
Abstract
Background:
Mothers of preterm and sick infants admitted to the neonatal intensive care unit (NICU) often encounter more difficulties with breastfeeding than mothers of healthy term newborns. The extent to which Baby-Friendly designation is associated with breastfeeding rates for NICU infants over time is unknown.
Objective:
This study aimed to determine the rate of breastfeeding initiation and continuation in a US, inner-city, level 3 NICU 10 years after Baby-Friendly designation.
Methods:
We compared the rate of breastfeeding initiation and continuation among breastfeeding-eligible mothers with infants admitted to the Boston Medical Center NICU in 1999 and 2009, using chi-square tests.
Results:
Breastfeeding initiation increased from 74% in 1999 to 85% in 2009 (P = .04). Any breast milk at 2 weeks of age increased from 66% to 80% (P = .05), and exclusive breastfeeding at 2 weeks remained stable between 1999 and 2009. Breastfeeding initiation increased from 68% to 86% among black mothers from 1999 to 2009 (P = .01).
Conclusion:
Improvement in breastfeeding initiation and any breastfeeding at 2 weeks of age continued 10 years after Baby-Friendly designation among mothers with NICU infants in a US, inner-city, level 3 NICU.
Well Established
Baby-Friendly Hospital Initiative (BFHI) designation appears to be associated with increased breastfeeding rates among vulnerable infants admitted to the neonatal intensive care unit (NICU), but whether increases in breastfeeding rates persist long term is unknown.
Newly Expressed
Breastfeeding initiation for infants admitted to the NICU continued to improve 10 years after BFHI designation at our hospital, reflecting a sustained association between BFHI designation and breastfeeding rates in the NICU.
Background
Human milk constitutes the optimal nutrition for preterm and sick infants admitted to the neonatal intensive care unit (NICU).1-6 Breast milk production can be especially difficult for mothers of hospitalized infants because these mothers must initiate and maintain breast milk production with hand expression and/or use of electric breast pumps, even while some of them are critically ill themselves.
The United Nations Children’s Fund (UNICEF) and the World Health Organization (WHO) launched the Baby-Friendly Hospital Initiative (BFHI) in 1991 to increase breastfeeding rates worldwide. Boston Medical Center (BMC), an inner-city teaching hospital, became Baby-Friendly designated in 1999, and at that time, rates of any and exclusive breastfeeding rose significantly among healthy, term infants, as well as among infants in our NICU.7,8 Our 2003 study reporting increases in breastfeeding among NICU infants after Baby-Friendly designation 7 is one of the very few studies examining the association between BFHI implementation and breastfeeding rates of NICU infants. Indeed, we have been unable to locate any other studies in English, except for 1 short report, specifically dealing with this topic. 9 When Renfrew published a review in 2010 of interventions to increase breastfeeding in neonatal intensive care, 10 our 2003 study 7 was 1 of only 2 located looking at the NICU and the BFHI, and the only one that was rated good quality.
At the time of writing, there were no internationally recognized Baby-Friendly-specific guidelines for NICU infants. Hospitals in some nations, such as Norway, have introduced NICU-specific Baby-Friendly certification,11,12 and currently, an international expert workgroup is working to create guidelines and assessment criteria for Baby-Friendly designation specific to the NICU. 13 In the United States, NICUs are not assessed for Baby-Friendly compliance independently of the general maternity service, and the BMC NICU has not undergone, at any point, a NICU-specific assessment. At the time of our certification in 1999, the NICU was required to provide staff and patient education following the same guidelines as other areas of the hospital undergoing assessment; required to purchase formula like the rest of the hospital; and not permitted to promote breast milk substitutes. Within the context of this increased interest in Baby-Friendly and the NICU population, we conducted a study to determine whether improvements in breastfeeding initiation and continuation were sustained a decade after BFHI designation at BMC.
Methods
Study Participants
Research assistants extracted data from the medical records of all mothers and infants admitted to the BMC NICU in 1999 and 2009. We used the same eligibility criteria described in our previous study 7 when comparing breastfeeding rates from 1995 to 1999. Exclusion criteria are shown in Figure 1. Two changes with regard to potential participants occurred in the BMC NICU between 1999 and 2009. The level 3 NICU expanded from a 15- to a 22-bed facility, and we updated our hospital policy for breastfeeding eligibility in accordance with revisions to the American Academy of Pediatrics policy1,14 (thus, breastfeeding for women on physician-prescribed methadone or buprenorphine was not recommended in 1999, but was in 2009). The Boston University Medical Center Institutional Review Board approved this study.
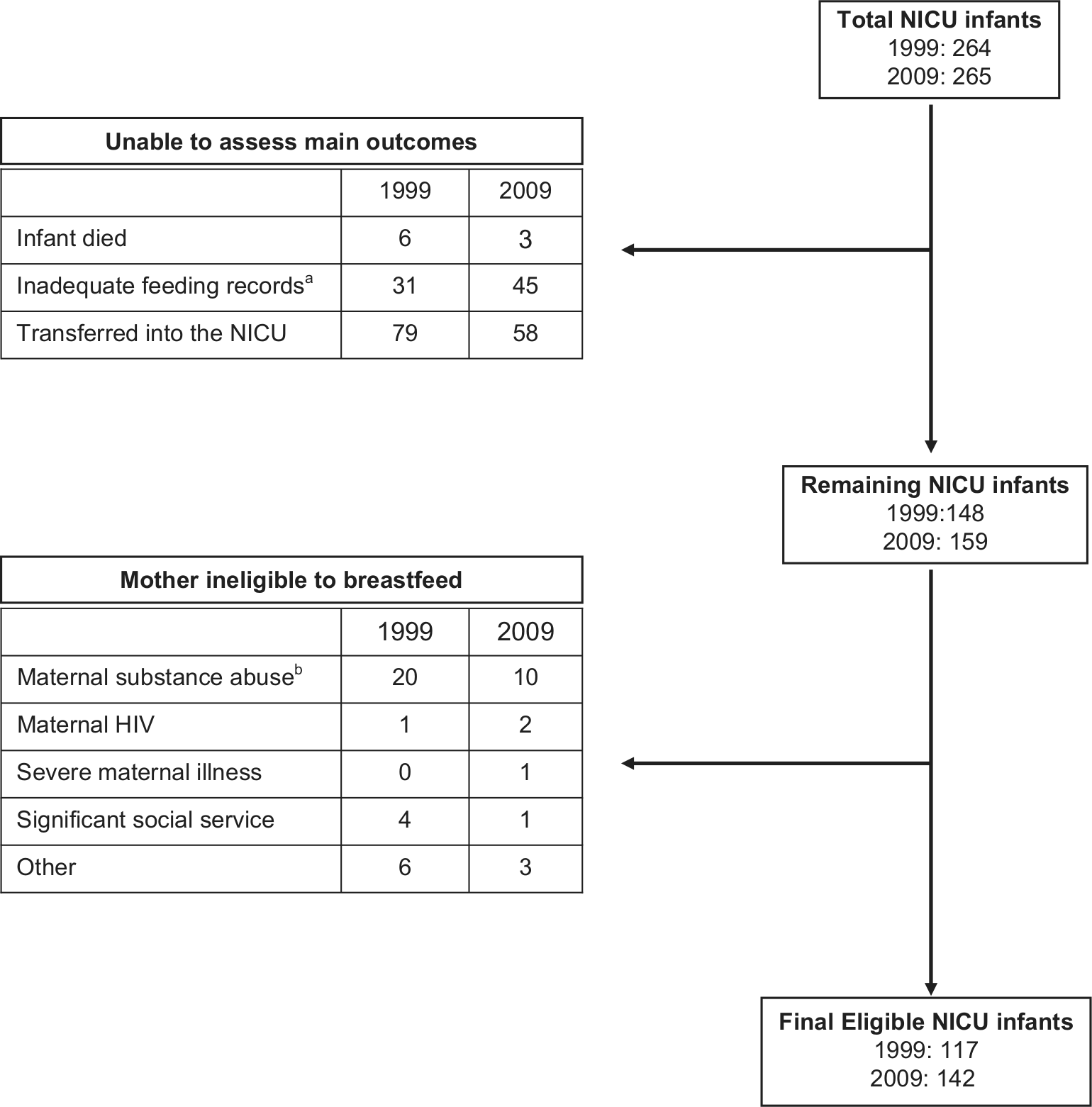
Exclusion Flowchart
Main Outcomes
In keeping with our original study, we defined breastfeeding initiation as any administration of breast milk by any method (tube, breast, alternative such as bottle or syringe) in the first week of enteral feedings. 7 We did this because many NICU infants do not receive enteral feedings in the first few days, or mothers may not be able to provide milk in the first day or two of life but may go on to breastfeed. Any infant who did not receive breast milk in the first week of enteral feeds was counted as a nonbreastfeeder. We examined breastfeeding continuation as breast milk administration at 2 and 6 weeks of life for those infants who received feedings and remained in the NICU at 2 and 6 weeks, respectively. We tallied the total number of breast milk feedings, with or without medications, human milk fortifier, or other supplements, as well as formula feedings for a 48-hour period on days 13 and 14 of life (2 weeks of age) and days 41 and 42 of life (6 weeks of age). We defined exclusive breast milk feeders as infants who received all feedings of breast milk; mixed feeders as infants who received 1 or more feedings from formula, and exclusive formula feeders as infants who received no breast milk. So, for example, if an infant received 15 total feedings on days 13 and 14 of life, and all feedings were of breast milk, he or she was categorized as an exclusive breastfeeder. If an infant received 15 total feedings, and 1 or more of the feeds were of formula and the others breast milk, he or she was categorized as a mixed feeder. We also examined whether infants received “any breast milk”; this category combined infants classed as exclusive breastfeeders and mixed feeders.
Demographics
We extracted maternal age, race (self-defined at hospital admit), insurance status, mode of delivery (vaginal or cesarean section), infant birth weight, gestational age, and sex from the medical record.
Practices in the NICU
Most infant-feeding-related practices that take place during the infant’s NICU stay have remained consistent since the original study. As a Baby-Friendly hospital, we provide infant feeding information to mothers pre- and postpartum, and ongoing education to perinatal providers at all levels. We adhere to the International Code of Marketing of Breast-milk Substitutes, 15 paying for all preterm and term formulas and ensuring no promotion of infant formula. Our infant feeding policy addresses hand expression, initiation of pumping within 6 hours of birth, and continued pumping when mothers and infants are separated, and we offer alternatives to the bottle (syringe and finger feeding). We educate families about unique benefits of breast milk for preterm infants during our education to staff and families and have specific policies for preterm infants including skin-to-skin kangaroo care. These practices were the only ones required for Baby-Friendly designation of a hospital with a NICU in 1999 in the United States. In addition (although this is not a Baby-Friendly requirement), we loan breast pumps to low-income women during the NICU course. 16 The implementation of these policies has not changed during this 10-year period.
One change that has occurred over this period is increased hospital support by international board certified lactation consultants (IBCLCs). In 1999, we had 0.4 IBCLC full-time equivalent (FTE) IBCLCs covering all areas of the hospital for the 2000 births per year, and by 2009 that coverage had increased to 2.5 FTE for our increased, 2500 births per year. Although BMC’s IBCLCs work with NICU mothers during the immediate postpartum period and train NICU nurses to support mothers in breastfeeding, we do not have IBCLCs dedicated to the NICU.
Statistical Analysis
We examined differences in participant characteristics according to year of NICU admission (1999 and 2009) using chi-square tests. Then we examined differences in breastfeeding initiation among all mothers and black mothers using chi-square tests. We examined differences in breastfeeding exclusivity and any breastfeeding at 2 weeks and any breastfeeding at 6 weeks among infants still hospitalized at these time points in 1999 and 2009 using chi-square tests. A P value < .05 was considered statistically significant. Data were analyzed using STATA 12.0 (STATA Corporation, College Station, Texas, USA).
Results
The total number of infants analyzed in 1999 was 117 and, in 2007, 142 (Figure 1).
There were no statistically significant differences in the population studied between 1999 and 2009, except for birth weight (Table 1).
Participant Characteristics and Breastfeeding Initiation and Continuation at 2 Weeks of Life According to Year of Neonatal Intensive Care Unit (NICU) Admission
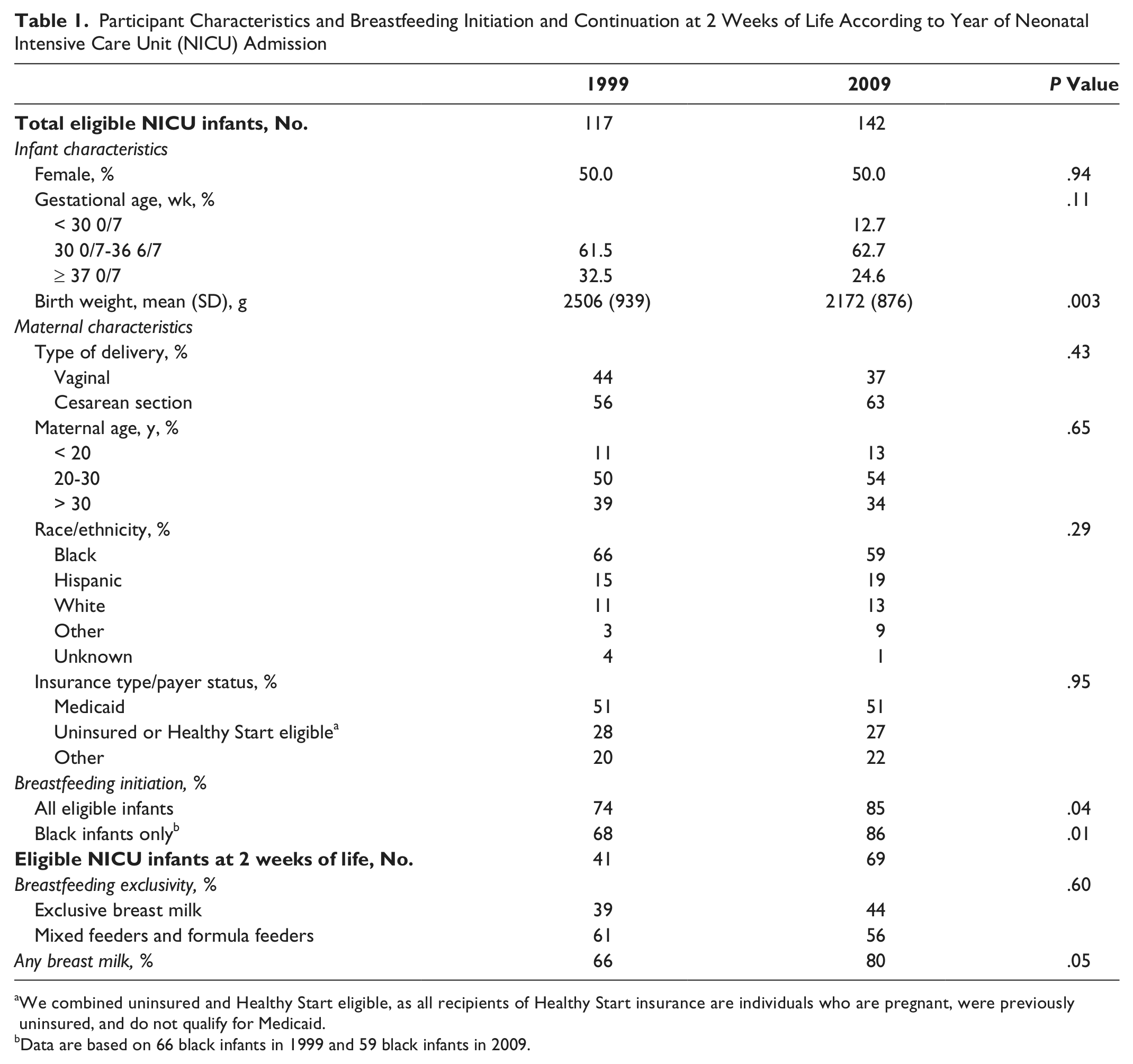
We combined uninsured and Healthy Start eligible, as all recipients of Healthy Start insurance are individuals who are pregnant, were previously uninsured, and do not qualify for Medicaid.
Data are based on 66 black infants in 1999 and 59 black infants in 2009.
Breastfeeding initiation increased from 74% to 85% among all infants (P = .04) and from 68% to 86% among black infants (P = .01), from 1999 to 2009, respectively (Table 1). In 1999, 41 infants (35%) remained in the NICU after 2 weeks, and in 2009, 69 (49%) remained in the NICU at 2 weeks. Any breast milk at 2 weeks of age increased from 66% to 80% (P = .05), and breastfeeding exclusivity at 2 weeks remained stable. At 6 weeks of age, only 9 infants remained in the NICU in 1999 and 24 in 2009. We found that 67% received any breast milk in 1999 compared to 54% in 2009, and we did not analyze with chi-square because of small sample sizes.
Discussion
During a 10-year period of Baby-Friendly certification at our inner-city teaching hospital, breastfeeding initiation and any breastfeeding at 2 weeks of age continued to improve, and breastfeeding exclusivity at 2 weeks of age was sustained among NICU infants. The increase in breastfeeding initiation was particularly significant among black infants. This is an important finding, as the rate of preterm birth is highest 17 and breastfeeding rates are lowest among black infants 18 compared to other racial/ethnic groups in the United States.
A limitation of this study is that we cannot measure the impact of specific factors that may have affected changes. Baby-Friendly designation does not require or depend specifically on IBCLC support, but it is likely that increased IBCLC coverage has helped to raise breastfeeding rates; however, increased IBCLC coverage is itself an outcome of Baby-Friendly certification. More women at BMC are now breastfeeding,8,19,20 and thus more support is needed in all areas to manage the increased numbers of women requiring breastfeeding support. In addition, limitations of our data meant that we were not able to perform logistic regression controlling for confounders. Longer term follow-up beyond NICU discharge would also be useful.
Strengths of our study include our ability to examine rates in predominantly black, Medicaid-eligible mother–infant pairs. We found the most dramatic increase in breastfeeding initiation after endorsement of Baby-Friendly policies in our NICU among black mothers, a group that has been shown to have the lowest breastfeeding initiation rates nationally. 18 This trend has continued, with ongoing significant increases in this racial group, and suggests that adherence to Baby-Friendly policies at other NICUs with similar disadvantaged populations may also be associated with increases in breastfeeding initiation. It is interesting that despite somewhat vague and nonspecific criteria for NICUs in US Baby-Friendly hospitals compared to other nations, the NICU in our Baby-Friendly hospital has demonstrated positive and sustainable breastfeeding outcomes since designation. More stringent criteria are being created internationally 13 ; presumably, applying these more proactive measures would have an even bigger impact on breastfeeding prevalence in the NICU.
Conclusion
Over a 10-year period in a US, inner-city, Baby-Friendly hospital, rates of breastfeeding initiation and any breastfeeding at 2 weeks continued to rise, especially among black infants. Improvement in rates of breastfeeding initiation and continuation in this setting can continue many years after the BFHI is first implemented.
Footnotes
Acknowledgements
We would like to acknowledge Marcy McMahon, Robin Humphreys, Roxanne Hyeck, Boston Medical Center, International Board Certified Lactation Consultants, and the BMC NICU nursing staff for their ongoing support for breastfeeding, as well as Gregory Makrigiorgos and Georgina Toledo for their help with data collection.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for the study was provided by the Department of Pediatrics at Boston Medical Center.