
Abstract
Background:
Exclusive breastfeeding is recommended for the first 6 months of life and has significant benefits for both mother and child. Pregnancy-specific anxiety is a distinct and definable syndrome that has been identified as a robust predictor of pregnancy outcomes, but whether it is associated with exclusive breastfeeding status has not been determined.
Research aims:
To examine the association between pregnancy-specific anxiety in each trimester of pregnancy and exclusive breastfeeding status early in the postpartum period.
Methods:
Data were available from 412 women who participated in a longitudinal pregnancy cohort study. Pregnancy-specific anxiety and exclusive breastfeeding status were assessed using an online self-report questionnaire.
Results:
Logistic regression analyses showed that a one-unit increase in pregnancy-specific anxiety in the first (OR = 0.94, 95% CI [0.90, 0.98]) and third (OR = 0.95, 95% CI [0.91, 0.99]) trimester of pregnancy was associated with a 5–6% decrease in the odds of exclusive breastfeeding at 6–8 weeks postpartum.
Conclusions:
Pregnancy-specific anxiety was associated with lower odds of exclusive breastfeeding at 6–8 weeks postpartum. Prenatal interventions designed to increase exclusive breastfeeding duration may benefit from the incorporation of strategies that help reduce worries and concerns unique to the pregnancy experience.
Key Messages
Pregnancy-specific anxiety is a distinct and definable syndrome that has been identified as a robust predictor of pregnancy outcomes, but whether it is associated with exclusive breastfeeding status has not been determined.
Pregnancy-specific anxiety in the first and third trimester was associated with a decrease in the odds of exclusive breastfeeding at 6–8 weeks postpartum.
Prenatal interventions designed to increase exclusive breastfeeding duration may benefit from the incorporation of strategies designed to address worries and concerns unique to the pregnancy experience.
Background
Anxiety or distress related to pregnancy is a distinct and definable syndrome characterized by elevated worries or concerns about aspects unique to pregnancy (e.g., medical care, physical symptoms, bodily changes, infant health; Blackmore et al., 2016). Although pregnancy-specific anxiety may co-occur with more generalized anxiety, it is considered a contextually bound emotional state (Bayrampour et al., 2016). Over the last 20 years, researchers have shown that pregnancy-specific anxiety may be a more robust predictor of adverse perinatal and child health outcomes than other types of anxiety or stress that extend to or occur within the pregnancy period (e.g., state or trait anxiety, perceived stress, stressful live events; Guardino & Schetter, 2014). Despite the convergence of literature on the negative influences of pregnancy-specific anxiety, how it relates to exclusive breastfeeding (EBF) practices is not well understood (Fallon, Halford, Bennett, & Harrold, 2016).
EBF is recommended for the first 6 months of life due to the substantial short- and long-term health benefits for both infant and mother (American Academy of Pediatrics, 2012). For example, infants who are breastfed exclusively for less than 4 months are at an increased risk of infections in the respiratory and gastrointestinal tracts (Quigley, Carson, Sacker, & Kelly, 2016) and of ear, throat, and sinus infections (Li, Dee, Li, Hoffman, & Grummer-Strawn, 2014). In the long-term, breastfeeding may reduce the odds of overweight/obesity and Type 2 diabetes in childhood and later on in life (Horta, de Mola, & Victora, 2015). For mothers, the short-term benefits of breastfeeding include reductions in postpartum blood pressure among women with cardiometabolic complications during pregnancy (Countouris et al., 2016) and, for some, a reduced risk of postpartum depression (Borra, Iacovou, & Sevilla, 2015). In the long-term, a cumulative lifetime lactation of ≥ 12 months has been associated with a reduction in rates of breast and ovarian cancers (Chowdhury et al., 2015), and with lower rates of cardiovascular disease risk factors (e.g., Type 2 diabetes, hypertension; Bonifacino, Schwartz, Jun, Wessel, & Corbelli, 2018; Zhang, Zhang, Liu, Li, & Wang, 2015).
Although most women will initiate breastfeeding soon after birth, only 32% of Canadian women breastfeed exclusively for at least 6 months (Statistics Canada, 2018). Given the multifactorial nature of EBF, there has been significant work aimed at identifying modifiable factors associated with shorter breastfeeding duration. Aside from obstetrical (e.g., birth complications) and maternal-infant (e.g., maternal illness, short maternity leave, positioning and/or latching) characteristics that may influence breastfeeding practices, researchers have also identified several maternal psychosocial factors that influence breastfeeding initiation and EBF continuation. These factors include prenatal and postpartum depressive symptoms (Figueiredo, Canário, & Field, 2014), postpartum specific-anxiety (Fallon et al., 2017), generalized psychological distress (de Jager, Skouteris, Broadbent, Amir, & Mellor, 2015), and breastfeeding self-efficacy (Dennis, 2003). There has also been considerable interest in how prenatal anxiety (e.g., state/trait anxiety) relates to infant feeding practices. A recent review of this literature (Fallon et al., 2016) indicated that high prenatal anxiety was associated with reductions in breastfeeding intention and exclusivity, but that relationships between prenatal or pregnancy-specific anxiety and other infant feeding practices (e.g., breastfeeding initiation and duration) remain unclear.
Given the importance of pregnancy-specific anxiety and EBF for maternal and child health outcomes, the aim of this study was to examine the association between pregnancy-specific anxiety in each trimester of pregnancy and EBF status early in the postpartum period. We predicted that greater pregnancy-specific anxiety in each trimester of pregnancy would be associated with a significant reduction in the odds of EBF at 6–8 weeks postpartum.
Methods
Design
This study was a secondary analysis of existing data that were available from the Healthy Behaviours During Pregnancy and Postpartum Study. The study design was a prospective, longitudinal, self-report survey that was selected so data could be obtained at several timepoints across the pregnancy and postpartum period. Given that the perinatal period is a unique and demanding time for women, online self-report surveys were used to reduce participant burden and maximize study participation.
The primary study aim was to investigate the influence of behavioral and psychosocial factors on gestational weight gain, but data were also available on several other maternal, obstetrical, and infant health outcomes, including infant feeding practices. Ethics approval was granted by McGill Faculty of Medicine Institutional Review Board and the ethics review boards of the participating hospitals.
Setting
The study was conducted from May 2014 to February 2018 in Montréal, Québec, Canada (population 1.7 million). In the province of Québec, approximately 25% of women who initiated breastfeeding reported EBF for at least 6 months, slightly less than the Canadian national average (32%; Statistics Canada, 2018).
Women typically spent 24 to 48 hr in hospital following birth, depending on the type of delivery. To promote breastfeeding initiation, obstetrical teams at each hospital encouraged immediate skin-to-skin contact after delivery and monitored infant feeding practices during the hospital stay. Following hospital discharge, women were provided with a home-visit from a public health nurse to assess maternal (e.g., postpartum bleeding, pain, mood) and infant (e.g., weight gain, feeding practices) adjustment. At this visit, breastfeeding latch was assessed, if necessary, and parents were provided with information about breastfeeding support services available through nearby local community services centers and hospitals. These services can include free breastfeeding support groups, consultation with nurses and lactation specialists, and specialized hospital breastfeeding clinics. Infants were then seen by a physician at 2 and 4 weeks, and at 2, 4, and 6 months, and infant feeding practices were typically discussed at each appointment. All health care services offered in health clinics or hospital and community health service centers were provided free of charge to Canadian citizens and permanent residents under the publicly funded Québec provincial health care system.
Sample
Convenience sampling was used to recruit women who were ≥ 18 years of age with a singleton pregnancy who were ≤ 20.0 weeks gestation, able to communicate in English or French, and able to access the internet. Exclusion criteria were pre-existing Type 1 or 2 diabetes and gestational diabetes mellitus, due to dietary requirements and restrictions that may have influenced weight gain during pregnancy.
At study entry, 754 participants completed the online questionnaires. Of these participants, 299 (39%) withdrew or only provided partial data, and 37 (4.8%) had not yet reached the stage of completing the later follow-up. Women who withdrew or provided only partial data reported significantly greater depressive symptom severity in each trimester of pregnancy relative to women who responded to all four assessments. There were no differences between women who completed versus those who withdrew from the follow-up assessments on any other sociodemographic and psychosocial variables. A final sample of 412 participants provided complete data at all three timepoints during pregnancy and at the 2-month postpartum assessment (412/754, 54%) and were included in analyses.
As this study was a secondary analysis of existing data, a priori power analyses were not calculated to determine sample size adequacy. The final sample size is comparable to those reported in the literature on prenatal anxiety as a predictor of infant feeding outcomes (Fallon et al., 2016), and was adequate for the statistical analyses performed.
Measurement
Demographics
Data on maternal demographics (age, ethnicity, education, pre-pregnancy height, and weight), psychological variables (depressive symptom severity and pregnancy-specific anxiety), and obstetric characteristics (parity) were obtained through the online questionnaires. Maternal height and weight were converted to metric units to obtain pre-pregnancy body mass index (BMI) in kg/m2.
Breastfeeding Intention, Initiation, and EBF Status
Breastfeeding intention was assessed in the second trimester of pregnancy, and breastfeeding initiation and exclusive breastfeeding status were assessed at the first postpartum assessment. During the second trimester, participants were asked to indicate whether they planned to breastfeed their baby (yes/no) and, if so, for how long in months. At the postpartum assessment, participants were asked to indicate: (1) whether they had ever breastfed or expressed milk to feed their infant (breastfeeding initiation; yes/no); (2) whether they had completely stopped breastfeeding and expressed milk for their baby (yes/no); and (3) to indicate how old their infant was when he or she was first fed formula, or if their infant had never been fed formula. EBF was defined according to the World Health Organisation definitions for infant feeding (World Health Organisation, 2008) whereby the infant receives only human milk from birth onward and may include oral rehydration solution, drops, or syrups (vitamins, minerals, medicines).
Pregnancy-Specific Anxiety
The Prenatal Distress Questionnaire Revised (PDQ) is a 17-item self-report questionnaire that asks women to indicate the degree to which they feel bothered, upset, or worried about pregnancy-specific stressors (e.g., medical care, physical symptoms, parenting, bodily changes, and infant health) on a 3-point scale (not at all, somewhat, very much; Lobel et al., 2008) with total scores ranging from 0 to 34. In the present study, the PDQ demonstrated high internal consistency in the first (Cronbach’s α = 0.82), second (Cronbach’s α = 0.82), and third (Cronbach’s α = 0.83) trimesters of pregnancy, and were consistent with previously reported scale reliability (Alderdice, Lynn, & Lobel, 2012; Lobel et al., 2008). The PDQ has been associated with birth outcomes (e.g., preterm birth) and poor health behavior (e.g., smoking; Lobel et al., 2008). To our knowledge, however, the PDQ has not been used to predict breastfeeding outcomes.
Depressive Symptoms
The Edinburgh Postnatal Depression Scale (EDPS) was used to assess depressive symptoms during the perinatal period (Cox, Holden, & Sagovsky, 1987). The EPDS is a 10-item self-report questionnaire, with each item rated on a 4-point scale to produce a summative score ranging from 0–30; higher scores indicate greater depressive symptom severity (Cox et al., 1987). The EPDS has also been validated against standardized interview schedules and other self-report instruments for use during pregnancy (Bergink et al., 2011). In this sample, the EPDS demonstrated adequate reliability (Cronbach’s α > 0.80) in the first, second, and third trimesters of pregnancy. Depressive symptom severity was included as a covariate given that it has been previously linked to breastfeeding outcomes (Figueiredo et al., 2014). Depressive symptoms were assessed concurrently with pregnancy-specific anxiety in each trimester of pregnancy.
Data Collection
Pregnant women were recruited from obstetrical practices and prenatal clinics located within the three McGill University affiliated hospitals that cater to a large heterogenous and multiethnic population. These three sites are among the largest birthing centers in Montréal and together have over 11,100 deliveries annually. Potential participants were approached by a researcher who explained the study aims and determined whether they would be interested in participating. If they were, they were emailed a link to complete an online informed consent form that provided them with a description of the research project.
Following informed consent, participants were provided with a link to a secure website address where they could access and complete online, self-report questionnaires at five timepoints (12, 24, and 36 weeks gestation, and 6 weeks and 6 months postpartum) that were made available using FluidSurveys and Survey Monkey (www.surveymonkey.com). The questionnaires measured demographic information, emotional well-being, dietary knowledge, and lifestyle behaviors and took approximately 30–45 min to complete. Participants were given one week to complete the questionnaires and reminder phone calls were made, if necessary. To encourage ongoing study participation, participants were compensated through a lottery system at each data collection timepoint. Participants usernames were not stored with their responses and all data were stored securely and anonymously on a password protected server.
Data Analysis
Statistical analyses were performed using SPSS 24.0 (IBM, 2016) and RStudio (RStudio Team, 2016) using general linear modeling (GLM). Three logistic regression models were used to examine the association between pregnancy-specific anxiety in the first, second, and third trimester and EBF status. Breastfeeding status was collapsed into a binary variable and treated as the primary outcome. EBF was considered present (1) if participants indicated that their child was never fed formula, or absent (0) if their infant was fed formula one or more days after birth. Regression coefficients are presented as unstandardized beta coefficients (b) that denote the log odds of EBF associated with a one-unit change in PDQ total score. To assist with interpretation of the results, beta coefficients and confidence interval (CI) endpoints were exponentiated (elog odds) into an odds ratio (OR) metric (Hosmer, Lemeshow, & Sturdivant, 2013)
A range of potentially confounding variables were identified from previous literature that examined the association between pre- or post-partum psychosocial variables and breastfeeding outcomes (maternal age, ethnicity, education, income, parity, and pre-pregnancy BMI, depressive symptom severity in each trimester (Adedinsewo et al., 2014; Fallon et al., 2017). Bivariate analyses were conducted between the potential confounders, PDQ total score in each trimester, and EBF status. Confounders that were associated with PDQ total score in one or more trimesters of pregnancy and with EBF were included in the final regression models and resulted in the exclusion of maternal education.
Results
Participant Characteristics and Breastfeeding Practices
Maternal and infant characteristics and breastfeeding practices are presented in Table 1. On average, questionnaires were completed at 13.14 (SD = 2.20), 24.11 (SD = 2.22), and 36 (SD = 2.21) weeks of gestation, and at 7.56 (SD = 2.01) weeks after birth. Participant age at study enrollment ranged from 21–46 years (M = 33.28, SD = 4.21), and pre-pregnancy BMI from 16.14–60.57 (M = 23.55, SD = 4.81). The majority of infants were born at term (M = 39.19, SD = 2.27) and in the normal range of birthweight (M = 3440.08, SD = 563.96).
Characteristics of Maternal and Infant Pairs (N = 412).
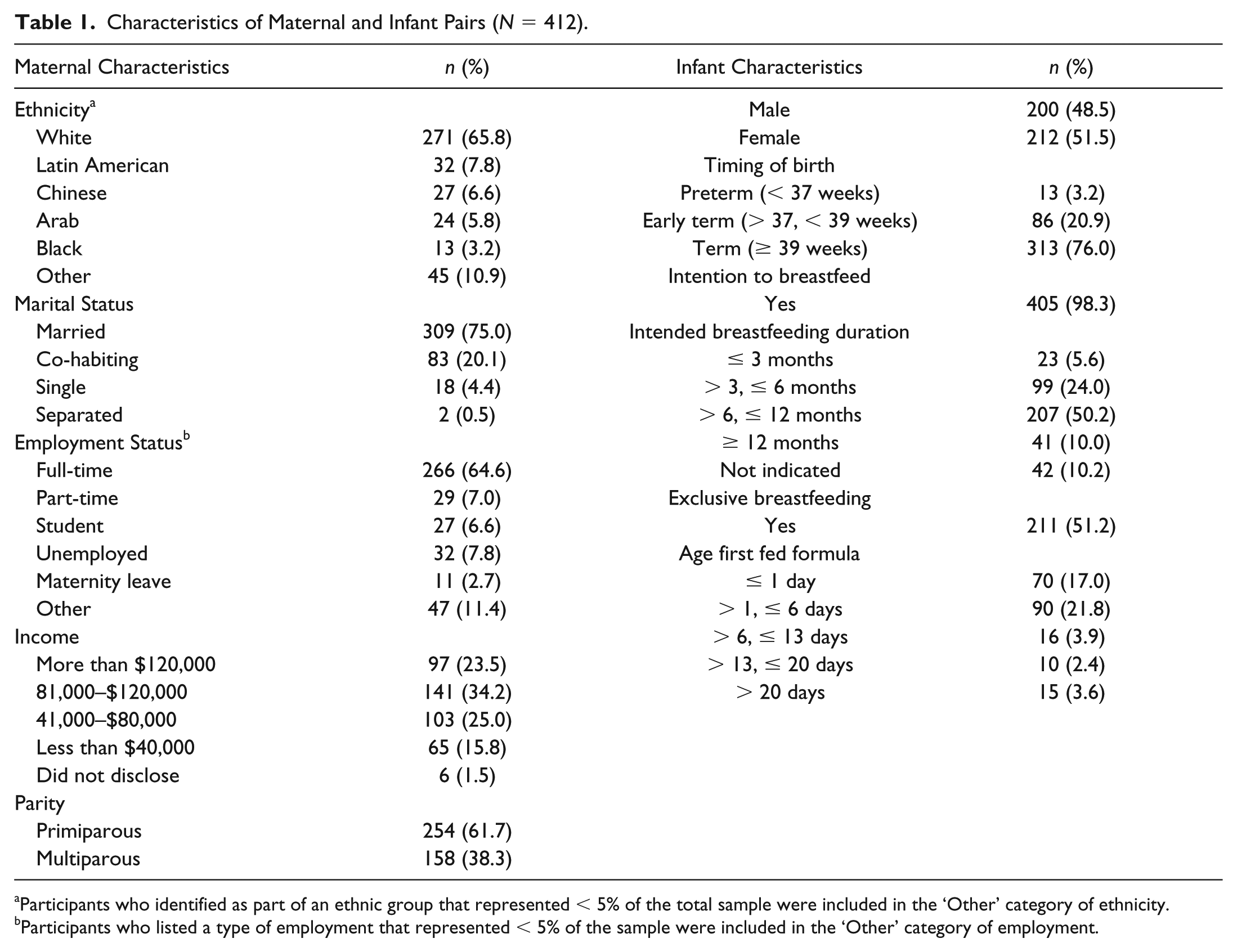
Participants who identified as part of an ethnic group that represented < 5% of the total sample were included in the ‘Other’ category of ethnicity.
Participants who listed a type of employment that represented < 5% of the sample were included in the ‘Other’ category of employment.
Participants reported experiencing some pregnancy-specific anxiety in the first (M = 10.66, SD = 5.60, Range = 0–26), second (M = 10.39, SD = 5.62, Range = 0–28), and third (M = 10.67, SD = 5.38, Range = 0–29) trimester of pregnancy. Almost all participants indicated that they planned to breastfeed their infant, and half reported that they would like to breastfeed for 6–12 months (M = 9.93, SD = 4.87, Range = 2–36). At the postpartum assessment, most participants reported that they had breastfed or pumped human milk to feed their baby even for a short period of time, and that they were still breastfeeding or pumping milk for their baby. Only half of the participants had exclusively breastfed their infant; of those who reported that their infant had been fed formula (n = 201), 80% (n = 160) were fed formula within the first 6 days after birth.
Pregnancy-Specific Anxiety and EBF Status
Three logistic regression models were conducted to test hypotheses that greater pregnancy-specific anxiety in the first, second, and third trimester of pregnancy would be associated with lower odds of EBF. Results are presented in Table 2.
Results of Logistic Regression Analyses Predicting EBF Status from Pregnancy-Specific Anxiety in Each Trimester of Pregnancy (N = 412).
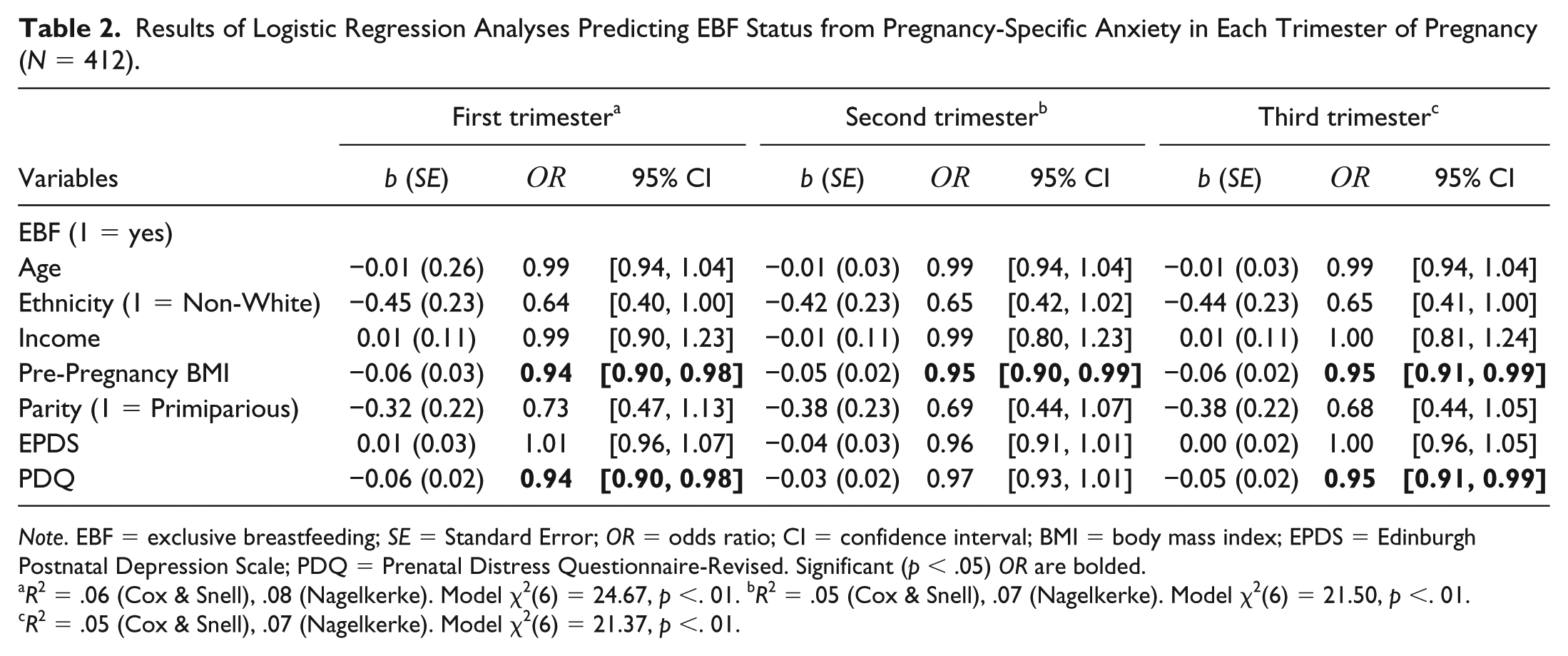
Note. EBF = exclusive breastfeeding; SE = Standard Error; OR = odds ratio; CI = confidence interval; BMI = body mass index; EPDS = Edinburgh Postnatal Depression Scale; PDQ = Prenatal Distress Questionnaire-Revised. Significant (p < .05) OR are bolded.
R2 = .06 (Cox & Snell), .08 (Nagelkerke). Model χ2(6) = 24.67, p <. 01. bR2 = .05 (Cox & Snell), .07 (Nagelkerke). Model χ2(6) = 21.50, p <. 01. cR2 = .05 (Cox & Snell), .07 (Nagelkerke). Model χ2(6) = 21.37, p <. 01.
In the first regression, the final model significantly predicted EBF status, correctly identifying 61% of cases. After statistically accounting for the influence of maternal age, ethnicity, household income, pre-pregnancy BMI, parity, and concurrent depressive symptom severity, greater pregnancy-specific anxiety was associated with a reduction in odds of EBF. Specifically, a one-unit increase in PDQ total score in the first trimester of pregnancy was associated with 6% lower odds of EBF (OR = 0.94, 95% CI [0.90, 0.98]). Of the covariates, greater pre-pregnancy BMI was associated with lower odds of EBF.
Although the second regression model also significantly predicted EBF status, correctly identifying 62% of cases, the association between pregnancy-specific anxiety in the second trimester of pregnancy and EBF status was not statistically significant.
The third regression model also significantly predicted EBF status, correctly identifying 60% of cases, and there was a significant association between pregnancy-specific anxiety and EBF status. Specifically, a one-unit increase in PDQ total score in the third trimester of pregnancy was associated with 5% lower odds of EBF (OR = 0.95, 95% CI [0.91, 0.99]). Of the covariates, only pre-pregnancy BMI remained significant and was associated with lower odds of EBF (Table 2).
Discussion
Our aim was to prospectively examine the relationship between pregnancy-specific anxiety and EBF status early in the postpartum period. Results of this study showed that a one-unit increase in pregnancy-specific anxiety in the first and third trimester of pregnancy was associated with a 5–6% decrease in odds of EBF at 6–8 weeks postpartum, even after statistically adjusting for the influence of concurrent depressive symptom severity. Based on our findings, we suggest that in addition to greater prenatal depressive symptoms (Figueiredo et al., 2014) and state/trait anxiety (Adedinsewo et al., 2014), pregnancy-specific anxiety may be an important and unique psychosocial factor that influences infant feeding practices.
Although the pathway through which pregnancy-specific anxiety influences EBF duration is unknown, previous researchers who have applied self-efficacy theory (Bandura, 1977) to understand how psychosocial factors influence breastfeeding practices provide a useful framework to understand our results (Dennis, 1999). Self-efficacy refers to one’s perceived ability to initiate, perform, and maintain a specific behavior and to cope with obstacles (Bandura, 1977). Within this framework, breastfeeding initiation and continuation represent specific health behaviors that can be affected by individual perceptions of ability, and by attitudes or emotional states (Dennis, 1999). Thus, it is plausible that pregnancy-specific anxiety affects EBF duration through its influence on a mother’s perceived ability and confidence to perform pregnancy-related behaviors including exclusively breastfeeding her child (de Jager et al., 2014). Further, women who experience greater levels of pregnancy-specific anxiety and who have low breastfeeding self-efficacy may also encounter more breastfeeding difficulties and underestimate their ability to cope with breastfeeding problems that, in turn, influence EBF duration (de Jager et al., 2013, 2014). Future research could investigate whether pregnancy-specific anxiety has a greater influence on breastfeeding self-efficacy than other forms of anxiety that extend to or occur within the perinatal period to assist with identification of women at risk for shorter EBF duration, and to guide prenatal interventions designed to promote prolonged EBF.
There are additional results outside the main study aims that are worth mentioning. First, of those participants who fed formula to their infant, most reported doing so within the first week postpartum, supporting the notion that it is important for breastfeeding interventions to occur during the prenatal period and/or shortly after birth (Schreck et al., 2017). Second, non-white ethnicity was associated with a 36% decrease in odds of EBF that, although not statistically significant, is meaningful given the large effect size and may represent an important variable that influences EBF duration. Third, pre-pregnancy BMI was also a significant predictor of EBF, and the magnitude of the effect was similar to that of pregnancy-specific anxiety, highlighting that physical and psychosocial characteristics are equally important to consider. A review of research literature on the association between pre-pregnancy BMI and reduced breastfeeding initiation and duration indicated that there is a relatively consistent effect, but the mechanism of risk remains unclear (Bever Babendure et al., 2015).
Although the relationship between pre-pregnancy BMI and EBF status is likely influenced by both physiological and behavioral factors (Bever Babendure, Reifsnider, Mendias, Moramarco, & Davila, 2015), some research has shown that overweight and obese women are also less confident in their abilities to meet breastfeeding goals and have lower recognition of EBF benefits for infant health outcomes relative to infant formula (Kirkegaard et al., 2015). Given associations between pre-pregnancy BMI and psychosocial and attitudinal aspects of breastfeeding, future research could examine whether overweight and obesity during the perinatal period are associated with specific concerns or barriers to EBF. Furthermore, whether or not psychosocial, physiological, and behavioral factors interact or influence one another in the prediction of EBF is an opportunity for further research.
The prospective study design and large sample size are significant strengths of the present study, and the online questionnaire data collection procedure reduced participant burden, an important consideration given increased demands during the pregnancy period. The assessment of pregnancy-specific anxiety and concurrent depressive symptom severity at three timepoints during pregnancy allowed the examination of temporal differences in how psychological states influence EBF status. Given that significant associations with EBF status were observed in the first and third, but not second trimester of pregnancy, trajectories of pregnancy-specific anxiety may also be important to consider. Prior reports have shown that women tend to experience higher levels of some depressive symptoms in the first and third trimesters of pregnancy (Amiel Castro et al., 2017); it is possible that pregnancy-specific anxiety follows a similar pattern. Whether changes in pregnancy-specific anxiety that occur over the course of pregnancy influence infant feeding practices or other obstetrical outcomes is a target for further study.
Limitations
Since this study was a secondary analysis of existing data and not specifically designed to examine breastfeeding outcomes, there was no assessment of EBF intention, frequency of formula feeding, or about how human milk was fed (e.g., bottle-fed or breastfed). No information was obtained about other liquids, drops, or syrups given to the infant. Thus, while EBF could be determined, we were unable to categorize the variable according to World Health Organisation recommendations for assessing infant feeding practices that include predominant breastfeeding, complementary feeding, breastfeeding, and bottle feeding (World Health Organisation, 2008). The postpartum assessment in this study was also shorter than the recommended EBF duration of at least 6 months (World Health Organisation, 2013).
The use of convenience sampling resulted in selection bias and limits the generalizability of our findings. Although the sample was ethnically diverse, participants were well educated and from higher socioeconomic status households. Further, participants with incomplete data or who withdrew from the study reported greater depressive symptom severity. Thus, whether the observed pattern of results would be similar in a more disadvantaged sample with greater depressive symptom severity is not known but is an opportunity for further study.
Finally, the relatively low effect size indicates that there may be important psychosocial and behavioral variables to consider in the prediction of EBF duration that were not included in our statistical models. Future researchers could include variables that may potentially influence, moderate, or mediate the association between pregnancy-specific anxiety and EBF duration (e.g., social support, perceptions of milk supply, breastfeeding self-efficacy) to elucidate potential mechanisms of risk and inform breastfeeding interventions.
Conclusion
In sum, pregnancy-specific anxiety had an adverse influence on EBF early in the postpartum period. Psychosocial interventions designed to improve EBF duration may benefit from the inclusion of strategies to address worries and concerns unique to the perinatal period.
Supplemental Material
Surveys – Supplemental material for The Association Between Pregnancy-Specific Anxiety and Exclusive Breastfeeding Status Early in the Postpartum Period
Supplemental material, Surveys for The Association Between Pregnancy-Specific Anxiety and Exclusive Breastfeeding Status Early in the Postpartum Period by Kristin Horsley, Tuong-Vi Nguyen, Blaine Ditto and Deborah Da Costa in Journal of Human Lactation
Footnotes
Acknowledgements
The authors are extremely grateful to all the women who took part in this study during a unique time in their lives, and to the whole study research team.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canadian Institutes of Health Research (grant #247035).
Supplemental Material
Supplementary Material may be found in the “Supplemental material” tab in the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.