
Abstract
Background:
Human milk is considered the gold standard for infant nutrition, but more data are needed that examine the constellation of weight-related concerns as barriers to exclusive breastfeeding.
Research aims:
The aim of this study was to examine how mothers’ concerns regarding their own and their infants’ weight, as well as disordered eating behaviors, were associated with breastfeeding self-efficacy and exclusive breastfeeding at 6 months.
Methods:
A prospective, quantitative, and self-report online survey design was used. Participants included 206 women (88.30% White, 59.20% with graduate degrees), with a mean age of 33.04 years (SD = 4.31 years) and a mean prepregnancy body mass index (BMI) of 24.80 kg/m2 (SD = 5.50 kg/m2), who had given birth within the past 6 months.
Results:
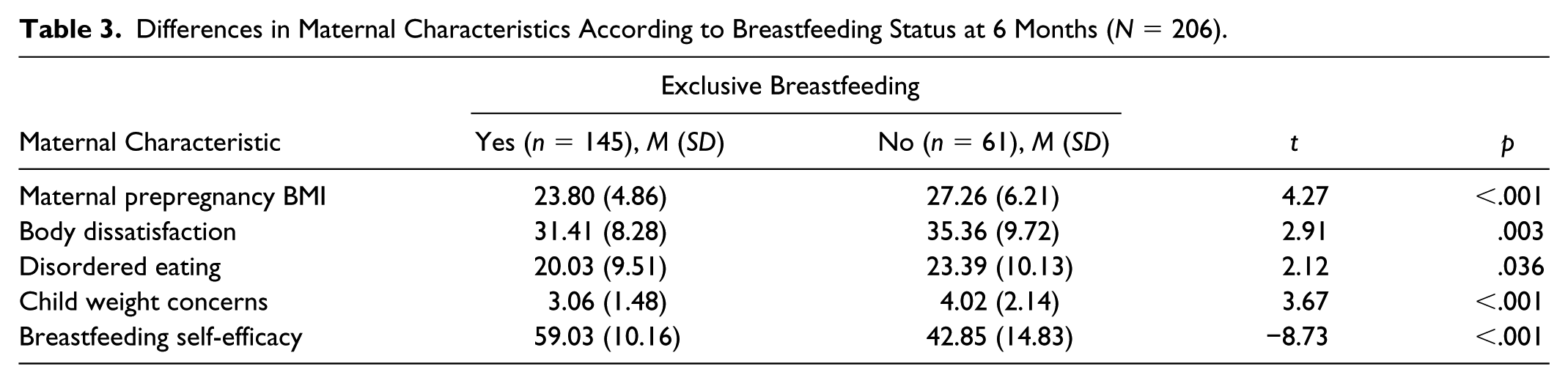
Participants who reported not exclusively breastfeeding at 6 months had significantly higher prepregnancy BMI (p < .001), higher body dissatisfaction (p = .003), more disordered eating (p = .036), higher child weight concerns (p < .001), and lower breastfeeding self-efficacy (p < .001). Mediation modeling revealed a direct negative relationship between prepregnancy BMI and exclusive breastfeeding at 6 months (p < .001). Indirect negative relationships between prepregnancy BMI and exclusive breastfeeding at six months via (a) body dissatisfaction, (b) disordered eating, and (c) child weight concern, as well as breastfeeding self-efficacy (entered as concurrent mediators), were all significant.
Conclusions:
Mothers’ weight, body image and eating concerns, concern regarding their children’s weight, and breastfeeding self-efficacy may constitute critical barriers to exclusive breastfeeding at 6 months. Interventions to improve breastfeeding duration and confidence should target maternal body image and eating concerns.
Background
Breastfeeding is considered the gold standard in infant feeding, as it provides ideal nutrition for infants. In fact, both the World Health Organization (2016) and the American Academy of Pediatrics (2012) recommend exclusive breastfeeding from birth until 6 months of life. In addition to the nutritional advantages, breastfeeding provides an array of benefits for the mother and infant. For the mother, these include a reduction in the risk for breast cancer, diabetes, cardiovascular disease, postdelivery complications, and postpartum depression (American Academy of Pediatrics, 2012). For the infant, breastfeeding offers immunologic and developmental advantages, with a recent meta-analysis indicating that breastfed children have an intelligence quotient 3.4 points higher than children who were never breastfed (Salone, Vann, & Dee, 2013; Victora et al., 2016). In addition, breastfeeding has been identified as an important protective factor against childhood obesity, with a dose-dependent relationship emerging, such that longer duration of breastfeeding is associated with lower risk for childhood obesity (Salone et al., 2013). Specifically, for every additional week that an infant is exclusively breastfed, it has been reported that the risk for childhood obesity decreases by 0.66% (Mosca & Gianni, 2017). Despite these important benefits of breastfeeding, exclusive breastfeeding rates remain relatively low in the United States. According to the 2016 Centers for Disease Control and Prevention (2016) Breastfeeding Report Card, 81.10% of women begin breastfeeding at birth and 51.80% are still breastfeeding at 6 months, with 22.30% exclusively breastfeeding at 6 months. Given these lower exlusive breastfeeding rates at 6 months relative to those who initiated breastfeeding at birth, it is important to determine the factors that may influence lower levels of breastfeeding, in an effort to establish mechanisms and strategies to better support mothers and their infants. The purpose of this study was to examine the pathways through which higher maternal weight was associated with lower rates of exclusive breastfeeding at 6 months to identify modifiable factors that may serve as intervention targets.
Key Messages
The constellation of weight-related concerns, as barriers to exclusive breastfeeding, remains unknown.
Mothers’ weight, body image and eating concerns, concern regarding their children’s weight, and breastfeeding self-efficacy constitute critical barriers to exclusive breastfeeding at 6 months.
Interventions focused on improving breastfeeding duration and confidence should also be targeted toward maternal body image and eating concerns.
One of the critical factors associated with lower rates of breastfeeding is high maternal weight. Maternal prepregnancy obesity has been reported to be highly associated with reduced breastfeeding initiation (Modrek et al., 2017) and duration (Averett & Fletcher, 2016). Grube et al. (2016) found that controlling for level of education and family income, breastfeeding duration was significantly shorter (2.7 months) among mothers with obesity compared with the normal-weight group. These data indicate that at the early timepoints after birth, mothers with obesity may encounter greater difficulties around breastfeeding. Although this relationship between higher maternal weight and poorer breastfeeding outcomes has been shown to be robust (Martinez, Chapman, & Perez-Escamilla, 2016; Ramji, Challa, Murphy, Quinlan, & Crane, 2017; Visram et al., 2013), the reasons for lower rates and shorter durations of breastfeeding among mothers with high weight are less well understood. However, it has been suggested that body-image issues, as well as other breastfeeding factors (e.g., poor latch, difficulty positioning the infant during breastfeeding, and poor human milk ejection), may also play a role (Grube et al., 2016). To date, research has not yet explored the role of body image in explaining the relationship between elevated weight and shorter breastfeeding duration; this represents an important gap.
Pregnancy and the postpartum period have been identified as periods of heightened vulnerability for weight and body-image concerns. Pregnancy typically moves women further away from sociocultural body ideals that emphasize thinness, and increasing pressure is placed on women to return to their prepregnancy shape and weight as quickly as possible (Flores, Mielke, Wendt, Nunes, & Bertoldi, 2018; Grube et al., 2016). This pressure to lose weight may result in heightened levels of body image distress after pregnancy, as well as disordered eating among a subsample of women through their efforts to accelerate weight loss (Wojcicki, 2011). Consistent with this, high rates of weight-related concerns and accompanying disordered eating have been documented among postpartum women (Lovering, Rodgers, Edwards George, & Franko, 2018) and have been associated with poor outcomes for mothers and infants (Lovering et al., 2018). In addition, women have reported experiencing stress related to postpartum weight loss and disordered eating (Fuller-Tyszkiewicz, Skouteris, Watson, & Hill, 2013; Lovering et al., 2018). Higher weight before and during pregnancy has been associated with increased body dissatisfaction (Skouteris, 2011; Skouteris, Carr, Wertheim, Paxton, & Duncombe, 2005). Thus, body-image and eating concerns may be critical for some women during the postpartum period and associated with higher weight before pregnancy.
The elevated levels of body-image and eating concerns experienced by some women during pregnancy and the postpartum period may contribute to explaining the association between higher maternal weight and lower rates of breastfeeding. Indeed, higher weight and accompanying body image concerns may lead some women to be less comfortable and self-efficacious while breastfeeding because of the increased focus and awareness of their bodies, which might be accompanied by negative thoughts and emotions. In addition, higher levels of body image concerns may lead some women to be more self-conscious when breastfeeding with others present or in public (Lovering et al., 2018). De Jager, Broadbent, Fuller-Tyszkiewicz, and Skouteris (2014) found that women with higher rates of body dissatisfaction postpartum were less likely to breastfeed and experienced lower breastfeeding self-efficacy. Similarly, the role of body image in exclusively breastfeeding mothers was examined at 6 months postpartum; the findings revealed that feeling fat was negatively associated with breastfeeding duration, as well as breastfeeding self-efficacy (Fuller-Tyszkiewicz et al., 2013). Lower breastfeeding self-efficacy mediated the relationship between feeling fat and shorter exclusive breastfeeding duration (de Jager et al., 2014). However, to date, few data are available regarding the role of disordered eating.
In addition to concerns regarding their own weight and shape, mothers may experience concerns regarding the weight of their infants or their tendency to gain weight over time (de Jager et al., 2015). These concerns have been shown to be particularly high among mothers with higher weight themselves (de Jager et al., 2015) and higher body dissatisfaction (Rodgers et al., 2013). Concerns regarding children’s weight have been associated with more controlling and restrictive feeding practices, which in turn have been associated with higher infant weight gain (Gregory, Paxton, & Brozovic, 2010; Thompson, 2013). Thus, higher maternal weight, body-image concerns, concerns regarding children’s weight, and feeding practices that promote greater weight gain seem to form a constellation of factors that may result from pressures surrounding weight and shape, paradoxically promoting greater weight gain in infants. To date, however, the role of breastfeeding in this constellation has not been examined. On the basis of the relationships described above, it is possible that concerns regarding children’s weight might mediate the relationship between higher maternal weight and lower breastfeeding self-efficacy and exclusive breastfeeding duration.
The aim of this study was to examine how mothers’ concerns regarding their own and their infants’ weight, as well as disordered eating behaviors, were associated with breastfeeding self-efficacy and exclusive breastfeeding at 6 months. Specifically, we hypothesized that the relationship between higher maternal weight before pregnancy and lower levels of exclusively breastfeeding at 6 months would be mediated by (a) maternal body-image concerns, (b) maternal disordered eating, and (c) maternal concerns for children’s weight, which in turn would be associated with lower breastfeeding self-efficacy (Figure 1).
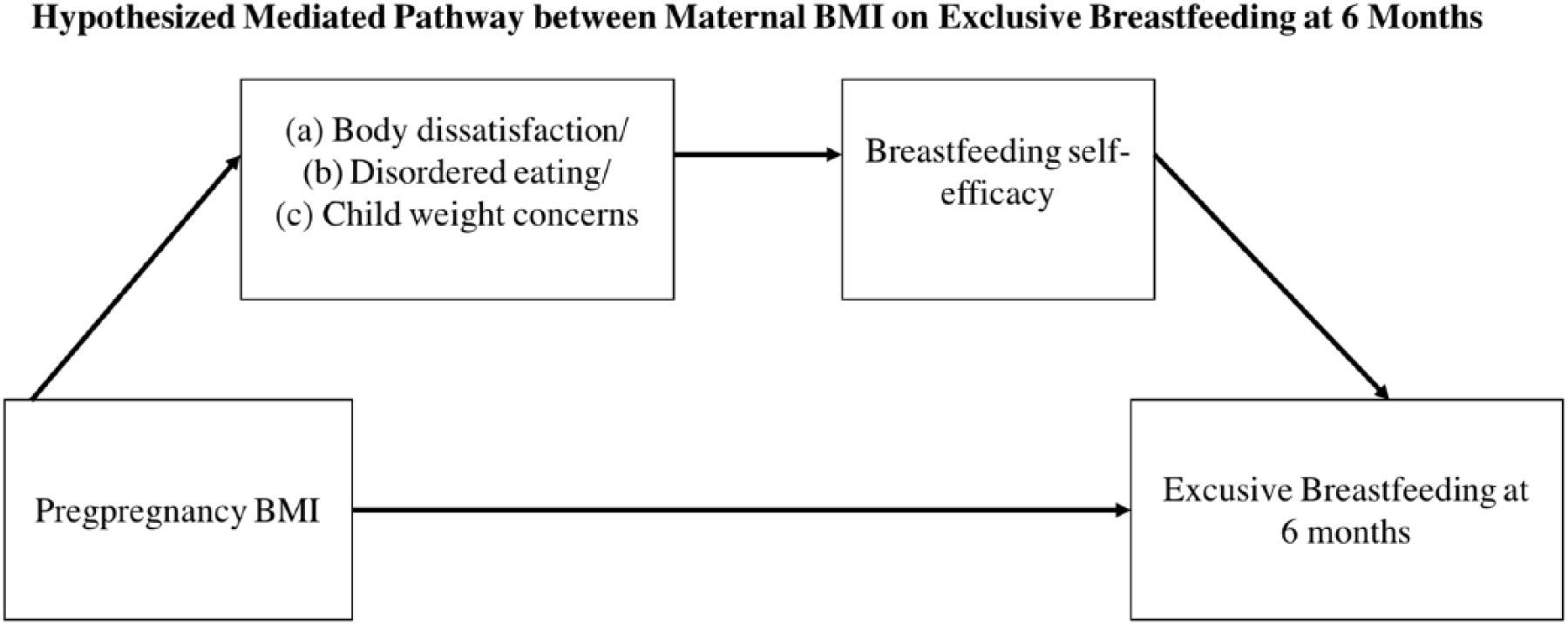
Hypothesized indirect relationships between prepregnancy body mass index (BMI) and exclusive breastfeeding at 6 months via maternal shape and weight concerns and breastfeeding self-efficacy.
Methods
Design
We used a prospective, quantitative, and self-report online survey design. This study design is the most appropriate to obtain data on the relation between mothers’ concerns regarding their own and their infants’ weight, as well as disordered eating behaviors, and breastfeeding self-efficacy and exclusive breastfeeding at 6 months. This study was approved by the institutional review board at Northeastern University.
Setting
The Web-based survey was administered using Qualtrics Version 2016 (Qualtrics, Provo, UT). Responses were collected in late 2016. The survey took participants approximately 20 minutes to complete. At the end of the survey, mothers were offered to take part in a raffle for an iPad mini.
Sample
The target population was mothers who had given birth within the past 6 months. The sample population was a convenience sample recruited via circulating flyers and the study link via social media and on pregnancy-related groups and forums. Eligible women were at least 18 years of age. Women were told that the decision to participate was voluntary and that they could stop the survey at any time.
Measurement
Demographic, maternal health, and infant information was collected using questionnaires designed by the researchers. Demographic variables included ethnicity, marital status, gender, and education. Maternal health variables included eating disorder history, mental health history, maternal weight (current, prepregnancy, and highest during pregnancy) and height, complications during pregnancy, delivery week, delivery type, exclusive breastfeeding, and diagnosed feeding complications. Participants reported on their infants’ sex, whether they were born preterm or full-term, their birthweight, and if they received care in the neonatal intensive care unit (NICU).
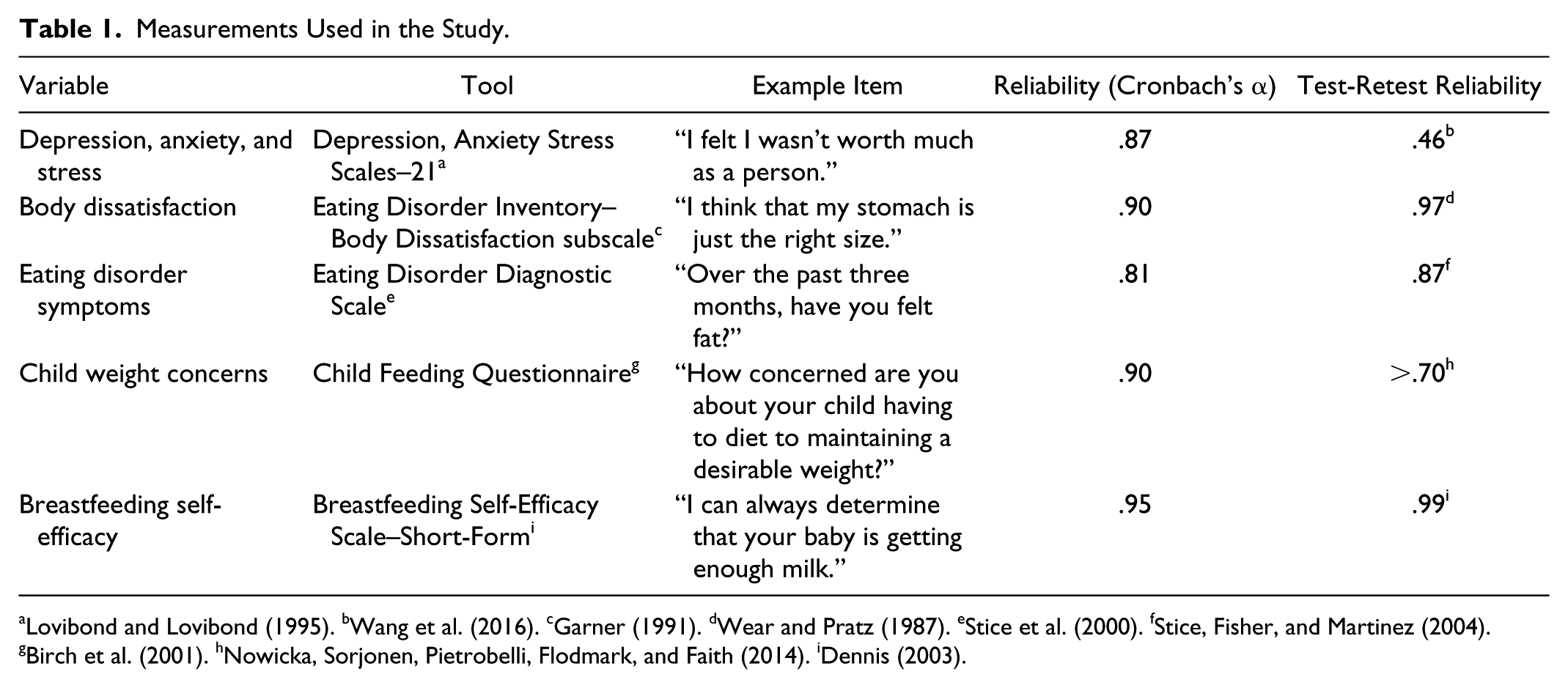
Next, the survey included the Eating Disorder Inventory–Body Dissatisfaction subscale (Garner, 1991), Child Feeding Questionnaire (Birch et al., 2001), Eating Disorder Diagnostic Scale (Stice, Telch, & Rizvi, 2000), Breastfeeding Self-Efficacy Scale–Short Form (Dennis, 2003), and Depression Anxiety Stress Scales–21 (Lovibond & Lovibond, 1995) (see Table 1).
Measurements Used in the Study.
Data Collection
Data were collected using the online survey platform Qualtrics. Women who met eligibility criteria accessed the survey through a link, which brought them to an electronic informed consent form. Upon consent, the participants could proceed to the first page of the survey. The survey was anonymous. Furthermore, all data were stored on secure, password-protected computers in our securely locked lab to ensure that confidentiality was maintained.
Data Analyses
SPSS Version 24.0 (IBM, Armonk, NY) was used to analyze these data. Descriptive analyses were conducted for all participants. The study sample was parsed according to breastfeeding status, and χ2 and independent-samples t tests were completed to examine differences in maternal and infant characteristics. Next, a correlations matrix was computed to examine bivariate associations among maternal characteristics and exclusive breastfeeding at 6 months. To better understand the relation among these variables, mediation analyses were conducted using the Process Macro (Birch et al., 2001). Bootstrapping analyses were used to examine indirect effects. Bootstrapping relies on conducting the analysis multiple times in random subsamples of the entire sample, to obtain a more reliable estimate of effects, and is recommended as a more conservative and powerful way of examining mediation effects (Hayes, 2013).
Results
Characteristics of the Sample
A sample of 206 women (mean age = 33.04 years, SD = 4.31 years) who had given birth within the past 6 months completed our online survey via Qualtrics. The sample characteristics are presented in Table 2. Participants reported their own information regarding marital status, education, sexual orientation, age, height, ethnicity, and if they had ever been diagnosed with an eating disorder. Participants were asked to report their prepregnancy weight and height. BMI was then calculated as weight (kg)/[height (m)]2, yielding a mean prepregnancy BMI of 24.80 kg/m2 (SD = 5.50 kg/m2).
Sample Demographic Characteristics (N = 206).
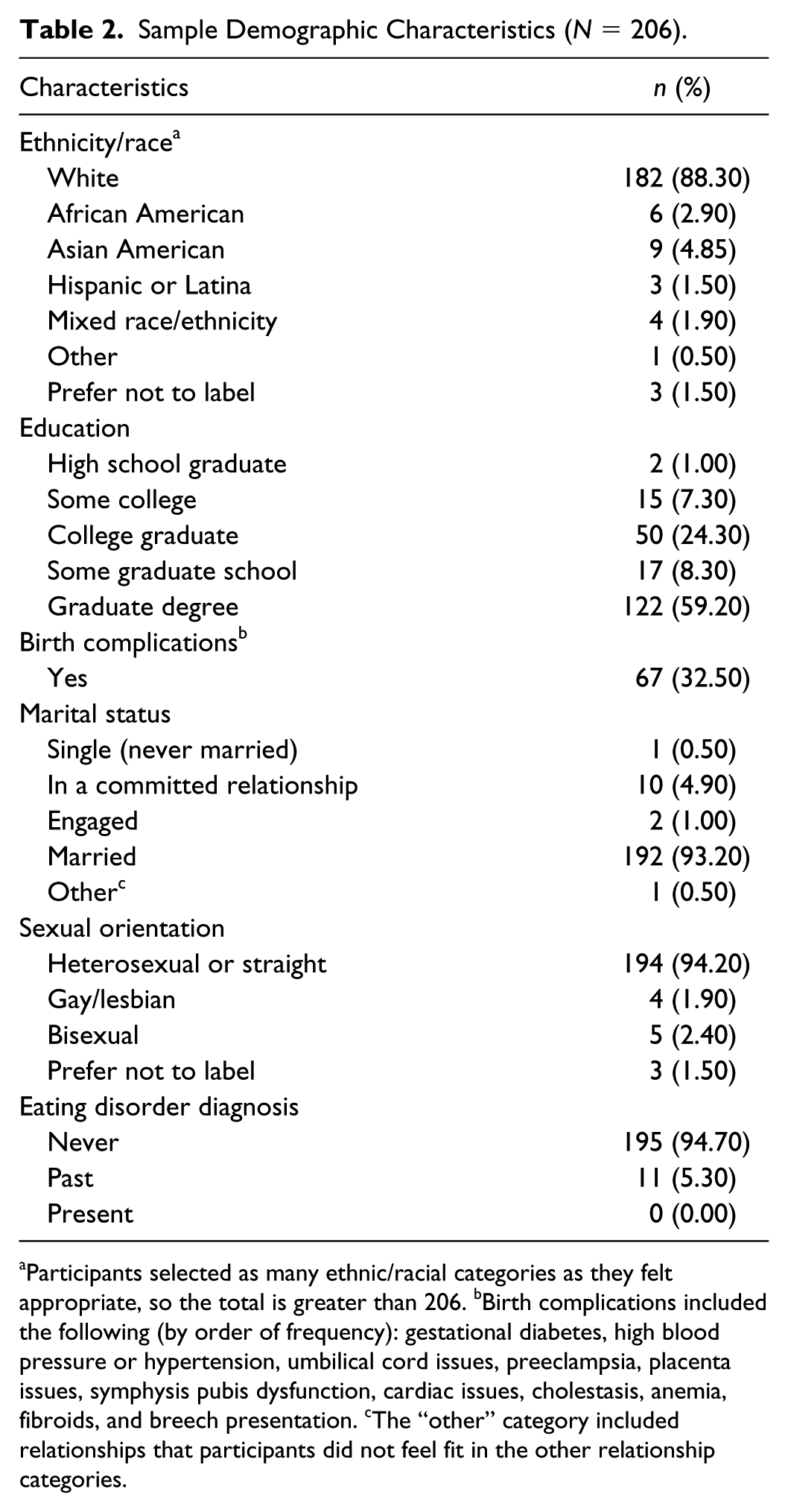
Participants selected as many ethnic/racial categories as they felt appropriate, so the total is greater than 206. bBirth complications included the following (by order of frequency): gestational diabetes, high blood pressure or hypertension, umbilical cord issues, preeclampsia, placenta issues, symphysis pubis dysfunction, cardiac issues, cholestasis, anemia, fibroids, and breech presentation. cThe “other” category included relationships that participants did not feel fit in the other relationship categories.
The descriptive statistics for a subsample of women who reported exclusive breastfeeding at 6 months (n = 145) are compared with a subsample of women (n = 61) who reported not exclusively breastfeeding at 6 months in Table 3. Among mothers who reported exclusively breastfeeding at 6 months, 14.50% identified as members of ethnic minorities, compared with 8% of those who did not exclusively breastfeed. Infants who had received care in the NICU (19.60%) were significantly less likely to no longer be exclusively breastfed by the age of 6 months, compared with infants who had not received care in the NICU (8%), χ2(1) = 5.33, p = .031. No differences were found for infant gender, χ2(1) = 0.02, p = 1.00, preterm status, χ2(1) = 2.10, p = .165, or birthweight, t(200) = −1.60, p = .112.
Differences in Maternal Characteristics According to Breastfeeding Status at 6 Months (N = 206).
Bivariate correlations among maternal variables were examined (Table 4). Findings revealed that overall, maternal characteristics were associated with one another. Specifically, higher prepregnancy BMI was associated with higher levels of body dissatisfaction, disordered eating, and child weight concerns, as well as lower levels of breastfeeding self-efficacy. Similarly, higher levels of body dissatisfaction were associated with higher levels of disordered eating, and both of these variables were associated with higher levels of child weight concerns, and lower levels of breastfeeding self-efficacy.
Bivariate Correlations Between Maternal Characteristics (N = 206).
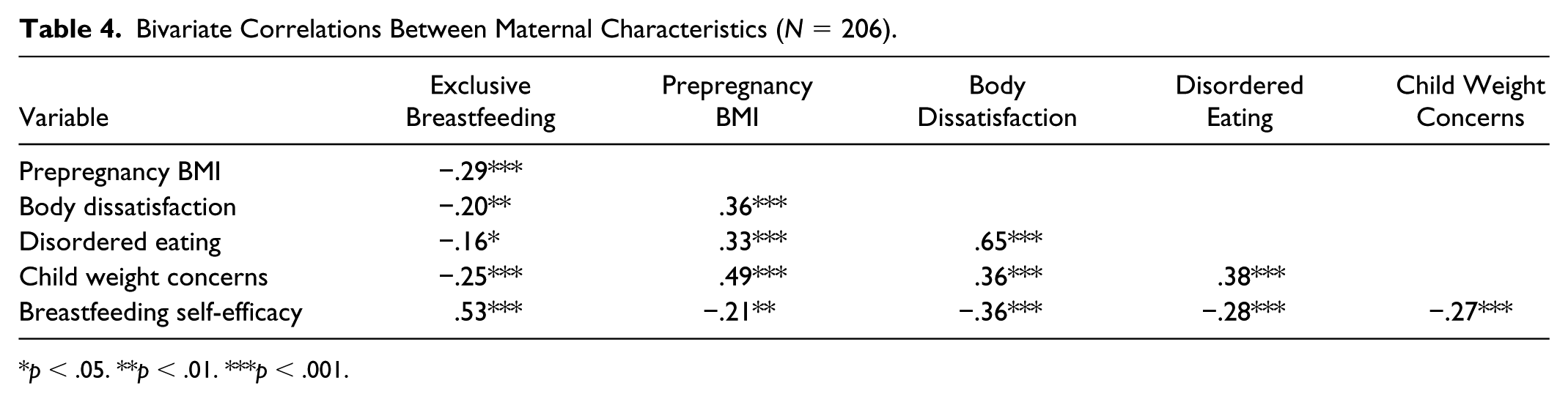
p < .05. **p < .01. ***p < .001.
To test the hypothesis that the association between maternal BMI and exclusive breastfeeding at 6 months was mediated by maternal body- and shape-related concerns and by maternal breastfeeding self-efficacy, the presence of significant indirect associations was examined (see Figure 1). The indirect relationship between prepregnancy BMI and exclusive breastfeeding at 6 months via maternal characteristics was tested using three successive models in which one of the maternal shape- or weight-related variables (body dissatisfaction, disordered eating, or child weight concerns) and breastfeeding self-efficacy were entered as two concurrent mediators.
Findings from 5,000 bootstrapped samples examining the indirect relationship between current BMI and exclusive breastfeeding at 6 months revealed that the hypothesized negative indirect association between prepregnancy BMI and exclusive breastfeeding at six months via body dissatisfaction and breastfeeding self-efficacy was significant (coefficient = −.03, SE = .013, 95% confidence interval [CI] = −.06 to –.01). In addition, the direct negative relationship between prepregnancy BMI and exclusive breastfeeding at 6 months was significant (coefficient = −.11, SE = .038, 95% CI = −.17 to –.04). The overall model significantly predicted exclusive breastfeeding at 6 months (p < .001). Similar results emerged when testing the indirect relationship between prepregnancy BMI and exclusive breastfeeding at 6 months via disordered eating and breastfeeding self-efficacy. Findings from 5,000 bootstrapped samples revealed that the hypothesized negative indirect association via both mediators was significant (coefficient = −.02, SE = .012, 95% CI = −.05 to –.01). In addition, the overall model significantly predicted exclusive breastfeeding at 6 months (p < .001), and the negative direct relationship between BMI and exclusive breastfeeding at 6 months was significant (coefficient = −.12, SE = .038, 95% CI = −.19 to –.04). Finally, a similar pattern emerged when testing the indirect relationship between prepregnancy BMI and exclusive breastfeeding at 6 months via child weight concern and breastfeeding self-efficacy. Findings from 5,000 bootstrapped samples revealed that the hypothesized negative indirect relationship via both mediators was significant (coefficient = −.02, SE = .014, 95% CI = −.06 to –.01). Again, the overall model significantly predicted exclusive breastfeeding at 6 months (p < .001), and the direct negative relationship between BMI and exclusive breastfeeding at 6 months was also significant (coefficient = −.10, SE = .040, 95% CI = −.17 to –.02). Thus, our findings provided support for all three mediated pathways.
Discussion
Overall, our findings confirmed that participants who were not exclusively breastfeeding at 6 months had higher prepregnancy BMI (Dennis, 2003) and suggested that higher body dissatisfaction, disordered eating, child weight concerns, and reduced breastfeeding self-efficacy may contribute to explaining this relationship. Previous data obtained from interviewing overweight mothers revealed that they often feel awkward breastfeeding in public because of possible exposure of their bodies (Hayes, 2013). In this way, body-shape and weight preoccupations stemming from the sociocultural context may account for the association between weight and lower rates of breastfeeding, suggesting that focusing on perceptions rather than weight itself might be a promising avenue for reducing this association.
Consistent with previous research (Briere, McGrath, Cong, & Cusson, 2014; Michels et al., 2017), our findings revealed a relationship between higher prepregnancy BMI and lower likelihood of exclusive breastfeeding at 6 months. However, this relationship was found to be mediated by a number of psychological factors. Although the role of body dissatisfaction as a barrier to exclusive breastfeeding at 6 months has been previously documented (Briere et al., 2014; Cartwright, Atz, Newman, Mueller, & Demirci, 2017; Ericson, Flacking, & Udo, 2017), the findings regarding the parallel roles of maternal disordered eating and concerns of the infant’s weight are novel and an important contribution. More specifically, the ways that sociocultural pressures surrounding body weight and shape may contribute to maternal behaviors aimed at altering appearance at the expense of health, in this situation, perhaps earlier breastfeeding cessation. Given the documented association between earlier breastfeeding cessation and higher risk for childhood obesity (Castillo, Santos, & Matijasevich, 2016; Tao et al., 2017; Visram et al., 2013), we suggest perhaps there is a paradoxical cycle whereby higher weight and associated concerns may lead to engaging in behaviors that place infants at increased risk for childhood obesity. Additional longitudinal research examining the bidirectional relationships between maternal concerns and behaviors and feeding and weight outcomes in infants is necessary to further explore these relationships.
Breastfeeding has been associated with a number of outcomes that may encourage women with body-shape and weight concerns to pursue it, including faster weight loss postpartum (Mosca & Gianni, 2017). However, recent data indicate that mothers may not be fully aware of the benefits of breastfeeding. Indeed, only half of mothers (n = 182) who were currently breastfeeding or had recently done so, reported knowledge that breastfeeding had a positive influence on their bodies. The following themes were described: (a) returning to prepregnancy body shape, (b) health benefits, (c) physical benefits, (d) eating benefits, (e) psychological benefits (Keddem, Frasso, Dichter, & Hanlon, 2018; Lau, Lok, & Tarrant, 2018). These low rates of knowledge surrounding the positive influence of breastfeeding further emphasize the need for more education for mothers.
Our findings may better elucidate who would benefit from more breastfeeding support and when that support should be provided. Prepregnancy BMI, in conjunction with weight and shape concerns, can contribute to identifying who may be at risk for cessation of breastfeeding prior to 6 months. In addition, our findings provide initial support for interventions targeting body image and eating concerns at the dyadic level. Previous researchers have suggested that these types of interventions might be most effective when presented to the mother before birth, as each mother’s planned breastfeeding duration has been reported to be associated with the actual duration of breastfeeding (de Jager et al., 2015). Ideally, breastfeeding support would be initiated during pregnancy and continued throughout the first year of life. Jiang et al. (2014) found that weekly text messages regarding infant feeding practices from the third trimester to 12 months postpartum significantly increased the median duration of exclusive breastfeeding. These data are consistent with other data showing that when mothers are counseled and educated on the benefits of breastfeeding, the rates of exclusive breastfeeding increased (McGinnis, Lee, Kirkland, Miranda-Julian, & Greene, 2018; Senghore, Omotosho, Ceesay, & Williams, 2018). To further understand these implications, researchers need to prospectively study breastfeeding interventions prior to birth and throughout the first year of life in randomized trials across many patient populations.
Limitations
A number of potential limitations need to be acknowledged, namely, the use of an online survey, which depended on a convenience sample with the potential for sampling bias and the possibility of inaccuracy of maternal report. It is likely that the way in which we recruited participants influenced the composition of the sample. Given these limitations, these data are difficult to generalize to mothers of different ethnicities and races, marital statuses, or education levels. Finally, our data were correlational, and prospective studies examining these relationships overtime will be better placed to examine temporal relationships.
Conclusions
Maternal weight, body-image and eating concerns, concerns regarding children’s weight, and breastfeeding self-efficacy may constitute critical barriers to exclusive breastfeeding at 6 months. Interventions to improve breastfeeding duration and confidence should include maternal body image and eating concerns. Further research exploring these findings across broad populations and ethnicities and races using longitudinal designs are warranted.
Footnotes
Acknowledgements
We would like to thank the mothers who participated in this survey.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.