
Abstract
In the past decade, biological nurturing and activation of maternal and infant instincts after birth have constituted a major advance in clinical breastfeeding support. Yet, physiologic breastfeeding initiation is not enough to ensure ongoing pain-free and effective breastfeeding for many pairs. Current interventions, including “hands-off” mammalian approaches, do not improve breastfeeding outcomes, including in randomized controlled trials. Back-arching, difficulty latching or staying on the breast, and fussing at the breast are common signs of infant positional instability during breastfeeding. These cues are, however, often misdiagnosed as signs of medical conditions or oral connective tissue abnormalities, and underlying positional instability is not addressed. New clinical approaches are urgently required. This article offers a clinical approach to fit and hold (or latch and positioning)—gestalt breastfeeding, which aims to optimize positional stability and intraoral breast tissue volumes for pain-free effective breastfeeding. The word gestalt (pronounced “ger-shtolt”) means a whole that is more than the sum of its parts. Gestalt breastfeeding builds on the theoretical foundations of complexity science, physiologic breastfeeding initiation, and new understandings of the biomechanics of infant suck elucidated in ultrasound studies. It also integrates simple psychological strategies from applied functional contextualism, popularly known as Acceptance and Commitment Therapy, empowering women to attend mindfully to breast sensations and their infant’s cues. Gestalt breastfeeding can be reproduced for research purposes, including in comparison studies with oral surgery, and has the potential to improve breastfeeding outcomes.
Keywords
Background
In the past decade, the physiologic approach to breastfeeding initiation, which includes skin-to-skin contact, biological nurturing, and activation of both maternal and infant instincts in the first hours after birth, has constituted a major advance in clinical breastfeeding support (Colson, Meek, & Hawdon, 2008; Moore, Berman, Anderson, & Medley, 2016; Schafer & Watson Genna, 2015; Smillie, 2016; Widstrom et al., 2011). Yet, physiologic breastfeeding initiation is not enough to ensure ongoing pain-free and effective breastfeeding for many pairs over time (Brodribb, Kruske, & Miller, 2013). Although a Cochrane review demonstrated that face-to-face support by trained personnel, whether professional or lay, helps breastfeeding outcomes overall (McFadden et al., 2017), specific clinical interventions, including “hands-off” mammalian interventions, have not been shown to contribute to improved breastfeeding outcomes, including in randomized controlled trials (de Oliveira, Giugliani, & do Espirito Santo, 2006; Forster et al., 2004; Henderson, Stamp, & Pincombe, 2001; Kronborg, Maimburg, & Vaeth, 2012; Kronborg & Vaeth, 2009; Labarere et al., 2003; Svensson, Velandia, Matthiesen, Welles-Nystrom, & Wistrom, 2013; Wallace et al., 2006; Wood, Woods, Blackburn, & Sanders, 2016).
For example, nipple pain affects 34% to 96% of breastfeeding women (Berens, Eglash, Malloy, & Steube, 2016) and is a common reason for breastfeeding cessation (Odom, Scanlon, Perrine, & Grummer-Strawn, 2013). Yet, studies that combine typical approaches to fit and hold with various topical applications for nipple pain show no convincing benefit (Dennis, Jackson, & Watson, 2014). New, theoretically sound approaches to clinical breastfeeding support are urgently required (Wood et al., 2016).
In this discussion, we use the term fit and hold to refer to the way a woman’s highly anatomically variable breast and body and her infant’s highly anatomically variable intraoral cavity, face, and body interact and fit together in breastfeeding (commonly referred to as latch and positioning or attachment and positioning). A woman’s unique anatomy, including breast size and elasticity; abdominal shape; lap length; nipple shape, size, and direction; and upper and forearm length and shape, and her infant’s unique anatomy, including palate contour; oral connective tissue length, attachments and elasticities; tongue length; oral cavity size; and chin recession or shape need to fit together in a way that supports positional stability, nipple protection or healing, and optimal milk transfer. This is particularly important in mother–infant pairs facing anatomic challenges, including (but not limited to) inelastic breast tissue, pendulous breasts, recessed infant mandible, high infant palate, and obesity.
In addition to nipple pain and damage, suboptimal fit and hold results in difficulty latching onto and staying on the breast, back-arching, marathon feeds, excessively frequent feeds, excessive night-waking, fussiness at the breast, excessive crying, poor weight gain, and low supply. Suboptimal fit and hold often remains unidentified or misdiagnosed, including by breastfeeding support professionals, and its signs are misattributed to gastroesophageal reflux disease, allergy, or most recent, oral connective tissue restriction (Douglas, 2013; Douglas, 2016; Douglas & Hill, 2011). The effects of suboptimal fit and hold and other undiagnosed breastfeeding problems on infant behavior may include a conditioned hyperarousal of the sympathetic nervous system, as detailed in the neurobiological model of unsettled infant behavior (Douglas & Hill, 2013). Parents commonly introduce infant formula in response to infant behaviors that typically result from suboptimal fit and hold (Odom et al., 2013; Wasser et al., 2011).
The breastfeeding mother–infant pair is usefully conceptualized as a complex adaptive system (Douglas, Hill, & Brodribb, 2011). Inherent patterns of self-organization emerge out of the multiple feedback loops that operate within the breastfeeding mother–infant complex adaptive system. These are determined by evolutionary history, emphasizing the importance of supporting a woman’s attention to the sensations within her own body and to her infant’s communications or cues. Because of these multiple neurohormonal and behavioral feedback loops, the breastfeeding pair is innately flexible and adaptive, ensuring resilience in the face of perturbation.
From the perspective of complexity science, clinical problems emerge out of multiple unpredictable interactions between coevolving components in the complex adaptive system, rather than from the failure of a single component (e.g., oral connective tissues). Simplistic medicalized interventions (such as proton pump inhibitors, or frenotomy for restricted oral connective tissues in the absence of classic tongue-tie) disempower mothers and risk unintended consequences. The breastfeeding mother–infant complex adaptive system also displays sensitivity to initial conditions, so that small disruptions in the breastfeeding relationship early on, in the first hours, days, or weeks, may have unpredictable and disproportionate effects later (Douglas & Hill, 2013; Douglas et al., 2011).
What Is Gestalt Breastfeeding?
In our specialist breastfeeding clinic, where mother–infant pairs seeking help have often already consulted with multiple breastfeeding support professionals, we have developed an innovative approach for both prevention and repair of breastfeeding problems—gestalt breastfeeding (see Table 1). The word gestalt (pronounced “ger-shtolt”) means a whole that is more than the sum of its parts. Gestalt breastfeeding integrates the theoretical frames of complexity science and physiologic breastfeeding initiation (Schafer & Watson Genna, 2015) with new understandings of the biomechanics of infant suck elucidated in ultrasound studies (Douglas & Geddes, 2017; Geddes & Sakalidis, 2016). In our clinical experience, infants with breastfeeding problems, including those diagnosed with oral ties (in the absence of classic tongue-tie) whose parents seek a second opinion as well as infants with oral aversion or ongoing breastfeeding difficulties after laser or deep scissors frenotomies, quickly respond to this intervention. Gestalt breastfeeding downregulates amplified feedback loops to support the mother–infant complex adaptive system’s empowerment and resilience.
Chapter Headings and Subtitles of the Gestalt Breastfeeding Online Program, Accompanied by Explanatory Text, Videos, and Photographs
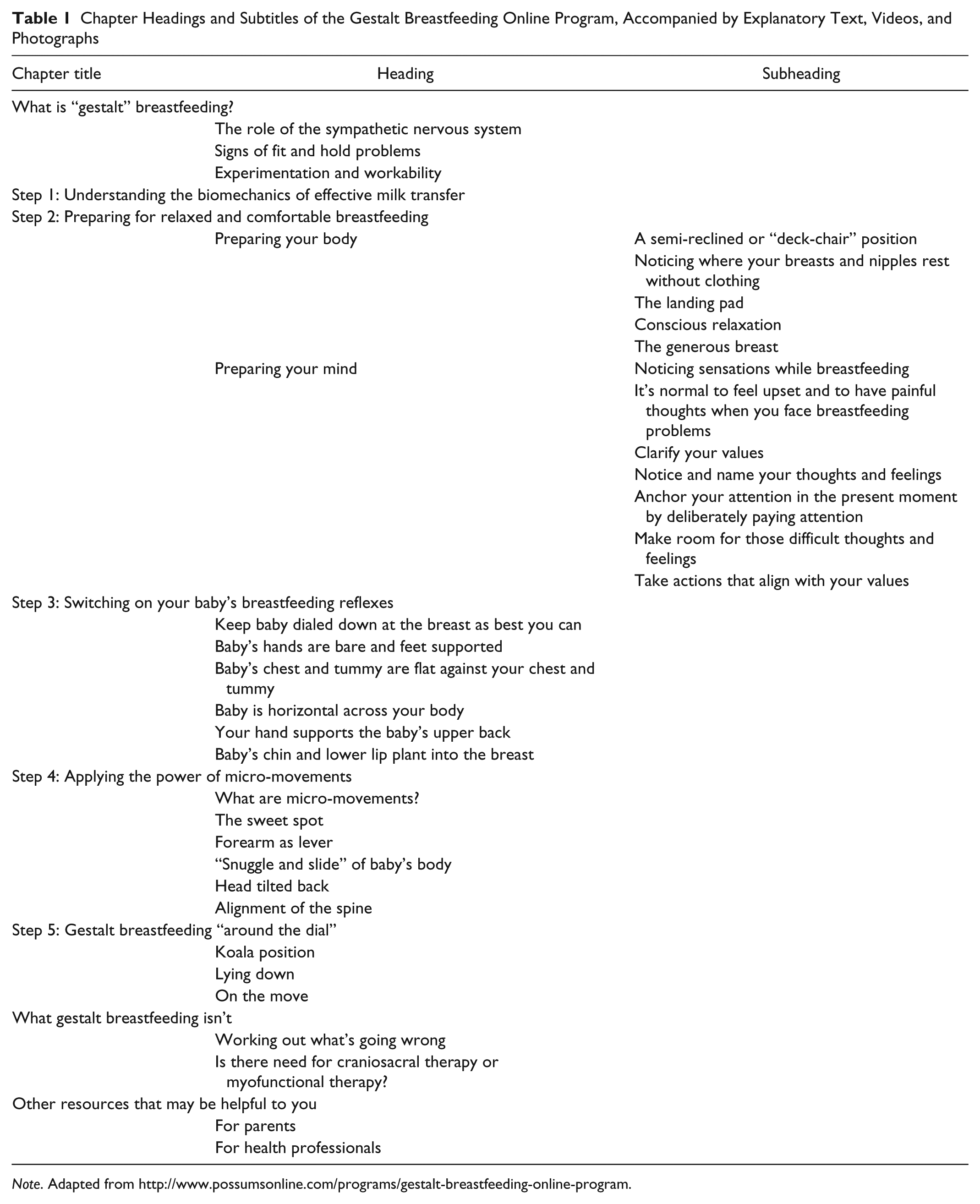
Note. Adapted from http://www.possumsonline.com/programs/gestalt-breastfeeding-online-program.
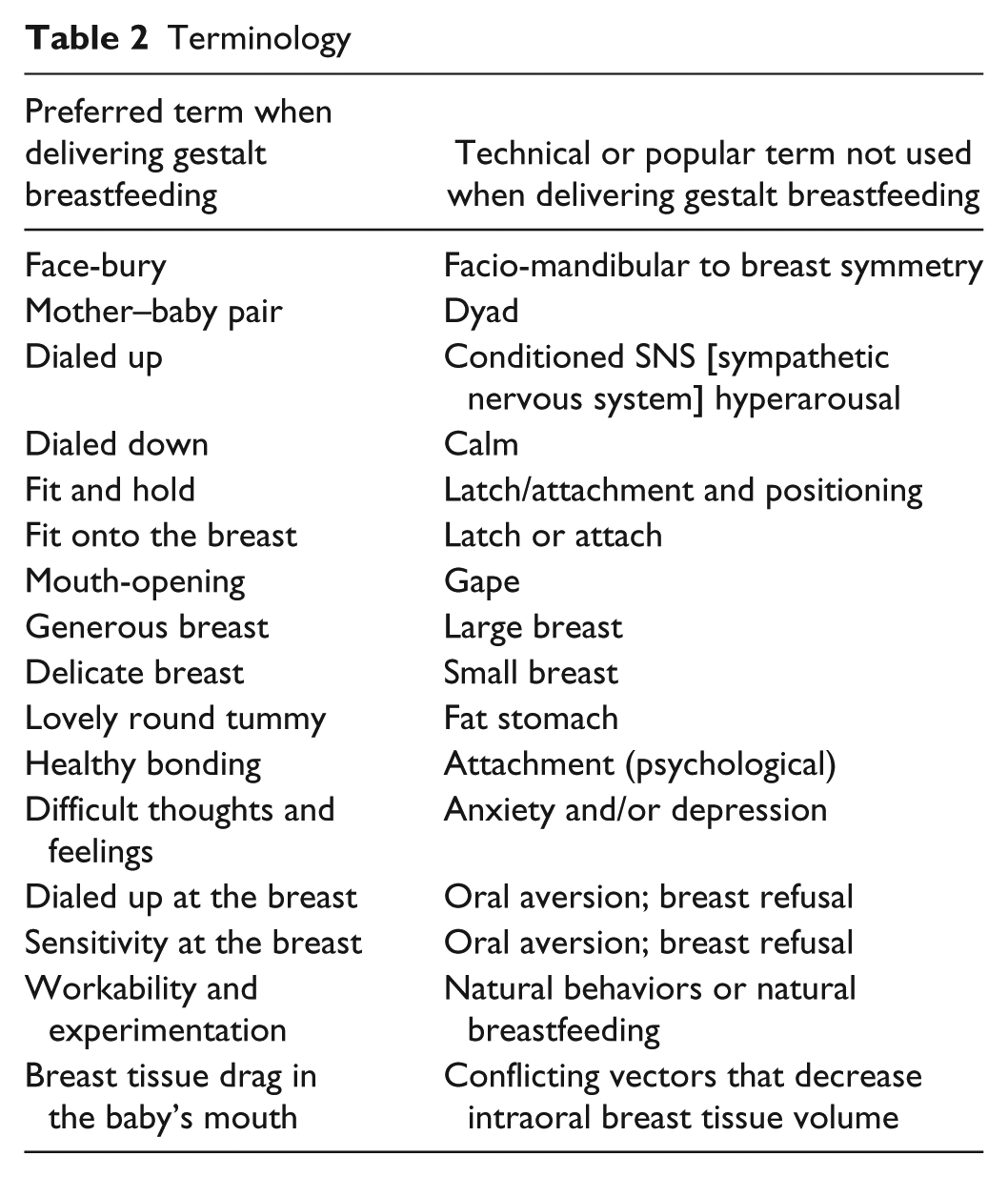
We offer a mother information and support in five steps, delivered flexibly in response to her needs, so that she is empowered to experiment and discover a fit and hold that works for her and her infant across their unique anatomic configurations. We are careful to avoid ideology (Burns, Schmied, Fenwick, & Sheehan, 2012) and to use words that are nonmechanistic and emotionally neutral or encouraging (see Table 2). A typical intervention starts with observation of the mother–infant pair’s usual fit and hold. (The woman may be invited to demonstrate this fully clothed using a doll if she has severe nipple damage.)
Terminology
Step 1: Understanding the Biomechanics of Healthy Breastfeeding
Ultrasonography of breastfeeding pairs demonstrates that milk transfer occurs in response to the intraoral vacuum generated by reflex downward excursion of the jaw, at the same time as the mammary ducts contract with milk ejection. The infant tongue moves downward as a single unit in tandem with jaw depression (Douglas & Geddes, 2017; Geddes & Sakalidis, 2016).
The breastfeeding infant’s tongue is most accurately conceptualized as an adaptive, supple organ that molds to fit around available intraoral breast tissue, cushioning it. The shape of the tongue alters in response to the volume of breast tissue in the mouth. The greater the intraoral breast tissue volume, the closer the nipple is to the junction of the hard and soft palate, which protects it from damage. The tongue does not grasp the breast. The tongue also does not need to extend beyond the lower gum, lateralize, or lift independently during sucking (Douglas & Geddes, 2017; Geddes & Sakalidis, 2016).
Positional stability requires the elimination of conflicting intraoral vectors of force. Conflicting vectors are commonly created, for example, by the weight of the breast tissue pulled downward by gravity or by breast tissue drag off to the side because the infant’s head is positioned too far toward the ipsilateral maternal arm. Conflicting vectors compromise intraoral breast tissue volume. In the context of positional stability, the intraoral vacuum draws incrementally more breast tissue into the oral cavity with each drop of the jaw, until the mouth is full of breast tissue and the jaw is wide open (Douglas & Geddes, 2017).
When an infant’s position is unstable, she or he has difficulty latching on, fusses and pulls off the breast, back-arches, or seems to refuse to feed. Conflicting vectors of force are being generated, so that there is drag on the intraoral breast tissue. Positional instability results in suboptimal intraoral breast tissue volume, which may result in poor milk transfer and nipple pain (Douglas & Geddes, 2017).
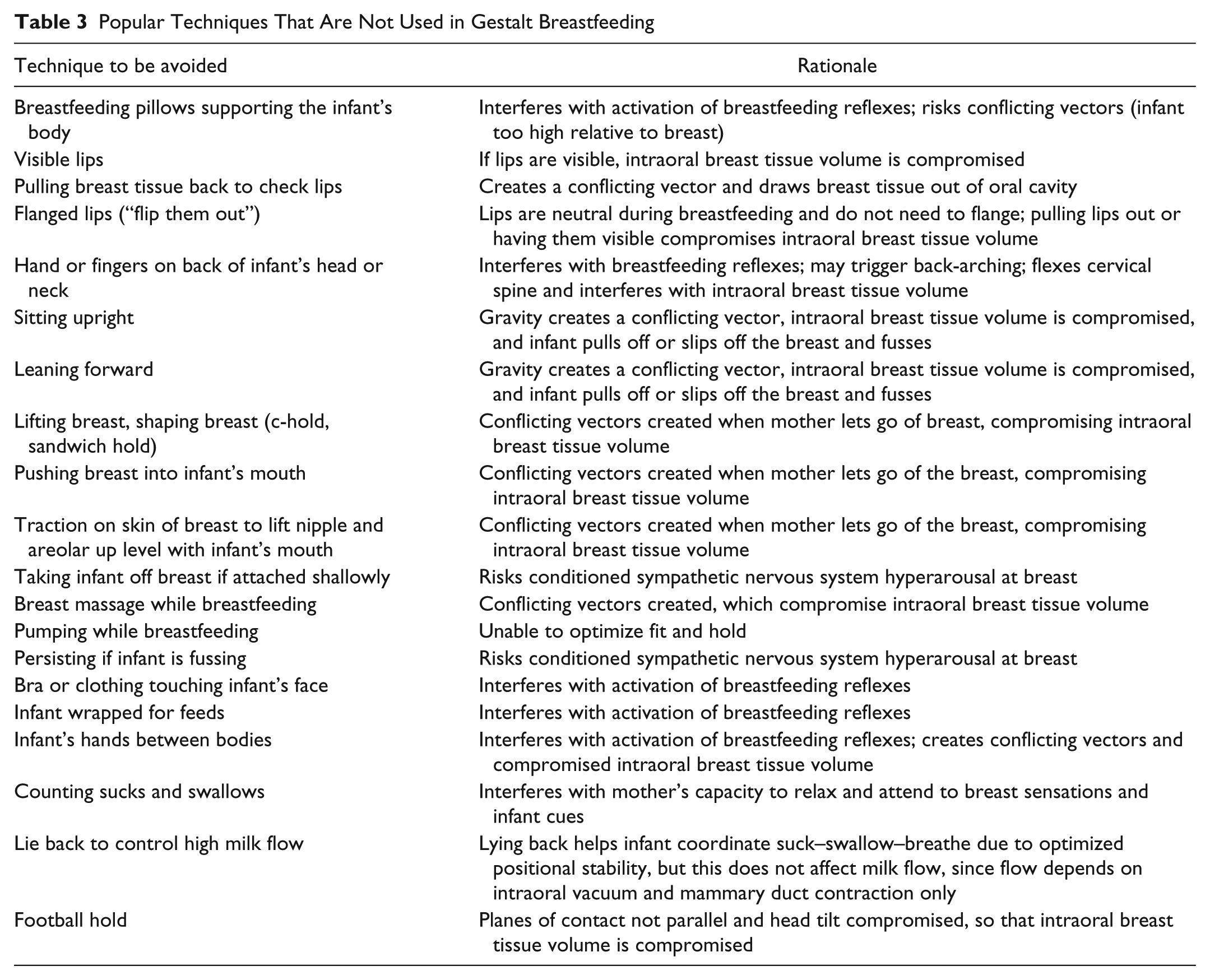
Step 1 includes a short demonstration video illustrating the biomechanics of healthy infant suck. A knitted breast is used to illustrate the problem of breast tissue drag, the desired outcome of optimal intraoral breast tissue volume, and symmetrical face–breast bury. The breastfeeding support professional then helps the mother–infant pair experiment with Steps 2 through 4 in an iterative and flexible way. Many techniques popularly used in clinical breastfeeding support are not used in gestalt breastfeeding, because they interfere with the infant’s breastfeeding reflexes and intraoral breast tissue volumes (see Table 3).
Popular Techniques That Are Not Used in Gestalt Breastfeeding
Step 2: Preparing Body and Mind for Comfortable Breastfeeding
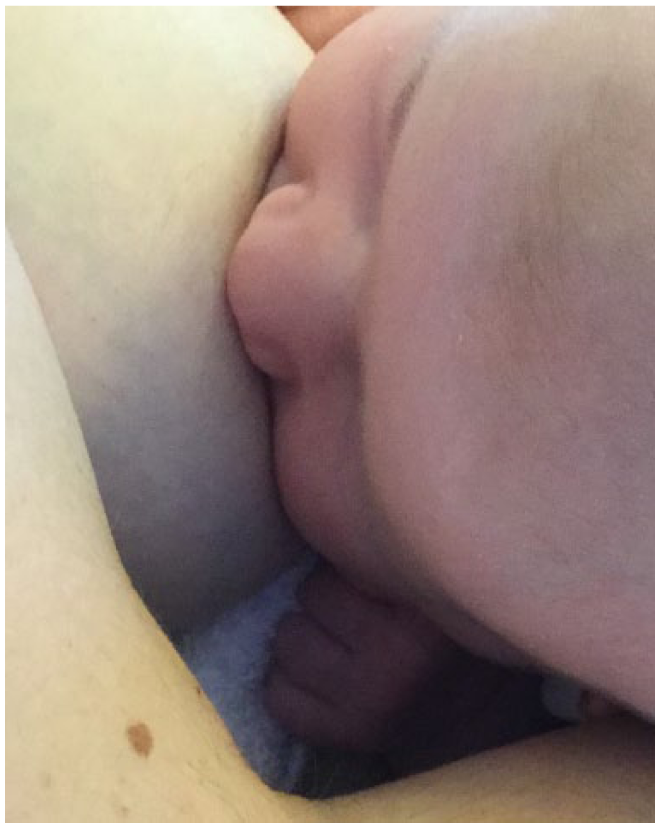
The semireclined position helps activate the infant’s breastfeeding reflexes and allows the woman’s body and shoulders to relax, as her lap opens up (Colson et al., 2008; Schafer & Watson Genna, 2015; Smillie, 2016). Breastfeeding often improves in the semireclined position, but this is not because gravity slows down milk flow. Milk flow depends on the vacuum generated intraorally in tandem with mammary duct contraction. Breastfeeding improves in the semireclined position because the infant is more positionally stable and better able to coordinate sucking, swallowing, and breathing (see Figure 1).

The semireclined position in gestalt breastfeeding, with good spinal alignment and face–breast bury. If the mother were to tuck the infant’s pelvis further under her left breast and around her body, further extension of the neck would occur, but this fit and hold was proving workable for her and the infant.
The breast needs to be exposed so that a circular “landing pad” with an approximately 5-cm radius about the nipple and areola is available for the face–breast bury. The landing pad, and therefore the breastfeeding reflexes, can be compromised by encroachment of bras and clothing, by an upper arm held too close, or by the way in which a pendulous breast and nipple fall in relation to the abdomen.
Teaching a woman to lift and shape her breast increases the risk of nipple pain 4-fold (Thompson et al., 2016). This is because when she lets go of the breast, a vector of force is generated by the downward pull of gravity on the breast, which conflicts with the direction of the intraoral vacuum. Sometimes, the breast requires the support of a folded cloth underneath to expose an adequate landing pad. Occasionally, women with very generous breasts or downward pointing nipples need to lift the breast a little with their hand to expose an adequate landing pad. These women require careful education about the risk of generating a conflicting vector of force and how to use the infant’s face to carry the weight of the breast once they let go, so that there are no vectors of force conflicting with the intraoral vacuum, compromising intraoral breast tissue volume and positional stability (see Figure 2).

This mother with a generous breast presented with severe nipple pain and damage. She achieved pain-free effective breastfeeding by experimenting with the principles of gestalt breastfeeding. She is in a very reclined position, which does not show in this photo. Although the infant has some lateral flexion of the neck, due to the way the mother’s capacity to use her forearm as head support is constrained by the need to support her breast, she has found a fit and hold that is workable for them.
Breastfeeding problems are linked with maternal distress and anxiety, predisposing to mood changes (Dias & Figueiredo, 2015). Gestalt breastfeeding integrates applied functional contextualism (popularly known as Acceptance and Commitment Therapy), a third wave behavioral psychology (Whittingham & Douglas, 2016). Women are empowered to use strategies of conscious muscle relaxation, in particular of the shoulders and arms; deep breathing; cognitive defusion from difficult thoughts; “making room for” difficult feelings; and anchoring attention in the present moment, in order to respond to subtle changes in both infant cues and breast sensation. Gestalt breastfeeding relies on the concept of workability, also drawn from applied functional contextualism, to mitigate against the damaging effects of perfectionism.
Step 3: Switching on Your Baby’s Breastfeeding Reflexes
Gestalt breastfeeding teaches parents five strategies that switch on an infant’s breastfeeding reflexes (Colson et al., 2008; Schafer & Watson Genna, 2015; Smillie, 2016). These are most reliably achieved across diverse anatomic configurations in a cradle hold in the semireclined position:
The infant’s chest and abdomen lie flat against the woman’s body and breasts, facilitated by the semireclined position (see Figure 3).
The infant’s bare hands move freely in order to pat the breast and embrace the woman’s body and are never trapped between her and the infant’s body.
Firm pressure of the infant’s chin and lower lip on the breast stimulates mouth-opening and sucking reflexes (Cantrill, Creedy, Cooke, & Dykes, 2014). This occurs when the infant is positioned so that her or his face lies on the breast and the infant is able to orient herself or himself by moving the head with rooting or bobbing movements. It is not necessary to take the infant off the breast and reattach if the initial latch is shallow. Repeated attempts to achieve a wider gape or to bring the infant on with an “asymmetric latch” are often not successful, may worsen pain, and can cause a conditioned sympathetic nervous system hyperarousal at the breast for some infants (Douglas & Hill, 2013; Thompson et al., 2016). Instead of focusing on how the infant comes on to the breast, the mother is encouraged to commence micro-movements as soon as the infant starts sucking so that she or he is quickly positioned for optimal intraoral breast tissue volume as the feed progresses, with elimination of conflicting vectors.
The infant’s cervical, thoracic, lumbar, and sacral spines are aligned, with gentle forward spinal flexion achieved as the infant wraps around the maternal body. The neck is moderately extended, without lateral flexion or rotation of the cervical spine (see Figure 4).
Gentle pressure between the infant’s shoulder blades supports her or his core stability, allowing strong independent movements of the infant’s head and neck, although force is never applied. In contrast, a hand pressing on the back of the infant’s head or neck both flexes the neck and risks interfering with the infant’s breastfeeding reflexes and should be avoided (Thompson et al., 2016).

This woman presented at Day 3 with nipple pain. The infant was less able to tilt his head back when breastfeeding on the right at first, due to the delicate shape of her breast. His most workable fit and hold was vertically down her body in a reclined position.

He also fed comfortably in a reclined cradle hold.
Step 4: Applying the Power of Micro-movements
Micro-movements are small experimental movements of the infant’s body relative to the woman’s breast and body, made by the woman as she supports the infant in her arms at the same time as gravity draws the infant into her body. Movements of 1 or 2 mm at a time are made in multiple directions and frequently throughout the feed. One kind of micro-movement occurs as the woman uses her forearm to change the angle of the infant’s facial contact with the breast; another kind of micro-movement occurs as she slides the whole of the infant’s body against hers. Experimentation with micro-movements, by observing the infant’s responses and mindfully attending to changing breast and nipple sensation, is key to effective pain-free milk transfer. Micro-movements ensure that the infant is relaxed and stable and that the woman is able to find a fit and hold in which she experiences a deep drawing sensation of her breast tissue, without pinching or pain.
The forearm is used as a lever to achieve face–breast symmetry, so that the lower half of the face is deeply buried into the breast, creating an interface line that is parallel to, or square with, the breast (see Figure 5). This is vitally important in the context of unpleasant nipple sensation or pain. Four points—the nose and buried upper lip (with the nose either apposed to the breast or just a millimeter or two above it), both cheeks, and the chin—are symmetrically buried into the breast (Thompson et al., 2016). The lips sit neutrally against the breast and are not visible. They do not need to flange, and if they are visible, intraoral breast tissue volume is compromised (Douglas & Geddes, 2017). Pulling the breast tissue back to visualize the infant’s lips, or using a finger to make the lips turn out, pulls breast tissue out of the intraoral cavity and should be avoided. Once a workable position has been found, the mother’s elbow typically requires the support of a firm cushion, so that her shoulder and arm can relax and musculoskeletal pain does not occur.
In an effective face-bury, the lower half of the face is buried into the breast, with a parallel or square face–breast interface. The four points of the nose, cheeks, and chin are symmetrically buried. The lips are not visible.
After permission to touch the woman’s arms is obtained, the breastfeeding support professional may ask the mother to take deep breaths and consciously relax her shoulders and arms as she holds her infant against her body. Then, the breastfeeding support professional places hands gently on the woman’s forearms to assist with micro-movements, carefully optimizing the face–breast interface and asking the woman for feedback about breast sensations. Together, the woman and breastfeeding support professional watch and respond to the infant’s subtle cues. This hands-on work helps the mother to lay down new neurological pathways in the clinical consultation, so that she can retrieve somatic memories when experimenting for herself later.
Once the biomechanics of infant suck are properly explained, it becomes clear to parents that digital tongue massage, other orofacial muscle stretching and massage, and oral connective tissue stretching will not alter sucking dynamics in neurotypical infants with breastfeeding difficulty. This kind of manual therapy risks disempowering the mother–infant pair, by shifting the focus from the mother’s empowered capacity to achieve optimal milk transfer through bodily fit and hold to an externally applied, “fix the baby” intervention. Frequent digital intraoral maneuvers also risk oral aversion.
Step 5: Experimenting With “Around the Dial” Breastfeeding
Once women understand the biomechanics of breastfeeding and have experienced the benefits of strategies for ensuring optimal intraoral breast tissue volume, they may choose to experiment with gestalt breastfeeding in a range of positions “around the dial” of the breast. All positions around the dial require the same attention to the details of positional instability, face–breast symmetry, and intraoral breast tissue volume.
Lying down breastfeeds may be addressed in the first consultation, because of night management benefits. Maternal hips and knees should not be flexed, firm pillow support behind the mother’s spine is required, and the infant lies on her or his side, pressed flat against the mother’s body. The mother’s arm is not under the infant’s head.
Other positions around the dial are usually only explored later. The koala position often creates conflicting vectors and, in our experience, works for a minority of women, depending on lap length and other anatomic configurations. We almost never use the football hold, due to the high incidence of conflicting vectors observed in this position. In time, women learn to replicate the bodily sensations of gestalt breastfeeding in situations of minimal postural recline.
Conclusion
Maternal nipple pain and infant behaviors such as back-arching during breastfeeds, crying and fussing with breastfeeds, or difficulty fitting onto or staying on the breast are often signs of positional instability. Current fit and hold interventions, including hands-off mammalian approaches, do not improve breastfeeding outcomes, including in randomized controlled trials. Given the limitations of existing fit and hold interventions, it is not surprising, then, that signs of positional instability are often inappropriately medicalized by breastfeeding support professionals who hope to offer solutions. For example, in the absence of classic tongue-tie, many mother–infant pairs with positional instability problems are referred for laser frenotomies of the lingual and maxillary labial frenula (Joseph et al., 2016; Walsh, Links, Boss, & Tunkel, 2017), despite lack of evidence of efficacy and risk of side effects (O’Shea et al., 2017). There is an urgent need for an effective, reproducible (yet flexible and woman centered) fit and hold intervention.
The authors of a recent systematic review, which found that breastfeeding mothers had difficulty transferring what they gained from existing interventions into real-life breastfeeding practices, called for theory-based breastfeeding interventions focused on modifiable causes of breastfeeding cessation and for intervention fidelity (Wood et al., 2016). Gestalt breastfeeding responds to this call by directly addressing the two most common reasons that parents give for commencing infant formula: nipple pain and unsettled infant behavior (Brown, Dodds, Legge, Bryanton, & Semenic, 2014; Odom et al., 2013; Redsell et al., 2010; Wasser et al., 2011). Gestalt breastfeeding integrates four theoretical frames: first, complexity science; second, physiologic breastfeeding initiation; third, findings of ultrasound studies investigating the biomechanics of infant suck; and fourth, applied functional contextualism, a modern form of cognitive behavioral therapy. Building on these strong theoretical foundations, a novel intervention has been developed (see Table 4).
What Is New About Gestalt Breastfeeding?
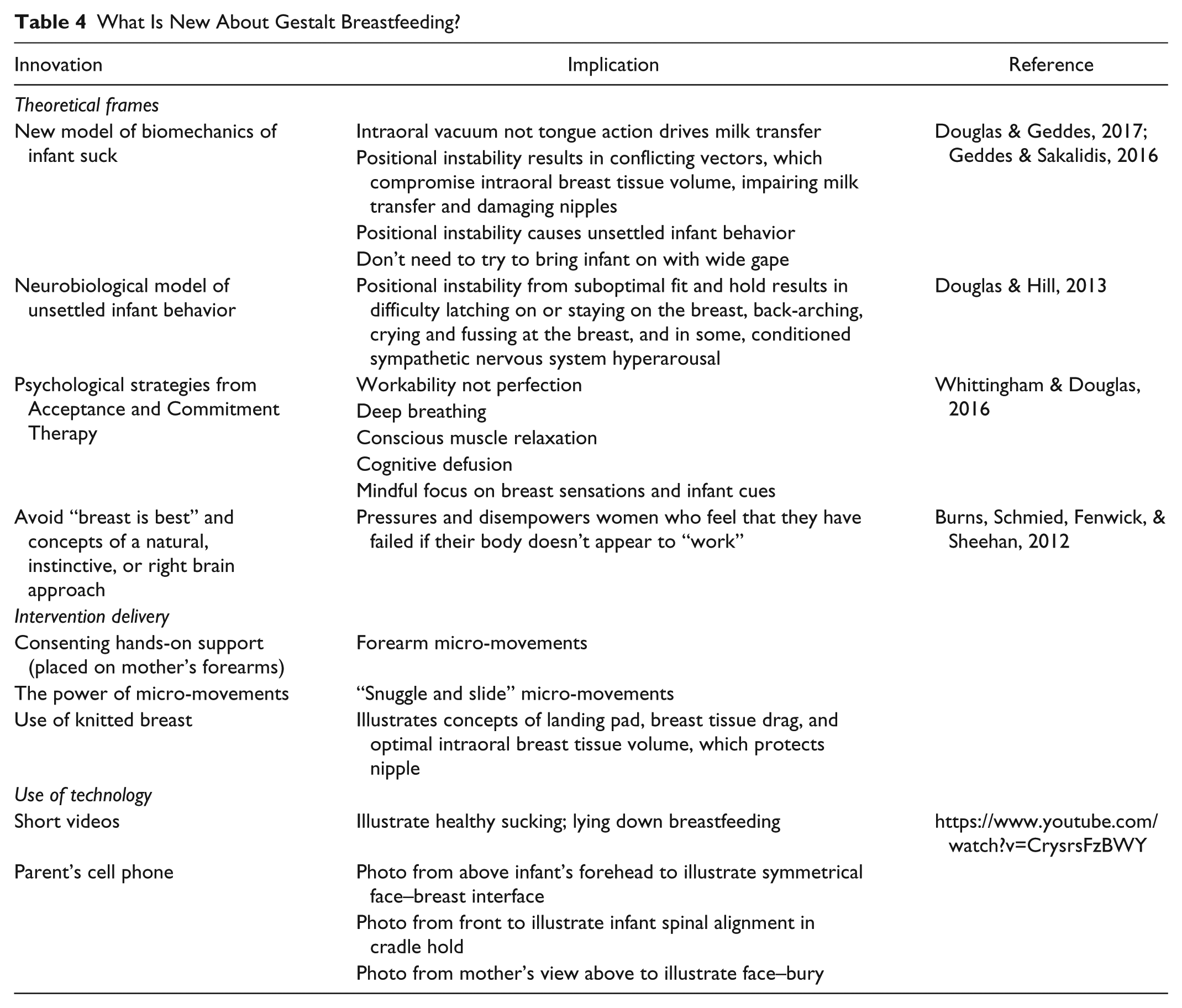
Gestalt breastfeeding aims to optimize positional stability and intraoral breast tissue volume, so that nipple pain is prevented or repaired and milk transfer optimized across a wide variety of maternal and infant anatomic diversities. Gestalt breastfeeding promotes the empowerment and resilience of the complex adaptive system of the breastfeeding pair, by supporting women to experiment with breast sensation and observation of and response to infant cues. Gestalt breastfeeding can be taught to breastfeeding support professionals and reproduced for research purposes, including in comparison studies with oral surgery. This new approach to clinical breastfeeding support has the potential to improve breastfeeding outcomes and is currently undergoing evaluation.
Footnotes
Acknowledgements
Gestalt breastfeeding builds on the work of many clinical breastfeeding support pioneers. In particular, the authors acknowledge the work of Anne-Marie Widström, Rebecca Glover, Jack Newman, Tina Smillie, Nancy Mohrbacher, Susan Colsen, and Cathy Watson Genna, all of whom will recognize elements of their contributions in gestalt breastfeeding. The authors recently discovered Robyn Thompson’s method, which has a similar focus on face–breast symmetry, and have used her four points of contact model in this article as another way of describing symmetrical face–breast bury. The Gestalt Breastfeeding Online Program, including videos of application in various cases, photographs, and greater detail of the strategies used in gestalt breastfeeding, is available online at ![]() . Accreditation of health professionals in the application of gestalt breastfeeding is available at
. Accreditation of health professionals in the application of gestalt breastfeeding is available at
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Pamela Douglas is the medical director of a charitable organization, The Possums Clinic (Possums for Mothers and Babies Ltd.). Ms Renee Keogh is a Lactation Consultant at The Possums Clinic. This organization sells two online products, the Gestalt Breastfeeding Online Package and the Possums Sleep Film (![]() ). All revenue goes toward further development of evidence-based education programs for parents and health professionals.
). All revenue goes toward further development of evidence-based education programs for parents and health professionals.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.