
Abstract
Background:
Breastfeeding reduces women’s risk of breast cancer. Since exclusive breastfeeding has a stronger hormonal effect, it could theoretically result in a greater reduction in breast cancer risk than any breastfeeding mode. No meta-analysis has examined breast cancer risk by breastfeeding mode.
Research aim:
The authors conducted a meta-analysis for breast cancer risk in parous women who breastfed exclusively or in any mode versus parous women who formula fed their infants, and they estimated the summary dose–response association by the accumulated duration of any breastfeeding mode.
Methods:
A systematic review of studies published between 2005 and 2015 analyzing breastfeeding and breast cancer risk in women was conducted in PubMed and EBSCOhost. A meta-analysis (n = 65 studies) with fixed effects (or random effects, if heterogeneity existed) was carried out stratified by breastfeeding mode and menopausal and parity status. A summary dose–response association was estimated using the generalized least-squares method.
Results:
The summary relative risk (SRR) for breast cancer in parous women who breastfed exclusively was 0.72, 95% confidence interval (CI) [0.58, 0.90], versus parous women who had never breastfed. For parous women who breastfed in any mode, the SRR was lower in both premenopausal women (0.86, 95% CI [0.80, 0.93]) and postmenopausal women (0.89, 95% CI [0.83, 0.95]). There was no heterogeneity or publication bias. There is weak evidence of a difference between exclusive and any breastfeeding mode (p = .08). The summary dose–response curve was nonlinear (p < .001).
Conclusion:
Exclusive breastfeeding among parous women reduces the risk of breast cancer compared with parous women who do not breastfeed exclusively.
Keywords
Background
Women benefit from breastfeeding (BF) (World Cancer Research Fund/American Institute for Cancer Research, 2007). The reduction in the incidence of breast cancer (BC), which is the most common cancer in women around the world, is the best-documented benefit of BF in women (Scoccianti et al., 2015). The biological mechanisms through which BF reduces women’s risk of BC can be explained by the differentiation of breast cells, a process in which these cells are modified to produce milk after pregnancy, reducing breast tissue susceptibility to carcinogenic effects such as estrogens (Petrakis et al., 1987). Furthermore, by inhibiting ovulation, BF reduces lifetime exposure to the mitogenic effect of estrogens (Russo, Hu, Yang, & Russo, 2000). The excretion of carcinogens through human milk and or exfoliation of breast tissue, which helps to eliminate cells with damaged DNA, reduces susceptibility to mutations (Romieu, Hernandez-Avila, Lazcano-Ponce, Weber, & Dewailly, 2000). In addition, breastfeeding a child and expressing human milk lowers serum concentrations of insulin in women (Gunderson et al., 2011), and there is evidence that chronically high serum concentrations of insulin can increase serum concentrations of insulin-like growth factor IGF-1, which is associated with proliferation and anti-apoptosis effects in breast tissue (Mawson et al., 2005).
Recent meta-analyses of epidemiologic studies showed that having ever breastfed, defined as having placed an infant to the breast at least once, is inversely associated with the risk of BC, and this protection is stronger if BF lasts ≥ 12 months (Anothaisintawee et al., 2013; Chowdhury et al., 2015; Nelson et al., 2012; Zhou et al., 2015). However, the summary relative risk (SRR) for BC varied according to BF duration (Anothaisintawee et al., 2013; Chowdhury et al., 2015; Nelson et al., 2012; Zhou et al., 2015); thus, evidence of a dose–response relation would strengthen the association. In addition, the SRR in these meta-analyses had a high level of heterogeneity (Anothaisintawee et al., 2013; Chowdhury et al., 2015; Nelson et al., 2012; Zhou et al., 2015). Heterogeneity is defined as the dispersion of effect sizes from study to study that is not due to a random error component but to differences between characteristics of individuals and studies. If heterogeneity is not explained through subgroup analysis, it could bias pooled estimations (Borenstein, Hedges, Higgins, & Rothstein, 2009). Part of the heterogeneity in the pooled estimations of BC risk may result from meta-analyses that did not distinguish BF mode and encompassed studies with exclusive, predominant, and partial BF modes in the ever-BF indicator (Chowdhury et al., 2015). Since exclusive BF, defined as feeding an infant only human milk (Chowdhury et al., 2015), is characterized by greater energy needs for milk production, mobilization of fat stores, and higher glucose utilization by the mammary gland, which leads to lower serum concentrations of insulin (Gunderson et al., 2011), and is also related to longer BF duration (Hills-Bonczyk et al., 1994), it can be postulated that it has a stronger protective effect on BC risk than any BF mode. Therefore, we conducted a meta-analysis (a) to estimate the SRR for BC in women who had breastfed exclusively or in any mode (exclusive, predominant, or partial) versus parous women who had never breastfed and compared between BF modes and (b) to estimate a summary dose–response association between the accumulated duration of any BF mode and the risk of BC.
Methods
Design and Setting
We conducted a systematic review of studies published between 2005 and 2015 analyzing BC risk and BF in women > 15 years of age. Since the World Cancer Research Fund conducted a comprehensive meta-analysis of BC risk and BF including studies published until 2005 (World Cancer Research Fund/American Institute for Cancer Research, 2007), we restricted our search between January 1, 2005, and December 31, 2015. Electronic searches in PubMed and EBSCOhost databases included the terms [breast neoplasms OR breast AND neoplasm OR breast cancer OR breast AND cancer OR carcinoma] AND [breastfeeding OR lactation]. Additional papers were identified through review of published systematic reviews and meta-analyses (Anothaisintawee et al., 2013; Nelson et al., 2012; Yang & Jacobsen, 2008). The protocol does not have a registration number.
Key Messages
Breastfeeding in any mode reduces women’s breast cancer risk, but the relation with exclusive breastfeeding has not been well studied.
Exclusive breastfeeding among parous women reduces the risk of breast cancer compared with parous women who do not breastfeed exclusively.
Breast cancer risk is further reduced if duration of any breastfeeding is extended at least a year.
Exclusive breastfeeding for 6 months should be promoted as a strategy to reduce breast cancer risk among parous women.
Sample
Titles and abstracts were evaluated to identify potentially relevant studies. Duplicate records were removed. Full text articles were assessed for eligibility with the following inclusion criteria: an original case-control (hospital-based or population-based) or cohort study that (a) assessed the effect of BF on the risk of BC; (b) evaluated ever BF and/or duration of BF in any mode (i.e., exclusive, predominant, or partial); (c) reported an odds ratio (OR), hazard ratio (HR), or relative risk (RR) with a 95% confidence interval (CI), adjusting for at least one covariate; (d) included women > 15 years of age; (e) included premenopausal women, postmenopausal women, or both; and (f) included parous or parous and nulliparous women. For studies that analyzed BF duration, additional criteria included those who have reported a sample size for cases and controls in case-control studies and a sample size for exposed and unexposed women in cohort studies. Since there were few studies that analyzed exclusive BF (n = 3), we included the studies that presented crude risk measures without adjusting for covariates (n = 1). A flow diagram according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA Statement) (Urrútia & Bonfill, 2010) and excluded articles, with reasons, is shown in Figure 1.
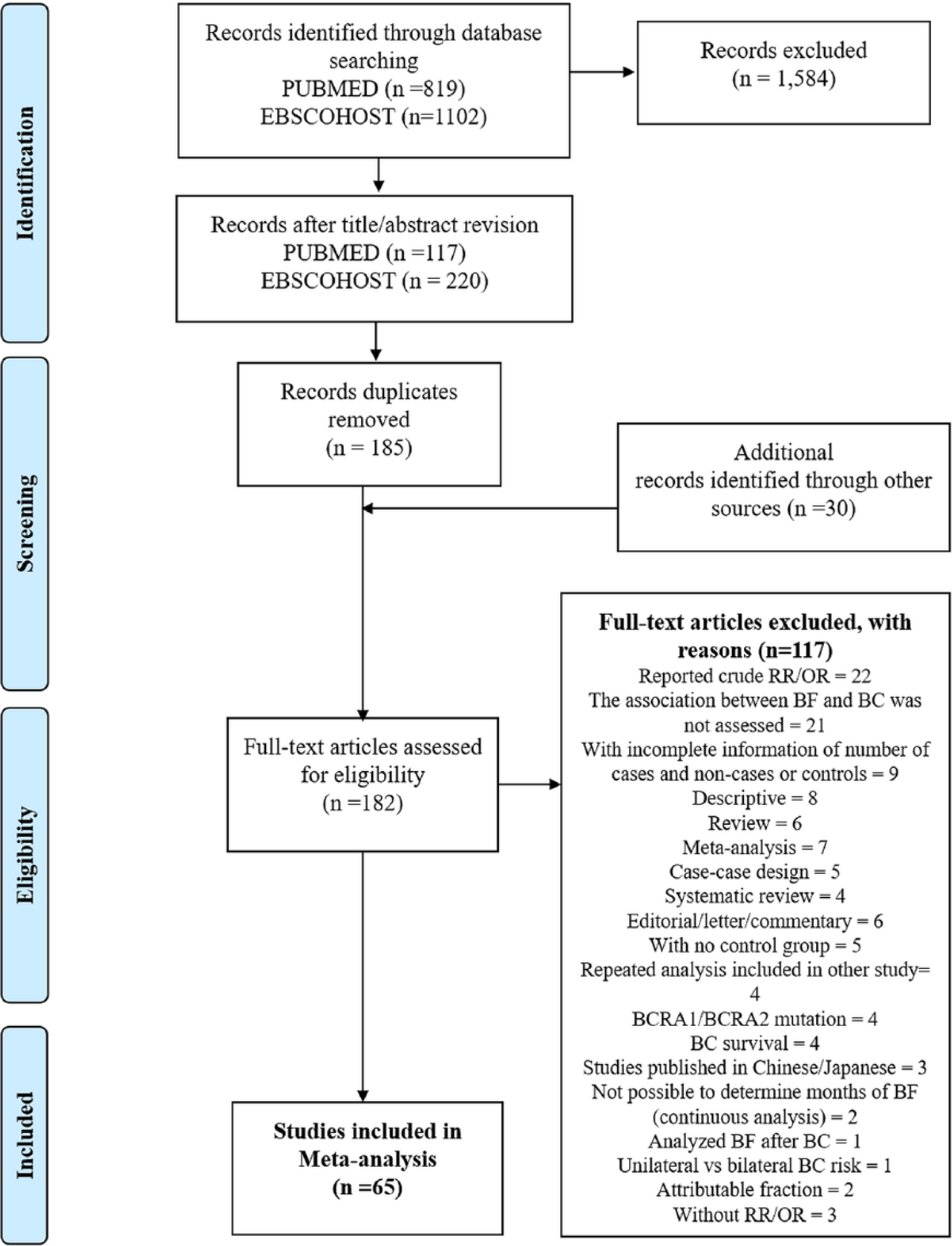
Flowchart of included and excluded articles for the meta-analysis. BC = breast cancer; BF = breastfeeding.
A total of 1,921 articles were found with the systematic review search. After title/abstract review, 337 records were selected, of which 185 were duplicated articles. Thirty additional records were identified through revision of other systematic review and meta-analyses (Anothaisintawee et al., 2013; Nelson et al., 2012; Yang & Jacobsen, 2008). Full text was assessed for eligibility in 182 articles. Only 65 articles met the established inclusion criteria and 117 were excluded for the reasons reported in Figure 1.
Data Collection
From each selected study, information was extracted and entered into an Excel database and then converted to Stata 13.1 for statistical analysis. If no measure of association was shown in a publication, we estimated the crude OR or RR and 95% CI with reported information about the number of cases and controls that were exposed and nonexposed to ever BF or to a specific BF duration category. If a study reported both crude and adjusted measures of association, only the adjusted measure was abstracted. We selected more than one measure of association per study when subgroup analyses were shown by menopausal status, breast cancer characteristics, parity status, BF mode (any and/or exclusive), and BF indicator (ever and/or duration). We did not extract information about measures of association that compared exclusive BF with any BF.
Data Analysis
To estimate the SRR and 95% CI for BC in women relative to exclusive BF or any BF mode in comparison with women who have never breastfed, we combined the logarithm for ORs and RRs of the selected studies in a meta-analysis. Conversion to logarithm avoids bias related to scale when pooling risk ratio measures (Borenstein et al., 2009). Odds ratios were considered to be equivalent to RRs since the incidence of BC was low (Nelson et al., 2012). The standard error for individual association measures was estimated as the difference in the upper and lower 95% CI natural logarithm divided by 2 × zα/2 (z = 1.96 for 95% CI) (Borenstein et al., 2009; Orsini, Bellocco, & Greenland, 2006). The summary estimates in logarithmic form and 95% CI were back-transformed into SRR by exponentiation (Borenstein et al., 2009). When more than one measure of association between ever BF and the risk of BC was available per study, we analyzed only mutually exclusive subgroups to avoid correlation between individual estimates.
The meta-analysis was performed with fixed effects using the inverse variance method, where each individual risk measure is weighted by the inverse of the within-study variance (Borenstein et al., 2009). Random effects were implemented if heterogeneity existed using the DerSimonian and Laird method, which considers the within-study and between-study variance (Borenstein et al., 2009).
Presence of heterogeneity of effect size between studies was assessed if the Q-test, a standardized measure of the deviation of each study’s effect from the overall effect, was statistically significant (p < .05) or when the variance between studies as a percentage of total variance (I2 statistic) was greater than 20% (Borenstein et al., 2009). Stratified analyses were performed by menopausal and parity status to evaluate heterogeneity. Differences between the SRR for BC relative to exclusive BF or any BF mode were assessed with the Q-test for heterogeneity based on analysis of variance (p < .05) (Borenstein et al., 2009).
A dose–response meta-analysis of the relation between the RR for BC and exposure to accumulated months of any BF mode was assessed using the generalized least-squares (GLS) method with random effects (Orsini et al., 2006). This method accounts for within-study covariance, allowing for more efficient estimations (Orsini et al., 2006; Orsini, Li, Wolk, Khudyakov, & Spiegelman, 2012).
Since most studies reported intervals of summarized BF duration, accumulated months of BF were estimated as the median of the lower and upper limits of the range, or as the smallest value of the range if no upper limit was defined (Orsini et al., 2006). The lower limit of the BF duration interval was defined in all observations. The reference group was 0 months of BF.
A linear and nonlinear trend of the dose–response relation was estimated. The nonlinear trend was a flexible estimation, with a curvature in the slope, modeled with a restricted cubic spline (to be linear in both tails) with knots (Orsini & Greenland, 2011; Orsini et al., 2012). Since the number of splines (k) determine the model’s fit, splines with three, four, and five knots were estimated as recommended for samples > 100 and the model with the highest likelihood ratio LRχ2 − 2k was selected (Harrell, 2001). The knot positions were fixed and equally spaced based on Harrell’s recommended percentiles for exposure data in order to have a sufficient sample in each knot: three knots (10th, 50th, and 90th), four knots (5th, 35th, 65th, and 95th), and five knots (5th, 27.5th, 50th, 72.5th, and 95th) (Harrell, 2001). Linear combinations of spline coefficients for each month of BF, with 0 months as the reference value, were computed to predict the SRRs for BC with a 95% CI for duration of BF ≤ 2 standard deviations (< 40 months) (Orsini & Greenland, 2011). A nonlinear trend existed if the joint null hypothesis that all the spline coefficients were equal to zero was rejected (p < .05) (Orsini et al., 2012). The Q-test of the model was used to verify if heterogeneity among studies, defined as the dispersion of effect sizes from study to study, was present (p < .05) (Orsini et al., 2006).
Models were stratified by parity status (parous and nulliparous or only parous women), study design (cohort, hospital-based or population-based case-control), and quality (studies that adjusted for age, parity, age at first pregnancy, and family history of BC) to explain sources of heterogeneity. Estimations were adjusted for menopausal status, parity status, study design, region of the world (Africa, Asia, Europe, Latin America, United States), and type of BC (incident, primary, invasive, and/or in situ tumor). All covariates were centered on the mean by subtracting the mean of each covariate in all the studies from the individual value in each study. Additional analyses were done in those studies that also adjusted for body mass index, oral contraceptive use, or hormone replacement therapy.
Publication bias was assessed by implementing the Begg test and Egger test for bias (p < .05) (Borenstein et al., 2009). All analyses were performed using Stata software version 13.1 with the mkspline, glst, xblc, metan, metabias, and metatrim commands (StataCorp, 2013).
Results
Studies that analyzed ever BF (n = 34) were included in the estimation of the SRR for BC (Aguilar Cordero et al., 2012; Akbari et al., 2011; Ambrosone et al., 2014; Beaber et al., 2008; Z. Butt et al., 2012; Chung et al., 2013; Gajalakshmi et al., 2009; Hadjisavvas et al., 2010; Horn et al., 2014; Hosseinzadeh et al., 2014; Ilic, Vlajinac, & Marinkovic, 2015; Iwasaki, Otani, Inoue, Sasazuki, & Tsugane, 2007; Kamarudin, Shah, & Hidayah, 2006; Kawai et al., 2012; Kim et al., 2007; Li et al., 2013; Liu et al., 2011; Lodha et al., 2011; Lord et al., 2008; Matalqah, Radaideh, Yusoff, & Awaisu, 2011; Millikan et al., 2008; Navarro-Ibarra, Caire-Juvera, Ortega-Vélez, Bolaños-Villar, & Saucedo-Tamayo, 2015; Palmer et al., 2011; Palmer et al., 2014; Phillips, Millikan, Schroeder, Barnholtz-Sloan, & Levine, 2009; Ritte et al., 2013; Shantakumar et al., 2007; Shema, Ore, Ben-Shachar, Haj, & Linn, 2007; Stendell-Hollis et al., 2013; Stuebe, Willett, Xue, & Michels, 2009; Sugawara et al., 2013; Ursin et al., 2005; Xing, Li, & Jin, 2010; Yanhua et al., 2012), out of which 33 studies examined any BF mode and only 3 studies measured exclusive BF (Kamarudin et al., 2006; Kawai et al., 2012; Sugawara et al., 2013), of which 1 reported crude risk measures without adjusting for covariates (Kamarudin et al., 2006).
To analyze BC risk by month of BF, we did not include studies that reported ever BF in the dose–response meta-analysis and incorporated only those studies that analyzed duration of BF (n = 47) (Akbari et al., 2011; Ambrosone et al., 2014; Awatef et al., 2010; Balasubramaniam, Rotti, & Vivekanandam, 2013; Bao et al., 2011; Beaber et al., 2008; Bhadoria, Kapil, Sareen, & Singh, 2013; S. Butt, Borgquist, Anagnostaki, Landberg, & Manjer, 2014; De Silva, Senarath, Gunatilake, & Lokuhetty, 2010; Dey et al., 2009; Gajalakshmi et al., 2009; Ghiasvand et al., 2012; Ghiasvand, Maram, Tahmasebi, & Tabatabaee, 2011; Hadjisavvas et al., 2010; Hajian-Tilaki & Kaveh-Ahangar, 2011; Huo et al., 2008; Ilic et al., 2015; Inumaru, Irineu Gomes Duarte Quintanilha, Aparecida da Silveira, & Veloso Naves, 2012; Islam et al., 2012; Kawai et al., 2012; Kim et al., 2007; Kruk, 2007; Lee et al., 2008; Li et al., 2013; Liu et al., 2011; Ma, Bernstein, Ross, & Ursin, 2006; Ma, Henderson, et al., 2010; Ma et al., 2009; Ma, Wang, et al., 2010; Mahouri, Dehghani Zahedani, & Zare, 2007; Millikan et al., 2008; Morales et al., 2013; Msolly, Gharbi, & Ben Ahmed, 2013; Okobia et al., 2006; Palmer et al., 2011; Peterson et al., 2008; Phipps et al., 2011; Phipps, Malone, Porter, Daling, & Li, 2008; Sarmento de Almeida, Leal Almeida, Rodrigues Araujo, & Weller, 2015; Shantakumar et al., 2007; Shema et al., 2007; Stuebe et al., 2009; Sweeney et al., 2008; Ursin et al., 2005; Warner, Colditz, et al., 2013; Warner, Tamimi, et al., 2013; Work et al., 2014). Only one study reported duration of exclusive BF (Stuebe et al., 2009). Since 16 studies reported a measure of ever BF and also the duration of BF, they were included in both meta-analyses. We present a summary of the characteristics of the included studies in Table 1.
Descriptive Statistics of Studies Included in Meta-Analysis by Breastfeeding Measure.
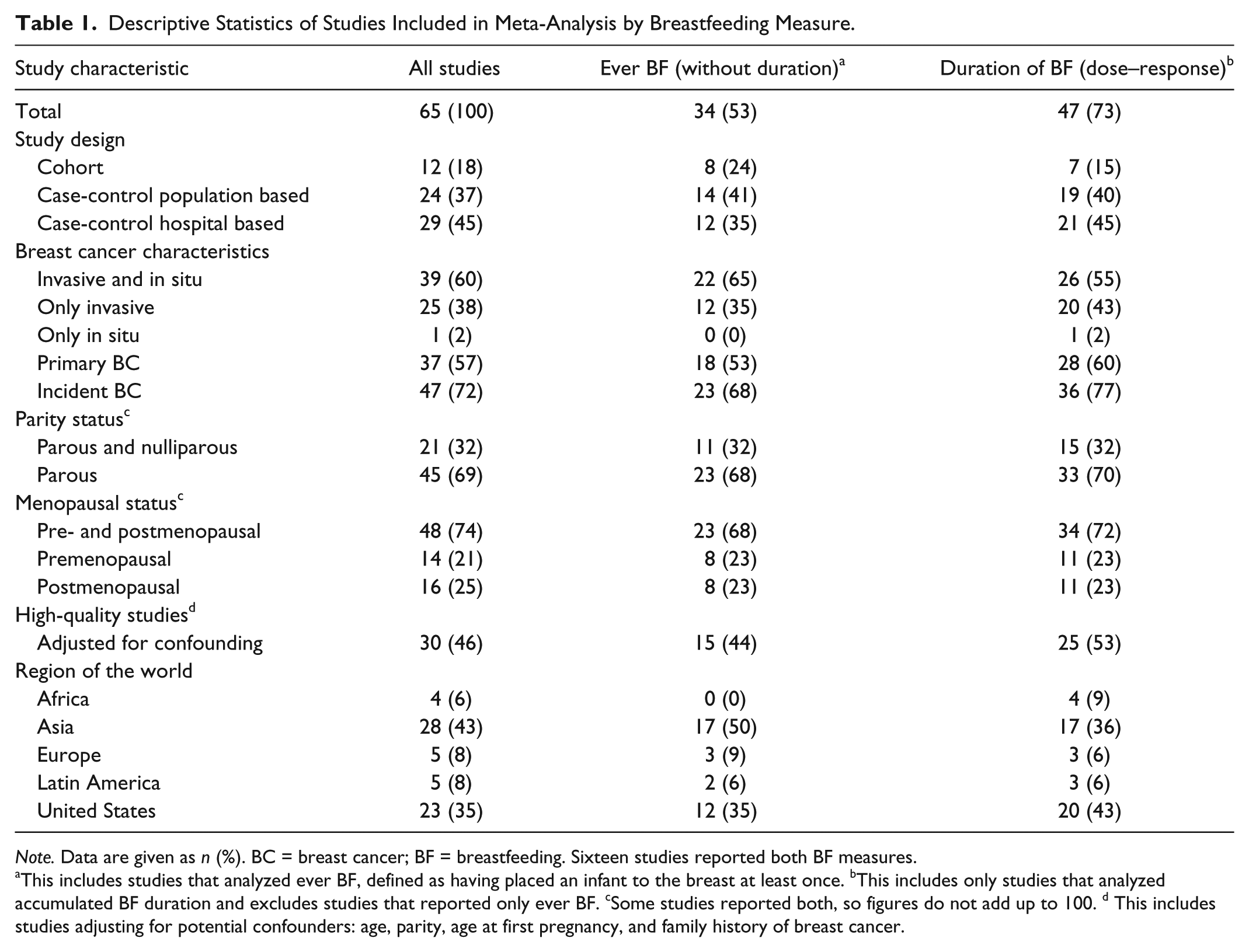
Note. Data are given as n (%). BC = breast cancer; BF = breastfeeding. Sixteen studies reported both BF measures.
This includes studies that analyzed ever BF, defined as having placed an infant to the breast at least once. bThis includes only studies that analyzed accumulated BF duration and excludes studies that reported only ever BF. cSome studies reported both, so figures do not add up to 100. d This includes studies adjusting for potential confounders: age, parity, age at first pregnancy, and family history of breast cancer.
Breast Cancer Risk and Breastfeeding Mode
The SRR for BC in women with any BF mode was 0.84, 95% CI [0.62, 1.13], compared with parous and nulliparous women who have never breastfed. Residual heterogeneity between studies was high (I2 = 54.2%, p < .001) (see Supplemental Figure 1).
The SRR for BC in women, stratified by menopausal and parity status, is shown in Table 2. In parous women who ever breastfed in any mode, the SRR was 0.86, 95% CI [0.80, 0.93], in premenopausal women and 0.89, 95% CI [0.83, 0.95], in postmenopausal women; there was no residual heterogeneity (I2 = 0%, p = .84 and p = .63, respectively). No publication bias was detected (Begg test p = .77 and Egger test p = .73 for premenopausal; Begg test p = .34 and Egger test p = .10 for postmenopausal).
Summary Relative Risk for Breast Cancer Relative to Ever Breastfeeding, by Menopausal and Parity Status.
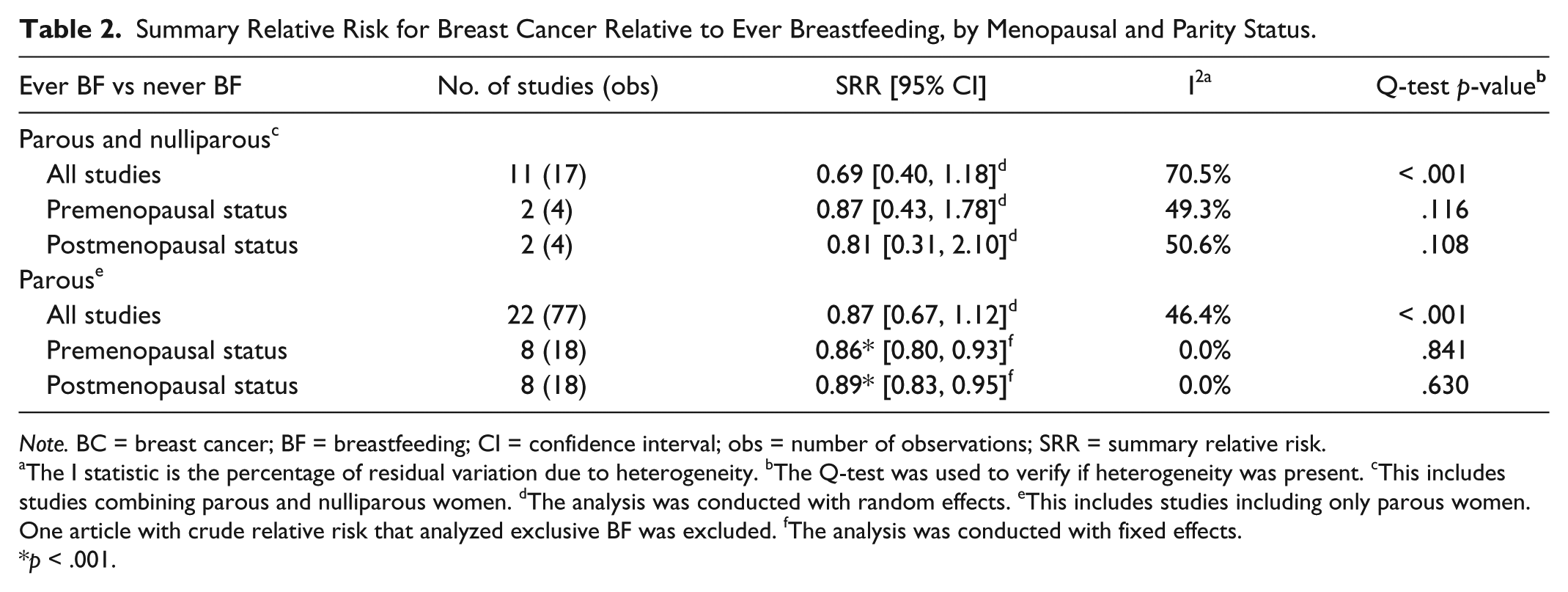
Note. BC = breast cancer; BF = breastfeeding; CI = confidence interval; obs = number of observations; SRR = summary relative risk.
The I statistic is the percentage of residual variation due to heterogeneity. bThe Q-test was used to verify if heterogeneity was present. cThis includes studies combining parous and nulliparous women. dThe analysis was conducted with random effects. eThis includes studies including only parous women. One article with crude relative risk that analyzed exclusive BF was excluded. fThe analysis was conducted with fixed effects.
p < .001.
In studies that examined parous women who exclusively breastfed in comparison with those who had never breastfed, the SRR was 0.72, 95% CI [0.58, 0.90], with low heterogeneity (I2 = 4.9%, p = .385) (see Figure 2). Two studies that analyzed exclusive BF reported association measures jointly in premenopausal and postmenopausal women (Kamarudin et al., 2006; Sugawara et al., 2013), and only one study reported four subgroup analyses by menopausal status and by hormone receptor status: positive estrogen and progesterone (ER+PR+) receptor BC tumor or negative receptor BC tumor (ER–PR–) (Kawai et al., 2012). Stratification of the SRR for BC by menopausal status was not possible due to the small sample size. There is weak evidence of a difference in effect size between the SRR for BC in parous women with exclusive BF versus any BF mode (Q-statistic = 3.05, p = .08).
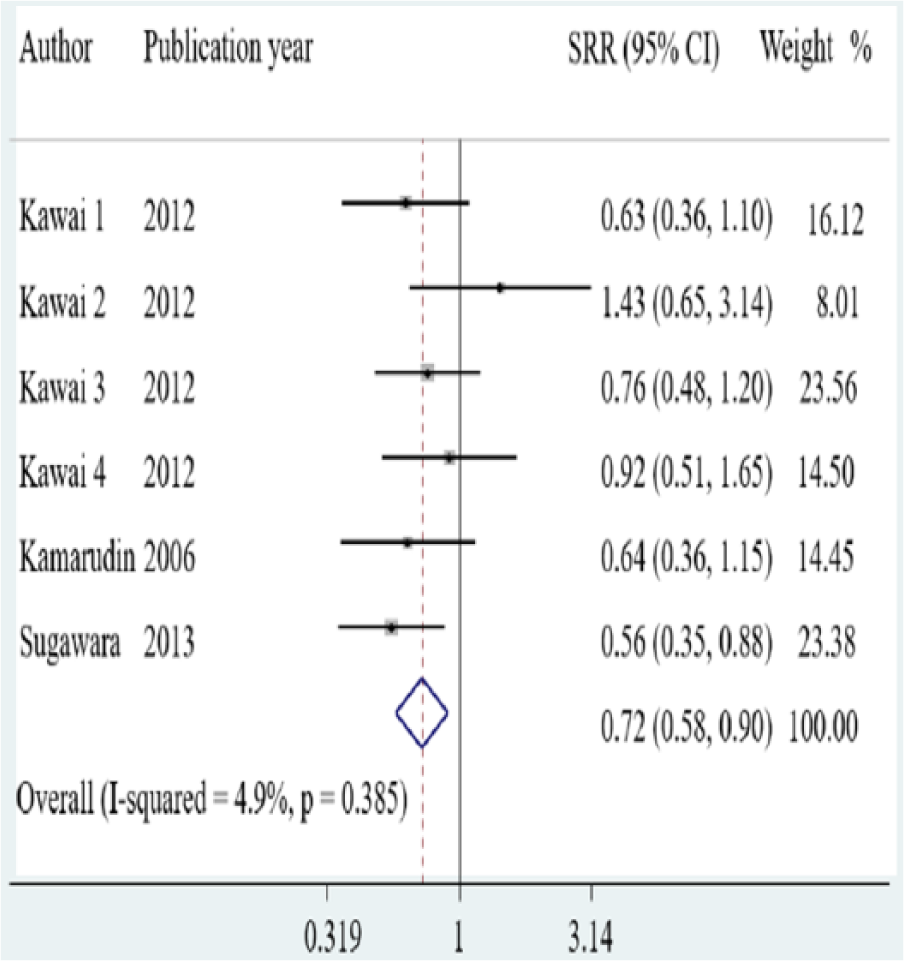
Forest plot of the relative risk for breast cancer in relation to exclusive breastfeeding (fixed effects). BC = breast cancer; BF = breastfeeding. The white diamond indicates the summary relative risk (SRR). SRR is compared with parous women who have never breastfed. Individual RR in each study is represented by the black squares with 95% confidence intervals denoted by horizontal lines. Gray squares represent the weight of each study, estimated as the inverse of the standard error of the RR. Kamarudin, Shah, and Hidayah (2006) and Sugawara et al. (2013) reported association measures between exclusive BF and BC risk jointly for premenopausal and postmenopausal women. Kawai et al. (2012) reported association measures of four subgroup analyses. Kawai 1: premenopausal women with positive estrogen and progesterone (ER+PR+) receptor BC tumor; Kawai 2: premenopausal women with negative estrogen and progesterone (ER–PR–) receptor BC tumor; Kawai 3: postmenopausal women with (ER+PR+); and Kawai 4: postmenopausal women with (ER–PR–).
Dose–Response Association Between Breast Cancer Risk and Duration of Breastfeeding
The dose–response association between the SRR for BC and the accumulated duration of any BF mode in high-quality studies, considered as those that adjusted for age, parity, age at first pregnancy, and family history of BC, analyzing only parous women is presented in Figure 3. We selected the model with five knots in the splines at the 5th, 27.5th, 50th, 72.5th, and 95th percentiles, since it had the highest likelihood ratio compared with models with three and four knots (see Supplemental Table 1).
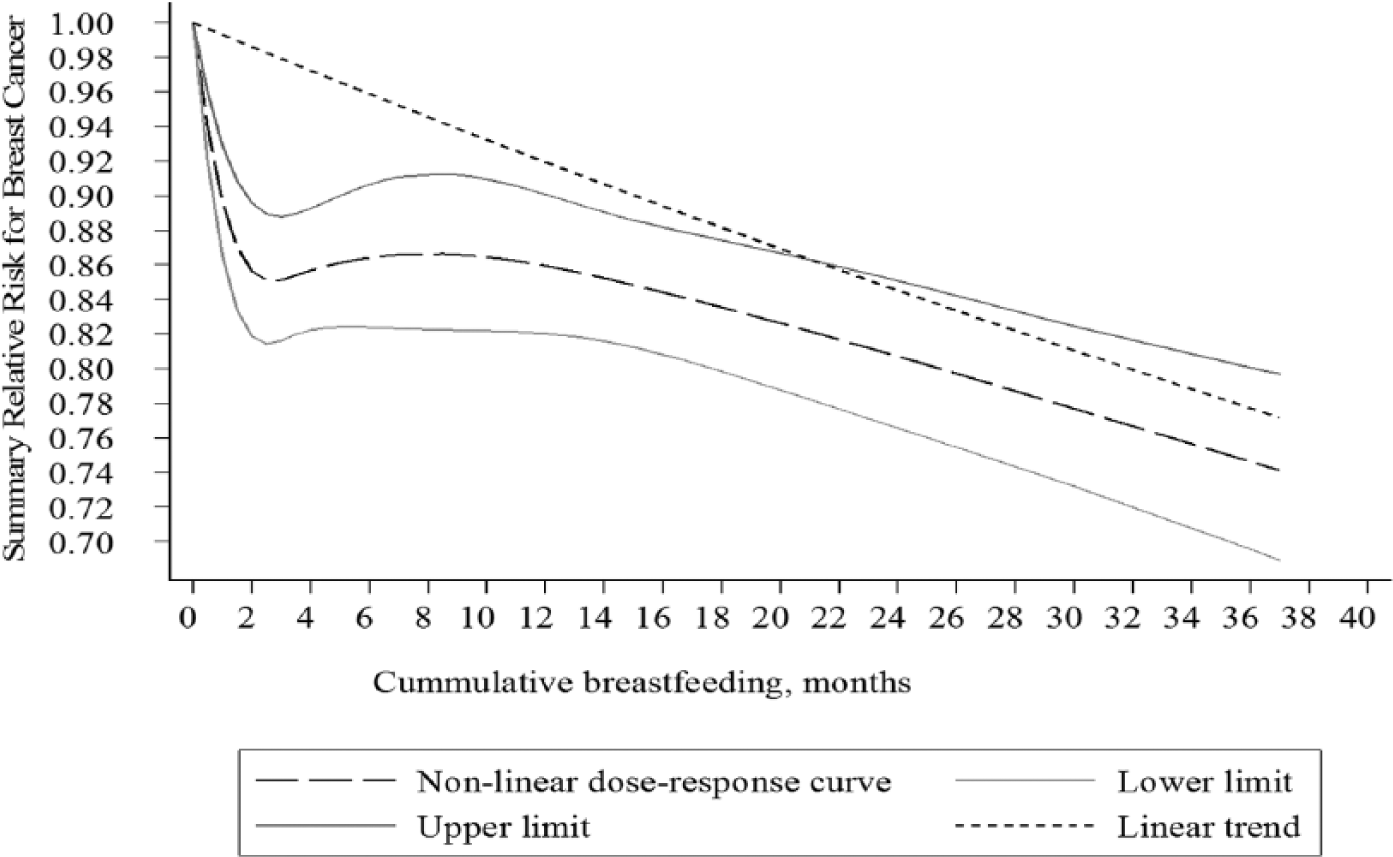
Dose–response relation between breastfeeding duration and breast cancer risk in parous women.
The SRR for BC when parous women breastfed for 6 months was 0.86, 95% CI [0.82, 0.91]. The dose–response association shows a decreasing nonlinear trend as the accumulated months of BF increase (p < .001). The dose–response curve of the SRR for BC had two inflexion points, decreasing faster in the first 6 months (0.86) and after 12 months of BF (see Figure 3).
Additional estimations of the dose–response association in all studies that analyzed BF duration and in high-quality studies that considered parous and nulliparous women are presented in Supplemental Table 2. Mean duration of accumulated BF was 13.8 months when considering all studies, 14.8 months in high-quality studies, and 14 months in high-quality studies that analyzed only parous women. After 6 months of accumulated BF, the SRR was higher in high-quality studies, particularly in studies that analyzed only parous women (see Supplemental Table 2).
Heterogeneity was present when analyzing all studies (p < .001) and high-quality studies (p = .0349), even after adjusting for relevant covariates (see Supplemental Table 2). There was no residual heterogeneity present in high-quality studies that analyzed parous women (p = .42) (see Supplemental Table 2). The summary dose–response and statistical tests were similar when considering studies that also adjusted for other confounding factors such as body mass index, oral contraceptive use, or hormone replacement therapy, but sample size was reduced by half (see Supplemental Table 3).
The relation between the SRR for BC and BF duration, stratified by study design in high-quality studies that analyzed only parous women, is shown in Figure 4. Mean duration of accumulated BF was ~ 11 months in the cohort and population-based case-control studies and 24 months in the hospital-based case-control studies. The SRR was higher in cohort studies than in case-control studies (p < .001). In the cohort studies, there was a negative linear dose–response association that seemed to increase and decrease at 6 months and 14 months of BF, respectively, but the slopes were not statistically significant. In the case-control population-based studies, the dose–response curve had a nonlinear trend (p < .001). The SRR sharply decreased from 0 to 6 months of accumulated BF and declined again in cases of BF > 14 months. In the case-control hospital-based studies, the dose–response presented a decreasing linear trend (nonlinearity test p = .261) observed until 9 months of accumulated BF, where it reached a plateau (see Figure 4). No heterogeneity was present by type of study design (p > .10). A small study effect (publication bias) was identified in the high-quality cohort studies that analyzed parous women (Egger test p = .015 and Begg test p = .026) and the case-control hospital-based studies (Egger test p = .805 and Begg test p = .04). No evidence of publication bias was detected in the high-quality case-control population studies (Egger test and Begg test p > .10).
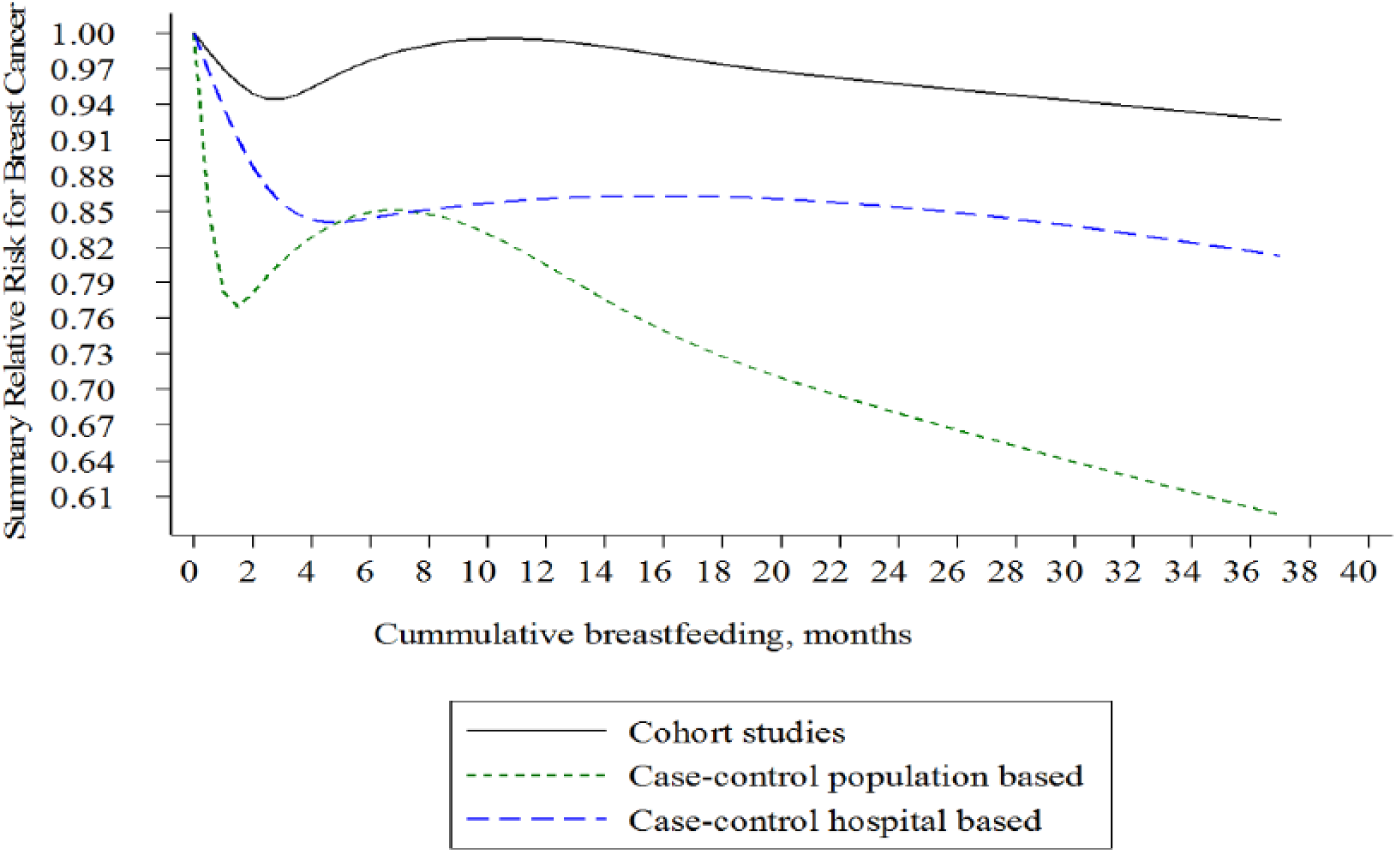
Dose–response relation between breastfeeding duration and breast cancer risk in parous women by study design.
Discussion
We estimated the SRR for BC in women who had ever breastfed, differentiating by mode of BF and the dose–response relationship between the accumulated months of any BF mode and BC risk. We also compared the SRR for BC by subgroup analyses of BF mode, parity and menopausal status of women, and quality of individual studies, to explain the wide variation of effect sizes between individual studies and reduce the bias exerted by heterogeneity in our pooled estimations.
This is the first meta-analysis that documents a protective effect of exclusive BF on the risk of BC. Parous women who breastfed exclusively had a 28% lower relative risk of BC compared with parous women who had never breastfed. Regarding any BF mode, BC relative risk was lower by 12% and 14% in premenopausal and postmenopausal parous women, respectively. Our dose–response meta-analysis revealed that BC risk in parous women was lower by increasing the accumulated duration of any BF mode, but the reduction was nonlinear—steeper at 6 months and after 12 months of BF duration.
Our SRR estimations for BC in parous women who breastfed are consistent with results of previously published meta-analyses where BC risk estimations varied from 7% to 13% in parous women (Chowdhury et al., 2015; Nelson et al., 2012). However, these studies had high heterogeneity (Chowdhury et al., 2015; Nelson et al., 2012), which could have biased their estimations (Borenstein et al., 2009). We found that parity status explained almost half of the heterogeneity in our pooled estimations. The SRR for BC was lower in studies that combined parous and nulliparous women than in those that analyzed only parous women, and this was also found in other meta-analyses (Anothaisintawee et al., 2013; Chowdhury et al., 2015; Nelson et al., 2012; Zhou et al., 2015). These results could be explained by the fact that parity confers protection against the risk of developing BC, in addition to the protective effect of BF (Collaborative Group on Hormonal Factors in Breast Cancer, 2002).
Although we found that menopausal status accounted for the remaining heterogeneity in the estimation of the SRR for BC, there was no significant difference between the pooled estimations by menopausal status in women. Our findings confirm that having ever BF protects from developing BC in premenopausal as well as in postmenopausal parous women to a similar degree (Collaborative Group on Hormonal Factors in Breast Cancer, 2002). This is important due to the presence of the most aggressive BC tumors (hormone receptor-negative) in premenopausal women (Islami et al., 2015). Results from a recent meta-analysis have shown that BF also protects from developing this type of BC (Islami et al., 2015).
Although there is weak evidence of a difference between the SRR for BC between exclusive and any BF mode, differences could be diluted since any BF mode is a heterogeneous group that includes the loose definition of all BF modes (i.e., exclusive, predominant, and partial). Moreover, misclassification bias could arise if a woman reported exclusive BF for at least one child, but her other children were partially or nonbreastfed (Kamarudin et al., 2006). In addition, the small sample size of studies that measured exclusive BF probably led to a low statistical power of the Q-test for heterogeneity between BF subgroups (Borenstein et al., 2009). Our estimations are robust since the analyzed studies were homogenous; all included only parous women and most of them were of high quality and were conducted in populations of premenopausal and postmenopausal women.
Exclusive BF is characterized by a stronger hormonal effect than other modes of BF since it requires greater energy needs for milk production and is associated with higher mobilization of fat stores and glucose utilization by the mammary gland, which leads to lower serum concentrations of insulin (Gunderson et al., 2011). In addition, it has been documented that exclusive BF is related to longer postpartum amenorrhea in women (Kramer & Kakuma, 2012), reducing the exposure to estrogen in lactating women compared with partial BF. These biological mechanisms could partly explain the greater protection of exclusive BF against BC. Exclusive BF is also related to longer BF duration (Hills-Bonczyk et al., 1994), which is related to a greater reduction in BC risk.
No other meta-analysis has estimated the dose–response relationship between BF duration and BC risk considering the correlation among BF measures within each study. Results from other studies that examined women whose BF duration was longer than 12 months found BC risk reductions between 15% and 53% (Chowdhury et al., 2015; Nelson et al., 2012; Zhou et al., 2015). All studies showed high heterogeneity. We have shown that potential confounders, such as parity, age at first pregnancy, and family history of BC (Collaborative Group on Hormonal Factors in Breast Cancer, 2002), explain the wide variation in estimates for BF duration and BC risk found in other meta-analyses.
Our estimates show that the summary dose–response curve of BC risk decreased in a nonlinear pattern with BF duration, and this relation was also found in a pooled re-analysis from 47 epidemiologic studies (Collaborative Group on Hormonal Factors in Breast Cancer, 2002). The nonlinearity of the dose–response could be derived from combining the different effect sizes of all BF modes that are included in the accumulated duration of BF. Our results suggest that assuming a linear relation would lead to biased upward estimations of BC risk reduction.
Stratifying the risk analysis by study design showed that the effect of BF duration on lowering the risk of BC was stronger in case-control than in cohort studies. Our findings are consistent with results from two recent meta-analyses (Chowdhury et al., 2015; Zhou et al., 2015). However, estimations of BC risk in case-control studies are more prone to bias compared with cohort studies since information on BF duration is collected after the diagnosis of BC, with potential recall bias between cases and controls leading to inaccurate risk estimations. Also, variability in the sources of data for documenting a diagnosis of cancer could be greater in case-control studies since most of them were performed in developing countries where National Cancer Registries are scarce and detection of cancer is possibly limited by access to care, all of which could bias risk estimations.
The dose–response curve in cohort studies exhibited weak evidence of a protective linear relationship only for the first 3 months of BF. Results from a cohort study in Norwegian women also found that women with shorter (< 4 months) or longer BF durations (> 10 months) had a lower RR of BC than women with a middle BF duration (Kvåle & Heuch, 1988). Our hypothesis is that the dose–response association of BC risk exhibited the untangled effects of both exclusive BF and total BF duration. We found that exclusive BF has a stronger effect on reducing the risk of BC than any BF mode and its duration is usually between 4 and 6 months of an infant’s life, which coincides with the steeper reduction observed in the BC risk dose–response association during the first months of BF.
Our study has some limitations related to the design of the individual studies included in our meta-analysis. Since cohort studies represented less than 20% of the sample, case-control studies were overrepresented and may have had a downward bias on our pooled RR estimations due to recall bias on BF. Second, residual confounding could be present in observational studies since there are variables related to BF and BC risk reduction such as lower pre-pregnancy body mass index and lower prevalence of smoking (Zhou et al., 2015), which are not measured or adjusted for in individual analyses. Third, our pooled estimations combine exclusive, predominant, and partial BF modes in an indicator of any BF mode, which could have reduced the precision of our estimates. Last, we could not perform a dose–response analysis by exclusive BF mode due to lack of data. Other studies of BC risk factors that identify BF mode and duration are needed to accurately estimate the different effects on BC risk reduction.
Regardless of these limitations, our meta-analysis shows that there is evidence that exclusive BF has a stronger protective effect against BC than any BF mode, and there is a dose–response association between BC risk and BF duration. Our pooled risk estimations were more accurate in comparison with other meta-analyses, since heterogeneity between studies was explained by BF mode, quality of the study, and menopausal and parity status. Also, bias inherent to observational studies was reduced as we considered studies that adjusted for age, parity, age at first pregnancy, and family history of BC, which are potential confounders. In addition, duration of BF was analyzed in a dose–response meta-analysis that considered the correlation of risk measures within each study, which led to unbiased estimations of the trend and nonlinearity test of the dose–response association.
Conclusion
Exclusive breastfeeding among parous women reduces the risk of breast cancer compared with parous women who do not breastfeed exclusively. Breast cancer risk is further reduced if duration of any breastfeeding is extended at least a year. It is opportune to inform women that breastfeeding is a behavior that can reduce breast cancer risk and also encourage the promotion of breastfeeding to improve their practices. We recommend that in the future, researchers collect more detailed information about women’s breastfeeding mode and its duration according to the World Health Organization definitions.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a scholarship from the Mexican National Council for Science and Technology (CONACyT for its Spanish acronym) with grant number 335672/232906 to M.U.M. The funder was not involved in the development of this meta-analysis.