or radio had shorter breastfeeding duration, as indicated by having a higher risk of stopping any breastfeeding, about 1.25 times (or 25%) higher than that of mothers who did not receive breastfeeding information from TV or radio. The positive association between exposure to breastfeeding information from print media and duration of any breastfeeding remained (the hazard ratio dropped from .87 in Table 2 to .75 in Table 5 and the significance level increased from P < .05 to P < .001). The negative association between recall of an advertisement from the NBAC and duration of any breastfeeding was no longer significant in the multivariate model (Table 5).
Hazard Ratios from Cox Proportional Hazards Models for Risk of Stopping Exclusive and Any Breastfeeding among Mothers who Ever Exclusively Breastfed or Ever Breastfed as a Function of Media Marketing a
Abbreviation: CI, confidence interval.
Data were derived from the Infant Feeding Practices Study II.8 Covariates include received breastfeeding supplies or formula or coupon from hospital, received free formula through mail, education, age, race, marital status, infant enrolled in Special Supplemental Nutrition Program for Women, Infants, and Children at first month, breastfed other child × parity, mother was breastfed, any friends breastfed, mother smoked while pregnant, mother’s prepregnancy body mass index, mother delivered by cesarean, infant characteristics (gestational age ≥ 39 weeks, baby birth weight > 7.5 pounds, and baby was a boy), employed full time at infant age 3 months, number of baby-friendly hospital practices mother experienced, mother had problem breastfeeding in first 2 weeks, breastfeeding pain intensity in first week, comfort nursing around not close friends prenatally.
Hazard ratios (HRs) < 1 indicate a reduced risk of breastfeeding cessation; hazard ratios > 1 indicate an increased risk of breastfeeding cessation. Because HRs represent the risk of cessation, values > 1 indicate decreased breastfeeding duration and values < 1 indicate increased breastfeeding duration.
P < .001.
Discussion
The key contribution to the literature from this research is the finding that mothers who recalled exposure to formula information were more likely to intend to use formula or to use it earlier and less likely to actually initiate breastfeeding. These mothers were more likely either to intend not to initiate breastfeeding or to intend a shorter duration of exclusive breastfeeding. Specifically from the multivariate models, we found that exposure to formula information from print sources was associated with shorter intended exclusive breastfeeding duration and exposure to formula information from websites was associated with lower odds of intended and actual breastfeeding initiation. Also, breastfeeding information from websites showed the most consistent associations, being positively related to intended duration of any breastfeeding, as well as intended and actual initiation. Breastfeeding information from print media was significantly associated with longer duration of any breastfeeding. However, breastfeeding information from broadcast media was significantly associated with shorter duration of any breastfeeding. It may be that most broadcast information about breastfeeding is in the form of news stories that negatively portray breastfeeding, such as about women arrested for breastfeeding in public 25 or about infants who suffered health problems because of breastfeeding inadequacy. 4
Consistent with previous research,1,26 we found that most pregnant women were exposed to information in the media about both infant formula and breastfeeding, but more women reported seeing information about formula than breastfeeding from each source except websites, from which a similar number of mothers received information.
Our results provide some evidence that different types of media information about formula marketing influence breastfeeding at different stages; formula information from print media was significantly related to shorter intended duration of exclusive breastfeeding, and formula information from websites was negatively related to both intended and actual initiation. Also, we found more significant associations between the breastfeeding outcome measures and media exposure from websites than for other types of media. It may be that women who are exposed to information on websites are more likely to be seeking the information, as opposed to passively receiving it, as might occur with broadcast or print media. If this is true, then those receiving information from websites or the Internet may have self-selected to receive a specific type of information, more so than women exposed to infant feeding information from other media. But it is also possible that websites are more effective at influencing mothers’ feeding decisions.
It is worth noting that after holding other variables constant in the model, most bivariate associations were no longer significant, and the positive associations between formula information and intended and actual breastfeeding initiation turned negative. The large differences in terms of strength, significance, and direction in the results between the bivariate and multivariate results for formula information indicate that the bivariate associations were confounded by other factors and could be misleading. For breastfeeding information, the bivariate associations that remained significant in the multivariate models were more consistent in that the direction of association did not change.
Literature analyzing popular magazines indicates that a relation exists between quantity of some types of media content and health behavior. A content analysis of Parents Magazine indicated that frequency of formula feeding advertisements negatively predicted breastfeeding in new mothers the next year. The overall absence of breastfeeding advertisements was notable in that study because it means that no equivalent advertising counter-message to the formula feeding advertisements existed. 1 Although we did not measure quantity of marketing pieces, we found that exposure to print information about breastfeeding was positively related to duration of any breastfeeding. Another study examined how 7 US parenting and women’s magazines framed breastfeeding and formula-feeding messages. Analysis of 615 articles published from 1997 to 2003 indicated that the magazines provided more information on breastfeeding than formula feeding; however, the messages tended to focus on breastfeeding barriers and placed much of the responsibility of infant feeding on the mother, while the role of social and partner support was diminished. 7
The study has several important strengths, including the longitudinal nature of the data, so that we were able to measure exposure to media information before actual breastfeeding initiation or duration. The sample, although not representative, has other positive characteristics, including the large sample size and the national distribution of healthy mothers and infants.
The study also has several limitations. Our measure of marketing exposure was limited to recalled exposure rather than objective exposure. Some mothers may have been exposed to (and influenced by) various types of information without remembering it, and they may have been more likely to recall being exposed to information that supported their feeding intentions. However, the lack of association between most measures of exposure and the breastfeeding intention measures suggests that this bias is not strong. Another limitation is that, although we measured exposure to information from different types of media, we did not have measures of exposure frequency, tone, or specific contents. This study also presents a limitation regarding measurement of media exposure. There was a time lag between measuring exposure and actual breastfeeding, and the study did not control for what women saw after the measurement of media exposure. Therefore, mothers could have been exposed to additional media information after the measurement but before the actual breastfeeding behaviors. Note that this limitation does not apply to the indicators of intended behaviors, which were measured at the same time as media exposure. Additional limitations are that the IFPS II did not have a nationally representative sample and the questionnaires were administered by mail, which required that mothers be able to read and write English and have a stable mailing address. Because the respondents in the study overrepresented non-Hispanic White, older mothers of higher socioeconomic status, the results cannot be generalized to the overall US population of mothers.
Conclusion
Most pregnant women were exposed to infant feeding information in the media, and more reported exposure to formula than to breastfeeding information. Formula information from print media was negatively related to intended duration of exclusive breastfeeding, and formula information from websites was negatively related to both intended and actual initiation. Mothers who recalled exposure to formula information from print or websites were more likely to intend to use formula instead of breastfeeding or to intend to use formula earlier and were less likely to initiate breastfeeding than mothers who did not recall seeing such information. These results reinforce conclusions from previous studies on the importance of increasing exposure to breastfeeding information in the various types of media. Future research might focus on media exposure frequency, specific tone or contents, or how media information impacts women’s decisions on breastfeeding through changing social norms.
The findings of this study should alert breastfeeding advocates to more frequently promote breastfeeding information in print media and on websites to counter the impact that formula marketing has on mothers’ feeding decisions. Because formula advertising is negatively associated with early breastfeeding decisions (intentions and initiation), breastfeeding messages need to reach women before childbirth.
Footnotes
Acknowledgements
The Authors prepared the article within the scope of their employment with the US Food and Drug Administration - Center for Food Safety and Applied Nutrition. Accordingly, the content of this article is a US government work and in the public domain within the United States.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The data collection was funded by the Food and Drug Administration, Centers for Disease Control and Prevention, Office of Women’s Health, National Institutes of Health, and the Maternal and Child Health Bureau in the US Department of Health and Human Services. This analysis was funded by the Food and Drug Administration.