Abstract

Breastfeeding is a human right for both mothers and infants because, by having breastfed or by being breastfed, nutritional status and health outcomes are more successful than when human milk substitutes are used (Victora et al., 2016). This stark difference is even more exacerbated during a crisis (Gribble, 2017). The importance of breastfeeding escalates, but unfortunately, the support for it is often compromised. Even those women who are breastfeeding at the start of a crisis can be pushed off course by inadequate support and detrimental aid practices such as the blanket distribution of formula (Gribble, McGrath, MacLaine, & Lhotsha, 2011). Nurture Project International (NPI) seeks to improve breastfeeding rates among families living in crisis by providing technical lactation support from International Board Certified Lactation Consultants and peer counselors as well as drafting and implementing training for local health professionals, peer supporters, and traditional birth workers.
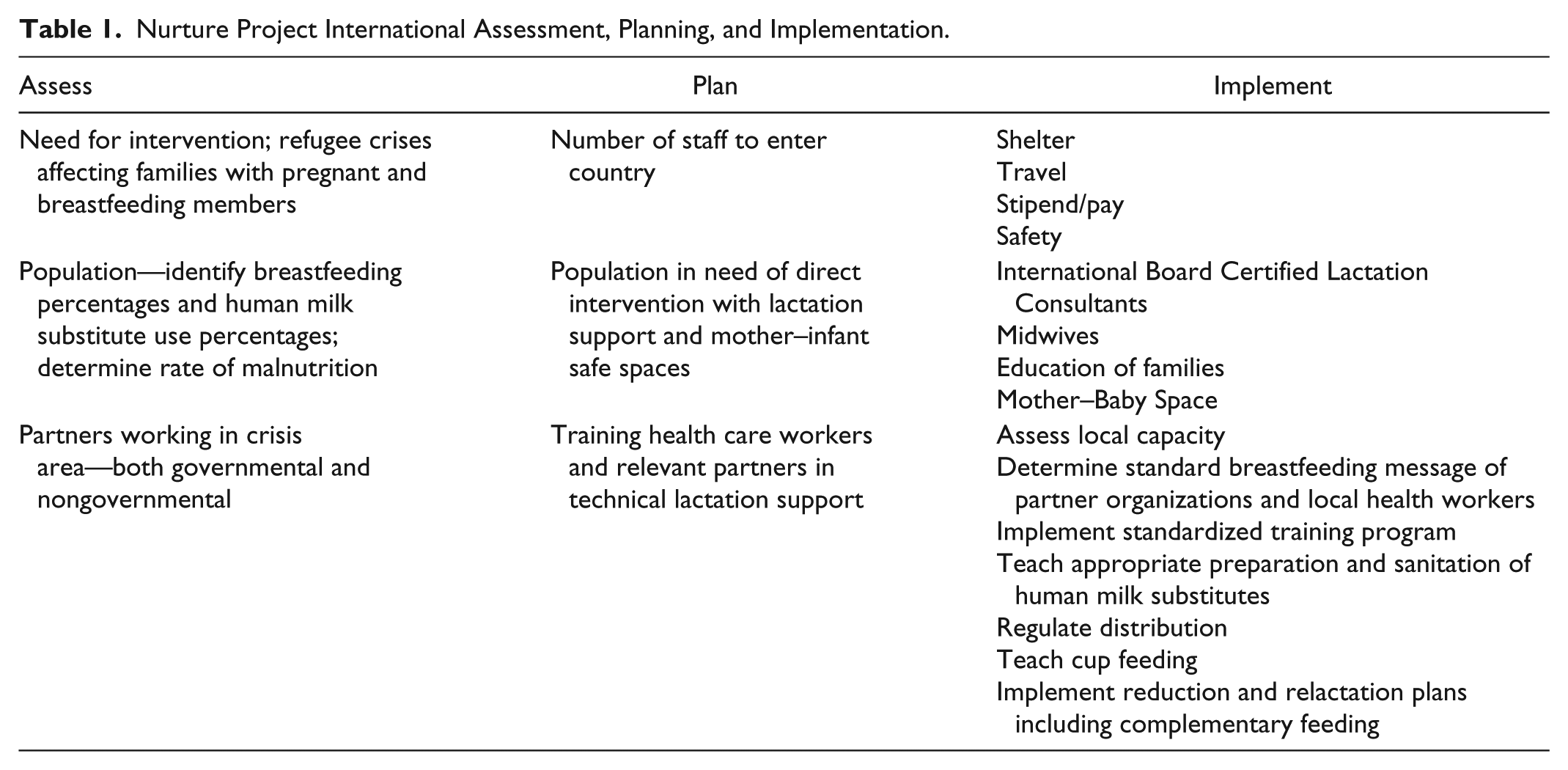
The challenges of life in crisis are intensified when someone is pregnant or lactating and if there are small children present—a population particularly vulnerable to malnutrition and disease (Carothers & Gribble, 2014). Increasing breastfeeding rates can improve nutrition and decrease illness (Carothers & Gribble, 2014). In addition to supporting breastfeeding, NPI provides technical support for nonbreastfed infants and their parents in order to establish and implement reduction and relactation plans to safely eliminate human milk substitutes whenever possible. NPI seeks to provide holistic care from pregnancy through birth and beyond and to train local health clinics with the evidence-based breastfeeding education needed to effectively support breastfeeding in crises (see Table 1 for the process). Currently, NPI is working in three countries. This work is detailed below to show NPI’s impact and extrapolate lessons learned from its work thus far.
Brooke Bauer, MPH

Nurture Project International Assessment, Planning, and Implementation.
Lactation Work in Refugee Camps
Greece
After years of conflict in Iraq, Afghanistan, and Syria, refugees have been fleeing these war-torn countries for safety in Europe (International Rescue Committee [IRC], 2017a). Nearly a half million people have made this journey with more than 100,000 refugees coming to Greece in the first half of 2017 (United Nations High Commissioner for Refugees, 2017a). As this area continues to be overwhelmed with new entries, services are hard to provide to an already overcrowded population (United Nations High Commissioner for Refugees, 2017a). Inadequate support for infant feeding in emergencies is problematic (Gribble et al., 2011). Larger nongovernmental organizations, traditionally responsive to disasters and supportive of breastfeeding in crises, do not focus their attention specifically on technical infant feeding support and instead provide general breastfeeding counseling and messaging. Furthermore, policy initiatives to support breastfeeding create the unforeseen problem of not appropriately responding to nonbreastfed infants. Smaller, more agile, but less experienced nongovernmental organizations fill the gap and frequently respond by providing donated human milk substitutes without the necessary education and support. NPI remedies this problem by meeting parents where they are and safely reducing human milk substitute use while focusing on relactation with technically skilled lactation care.
NPI facilitates safe human milk substitute use, when medically necessary, by (a) working within the community to meet nonbreastfed infants in their homes, instructing parents on proper preparation and sanitation, and providing long-term follow-up and support, (b) supplying adequate quantities of a human milk substitute, (c) focusing on safer methods of delivery such as cup feeding, (d) creating human milk substitute reduction plans either through relactation or introduction of complementary feeding, and (e) working in a multisectoral manner to advocate for technical infant feeding support. By taking control of all nonhuman milk products in the camps, implementing reduction plans through relactation efforts and the introduction of complementary foods, and working with key stakeholders, NPI’s interventions were able to decrease human milk substitute use. Depending on the camp, use was as high as 40% to 60%. Within several months, the rate plummeted to 0% in two camps and only 3% in another due to a medical need.
Iraq
After more than a decade of war, Iraq has suffered such violence and destruction that more than 3 million people have been displaced (IRC, 2017b). In Iraq, NPI has encountered challenges with local health clinics distributing human milk substitutes as standard practice. For this reason and to ensure continued care when NPI exits the country, the programs in Iraq have shifted from direct lactation care to building local capacity through training programs. NPI’s intervention is focused on training local reproductive health workers based in East and West Mosul as well as traditional birth attendants within the displaced Yazidi community as well as operating a women and children’s center in Khanke Camp in Dohuk, Iraq.
NPI trains local health care workers and establishes a network of peer supporters in accordance with the Community Management of Acute Malnutrition programs (United States Agency for International Development, 2016). NPI designed and implemented lactation training in emergencies for health workers, consisting of 40 hr over 8 days to include pre- and postlactation assessments. Additionally, health care workers are mentored during clinical lactation consults by NPI staff in the country. NPI’s community peer support training consists of workers receiving 20 hr of training followed by appropriate assessment and antenatal education. Peer supporters accompany NPI staff on home visits to see and discuss the dynamics of a lactation visit. It is NPI’s goal to standardize this training program and utilize it to combat malnutrition in all emergency situations in which NPI works.
Through training health care workers, NPI has been able to increase awareness of the importance of breastfeeding in emergencies and to create standard messages among clinic staff, emphasizing that (a) women can breastfeed in emergencies, (b) breastfeeding is the best source for ensuring infant health and nutrition in this dire situation, and (c) knowledge and support are available. By including the training of traditional birth assistants, NPI has been able to reach significantly more camp residents.
Bangladesh
In August 2017, the Arakan Rohingya Salvation Army attacked border police stations, and in response, the Myanmar government issued counter attacks against the Rohingya population (IRC & Relief International [RI], 2017). It has been reported that more than 600,000 Rohingya entered Bangladesh since late August because of these attacks (International Organization for Migration, 2017). It was estimated that by October 2017, 800,000 Rohingya were living in Bangladesh (IRC & RI, 2017). The speed and magnitude of these arrivals have overwhelmed the capacity of the government of Bangladesh and humanitarian agencies to respond to immediate needs (IRC & RI, 2017). Cox’s Bazar, the major entry point for the Rohingya, is already coping with poor performance in child-related indicators and vulnerability to natural disasters and is now confronted with a dire humanitarian crisis (World Health Organization, 2016).
In its Supplementary Appeal regarding the Myanmar refugee crisis, the United Nations High Commissioner for Refugees (2017b) identified infant and young child feeding practices as a health and nutrition goal to be supported. The Nutrition Sector (personal communication, 2017), in an Emergency Nutrition Assessment, echoed the importance of supporting nutrition by revealing the dangerous levels of malnutrition suffered by those entering Bangladesh. This report focused on women and children younger than 5 years and pointed out poor infant and young child feeding practices as a problematic area to be addressed. Furthermore, the joint report by the IRC and RI (2017) shows that 62% of families surveyed have a pregnant (18%) or breastfeeding (44%) member, thus underscoring the need for expert, technical lactation care to improve the nutrition status of this vulnerable group (p. 5).
Among infections, diarrhea and pneumonia account for the most childhood deaths (Black, Morris, & Bryce, 2003). The IRC/RI assessment identified that 73% of respondents have a cough and 82% reported having a cold (IRC & RI, 2017, p. 9). Also concerning is that 31% of families reported diarrhea (IRC & RI, 2017, p. 9). The Nutrition Sector Emergency Nutrition Assessment (2017) reiterated these dangerous percentages and expressed concern over the percentage of exclusive breastfeeding among infants younger than 6 months. Exclusive breastfeeding may mitigate the risk of infants dying from diarrhea or respiratory infection (Victora et al., 2016). Considering the high rates of illness among refugees, it is critical for these families to receive technical breastfeeding support to improve their health status.
NPI has deployed one team to assess the needs of families and to develop an appropriate response. NPI will likely utilize a direct contact approach, initially, as well as partner with relevant actors on the ground to help inform best practices and reach the most malnourished children. NPI teams will then focus on training local health care workers on technical infant and young child feeding response as well as using the newly released Community Management of Infant Malnutrition toolkit with technically trained traditional birth assistants, local reproductive health workers, and community health volunteers. Through consulting and outreach, NPI has been able to help inform the practices of those in contact with mothers and infants as well as reach the most malnourished children through lactation support and relactation help.
Lessons Learned
Each experience thus far has yielded important lessons to be learned. In Greece, NPI realized that a rapid and efficient response to nonbreastfed infants significantly improved breastfeeding rates in the camps. In Iraq, working with local health clinics, NPI discovered that it is essential to equip community health workers with evidence-based breastfeeding education to lessen the reliance on human milk substitutes and increase breastfeeding rates. The lessons from Greece and Iraq will be applied to NPI’s interventions in Bangladesh. Most certainly, there will be more things to learn during this intervention.
Challenges remain. Consistent and sufficient funding continues to be elusive. NPI began with a volunteer model because of a lack of funding. This is a difficult arrangement because there is too much turnover, particularly in the field. In Greece, volunteer lactation professionals would commit for about 2 weeks. This made passing information and continuing steady progress difficult. Going forward, NPI will seek paid staff for lactation positions in the field to ensure longer commitments, continuity of care for clients, and improved relationship building with partners. To ensure that this is possible, it is necessary for NPI to secure appropriate funding. In the past, larger donors expressed concern over the very specific nature of NPI’s work. As seen from the lessons learned, however, small, rapid, and targeted response has been the best way to address infant feeding problems in emergencies. Securing funding and moving to paid, staffed field positions will ensure that NPI is able to preassemble deployable teams to respond when and wherever disaster happens. Additionally, NPI will standardize all training materials and programs so that they can be readily implemented in any environment. This will include securing translators to translate all materials into the native language. Securing funding would dramatically change the impact of NPI.
Conclusion
NPI accomplishes this work by deploying teams of infant feeding specialists to include International Board Certified Lactation Consultants and peer counselors as well as midwives. The teams use a multisectoral approach and work in close partnerships with other nongovernmental organizations and government agencies, remaining flexible as the working environment constantly changes. NPI interventions are guided by the Operational Guidance for Emergency Relief Staff and Programme Managers, authored by the Infant Feeding in Emergencies Core Group (2017). In accordance with these regulations, NPI assesses the health and nutritional conditions of each contact and applies culturally sensitive interventions.
NPI has been effective in improving infant feeding in emergencies. By supplying knowledgeable, technically trained lactation support and rapidly responding to both breastfed and nonbreastfed infants, NPI has been able to dramatically improve breastfeeding rates in the emergencies in which it operates. Additionally, NPI has created specific lactation training for local health care workers and peer supporters so that they can effectively help parents breastfeed their children in crises. This small, rapid, targeted response is highly effective. Raising breastfeeding rates in emergencies improves health outcomes, allowing families to better recover from crises. For additional resources regarding infant and young child feeding in refugee crises, please see Table 2.
Infant and Young Child Feeding in Refugee Crises: Additional Resources.