
Abstract
Background:
The Baby-Friendly Hospital Initiative requires hospitals to pay market price for infant formula. No studies have specifically examined the effect of hospitals paying for infant formula on breastfeeding mothers’ exposure to Baby-Friendly steps.
Objectives:
To investigate the effect of hospitals implementing a policy of paying for infant formula on new mothers’ exposure to Baby-Friendly steps and examine the effect of exposure to Baby-Friendly steps on breastfeeding rates.
Methods:
We used a repeated prospective cohort study design. We recruited 2 cohorts of breastfeeding mother–infant pairs (n = 2470) in the immediate postnatal period from 4 Hong Kong public hospitals and followed them by telephone up to 12 months postpartum. We assessed participants’ exposure to 6 Baby-Friendly steps by extracting data from the medical record and by maternal self-report.
Results:
After hospitals began paying for infant formula, new mothers were more likely to experience 4 out of 6 Baby-Friendly steps. Breastfeeding initiation within the first hour increased from 28.7% to 45%, and in-hospital exclusive breastfeeding rates increased from 17.9% to 41.4%. The proportion of mothers who experienced all 6 Baby-Friendly steps increased from 4.8% to 20.5%. The risk of weaning was progressively higher among participants experiencing fewer Baby-Friendly steps. Each additional step experienced by new mothers decreased the risk of breastfeeding cessation by 8% (hazard ratio = 0.92; 95% CI, 0.89-0.95).
Conclusion:
After implementing a policy of paying for infant formula, breastfeeding mothers were exposed to more Baby-Friendly steps, and exposure to more steps was significantly associated with a lower risk of breastfeeding cessation.
Well Established
Hospital practices consistent with the 10 steps of the Baby-Friendly Hospital Initiative (BFHI) improve breastfeeding rates. The BFHI recommends that hospitals pay fair market price for infant formula products as discounted or free products may contribute to the unnecessary supplementation of breastfeeding newborns.
Newly Expressed
After public hospitals began paying for infant formula products, there was improvement in the number of Baby-Friendly steps that mothers experienced. A strong dose-response relationship was found between the number of Baby-Friendly steps experienced and breastfeeding duration.
Background
Breastfeeding provides optimal nutrition for the growth and development of infants, with benefits proportional to the exclusiveness and duration of breastfeeding. 1 Although both the American Academy of Pediatrics 1 and the World Health Organization (WHO) 2 recommend exclusive breastfeeding for the first 6 months of life, only about one-third of infants globally are exclusively breastfed for the first 4 months. 1 Early cessation is common among mothers in industrialized countries who initiate breastfeeding, as is early and regular supplementation of breastfeeding with infant formula,3-5 both of which substantially increase the risk of numerous adverse infant health outcomes. 6 Hospital practices remain a significant barrier to exclusive breastfeeding.7-10 Even with normal birth, breastfeeding initiation is often delayed, separation of mother and baby is common, breastfeeding support is inadequate, and a large proportion of infants is given supplemental formula.4,11
To counteract these negative influences on breastfeeding, in 1991 the WHO and the United Nations Children’s Fund (UNICEF) developed the Baby-Friendly Hospital Initiative (BFHI), which outlines 10 steps that hospitals must comply with to be designated as Baby-Friendly. 12 Numerous studies have found that the BFHI has a positive effect on the duration of breastfeeding, both at local13-15 and national levels. 16 In addition, others have found that although Baby-Friendly designation itself does not improve breastfeeding rates in developed countries with high breastfeeding initiation rates,17-19 mothers who are exposed to more Baby-Friendly steps have higher rates of both any and exclusive breastfeeding.10,17,20,21 A significant concern of the BFHI is ensuring compliance with the International Code of Marketing of Breast-milk Substitutes, 22 which prohibits the promotion and marketing of artificial milks to mothers within health care facilities. The BFHI stipulates that hospitals should not accept free or heavily discounted infant formula products from manufacturers and that they must pay market price for all breast milk substitutes. 23 Hospitals’ acceptance of free infant formula encourages and promotes non–medically indicated supplementation,24,25 which in turn shortens the overall duration of breastfeeding and negatively affects exclusive breastfeeding rates.4,11
In Hong Kong, a city with modern health care facilities and comprehensive, publicly funded antenatal and postnatal obstetric services, over 85% of new mothers now initiate breastfeeding in the immediate postnatal period. 26 However, as in many other industrialized countries, 27 breastfeeding duration is short, and exclusive breastfeeding rates are low. 28 Only about one-third of Hong Kong infants are still receiving any breast milk at 6 months of age. 29 The short duration of breastfeeding has been attributed to a number of influencing factors, such as high female workforce participation rates and short maternity leave, 30 a lack of family and community support for breastfeeding, 31 and suboptimal hospital practices that delay the initiation of breastfeeding and encourage formula supplementation.4,20 Hong Kong has 8 public and 10 private hospitals that offer obstetric services, none of which have been designated Baby-Friendly. In 2011, 67.8% of all births in Hong Kong took place in public hospitals. 32 The Hong Kong Hospital Authority (HA), a subvented government organization, manages all public hospitals, and various charitable, philanthropic, and religious organizations manage the private hospitals. Both public and private hospitals in Hong Kong have accepted free infant formula products from manufacturers. In 2006, the HA announced that all public hospitals would begin purchasing infant formula products at market price as an initial step toward hospitals becoming more Baby-Friendly. Ending the supply of free formula is often the most difficult step for hospitals to take, but it can result in more judicious use of infant formula.33,34 In addition, such a measure would necessitate the improvement of other hospital practices that support breastfeeding. To our knowledge, no other study has examined the effect of hospitals implementing a policy of paying for infant formula on Baby-Friendly hospital steps. Thus, the aims of this study were to (1) compare new mothers’ exposure to Baby-Friendly steps before and after public hospitals implemented a policy of paying for infant formula and (2) assess the association between new mothers’ exposure to Baby-Friendly steps and the duration of any and exclusive breastfeeding.
Methods
Design, Setting, and Participants
We used a repeated prospective cohort study design to evaluate exposure to Baby-Friendly steps and breastfeeding rates before and after hospitals began paying for infant formula. We recruited 2 cohorts of mother-infant pairs from 4 geographically and socioeconomically distributed public hospitals in Hong Kong (2 hospitals from Hong Kong Island and 2 from the Kowloon Peninsula) and followed them prospectively for up to 1 year or until weaned, whichever was first. The first cohort of 1417 mother-infant pairs was recruited during 2006 to 2007, prior to the planned implementation of the infant formula payment policy in April 2007. However, a sudden and large influx of mainland Chinese mothers coming to Hong Kong to give birth placed substantial constraints on the obstetric services in Hong Kong hospitals, 35 and the infant formula policy implementation was delayed until April 2010. The second cohort of 1287 mother-infant pairs was recruited from the same 4 hospitals from 2011 to 2012, after the infant formula payment policy was implemented, and served as the post-intervention group.
The participant selection criteria and data collection procedures were identical in both cohorts. Participant selection criteria were as follows: (1) intention to breastfeed, (2) singleton pregnancy, (3) Cantonese speaking, and (4) no serious medical or obstetrical complications. Participants planning to exclusively formula feed were not recruited. Participants were excluded from the study if they failed to meet these criteria and/or if their baby: (1) was born at < 37 weeks gestation, (2) had an Apgar score < 8 at 5 minutes, (3) had a birth weight < 2500 grams, (4) was born with any severe medical conditions or congenital malformations, (5) was placed in the special care nursery for > 48 hours after delivery, or (6) was placed in the neonatal intensive care unit after delivery.
Data Collection and Measurements
A trained research nurse recruited participants from the postnatal wards of the participating hospitals in the immediate postnatal period. In-hospital data collection consisted of baseline demographic data, maternal and infant data, exposure to 6 of the 10 Baby-Friendly steps (except Step 10), and in-hospital infant feeding data. Follow-up infant feeding data were collected by telephone at 1, 2, 3, 6, 9, and 12 months postpartum or until weaned. Demographic data were collected by maternal self-report using a self-administered questionnaire. The research nurse extracted the relevant maternal, birth, and infant feeding data, including exposure to Baby-Friendly steps, from the medical record and validated it with the participants. The 6 Baby-Friendly steps measured included (1) Step 4: help mothers to initiate breastfeeding within the first hour after birth; (2) Step 6: give newborn infants no food or drink other than breast milk, unless medically indicated; (3) Step 7: practice rooming-in; (4) Step 8: encourage breastfeeding on demand; (5) Step 9: give breastfeeding babies no artificial teats or pacifiers; and (6) Step 10: provide mothers with information about breastfeeding support upon discharge. These 6 steps were chosen as they are steps that affect individual mothers. Steps 1 and 2 apply to the hospital, and Step 3 would normally occur during the antenatal period. We also measured Step 5 (show mothers how to breastfeed and maintain lactation), but similar to other researchers, 10 the data suggested that exposure to this step was an indicator of women experiencing breastfeeding difficulties rather than the demonstration of breastfeeding to all new mothers. Therefore, we excluded this step from the analysis.
In-hospital infant feeding data were extracted from the newborn’s intake and output record kept at the bedside. Both the mother and the nurses make entries on the intake and output records, and the ward midwives routinely validate the entries with the patients at least once per 8-hour shift. Since most new mothers are discharged after 48 hours, in-hospital feeding status was based on the infant’s intake for the first 48 hours only. After hospital discharge, a trained study research assistant contacted participants by telephone at the prescribed follow-up time points to assess the infant feeding status. Participants were asked about the type and frequency of liquid feeds given to the infant in the 24-hour period before the interview. 36 If the participant had weaned during that follow-up interval, she was asked to report the total duration (in weeks) of both any and exclusive breastfeeding. Information relevant to Step 10 (refer mothers to breastfeeding support groups on discharge from hospital) was reported by the participants during the first telephone follow-up interview after hospital discharge, normally at 1 month postpartum.
In accordance with WHO definitions, infants were considered exclusively breastfed if they received no solids, no non–breast milk substitutes, and no water or other liquids (apart from vitamins or medications). 36 In the combined sample, we also assessed the effect of exposure to Baby-Friendly steps on the duration of any breastfeeding and exclusive breastfeeding. The classification of exclusive breastfeeding duration was based on the reported infant feeding method after hospital discharge and did not include formula given while in the hospital. 9
Statistical Analysis
Descriptive statistics were used to summarize and compare the sociodemographic characteristics of the 2 study cohorts. To assess our first study aim, we used chi-square statistics to compare the participants’ exposure to the 6 Baby-Friendly steps before and after the implementation of the infant formula payment policy. Because of differences in the sociodemographic characteristics of the 2 cohorts, we performed unadjusted and adjusted logistic regression analyses to compute the odds ratios (ORs) of exposure to each Baby-Friendly step in Cohort 2, with Cohort 1 serving as the reference group. In addition, we compared the time to first breastfeed between the 2 cohorts using Kaplan-Meier failure curves. For our second study aim, we combined the data from both study cohorts and performed unadjusted and adjusted Cox proportional hazards regression to assess the association between the individual and the total number of Baby-Friendly steps experienced by participants and the duration of any and exclusive breastfeeding. The proportional hazards assumption was tested by assessing the log-log plot of Kaplan-Meier survival curves. Using an unadjusted parametric survival model, we also predicted the median number of weeks of any and exclusive breastfeeding in weeks attributable to exposure to the individual and cumulative Baby-Friendly steps. In all multivariable models, adjustment was made for those key sociodemographic variables that were significantly different between the 2 cohorts (P < .05) and for factors that have been previously shown to affect breastfeeding rates in this population.28,37 All Kaplan-Meier curves were compared using the log-rank test of equality or the test for trend of survivor functions, whichever was most appropriate. 38 For all analyses, the duration of breastfeeding in participants who were lost to follow-up was censored at the time of last contact.
Ethical approval for the study was obtained from the Institutional Review Board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster and the participating study sites. Informed written consent was obtained from all participants. All data were analyzed using Stata version 13.1 statistical software (StataCorp LP, College Station, Texas, USA). 39 A 5% level of significance was used in all statistical tests.
Results
From June 2006 to July 2007, we recruited 1417 mother-infant pairs from 4 study sites to form the baseline sample (Cohort 1). After recruitment, we excluded 10 participants because they subsequently did not meet the study eligibility criteria (ie, the baby was transferred to the neonatal intensive care unit), 87 participants with whom we had no further contact after hospitalization, and 58 participants with missing data relevant to the analysis, leaving a total 1262 (89.1%) participants in the final analysis for Cohort 1. Of these 1262 participants, 31 (2.5%) had partial follow-up, and 1231 (97.5%) had complete follow-up. After the implementation of the infant formula payment policy, we recruited a second cohort (Cohort 2) of 1287 mother-infant pairs from the same 4 hospitals between October 2011 and July 2012. After recruitment of Cohort 2, we excluded 10 participants because they subsequently did not meet the study criteria, 37 (2.9%) participants with whom we had no further contact after hospitalization, and 32 participants with relevant missing data. This left a total of 1208 (93.9%) participants in the final analysis for Cohort 2. Of these 1208 participants, 36 (3%) had partial follow-up, and 1201 (97%) participants had complete follow-up. A total of 2470 mother-infant pairs from both cohorts were included in the analysis.
A comparison of the characteristics of the 2 cohorts is presented in Table 1. Participant ages and education levels were similar in the 2 cohorts. Participants in Cohort 1 were more likely to be primiparous and to have no previous breastfeeding experience and less likely to plan to exclusively breastfeed. Cohort 1 participants were also more likely to have attended antenatal childbirth and breastfeeding classes and to be returning to work within 6 months after childbirth. The husbands of participants in Cohort 1 were also more likely to prefer exclusive breastfeeding for the infant.
Comparison of the Characteristics of the 2 Study Cohorts.
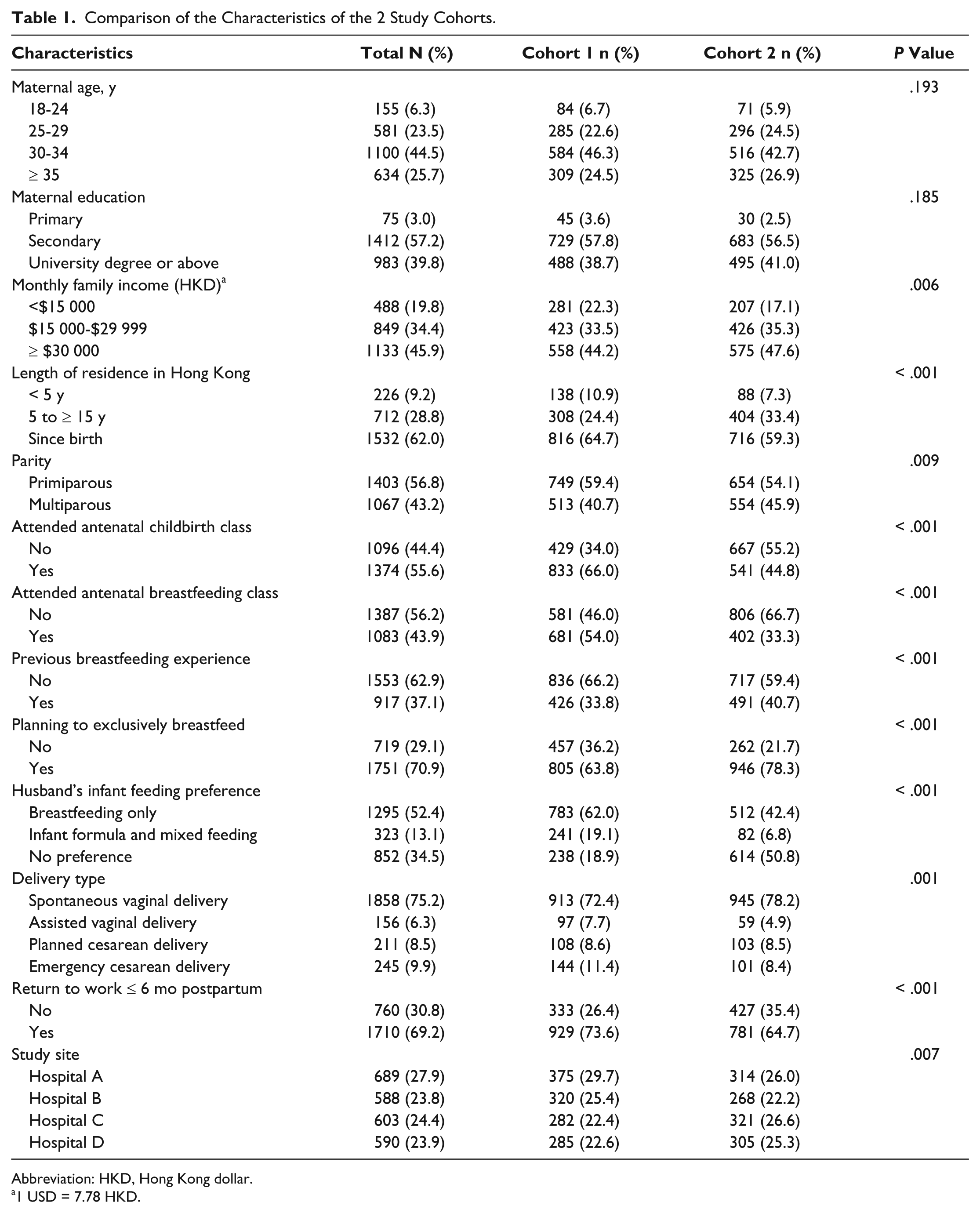
Abbreviation: HKD, Hong Kong dollar.
1 USD = 7.78 HKD.
The prevalence of the 6 measured Baby-Friendly steps that mothers were exposed to in-hospital before and after the implementation of the infant formula payment policy is presented in Table 2. A significantly higher proportion of infants in Cohort 2 were breastfed within 1 hour of birth (45% vs 28.7%; adjusted odds ratio [aOR] = 2.04; 95% CI, 1.61-2.59), given only breast milk in the hospital (41.4% vs 17.9%; aOR = 1.45; 95% CI, 1.07-1.96), and not given artificial teats or nipples (78.1% vs 58.4%; aOR = 6.02; 95% CI, 4.06-8.94). A significantly higher proportion of mothers reported that they were provided information about breastfeeding support options after discharge from the hospital (85.6% vs 75.8%; aOR = 2.14; 95% CI, 1.63-2.82). Rates of rooming-in and breastfeeding on demand did not change significantly between the 2 time periods.
Breastfeeding Mothers’ Exposure to 6 Baby-Friendly Steps by Study Cohort.
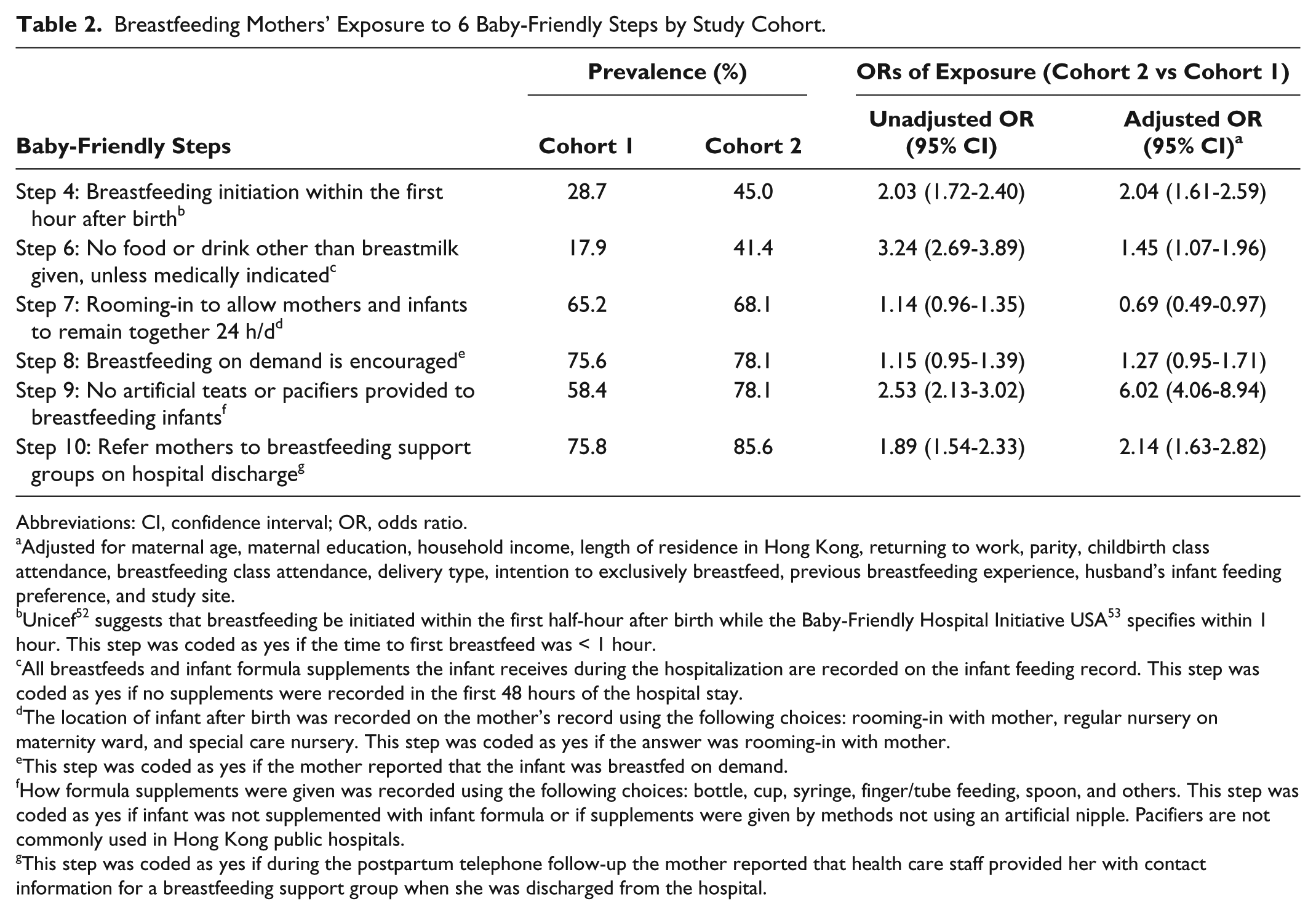
Abbreviations: CI, confidence interval; OR, odds ratio.
Adjusted for maternal age, maternal education, household income, length of residence in Hong Kong, returning to work, parity, childbirth class attendance, breastfeeding class attendance, delivery type, intention to exclusively breastfeed, previous breastfeeding experience, husband’s infant feeding preference, and study site.
Unicef 52 suggests that breastfeeding be initiated within the first half-hour after birth while the Baby-Friendly Hospital Initiative USA 53 specifies within 1 hour. This step was coded as yes if the time to first breastfeed was < 1 hour.
All breastfeeds and infant formula supplements the infant receives during the hospitalization are recorded on the infant feeding record. This step was coded as yes if no supplements were recorded in the first 48 hours of the hospital stay.
The location of infant after birth was recorded on the mother’s record using the following choices: rooming-in with mother, regular nursery on maternity ward, and special care nursery. This step was coded as yes if the answer was rooming-in with mother.
This step was coded as yes if the mother reported that the infant was breastfed on demand.
How formula supplements were given was recorded using the following choices: bottle, cup, syringe, finger/tube feeding, spoon, and others. This step was coded as yes if infant was not supplemented with infant formula or if supplements were given by methods not using an artificial nipple. Pacifiers are not commonly used in Hong Kong public hospitals.
This step was coded as yes if during the postpartum telephone follow-up the mother reported that health care staff provided her with contact information for a breastfeeding support group when she was discharged from the hospital.
The overall median time to initiation of the first breastfeeding decreased from 3.0 hours in Cohort 1 to 1.5 hours in Cohort 2 (P < .001). Furthermore, the median time to initiation of the first breastfeed among participants undergoing vaginal delivery decreased from 2 hours to 1 hour (P < .001) and for cesarean delivery decreased from 23 hours in Cohort 1 to 4 hours in Cohort 2 (P < .001) (Figure 1). Figure 2 shows the total number of Baby-Friendly steps that participants in each cohort were exposed to during the hospital stay. When compared with Cohort 1, participants in Cohort 2 were significantly more likely to experience all 6 Baby-Friendly steps (20.5% vs 4.8%; aOR = 11.7; 95% CI, 6.63-20.5).
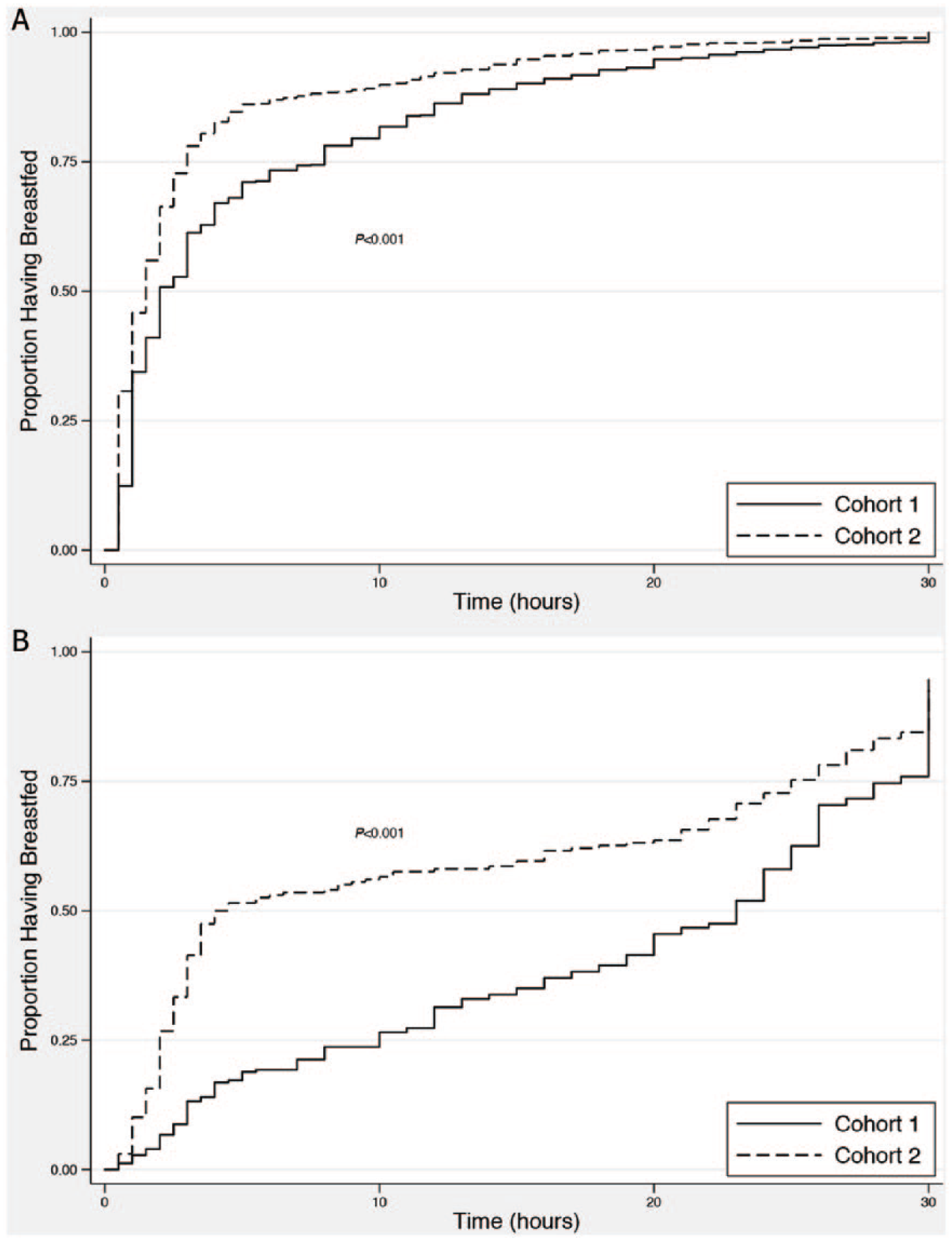
Time to the Initiation of the First Breastfeed by Study Cohort for (A) Vaginal and (B) Cesarean Birth.
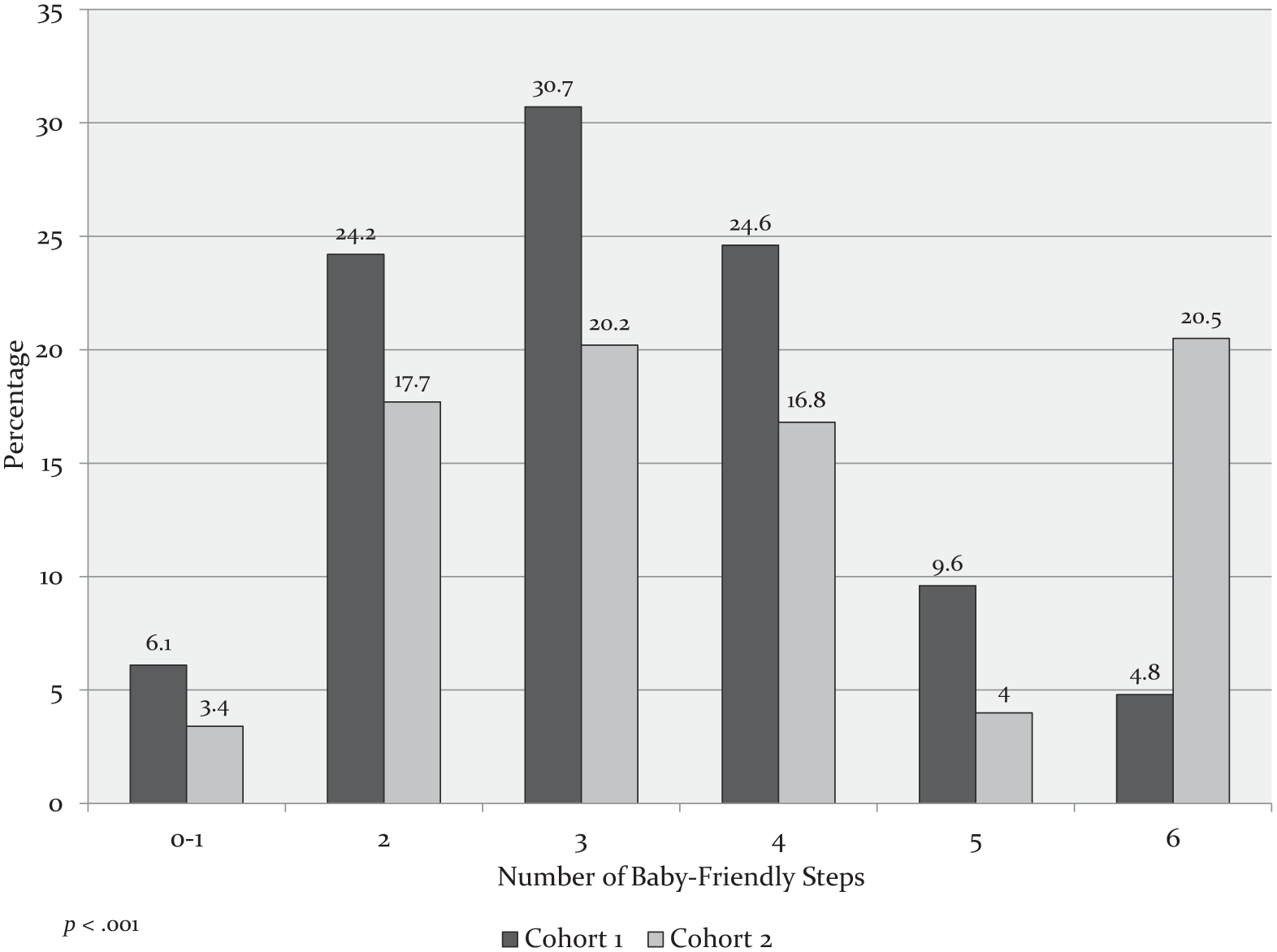
Number of Baby-Friendly Steps Experienced by Participants in Each Study Cohort.
Table 3 shows the associations between the individual Baby-Friendly steps and the risk of stopping any and exclusive breastfeeding. In the fully adjusted model, breastfeeding initiation within the first hour after birth (Step 4) was significantly associated with a lower risk of stopping breastfeeding, and exposed participants breastfed for approximately 5 additional weeks (15.5 weeks vs 10.9 weeks). In addition, receiving only breast milk while in the hospital (Step 6) was significantly associated with a lower risk of stopping any and exclusive breastfeeding. Participants exposed to Step 6 breastfed for approximately 10 additional weeks (19.8 weeks vs 10.2 weeks) when compared with those who were not exposed.
Association between Exposure to Baby-Friendly Steps and Risk of Stopping Any and Exclusive Breastfeeding.
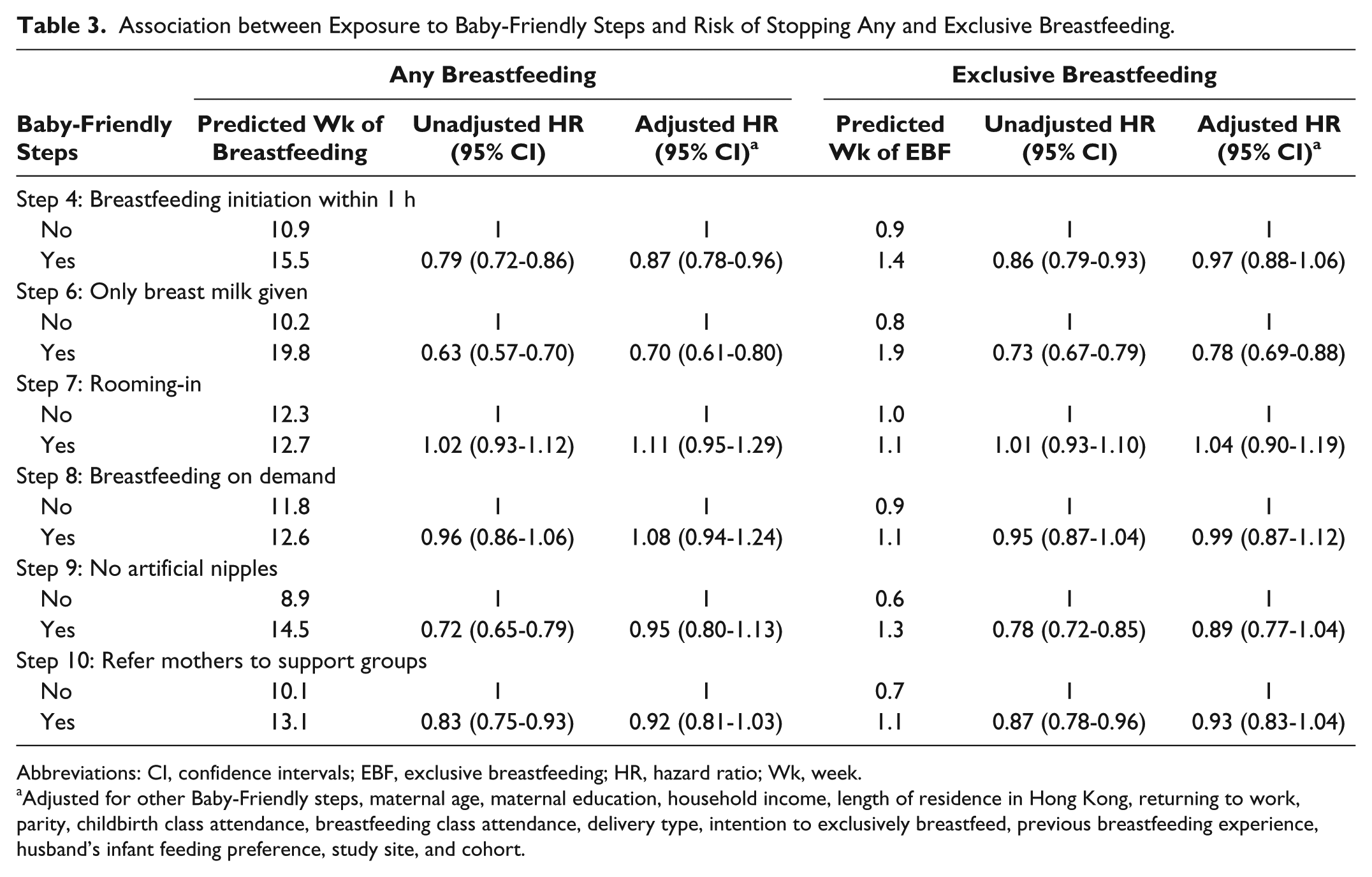
Abbreviations: CI, confidence intervals; EBF, exclusive breastfeeding; HR, hazard ratio; Wk, week.
Adjusted for other Baby-Friendly steps, maternal age, maternal education, household income, length of residence in Hong Kong, returning to work, parity, childbirth class attendance, breastfeeding class attendance, delivery type, intention to exclusively breastfeed, previous breastfeeding experience, husband’s infant feeding preference, study site, and cohort.
Kaplan-Meier curves show the association between the number of Baby-Friendly steps experienced and the duration of both any and exclusive breastfeeding (Figure 3). When compared with mothers who were exposed to all 6 Baby-Friendly steps, the duration of both any and exclusive breastfeeding was progressively shorter among participants experiencing fewer Baby-Friendly steps. After adjustment for potential confounders, the relationship decreased slightly, but the association between the number of Baby-Friendly steps experienced and breastfeeding duration remained (Table 4). When compared with participants who experienced all 6 Baby-Friendly steps, those who experienced 0 or only 1 step had almost double the risk of weaning from any breastfeeding (hazard ratio [HR] = 1.78; 95% CI, 1.39-2.28) and almost a 50% increase in the risk of weaning from exclusive breastfeeding (HR = 1.42; 95% CI, 1.13-1.79). Participants exposed to all 6 Baby-Friendly steps breastfeed 3 times longer than those who were exposed to ≤ 1 step (21 weeks vs 7.1 weeks). Finally, when compared with the group exposed to 0 or only 1 Baby-Friendly step, after adjustment for confounding variables, with each additional Baby-Friendly step experienced, the risk of weaning from any breastfeeding decreased by 8% (HR = 0.92; 95% CI, 0.89-0.95) and from exclusive breastfeeding by 7% (HR = 0.93; 95% CI, 0.91-0.96). The log–log plots for all Cox regression models showed that the proportional-hazards assumption was not violated.
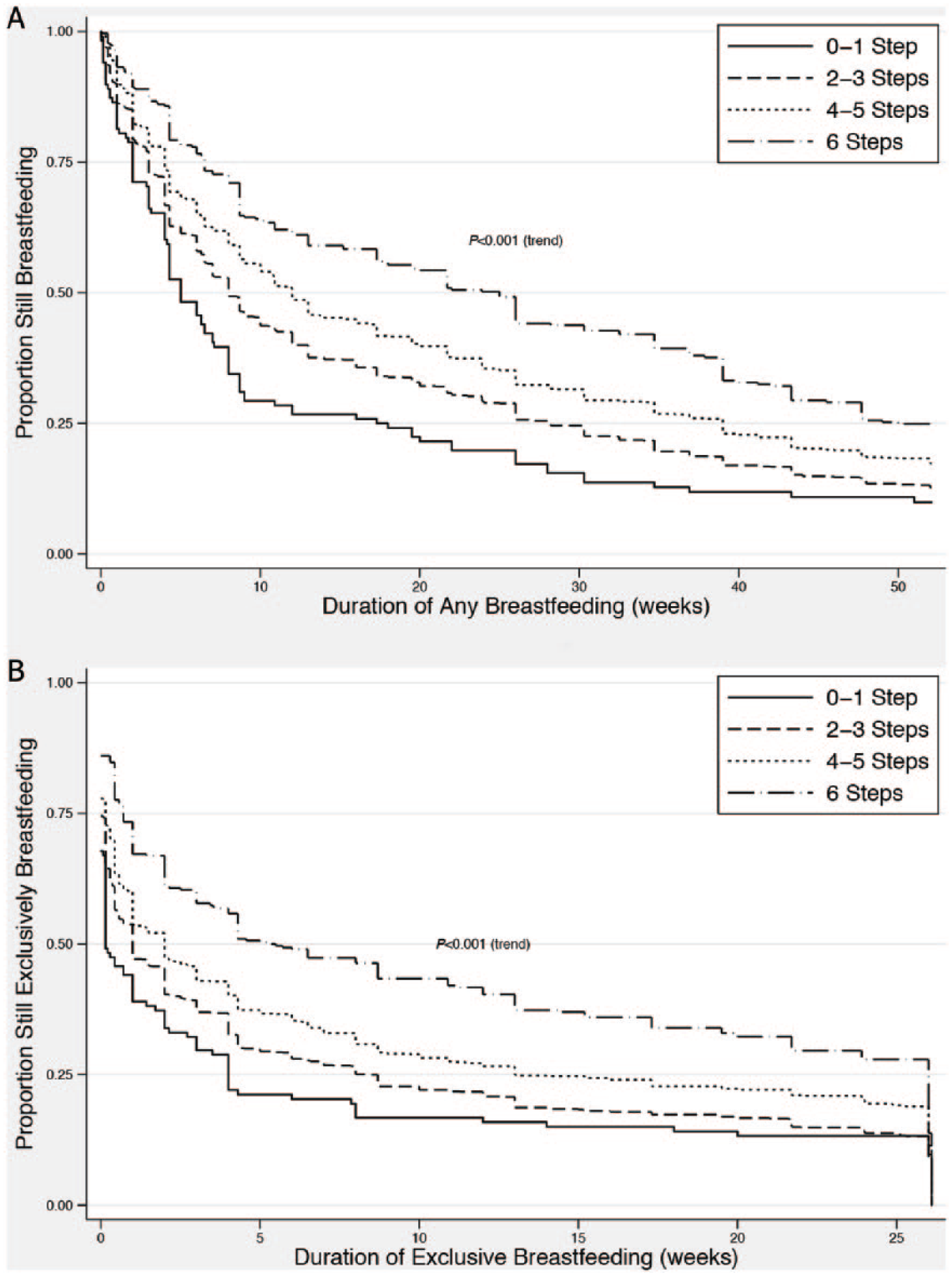
Exposure to Baby-Friendly Steps and the Risk of Cessation of (A) Any and (B) Exclusive Breastfeeding.
Association between the Number of Baby-Friendly Steps Experienced and Risk of Stopping Any and Exclusive Breastfeeding.
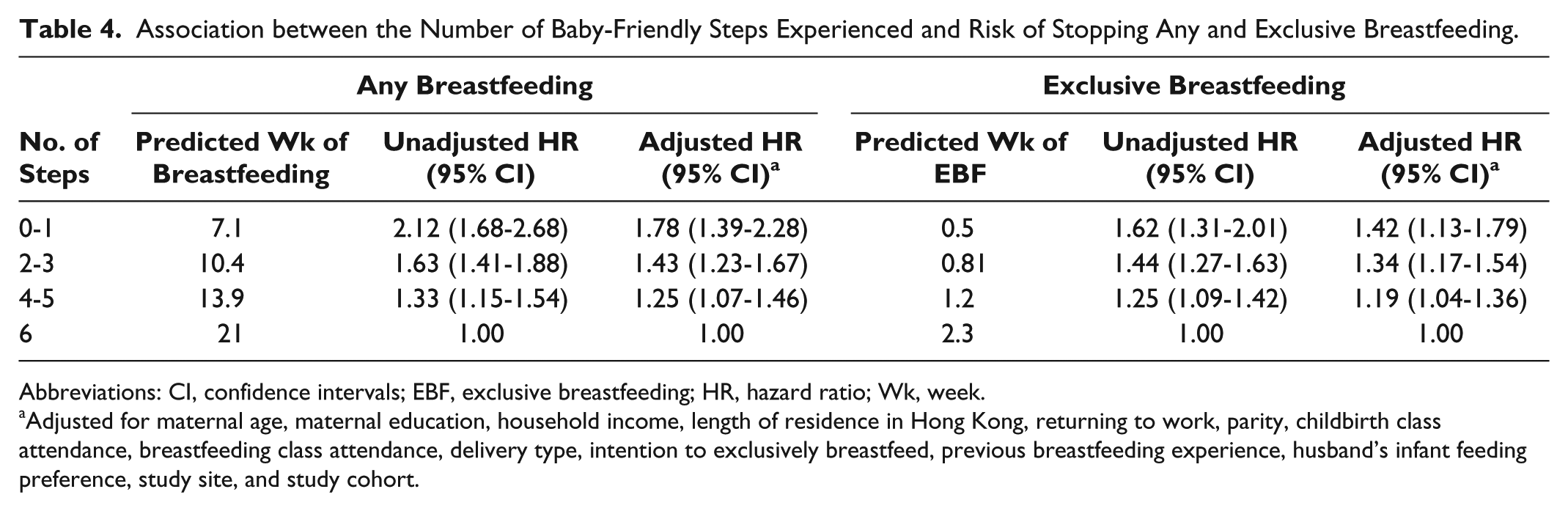
Abbreviations: CI, confidence intervals; EBF, exclusive breastfeeding; HR, hazard ratio; Wk, week.
Adjusted for maternal age, maternal education, household income, length of residence in Hong Kong, returning to work, parity, childbirth class attendance, breastfeeding class attendance, delivery type, intention to exclusively breastfeed, previous breastfeeding experience, husband’s infant feeding preference, study site, and study cohort.
Discussion
Mothers giving birth in Hong Kong public hospitals after the implementation of a policy to pay market price for infant formula were substantially more likely to initiate breastfeeding within the first hour after birth (Step 4), more likely to exclusively breastfeed during hospitalization (Step 6), more likely to not be given an artificial nipple (Step 9), and more likely to receive information about breastfeeding support upon hospital discharge (Step 10). Furthermore, participants in Cohort 2 were significantly more likely to be exposed to all 6 Baby-Friendly steps. However, even in Cohort 2, only one-fifth of participants were exposed to 6 Baby-Friendly steps, and over 20% were exposed to 2 or fewer steps, indicating that further improvement in hospital practices is necessary to create a more supportive environment for breastfeeding mothers.
After the implementation of the infant formula payment policy, a significantly higher proportion of infants was given only breast milk, suggesting that the elimination of free infant formula supplies may help to increase in-hospital exclusive breastfeeding rates. The provision of free or discounted infant formula products to health care institutions by infant formula manufacturers is an effective marketing strategy.34,40 There are strong financial incentives for manufacturers to undermine breastfeeding by ensuring that breastfeeding infants receive infant formula as early as possible. 41 Studies show that breastfeeding newborns that receive in-hospital formula supplements have significantly shorter breastfeeding duration than exclusively breastfed infants.4,11
Another important finding was the substantial improvement in early initiation of breastfeeding from Cohort 1 to Cohort 2 among participants undergoing operative deliveries. The median duration of the time to first breastfeed decreased from 23 hours to 4 hours, a notable improvement. The first hour after birth is crucial for initiating breastfeeding as this is the time when infants are most alert and their natural instincts facilitate breastfeeding. 42 An operative delivery can impede early breastfeeding initiation because it affects the neurobehavioral state of the neonate by increasing lethargy and suppressing natural sucking reflexes.42,43 Additionally, surgical deliveries and the resulting prolonged separation of mother and infant owing to anesthesia and postoperative recovery impedes early breastfeeding and contributes to delayed lactogenesis.44,45 Therefore, early breastfeeding initiation after operative deliveries may reduce the need for and the frequency of formula supplementation.
Consistent with previous studies,10,17 we found an association between exposure to Baby-Friendly steps and a lower risk of breastfeeding cessation. When examining the relationship between the individual Baby-Friendly steps and breastfeeding cessation, Step 6 had the strongest association. This is consistent with other studies10,20,46 and again reinforces the importance of avoiding unnecessary infant formula supplementation and supporting exclusive breastfeeding.4,11 Although our data failed to show a significant relationship between 4 of the 6 individual Baby-Friendly steps and breastfeeding duration, we were able to show a clear dose-response association between the number of steps and the risk of breastfeeding cessation. Participants who were exposed to ≤ 1 Baby-Friendly step had almost double the risk of breastfeeding cessation than participants who were exposed to all 6 Baby-Friendly steps. This finding provides further support to the findings of other studies10,17,20,46 that in populations with high breastfeeding attrition, exposure to Baby-Friendly steps may improve breastfeeding rates.
This study has several strengths. To our knowledge, this is the first study to examine the effect of hospitals implementing a policy to pay market price for infant formula products on new mothers’ exposure to Baby-Friendly steps. Thus, study findings support the BFHI position that hospital postnatal practices may substantially improve when these institutions pay market price for infant formula products. We had a relatively low dropout rate, and follow-up data were available for a high proportion of participants (92%). In addition, with the exception of Step 10, data on exposure to Baby-Friendly steps were collected during hospitalization and not assessed retrospectively, as is the case in most previous studies.10,17,46,47 This prospective data collection substantially reduced maternal recall bias.
However, there are some limitations to consider. First, our cohorts were not population based and thus may not be representative of the larger population. We do not have information on the total number of eligible participants and those who refused to participate. Mothers voluntarily participated in our study, and it is possible that women with more positive breastfeeding views were more likely to join the study. However, in-hospital exclusive breastfeeding rates and overall breastfeeding patterns in Cohort 2 are consistent with the most recent territory-wide survey of hospital practices 48 and breastfeeding rates in Hong Kong. 29 Second, breastfeeding duration was assessed by maternal self-report, and thus maternal recall bias is possible. However, recall bias is likely to be minimal as participants received regular and frequent telephone follow-up, and maternal reports of breastfeeding patterns are accurate for up to 20 years after the period of breastfeeding.49,50 Third, in-hospital infant feeding data were extracted from the infants’ intake and output records. While hospital policies are in place to help ensure the accuracy and completeness of the records, it is possible that errors or omissions on these records could lead to misclassification bias of the participants’ in-hospital infant feeding status (Step 6). Fourth, there were some baseline differences between our 2 cohorts, some of which predispose Cohort 2 to higher breastfeeding rates (ie, higher maternal education). Although we controlled for all of these variables in our multivariable analyses, it is possible that there is residual confounding that affected the study results. Finally, as this study investigated exposure to Baby-Friendly steps over 2 different time periods, the unanticipated extended interval between recruitment of the 2 study cohorts limits our ability to conclusively attribute the improvements in exposure to Baby-Friendly steps directly to the intervention. Although there were no territory-wide developments in breastfeeding education and/or promotion during the study interval, it is possible that hospitals would have become more Baby-Friendly over this time period, independent of any change in the payment system for infant formula products. However, another study from the same hospitals with the same participant selection criteria, in which breastfeeding data were collected immediately prior to the implementation of the infant formula payment policy in 2010, showed that there was no overall change in breastfeeding duration in the pre-policy implementation time interval. 51 In addition, the delay in the implementation of the infant formula payment policy did provide public hospitals with the necessary time to have a larger and broader discussion about the rationale for paying for infant formula and about how to become more Baby-Friendly.
Conclusion
After the implementation of the infant formula payment policy in Hong Kong public hospitals, there was a substantial improvement in the number of Baby-Friendly steps that new mothers experienced during the postnatal hospitalization. Adopting a policy of paying market price for infant formula products by hospitals is an important milestone in the process of becoming a more Baby-Friendly environment. Continued efforts by hospitals to become more Baby-Friendly would benefit mothers by supporting their breastfeeding goals and by assisting them to breastfeed longer. The process of attaining the Baby-Friendly designation, however, requires institutional commitment to the full implementation of the WHO guidelines and substantially higher compliance with the Baby-Friendly steps. In particular, hospitals will need to further improve rates of breastfeeding initiation within the first hour after birth and in-hospital exclusive breastfeeding rates.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Health and Medical Research Fund (Grant No. 05060721) from the Food and Health Bureau, Government of the Hong Kong Special Administration Region, the University of Hong Kong (Grant No. 10207306), the University of Hong Kong Strategic Research Theme of Public Health, and the School of Nursing, the University of Hong Kong.