
Abstract
Background:
Human immunodeficiency virus (HIV)–exposed uninfected (HEU) infants are a growing population in sub-Saharan Africa, with higher morbidity and mortality than HIV-unexposed infants. HEU infants may experience increased morbidity due to breastfeeding avoidance.
Objectives:
We sought to describe the burden and identify predictors of hospitalization among HEU infants in the first year of life.
Methods:
Using a retrospective cohort of HIV-infected mothers and their HEU infants in Nairobi, Kenya, we identified infants who were HIV-uninfected at birth and were followed monthly until their last negative HIV test, death, loss to follow-up, or study exit at 1 year of age. Incidence, timing, and reason for hospitalization was assessed overall as well as stratified by feeding method. Predictors of first infectious disease hospitalization were identified using competing risk regression, with HIV acquisition and death as competing risks.
Results:
Among 388 infants, 113 hospitalizations were reported (35/100 infant-years [the combined years of observation contributed by all infants in the study]; 95% confidence interval [CI], 29-42). Ninety hospitalizations were due to 1 or more infectious diseases (26/100 infant-years; 95% CI, 21-32)—primarily pneumonia (n = 40), gastroenteritis (n = 17), and sepsis (n = 14). Breastfeeding was associated with decreased risk of infectious disease hospitalization (subhazard ratio = 0.39; 95% CI, 0.24-0.64), as was time-updated nutrition status (subhazard ratio = 0.73; 95% CI, 0.61-0.89). Incidence of infectious disease hospitalization among formula-fed infants was 51/100 infant-years (95% CI, 37-70) compared to 19/100 infant-years (95% CI, 14-25) among breastfed infants.
Conclusion:
Among HEU infants, breastfeeding and nutrition status were associated with reduced hospitalization during the first year of life.
Well Established
Infant feeding recommendations for human immunodeficiency virus (HIV)–infected women must balance the benefits of breastfeeding against the risk of transmission of HIV via breast milk. World Health Organization guidelines have undergone several revisions and now recommend breastfeeding for HIV-infected mothers in resource-limited settings.
Newly Expressed
Among HIV-exposed uninfected infants in our retrospective Kenyan cohort, breastfeeding was associated with decreased risk of hospitalization due to infectious diseases in the first year of life. This decreased risk was observed among both exclusively breastfed and mixed-fed infants.
Background
An estimated 1.5 million human immunodeficiency virus (HIV)-infected women give birth in low- and middle-income countries annually. 1 In the absence of prevention of mother-to-child transmission (PMTCT) interventions, 30% to 45% of infants born to HIV-infected mothers will become infected 2 ; the remainder of children born to HIV-infected mothers are HIV-exposed uninfected (HEU). HEU children are a large and growing population, 3 particularly in sub-Saharan Africa where the HIV epidemic is concentrated. 1 As PMTCT programs become more accessible and successful, 1 the population of HEU children is expected to continue to grow. 3 Several studies have shown increased mortality among HEU infants in the first year of life.4 -8 HEU infants had increased risk of serious infections in the first year of life in a small South African study 9 and increased risk of hospitalization and severe febrile illness in the Ugandan PROMOTE study. 10 The ZVITAMBO trial in Zimbabwe found increased risk of sick-child visits to clinic throughout the first year for HEU infants, as well as increased risk of hospitalization in the neonatal period. 4
Increased morbidity and mortality among HEU infants may be due to a variety of maternal and infant immunologic and sociodemographic factors. 3 Breastfeeding avoidance by HIV-infected mothers in accordance with previous World Health Organization (WHO) guidelines, which recommended breastfeeding avoidance when alternative feeding was acceptable, feasible, affordable, sustainable, and safe (AFASS), 11 may also have contributed to poorer outcomes among HEU infants during the time that these guidelines were in effect. We evaluated incidence and predictors of hospitalization among Kenyan HEU infants in the first year of life, with an emphasis on the effects of infant feeding method and nutrition status.
Methods
The parent cohort study was approved by the University of Washington Institutional Review Board and the Kenyatta National Hospital Ethics and Research Committee. The current analysis was ruled exempt from ethics review as a secondary data analysis of a deidentified data set.
Study Design
We identified singleton and first-born twin infants who were confirmed to be HIV-uninfected at birth from a previously accrued cohort of HIV-infected mothers and their infants, details of which have been published previously.12 -14 Briefly, HIV-infected women were enrolled during pregnancy between 1999 and 2002 in Nairobi, Kenya, and followed until 1 year postpartum. Sociodemographic information was collected at enrollment and maternal CD4 count and log10 HIV viral load were assessed at 32 weeks gestation. Participants received short-course zidovudine for PMTCT as was standard care at the time of the study; mothers were counseled on infant feeding and the risk of HIV transmission via breast milk before electing to breastfeed or formula feed; for those choosing to breastfeed, exclusive breastfeeding for 6 months was recommended. Infants were examined by study physicians within 48 hours of delivery, at 2 weeks of age, and then monthly until 1 year of age. Clinical care was provided by study physicians at sick-child visits. During scheduled visits, infants underwent a detailed clinical exam and growth assessment, and mothers gave a history that included timing of and reason for hospitalization, as well as feeding method since the last visit.
Statistical Analysis
All analyses were conducted using Stata 14.0 (StataCorp, College Station, Texas, USA). Incidence and timing of (a) all-cause and (b) infectious disease hospitalization (IDH), including repeat hospitalizations, were assessed using maternal report and study physician referral records; infants contributed person-time until their last negative HIV test, death, loss to follow-up, or study exit. Incidence of IDH was also assessed, stratified by time-updated nutrition status (underweight vs not underweight) and by feeding method: infants exclusively breastfed to 6 months versus those never breastfed (formula-fed infants) and those who were breastfed for less than 6 months or had complementary feeding introduced before 6 months (mixed-fed infants). Univariate predictors of first IDH in the first year of life were identified using competing risk regression, with HIV acquisition and death as competing risks and robust standard errors. In sensitivity analyses, univariate predictors were adjusted for maternal HIV log10 viral load and CD4% at 32 weeks gestation, which were identified a priori as potential confounders. Dose-response by categorical predictors was assessed using a test for trend in survival functions. All predictors were assessed at baseline with the exception of infant growth and feeding information, which were collected longitudinally.
Infant growth and nutrition status were assessed by WHO weight-for-age Z-score (WAZ) and length-for-age Z-score (LAZ). WAZ < –2 was considered underweight and LAZ < –2 stunted. Growth information was time-updated to reflect the WAZ and LAZ at the most recent visit prior to the visit when mothers reported hospitalization or an infant was referred to hospital. Lagged WAZ and LAZ were used to avoid spurious associations due to acute weight loss accompanying the illness for which an infant was hospitalized. Feeding information was not time-updated in the main analysis; infants were considered breastfed throughout if mothers reported breastfeeding at 1 or more study visits, and formula fed if mothers never reported breastfeeding. Sensitivity analyses assessed the association between time-updated feeding method and hospitalization.
Results
Study Population
Mothers’ median age at enrollment was 25 years (interquartile range [IQR], 22-28); 90% were married, 70% did not work outside the home, and 30% were primiparous. At 32 weeks gestation, mothers’ median HIV viral load was 4.7 log10 copies/mL (IQR, 4.1-5.2), and median CD4 was 24% (IQR, 18-30). Of 388 HEU infants, 23 acquired HIV at a median of 33 days (IQR, 29-180) and 22 died at a median of 108 days (IQR, 73-149). Of the remaining 343 infants, 310 (91%) completed 12 months of follow-up. Seventy-six percent of infants were breastfed for a median of 273 days (IQR, 121-363). Mixed feeding was introduced at a median of 62 days (IQR, 15-153) for breastfed infants; only 36% of breastfed infants were exclusively breastfed until 6 months of age as recommended to HIV-infected mothers electing to breastfeed.
Burden and Causes of Hospitalization
Incidence of all-cause hospitalization was 35/100 infant-years (the combined years of observation contributed by all infants in the study; 95% confidence interval [CI], 29-42), representing 113 hospitalizations among 86 infants. Of the 113 hospitalizations, 38 were referrals by study physicians, and the remaining 75 were direct admissions to the hospital or referrals from other clinics. Incidence of hospitalization was highest in the first 3 months of life. Duration of hospitalization was available for 92 cases; median duration of hospitalization was 5 days (IQR, 3-10), and of 22 deaths in the cohort, 11 occurred among previously hospitalized children. Ninety hospitalizations among 70 infants were attributed to 1 or more infections (incidence 26/100 infant-years; 95% CI, 21-32)—primarily pneumonia (n = 40), sepsis (n = 18), and gastroenteritis (n = 17) (Figure 1). Fourteen hospitalizations were not due to infection; these were most commonly attributed to birth defects or birth complications (n = 5), and 9 had no cause recorded.
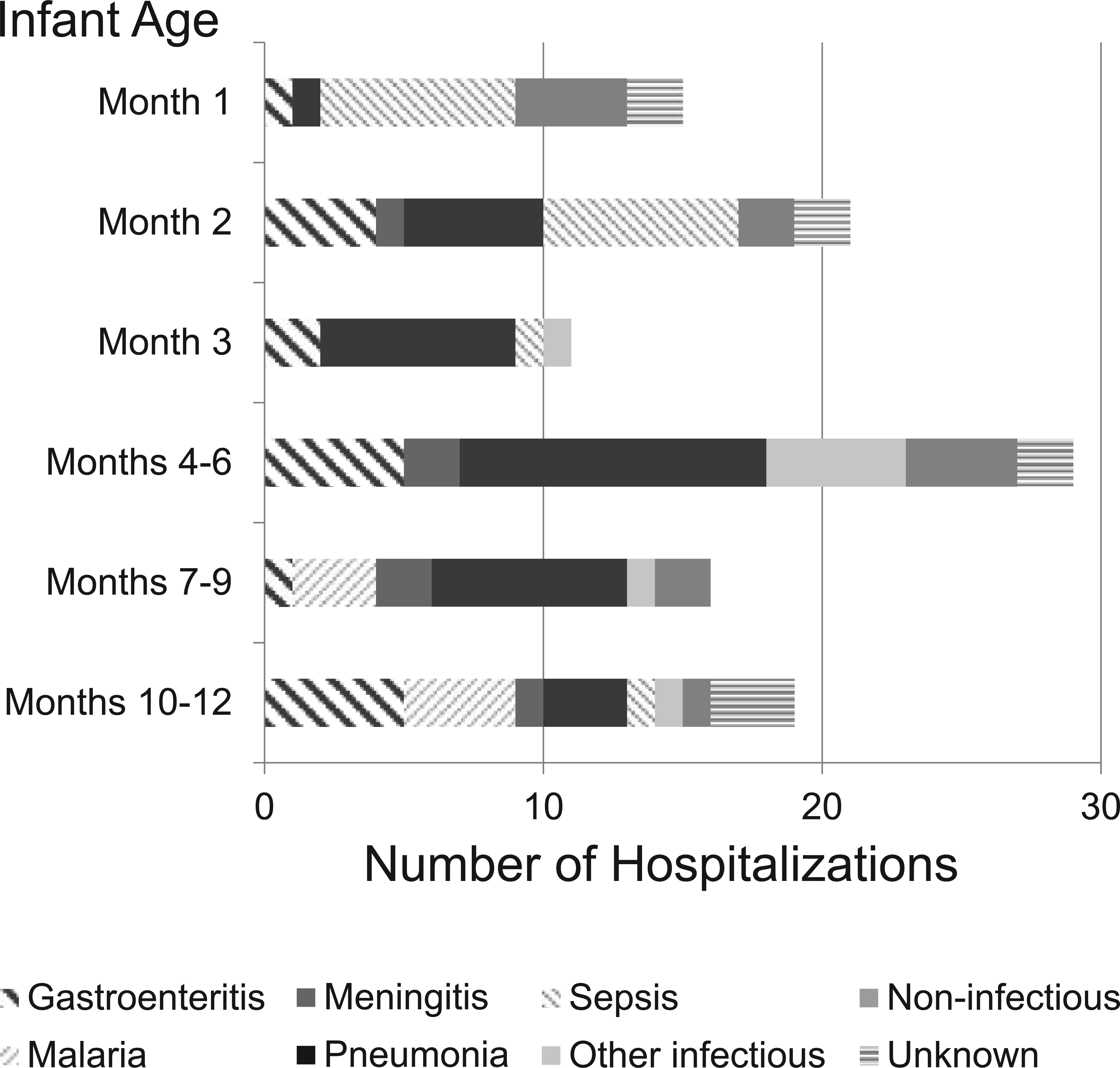
Frequency, Timing, and Primary Cause of Hospitalizations among 388 HIV-Exposed Uninfected Infants in the First Year of Life.
Competing Risk Regression
The analysis of IDH included 70 first hospitalizations and 16 competing events of infants dying or acquiring HIV without first being hospitalized. Maternal HIV log10 viral load and CD4% at 32 weeks gestation were not associated with IDH (Table 1), although greater than median viral load (> 4.7 log10 copies/mL) was associated with a trend toward increased IDH (subhazard ratio [SHR] = 1.5; 95% CI, 0.93-2.6). Preterm birth, low birth weight, and crowding in the home were not associated with IDH in the first year, although infants born preterm were at increased risk during the first 2 months (data not shown). Compared to formula feeding, ever breastfeeding was associated with a 61% decreased risk of IDH (SHR = 0.39; 95% CI, 0.24-0.64; P < .001). Similarly, in a sensitivity analysis considering time-updated feeding information, current breastfeeding was associated with a 62% reduced risk of IDH (SHR = 0.38; 95% CI, 0.22-0.65; P < .001).
Predictors of First Infectious Disease Hospitalization in the First Year of Life among HIV-Exposed Uninfected Infants. a
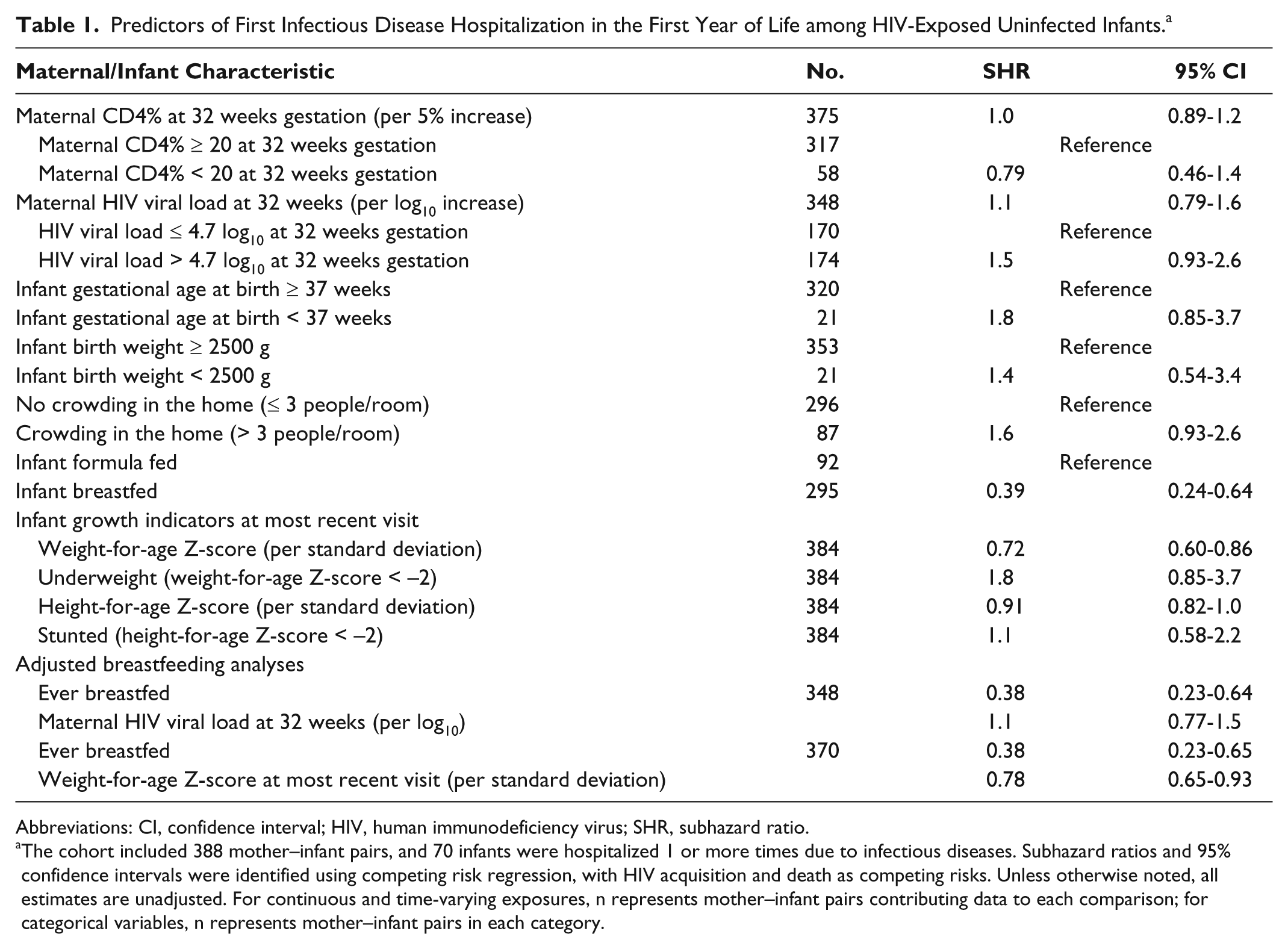
Abbreviations: CI, confidence interval; HIV, human immunodeficiency virus; SHR, subhazard ratio.
The cohort included 388 mother–infant pairs, and 70 infants were hospitalized 1 or more times due to infectious diseases. Subhazard ratios and 95% confidence intervals were identified using competing risk regression, with HIV acquisition and death as competing risks. Unless otherwise noted, all estimates are unadjusted. For continuous and time-varying exposures, n represents mother–infant pairs contributing data to each comparison; for categorical variables, n represents mother–infant pairs in each category.
Although height-for-age Z-score (HAZ) was not associated with subsequent IDH, better nutrition status, as indicated by higher weight-for-age Z-score (WAZ), was associated with a 28% decreased risk of IDH per standard deviation (SHR = 0.72; 95% CI, 0.60-0.86) within the subsequent time period. When the effect of time-varying WAZ on IDH was adjusted for feeding method, both remained independently significant. All estimates were unaffected by adjustment for maternal CD4% or HIV viral load at 32 weeks gestation (data not shown).
Allowing for repeat hospitalizations, overall incidence of IDH was 51/100 infant-years (95% CI, 37-70) among formula-fed infants and 19/100 infant-years (95% CI, 14-25) among breastfed infants. There was no difference in incidence among infants exclusively breastfed for 6 months (18/100 infant-years; 95% CI, 11-30) and those mixed-fed or breastfed for less than 6 months (20/100 infant-years; 95% CI, 14-28). When incidence of IDH was stratified by feeding method and underweight (WAZ < –2), a strongly significant dose-response was observed (Figure 2) (P = .0002).
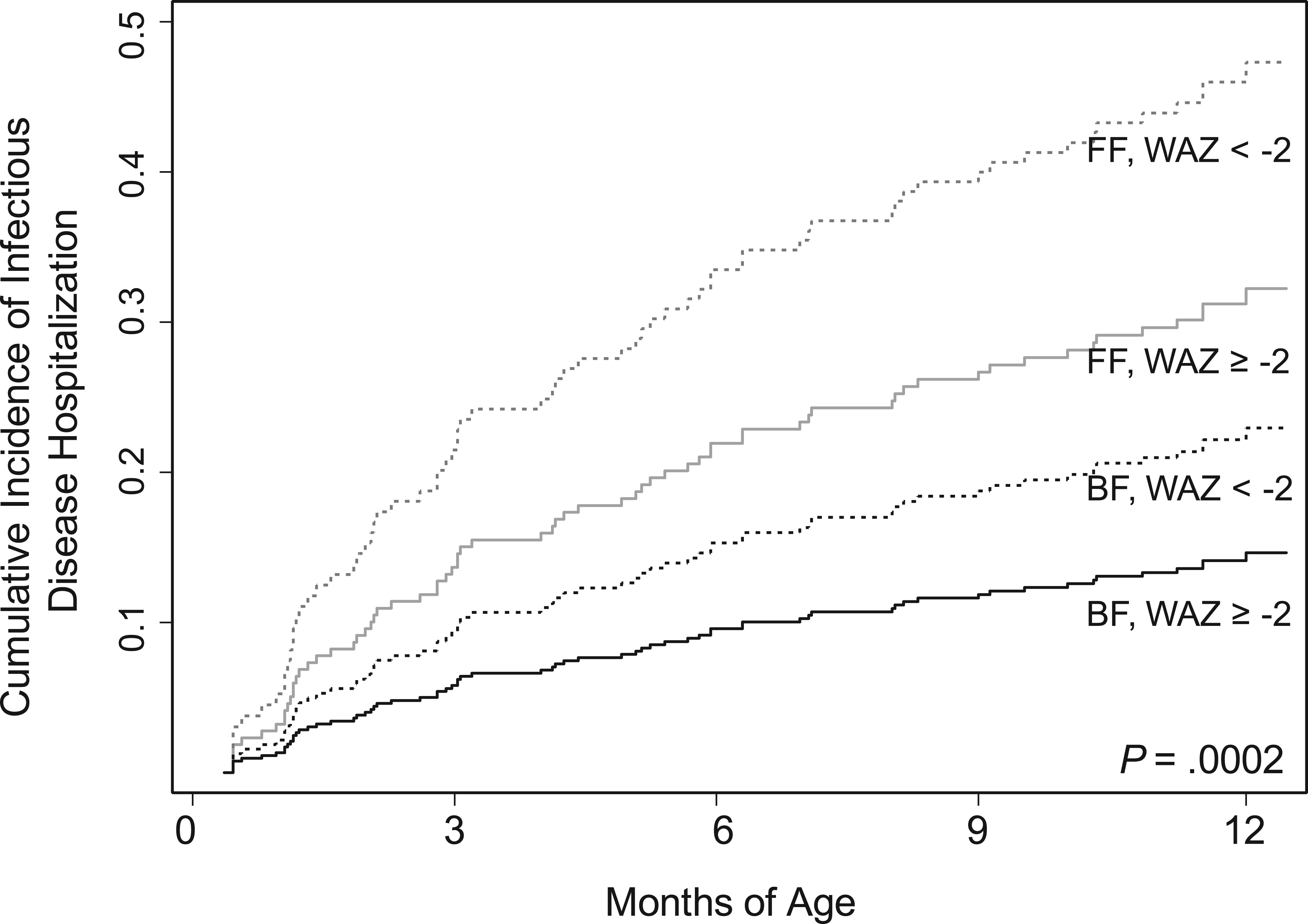
Cumulative Incidence of Infectious Disease Hospitalization among 388 HIV-Exposed, Uninfected Infants Stratified by Infant Feeding (FF vs BF) and Infant Weight (underweight [WAZ < –2] vs not underweight [WAZ ≥ –2]).
Discussion
We found a substantial burden of hospitalization in our cohort of HIV-exposed uninfected infants, primarily for infectious diseases. The incidence of hospitalization we observed, 35/100 infant-years, is somewhat higher than that reported in a South African study of HEU (23/100 infant-years), 15 which may be explained by access to safe public drinking water for all participants in that study. The proportion of infants hospitalized is also higher than that in a Zambian study in which 39 of 620 HEU infants had been hospitalized by 4 months of age. 16 Consistent with prior studies of HEU infants in Malawi 17 and Zambia, 16 however, most hospitalizations were due to pneumonia, sepsis, and gastroenteritis; the combined incidence of hospitalization due to pneumonia, severe febrile illness, and diarrhea in our study is comparable to that reported in the Malawian BAN study. 17
We observed substantially lower risk of hospitalization among breastfed infants than nonbreastfed infants, which is consistent with several prior studies of HEU infants. In a South African study in which mothers self-selected feeding method, a lower risk of hospitalization was observed among breastfed infants in the first 14 weeks of life, but this difference was no longer significant by 6 months. 18 The BAN study in Malawi, in which all infants breastfed, found increased risk of morbidity after weaning 4 ; the same effect was observed in a Zambian trial of early abrupt weaning.19,20 Gastroenteritis hospitalization was associated with lack of breastfeeding in an Indian study 21 and with early weaning in a Malawian study. 22
Whereas our study noted the effect of any breastfeeding, other studies have also noted strong protective effects of exclusive breastfeeding.23,24 Rates of exclusive breastfeeding were low in our cohort and duration was short, limiting our ability to compare exclusively breastfed infants and mixed-fed infants. In addition, there was some inconsistent reporting, with mothers reporting breastfeeding cessation and later reporting a return to breastfeeding. This may have been due to social desirability bias, with mothers wishing to appear to comply with study counseling recommending breastfeeding cessation at the time complementary feeding was introduced. Despite the limitations of the time-updated data, the strength of the association between feeding method and hospitalization was comparable when current breastfeeding was considered.
Maternal CD4 and HIV viral load during pregnancy have been associated with risk of severe morbidity among HEU infants in several African studies4,17 and a large French cohort. 25 This may be due to infant immune abnormalities following HIV exposure, 5 reduced maternal-derived antibody levels at birth, 26 or higher maternal morbidity and mortality leading to increased pathogen exposure and compromised care of the infant.3,8 We found no association between infant hospitalization and maternal CD4 in our study, possibly because CD4 counts and CD4% at 32 weeks gestation do not accurately reflect maternal health at delivery or postpartum. Time-updated CD4 would have been a preferable measure, but these data were missing in a large number of cases. We also did not observe an association between continuous maternal HIV viral load during pregnancy and infant hospitalization, although we observed a trend toward increased risk of IDH for children of mothers with higher than median viral loads during pregnancy; our study lacked power to detect an association of this magnitude.
Our observation that low WAZ was associated with increased rates of hospitalization is consistent with prior studies. 27 Children of HIV-infected mothers are at high risk of growth failure, 28 and this association has been related to breastfeeding cessation in a Zambian cohort. 29 It is interesting that adjustment for feeding method did not alter the association between WAZ and hospitalization in our cohort, and a dose-response was observed when the combined effect of underweight and breastfeeding was analyzed.
Our study had several limitations. Because our cohort lacked an HIV-unexposed uninfected (HUU) control group, we are not able to determine whether HEU infants were at higher risk of hospitalization than HUU infants in our setting; conflicting data on this question exist.4,6 Two thirds of infant hospital referrals were made by physicians outside our study clinics, meaning that reasons recorded were based on maternal report and may be imperfectly recalled. In focusing on hospitalization due to infectious disease, we excluded 9 hospitalizations for which the cause was unknown; it is possible that these hospitalizations were due to infectious causes and should have been included in the competing risk regression analysis. Last, our study was conducted prior to the introduction of new PMTCT guidelines (option B/B+), 30 in which mothers receive lifelong highly active antiretroviral treatment (HAART) starting during pregnancy or breastfeeding. These guidelines may result in improved HEU outcomes via improved maternal immunity, transferred immune responses, and decreased maternal morbidity.
Strengths of our study include cohort follow-up from birth through the first year of life, high retention rate, serial assessment of growth and morbidity by study physicians, and standardized collection of hospitalization data. For infants who acquired HIV during the study, timing of HIV infection was known, enabling us to include hospitalization history prior to HIV acquisition for these infants.
Conclusion
The most recent WHO guidelines regarding infant feeding support breastfeeding for all mothers with HIV, along with lifelong antiretroviral therapy started during pregnancy or breastfeeding. 30 These guidelines aim to both reduce mother-to-child transmission of HIV and improve maternal immunologic and virologic indicators, meaning that other correlates of infant hospitalization may emerge in future studies among HEU infants. Our results suggest that the new feeding guidelines may reduce serious morbidity and hospitalization among HEU infants and that the promotion of safe breastfeeding and improved nutrition will remain important for HEU infant health.
Footnotes
Acknowledgements
The authors wish to thank the CTL study clinical, laboratory, and data teams; the University of Nairobi and Kenyatta National Hospital for providing infrastructure for the study; and the Kizazi working group at UW Global WACh Center for their comments. They gratefully acknowledge the study participants.
Authors’ Note
Kristjana H. Ásbjörnsdóttir is a PhD student in the Department of Epidemiology at the University of Washington. She received her MPH in epidemiology from the University of Washington in 2012. A subset of these data was presented at the Society for Epidemiologic Research conference in Seattle, Washington, in June 2014.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The parent study was funded by US National Institute of Child Health and Human Development (grant R01 HD-23412). K.H.A. and G.J.S. were supported in part by NIH K24 HD054314. K.H.A. was supported by NIH Interdisciplinary Training in Cancer Research, T32 CA080416, and by a Trainee Support Grant from the Center for AIDS Research (CFAR) under NIH award number P30AI027757. J.A.S. and K.H.A. were supported in part by a New Investigator Award from CFAR under NIH award number P30AI027757. J.A.S. was supported by NIAID K01AI087369. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.