
Abstract
Background:
Aspirin has antipyretic and anti-inflammatory properties and is frequently used by pregnant and lactating women. However, its transfer in human milk when administered at low dose has not been reported.
Research aim:
This study aimed to evaluate the transfer of acetylsalicylic acid and its metabolite, salicylic acid, into human milk following the use of low dose aspirin.
Methods:
In this study, milk samples were collected at 0, 1, 2, 4, 8, 12, and 24 hours from seven breastfeeding women after a steady-state daily dose of 81 mg of aspirin. Milk levels of acetylsalicylic acid and salicylic acid were determined by liquid chromatography–tandem mass spectrometry.
Results:
Acetylsalicylic acid levels were below the limit of quantification (0.61 ng/ml) in all the milk samples, whereas salicylic acid was detected at very low concentrations. The average concentration of salicylic acid observed was 24 ng/ml and the estimated relative infant dose was 0.4%.
Conclusion:
Acetylsalicylic acid transfer into milk is so low that it is undetectable even by highly sophisticated methodology. Salicylic acid does appear in the human milk in comparatively low amounts, which are probably subclinical in infants. Thus, the daily use of an 81-mg dose of aspirin should be considered safe during lactation.
Background
Aspirin, or acetylsalicylic acid (ASA), is used as an analgesic, antipyretic, and anti-inflammatory agent. Aspirin is also well known to lower the risk of recurrent stroke, myocardial infarction, and vascular death in patients suffering from cardiovascular disease (Patrono, Coller, FitzGerald, Hirsh, & Roth, 2004; Patrono, Garcia Rodriguez, Landolfi, & Baigent, 2005). Thus, in low doses, it is commonly used as an antithrombotic agent to inhibit cyclooxygenase dependent platelet aggregation (Roth, Stanford, & Majerus, 1975).
Kinetically, aspirin absorption takes place in the stomach and upper intestine. Aspirin is rapidly hydrolyzed by esterases in the gastrointestinal mucosa and liver, which rapidly form the metabolite salicylic acid (SA) (Pedersen & FitzGerald, 1984). Acetylsalicylic acid has a brief half-life of only 15 to 20 minutes in plasma. Platelets in the portal circulation first come into contact with higher concentrations of aspirin before it is completely metabolized by the liver, thus accounting for its activity as a platelet aggregation inhibitor.
Low dose aspirin achieves its effects through the irreversible inactivation of cyclooxygenase (COX)-1. This prevents the enzymatic formation of thromboxane A2, a potent activator of vasoconstriction and platelet aggregation (Lecomte, Laneuville, Ji, DeWitt, & Smith, 1994; Patrono, 1994; Smith & Willis, 1971). The ASA-induced inhibition lasts for the life of the platelet, about 7 to 10 days. A daily dose of 80 mg produces chronic inhibition of platelet activity (Jakubowski, Stampfer, Vaillancourt, & Deykin, 1985). Low dose aspirin taken once daily is clinically effective in prevention and treatment of myocardial infarction (“Aspirin After Myocardial Infarction,” 1980; Sai et al., 2011; The RISC Group, 1990), acute ischemic stroke (Lewis et al., 1983), and transient cerebral ischemia (Fields, Lemak, Frankowski, & Hardy, 1977).
Much is already known about aspirin and its effects. However, its transmission in human milk, if taken at low dose, has not been studied thus far. Since breastfeeding is widely accepted as the ideal source of nutrition for infants, the decision to continue nursing while taking a drug requires knowledge of the amount being transferred to the milk. The purpose of this study was to determine the concentrations of ASA and its metabolite, SA, into human milk and estimate the relative infant dose.
Methods
Design
The study evaluated the pharmacokinetics of low dose aspirin, given as a daily dose, in lactating women. The Institutional Review Board of Texas Tech University approved this study (A12-3710), and written informed consent was obtained from all participants.
Sample Collection
The study enrolled seven lactating women ages 31 to 45 years, who were exclusively breastfeeding, were not pregnant, and had an average body weight of > 50 kg. Key exclusion criteria included the following: consumption of grapefruit or its juice and the intake of metoclopramide or domperidone. Each woman completely pumped milk from both breasts prior to using the drug. Milk samples were collected at 0, 1, 2, 4, 8, 12, and 24 hours after having taken the daily dose of 81 mg enteric-coated aspirin. At each time point, both breasts were completely pumped and the milk was mixed to ensure homogeneity. The average volume of 30 ml was collected for sample analysis. The mother was able to use the remaining expressed milk for her infant. They were stored at −80ºC until analysis.
Measurement
Samples were analyzed for ASA and its active metabolite, SA, using a validated, sensitive, and specific method by ultra high performance liquid chromatography–tandem mass spectrometry (UHPLC/MS/MS). This method employed a simple protein precipitation of milk sample using acetonitrile, followed by reverse phase chromatography on a Phenomenex Zorbax C18 column. The analytes—ASA and its metabolite, SA—were measured by multiple reaction monitoring on highly sensitive UHPLC/MS/MS equipment. The mass transitions m/z used for ASA were 179 to 137, and 137 to 93 for SA. Both were detected in negative polarity [M-H]–. Linear calibration curves were calculated for both analytes. The lower limit of quantification for ASA and SA in milk samples was 0.61 ng/ml and 1.2 ng/ml, respectively. The blank milk, spiked with a known concentration of ASA, was stored under comparable conditions as the patients’ samples. They were analyzed over time and gave consistent results, showing no ASA hydrolysis.
Key Messages
Women suffering from cardiovascular disease reduce their risk by taking daily antiplatelet medications such as aspirin at a low dose. However, levels of aspirin in human milk have not been reported.
This study reports a simple and sensitive method for the detection of acetylsalicylic acid and its metabolite, salicylic acid, in human milk samples.
This is the first study to highlight a significant low exposure of the drug to the infant and suggests that low dose aspirin is probably safe during breastfeeding.
Data Analysis
The pharmacokinetic parameter calculated was the area under the curve for the mean drug concentration in milk versus time from 0 to 24 hours using the log linear trapezoidal method. Other parameters calculated were the maximum observed concentration (Cmax), time at which the maximum drug concentration is observed (Tmax), and relative infant dose (RID). The RID is calculated by dividing the infant’s dose via milk (mg/kg/day) by the mother’s dose in mg/kg/day.
Results
A total of seven lactating women were enrolled in our study. Six of these women were on a regular regimen taking a daily low dose of 81 mg aspirin. The mean age of these participants was 32.3 years with an average body weight of 68 kg. The woman who took 325 mg of aspirin was 45 years old and weighed 70.3 kg. All the women were between 1 and 8 months postpartum.
In all milk samples, levels for ASA were undetectable, suggesting that aspirin is so rapidly cleared from the maternal plasma compartment that it penetrates milk at levels so low that they are undetectable even with this instrumentation.
The derived pharmacokinetic parameters for SA in human milk are summarized in Table 1. The average concentration (Cavg) for SA was estimated to be 24 ng/ml, calculated from the area under the curve, which was 576.43 ng.hr/ml as represented in Figure 1. The maximum observed concentration (Cmax) of SA was 114.9 ng/ml and was observed at 4 hours (Tmax). Assuming average mothers’ weight to be 67.8 kg, the calculated relative infant dose was only 0.4%.
Pharmacokinetic Parameters of Salicylic Acid After 81 mg Aspirin.
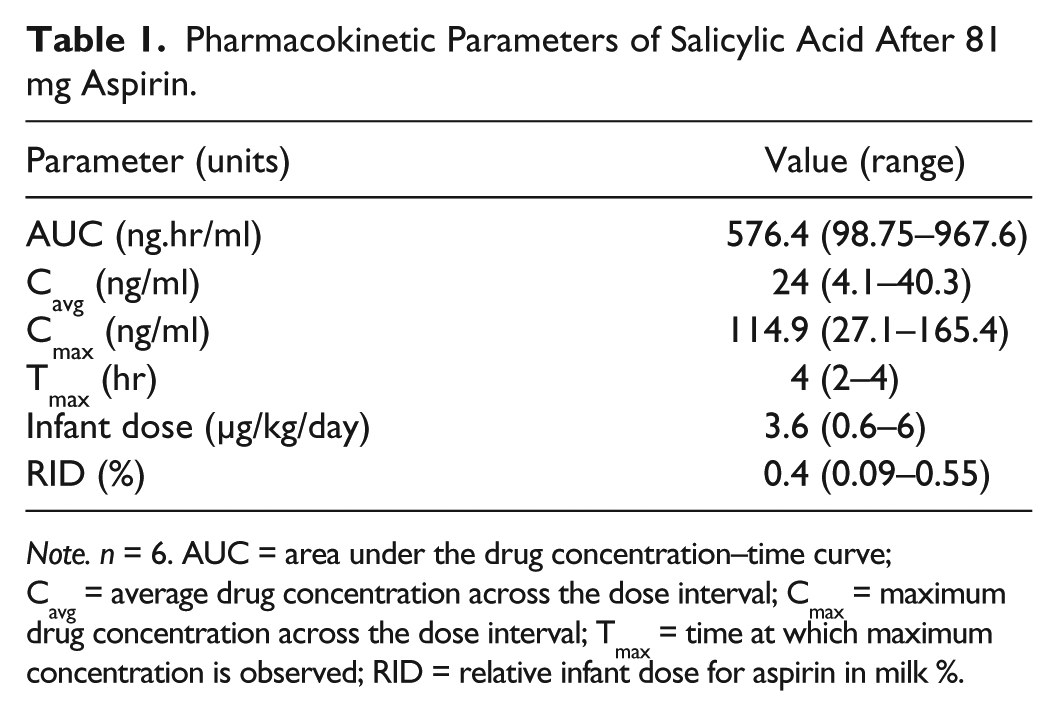
Note. n = 6. AUC = area under the drug concentration–time curve; Cavg = average drug concentration across the dose interval; Cmax = maximum drug concentration across the dose interval; Tmax = time at which maximum concentration is observed; RID = relative infant dose for aspirin in milk %.
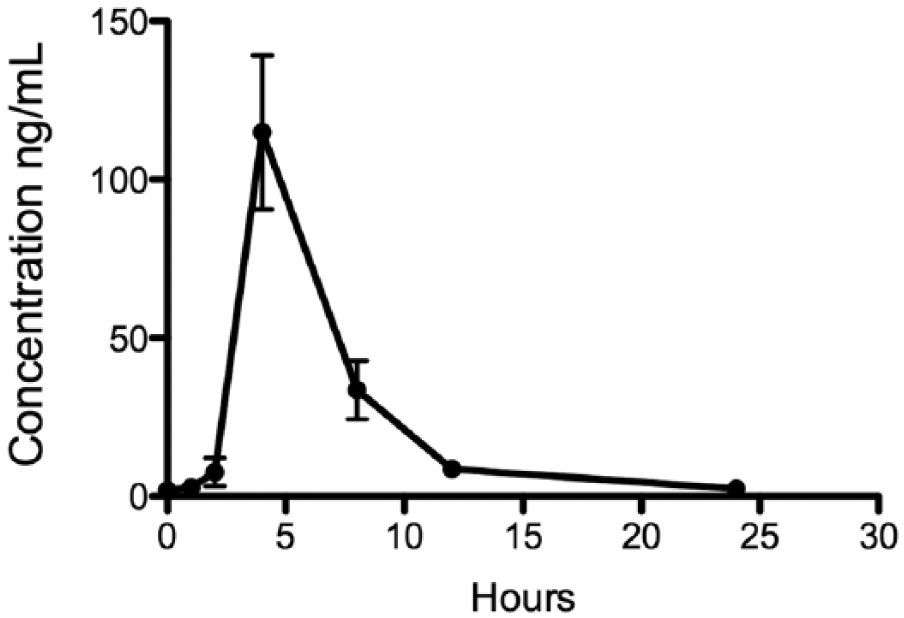
Mean milk concentration–time profile of salicylic acid in human milk following the oral administration of 81-mg aspirin tablets to breastfeeding mothers (n = 6).
In one patient consuming 325 mg/day of aspirin, human milk levels of ASA were comparable with those taking 81 mg, or undetectable (< 0.61 ng/ml). In this patient, the maximum concentration of SA was observed as 744.6 ng/ml, which peaked at 1 hour as represented in Figure 2. The area under the curve was 2579 ng.hr/ml and the average concentration estimated was 107.4 ng/ml. The relative infant dose calculated was 0.45%.
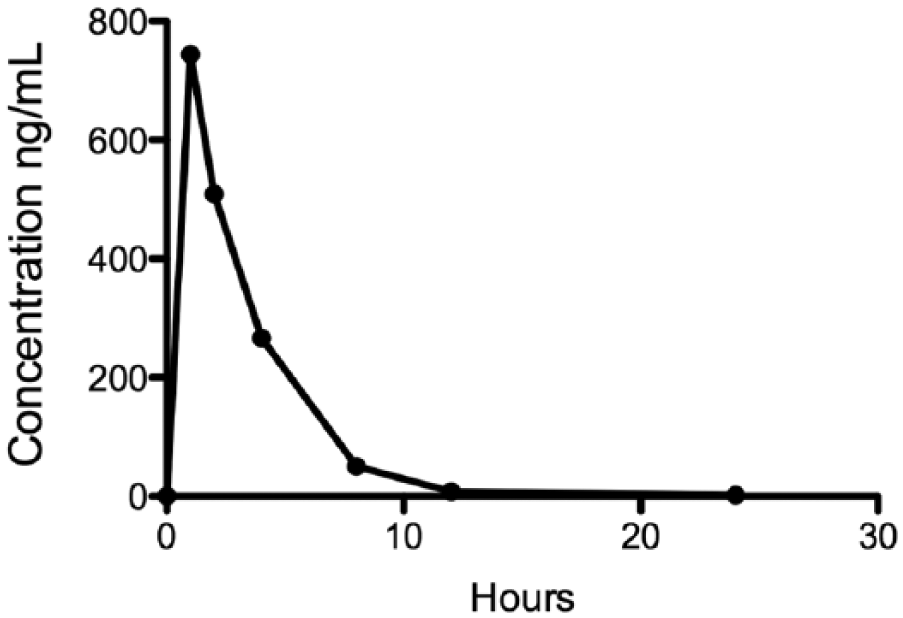
Milk concentration–time profile of salicylic acid in human milk following the oral administration of 325-mg aspirin tablet (n = 1).
No adverse effects or any concerns were reported for the infants. The results of this study suggest undetectably low doses of aspirin despite these two different doses. If administered in breastfeeding women, it should be quite safe for the infants.
Discussion
Virtually all drugs transfer into human milk to some degree. Drugs with high molecular weights, such as heparin and many new biological drugs, are mostly excluded from the intact milk compartment. The transfer of drugs into human milk is commonly described as the infant dose (mg/kg), expressed as a percentage of the maternal dose (mg/kg), also known as the relative infant dose (RID). A cutoff of 10% has been recommended as a guide for the safe use of most drugs into human milk (Begg, Atkinson, & Duffull, 1992). This is the first study to evaluate the steady-state levels of low dose aspirin and its transfer into human milk and provides quantitative information on the potential dose that an infant might consume during breastfeeding. This study suggests the relative infant dose to be 0.4% following a daily oral dose of 81 mg aspirin and 0.45% for a daily dose of 325 mg. The estimated daily infant dose of aspirin from milk of women receiving 81 mg/day (assuming mean milk consumption of 150 ml/kg/day) was 3.6 μg per kg of infant body weight. The enteric-coated aspirin versus the uncoated form of aspirin is expected to provide similar concentration levels in milk, as the difference lies only in their site of absorption. However, there may be a delay in the SA Tmax peak with the enteric-coated form of aspirin as compared with the uncoated form. Therefore, aspirin, if taken at low doses, penetrates the milk compartment minimally and is unlikely to have any clinical effect on the breastfed infant.
In one study in pregnant women receiving 100 mg aspirin daily, the authors found both ASA and SA in their plasma. At birth, plasma levels of ASA in newborns were below the limit of detection. Furthermore, low levels of SA were detected in only one infant (Leonhardt, Bernert, Watzer, Schmitz-Ziegler, & Seyberth, 2003). The prior study also suggested that during pregnancy, ASA was completely eliminated in 4 hours from maternal plasma and SA was detected at very low concentrations after 18 to 21 hours. This study clearly suggests that ASA undergoes rapid hydrolysis in the body. A case study of salicylates in milk of a nursing mother reported 1 mg/dl of SA at 3 hours following a dose of 975 mg of aspirin (Bailey, Weibert, Naylor, & Shaw, 1982). In another case report of a 9-week-old breastfed infant whose mother was taking 2.4 g per day, the infant’s serum contained 0.47 mmol/L (64.39 mg/L) of SA. The authors also reported that they were not able to quantify SA in mother’s milk as the lipids present interfered with the assay (Unsworth, d’Assis-Fonseca, Beswick, & Blake, 1987). This is likely due to a lack of sensitive and accurate analytic techniques during that period of time.
Aspirin is a polar, acidic drug with low lipid solubility and high protein binding—features that diminish substantial transfer into human milk. Higher doses of salicylates may cause toxic effects in breastfed infants. One case report has been found in the literature attributing infant toxicity to metabolic acidosis due to high serum salicylate (Clark & Wilson, 1981). In this study, the mother was taking high dose aspirin (650 mg every 4 hours); however, maternal concentrations were not reported. The American Academy of Pediatrics states that low doses of aspirin are acceptable for lactating mothers, but the higher therapeutic doses are not advised, as “the serum concentration of salicylate in breastfeeding infants has been reported to reach approximately 40% of therapeutic concentrations” (Sachs & Committee on Drugs, 2013).
The data above represent women who were taking high doses of aspirin. However, to date, no study has ever reported the levels with a low dose of aspirin in human milk.
Our study suggests that ingestion of a daily single dose of aspirin, even as low as 81 mg, does not seem to produce milk salicylate levels of clinical significance, thus suggesting that it is probably safe to use during breastfeeding.
Conclusion
Studies of drug excretion into human milk are medically very relevant. The present study conducted on seven breastfeeding women, all at steady state and taking low doses of aspirin, demonstrated undetectable quantities of ASA in their milk samples and very low concentrations of SA present, implying limited to no potential risk to a breastfeeding infant.
Footnotes
Acknowledgements
The authors thank the core facility of Texas Tech University for the usage of the AB Sciex API 5500 QTRAP UHPLC/MS/MS equipment. They would also like to thank the InfantRisk Center and Clinical Research Unit for their support in the collection of the milk samples.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.