
Abstract
Background:
A woman’s prior breastfeeding history may influence future decisions regarding infant feeding. Few quantitative tools utilizing this information have been demonstrated to predict breastfeeding success.
Research aim:
To evaluate the efficacy of a prenatal breastfeeding history (BAP) questionnaire administered in prenatal care to predict in-hospital formula supplementation among multiparous women.
Methods:
This is a prospective observational study of multiparous women with singleton pregnancies who presented to a Baby-Friendly urban tertiary care center for 1st prenatal visit at < 20 weeks’ gestation. The BAP tool generates a numerical score, with higher score (≥ 2) indicating prior successful breastfeeding experiences. The primary outcome was occurrence of non-medically indicated formula supplementation during the postpartum hospital stay. Student’s t test and Pearson’s chi-square test were used to compare continuous and categorical variables. A multivariable logistic regression was performed to assess the relationship of BAP score to formula supplementation. Of 587 women screened, 433 (73.8%) mother–infant dyads were analyzed.
Results:
Rates of formula supplementation in women with BAP scores ≤ 1 were 67% (156/234) compared with 37% (73/199) in women with higher scores (p < 0.0001). After controlling for race/ethnicity, insurance, and obesity, women with BAP scores of ≤ 1 were 2.6 times more likely to supplement formula than women with higher scores (aOR 2.62, 95% CI [1.70, 4.04], p < .0001).
Conclusion:
In this prospective validation study, women with negative prior breastfeeding experiences, as evidenced by a lower BAP score, were more likely to supplement formula during the postpartum hospital stay.
Background
Breastfeeding is a public health priority. The Centers for Disease Control and Prevention (CDC), World Health Organization (WHO), and multiple professional organizations recommend exclusive breastfeeding for the first 6 months of an infant’s life, followed by continued breastfeeding for at least 1–2 years or beyond, due to many well-documented maternal and child health benefits (American Academy of Pediatrics 2012; CDC, 2018) Many women, however, are not able to adhere to these guidelines despite their desire to do so (American College of Obstetricians and Gynecologists 2018; CDC, 2018). Difficulties with breastfeeding often start during the postpartum hospital stay, and ultimately result in decreased exclusivity and duration. This led to the introduction of the Baby-Friendly Hospital Initiative (BFHI), an accreditation process through which hospitals demonstrate proficiency in breastfeeding education and support through adherence to “Ten steps.” Step six of BFHI states “Do not provide breastfed newborns any food or fluids other than breast milk, unless medically indicated” (WHO, 2018, p. 15). Similarly, one Healthy People 2020 objective is a reduction in the percentage of infants receiving formula during the first two days of life from 24.2% to 14.2% (US Department of Health and Human Services, 2016). The introduction of formula is associated with shorter breastfeeding duration, and, by definition, non-exclusivity. The 2018 CDC Breastfeeding Report Card found that 17% of breastfeeding mothers in the United States used formula during the first two days after birth (CDC, 2018). In-hospital formula use has been found to increase the risk of breastfeeding cessation within 30–60 days after delivery (Chantry, Dewey, Peerson, Wagner, & Nommsen-Rivers, 2014).
Risk factors for breastfeeding problems are well known, and include young age, low socioeconomic status, maternal race/ethnicity, poor social support, and various maternal and obstetric comorbidities (Arora et al., 2017; Stough, Khalsa, Nabors, Merianos, & Peugh, 2018). There have been, however, very few tools created for the purpose of systematically identifying those women at risk of breastfeeding issues (Casal, Lei, Young, & Tuthill, 2017). Many of these tools rely on the importance of breastfeeding self-confidence, but few include the potential impact, if any, of prior breastfeeding experience on future efforts (Demirtas, 2015; Burns et al., 2018). One descriptive study of 180 multiparous women in the early postpartum period found that a history of breastfeeding problems with a prior infant was the only predictor of in-hospital formula supplementation (Demirtas, 2015).
A desire to confirm the importance of breastfeeding history for future breastfeeding success led to the development by Burns et al. (2018) of a breastfeeding history questionnaire (BAP). The BAP tool utilizes three questions regarding a woman’s breastfeeding history to create a numerical score as seen in Table 1. In Burns et al. (2018), women were asked, in the immediate postpartum period, questions regarding their prior breastfeeding experience with other children. Women with BAP scores ≤ 1 were more likely to formula supplement during their postpartum hospital stay (RR = 4.35, 95% CI [2.47, 7.65], p < .001). Both sensitivity and negative predictive value of a BAP score of ≥ 1 were over 85%, while specificity and positive predictive value were over 60% (Burns, 2018). A limitation of Burns et al. (2018) was the administration of the questionnaire after delivery of a new infant when feeding experiences with that baby may skew a mother’s perception of their breastfeeding history. Burns et al. (2018) also included both multiparous and primiparous women in their initial study. Primiparous women, by definition, would have a BAP score of 0. Therefore, a population of only multiparous women is the more appropriate population to determine the efficacy of this scoring system. Given these limitations, the aim of this study was to evaluate the efficacy of the BAP questionnaire, administered in prenatal care to predict in-hospital formula supplementation among multiparous women
Key Messages
The aim of this study was to validate a prenatal breastfeeding history questionnaire (BAP) utilizing a woman’s prior breastfeeding experience to predict in-hospital, non-medically indicated formula supplementation in a current pregnancy.
After controlling for race, insurance, and screening BMI, women with BAP scores of ≤ 1 were 2.6 times more likely to supplement formula than were women with higher scores.
In this prospective validation study, women with negative prior breastfeeding experiences, as evidenced by a lower BAP score, were more likely to supplement formula during the postpartum hospital stay.
Definition and Scoring of the BAP Questionnaire.
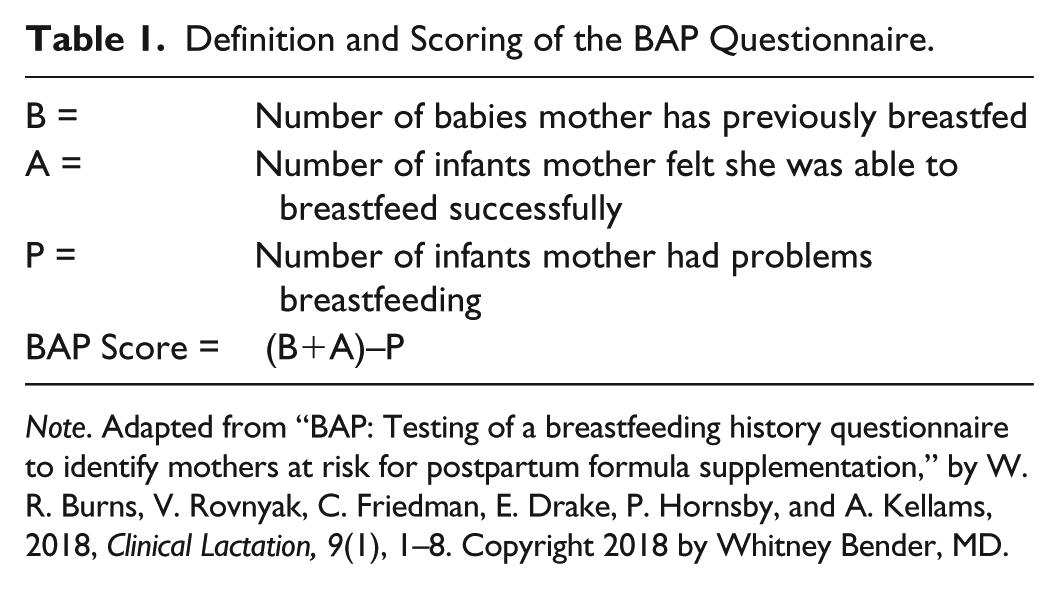
Note. Adapted from “BAP: Testing of a breastfeeding history questionnaire to identify mothers at risk for postpartum formula supplementation,” by W. R. Burns, V. Rovnyak, C. Friedman, E. Drake, P. Hornsby, and A. Kellams, 2018, Clinical Lactation, 9(1), 1–8. Copyright 2018 by Whitney Bender, MD.
Methods
Design
This study was a prospective, longitudinal, two-group survey. A prospective study was chosen given the aforementioned concerns about recall bias when administering the breastfeeding history questionnaire in the postpartum period. Institutional Review Board (IRB) approval was obtained prior to the study’s initiation.
Setting
This study was conducted at a Baby-Friendly urban tertiary care center in a metropolis in the Northeastern United States. The hospital serves a heterogeneous population with respect to race and socioeconomic status. Within this metropolis, the ever breastfeeding reported rate in 2016 was 77.9% compared with 82.5% nationwide (Murphy, Epstein, Shaw, McDaniel, & Steber, 2018). The hospital employs five International Board Certified Lactation Consultants (IBCLCs). It is standard for all women to receive a IBCLC visit in the postpartum period.
Sample
Multiparous women with singleton pregnancies who presented to a Baby-Friendly urban tertiary care center for first prenatal visit at < 20 weeks’ gestation were eligible for inclusion. Women who presented for first prenatal visit after 20 weeks’ gestation, with a medical contraindication to breastfeeding, pregnancy loss or termination, delivery < 37 weeks’ gestation, neonate admitted to the intensive care unit, or unplanned delivery at an outside hospital were excluded. In calculating our sample size, we assumed a risk of supplementation of 30–40% in the high BAP score (low risk) group versus 60% in the low BAP (high risk) group. Assuming a Type 1 error rate of 5% and equal distribution of women among both groups, we calculated that a sample size of 255 women would be required for a detectable odds ratio of 2.25 in our primary outcome, with 80% power.
Of the 937 multiparous women who presented for new obstetrics (OB) visits during the 6-month study period, 587 (62.6%) women completed BAP screening (Figure 1). Of these, 154 were excluded at the time of delivery, including 76 (12.9%) who delivered preterm neonates or neonates that required NICU admission and 78 (13.3%) who delivered at another institution. Therefore, 433 mother–infant dyads were available for analysis, giving the study adequate power to detect a difference in our primary outcome.
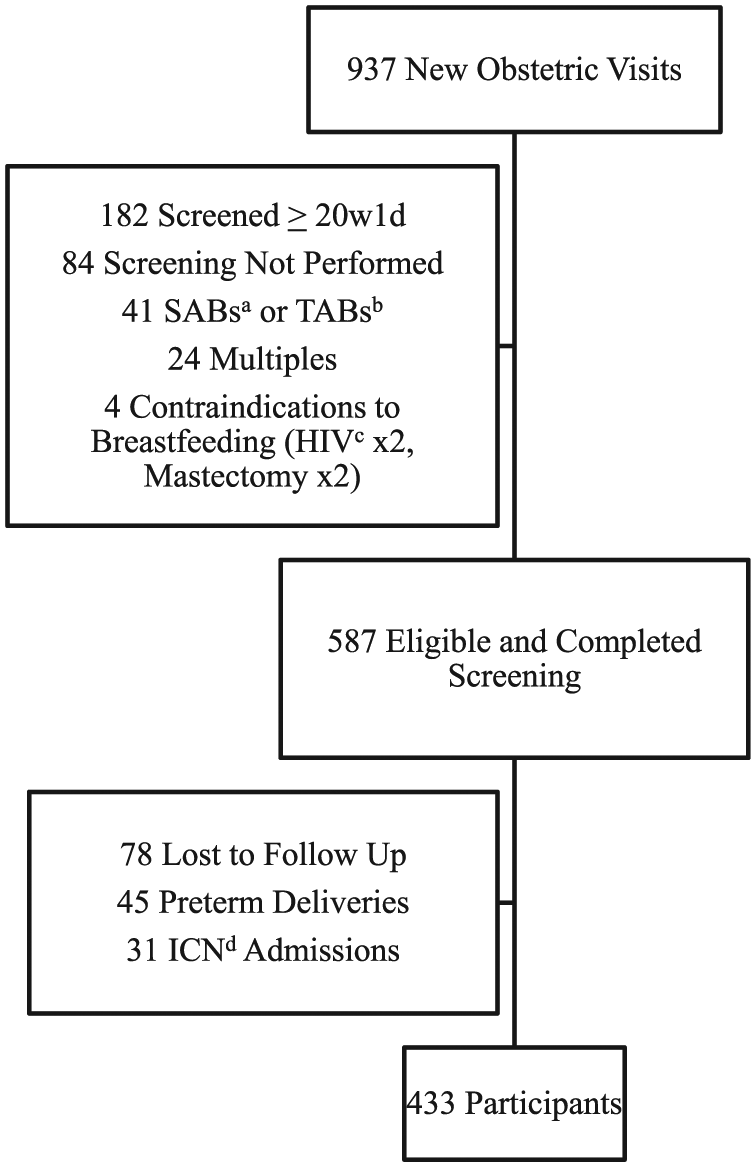
Sample Selection Process.
Measurement
Demographic, obstetric, and neonatal outcomes were abstracted from the EMR of the mother–infant dyad. Demographic information obtained included maternal age, maternal race/ethnicity, and maternal insurance status. Obstetric data abstracted included gravidity, parity, maternal comorbidities, gestational age at screening and delivery, delivery method, and delivery complications. Neonatal outcomes collected included birthweight, APGARs, and complications.
The development of the BAP tool has been described in a prior publication (Burns, 2018). In short, a panel of stakeholders refined questions that may be used to take a breastfeeding history prior to pilot testing in both the hospital and outpatient setting. Initial evaluation is described in a prior publication (Burns, 2018). A high score is indicative of prior successful breastfeeding experiences. For example, a woman who had breastfed two infants, felt successful with each of those children but had some latching problems with her first child, would have a score of 3. As another example, a woman who had breastfed one infant and felt unsuccessful secondary to supply issues would have a score of 0.
BAP screening information was recorded in and abstracted from the EMR. Breastfeeding was defined as receipt of human milk at the mother’s breast, via hand expression, or via bottle after breast pumping. Formula introduction and reason for formula use were also recorded. The primary outcome of interest was non-medically indicated formula supplementation during the postpartum hospital stay. Medically-indicated formula supplementation was documented in the medical record and was most commonly for excess weight loss or hypoglycemia. Women whose infants received medically-indicated formula supplementation only were counted as having exclusively breastfed, and women whose infants received medically-indicated formula supplementation in addition to formula per maternal request were counted amongst those women who fed formula.
Data Collection
For this study initial prenatal visits occurred between May and October 2016; deliveries occurred between September 2016 and June 2017. Data were abstracted from the EMR by a single researcher (WB). The IRB provided a waiver of informed consent for participants as utilizing the questions to obtain a breastfeeding history was made a standard of care in the health system. Questions from the BAP questionnaire were incorporated into the new obstetric note template in the electronic medical records (EMR) and asked as a part of routine clinical care. Providers received education on the use of the tool by the primary author (WB) prior to its incorporation into routine clinical care. Providers then asked the questions and recorded the answers in the history and physical note, at the time of the new obstetrical visit, as part of routine clinical care. The participating outpatient clinics included a single clinic staffed by resident physicians, nurse practitioners, and general obstetrician–gynecologist (OBGYN) attending physicians, as well as a clinic staffed by general OBGYN attending physicians and midwives. The answers were not subject to provider’s interpretation; if a mother felt she had a problem or a success, the answer was taken at her word. Patient race/ethnicity and insurance status were obtained directly from the chart as documented by patient self-report and scan of insurance cards respectively. Data were kept on an encrypted universal serial USB drive accessible only by a single researcher (WB).
Data Analysis
Student’s t test and Pearson’s chi-square test were used to compare continuous and categorical variables, respectively. Multivariable logistic regression was performed to assess the relationship of BAP score with formula supplementation after adjustment for covariates. We considered potential covariates from the literature as well as variables associated with the BAP score (p < .2). A backward selection strategy was used for multivariable models where we exclude any potential covariate that was not associated with our outcome, p > .05, unless removing this variable changed the association of interest by 10% or greater. The area under the receiver operating characteristic curve was calculated to measure discriminative capacity. Statistical analysis was performed using STATA 14.2 (Statacorp, 2015).
Results
Characteristics of the Sample
Demographic characteristics for the entire cohort are presented in Tables 2 and 3. When comparing participants based on BAP score, participants with scores ≤ 1 were more likely to be younger, publicly-insured, and obese at the time of delivery. They were also more likely to have maternal medical complications.
Characteristics of the Sample Grouped by BAP Scores (N = 433).
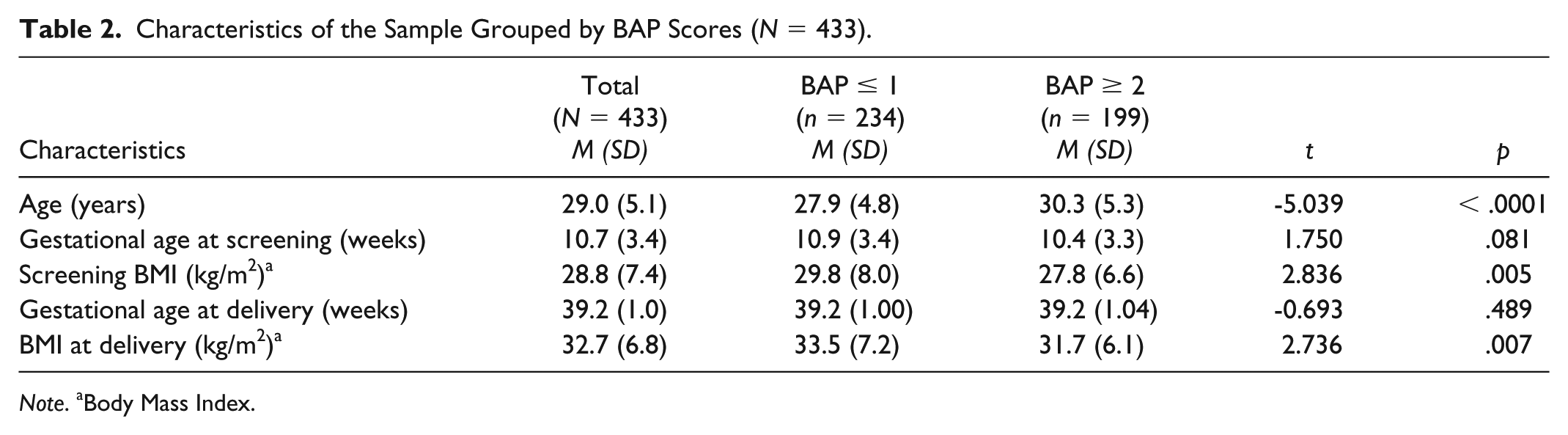
Note. aBody Mass Index.
Additional Demographics and Delivery Characteristics of the Sample Grouped by BAP Score (N = 433).
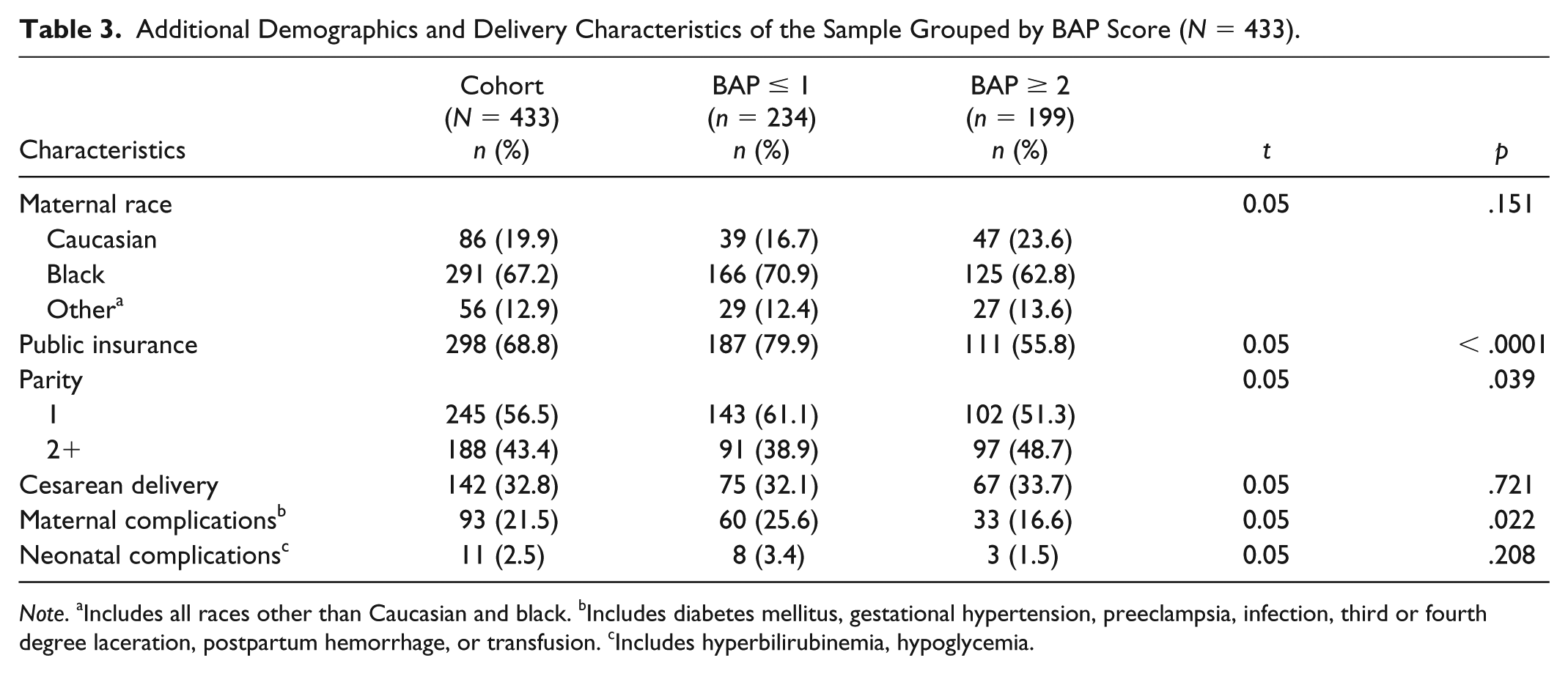
Note. aIncludes all races other than Caucasian and black. bIncludes diabetes mellitus, gestational hypertension, preeclampsia, infection, third or fourth degree laceration, postpartum hemorrhage, or transfusion. cIncludes hyperbilirubinemia, hypoglycemia.
Outcomes Based on BAP Scores
The mean BAP score was 1.4 (SD = 1.7) and the median was 1. Scores ranged from 0–12 as seen in Figure 2. Participants with BAP scores of ≤ 1 (n = 234) had a formula supplementation rate of 67% (n = 156) compared to 37% (n = 73) in participants with scores ≥ 2 (n = 199) (p < .0001). Of participants supplementing formula in the low risk group (n = 73) only 37% (n = 27) did so for more than 50% of feedings (Table 4). In contrast, of the participants with BAP score ≤ 1 who supplemented formula (n = 156), 50% (n = 78) did so for > 75% of feedings. After controlling for race/ethnicity, insurance status, and screening BMI, participants with BAP scores ≤ 1 were 2.6 times more likely to supplement formula than participants with higher scores (aOR 2.62, 95% CI [1.70, 4.04], p < .0001). BAP scores ≤ 1 remained strongly associated with formula supplementation as the analysis was restricted to formula use for > 50% and > 75% of feeds. (aOR 4.13, 95% CI [2.51, 6.80], p < .0001 and aOR 4.64, 95% CI [2.47, 8.08], p < .0001, respectively).
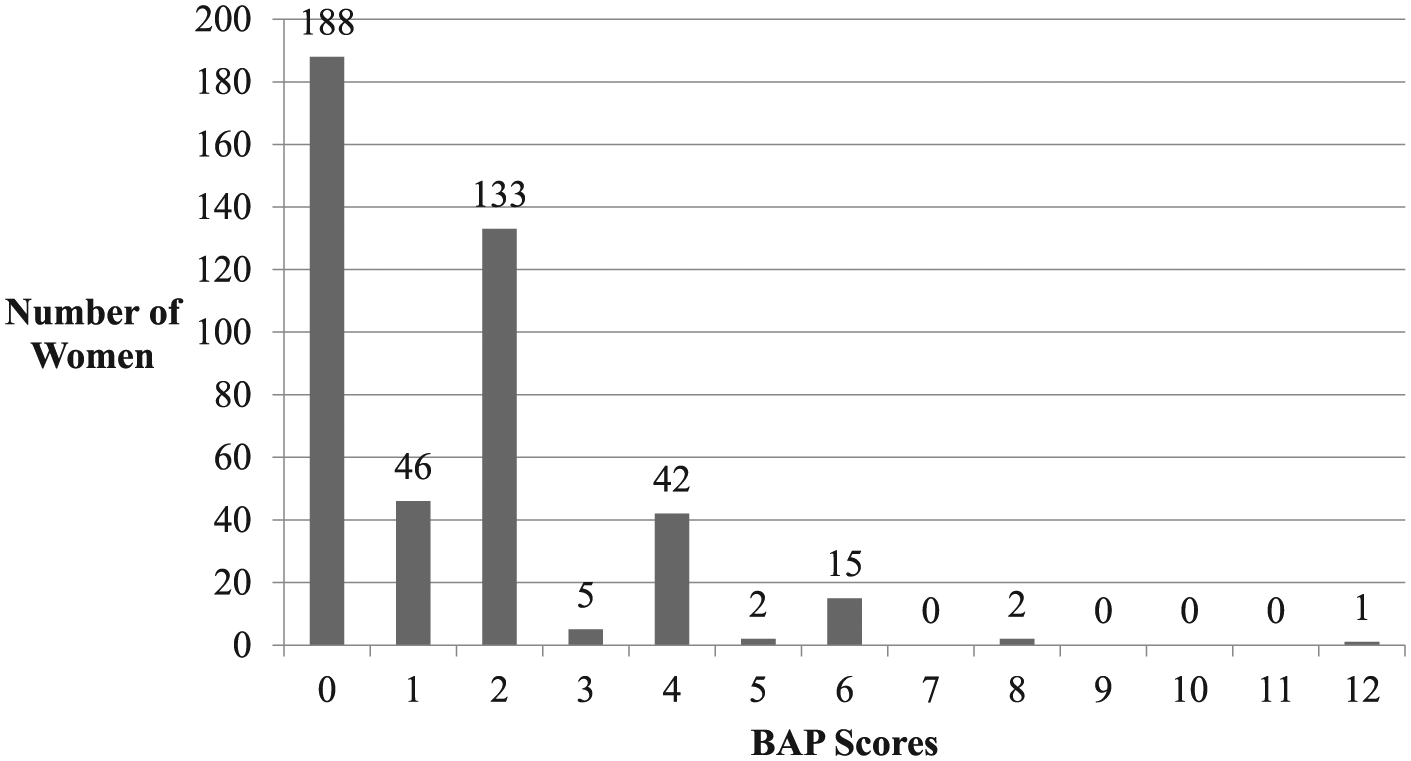
Distribution of BAP Scores (N = 433).
Formula Supplementation by BAP Score.
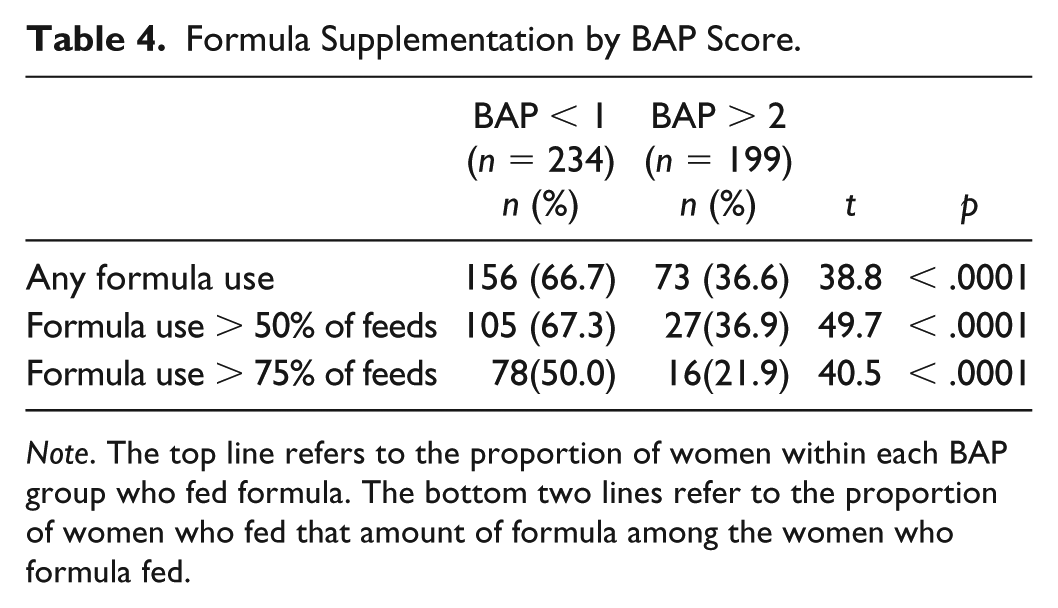
Note. The top line refers to the proportion of women within each BAP group who fed formula. The bottom two lines refer to the proportion of women who fed that amount of formula among the women who formula fed.
The sensitivity and specificity of a BAP score ≤ 1 for the prediction of any formula use in the hospital was 68.1% and 61.8%, respectively. The sensitivity of BAP score ≤ 1 increases to 79.0% and 83.0% for formula use for more than 50% of feedings and more than 75% of feedings, respectively. With regard to the discriminative capacity of the BAP tool, the area under the curve (AUC) was 0.69.
Discussion
Our results confirm that BAP scores can be used antenatally to identify multiparous women who are most likely to supplement formula during the postpartum hospital stay. Not only are women with BAP scores ≤ 1 more likely to supplement formula, but they are also more likely to utilize formula for the majority of infant feeds in the postpartum hospital stay. Our findings are consistent with the prior study that evaluated women in the immediate postpartum period, and strengthens the clinical applicability of the tool in identifying women at risk of breastfeeding difficulty. We have consistently found that scores ≤ 1 are associated with higher formula supplementation rates in the immediate postpartum periods, even after controlling for age, race/ethnicity, insurance status, screening BMI, and presence of maternal complications.
Importantly, the specificity of the BAP questionnaire increases as you restrict the outcome to increased use of formula as a proportion of total feeds in the hospital. This suggests that the tool is particularly useful for identifying women who are most likely to utilize formula for the majority of their infant feeds in the hospital. In comparison to other instruments previously developed to predict breastfeeding success including Breastfeeding Assessment Score (BAS) and Breastfeeding Attrition Prediction Tool (BAPT), our tool is significantly shorter and, as a result of its brevity, can encourage the provider and mother to engage in a discussion regarding infant feeding (Raskovalova et al., 2015; Casal, Lei, Young, & Tuthill, 2017).
Past studies have suggested focusing breastfeeding support efforts on women with diverse risk factors as well as primiparous mothers. However, the previous study by Burns et al. (2018) found multiparous mothers with scores of ≤ 1 to be more at risk of formula supplementation than primiparous women (Burns, 2018). Our findings confirm that poor past breastfeeding experiences can significantly influence breastfeeding success in future pregnancies. Identification of these women during prenatal care gives the obstetrical provider and mother ample time to discuss the experiences that caused a low score and, perhaps, formulate a plan to address these issues. Additional research will also focus on an appropriate antepartum or immediate postpartum intervention for multiparous women with BAP scores < 1 to help these women develop and reach breastfeeding goals.
Limitations
In our study, the questionnaire was administered by a variety of providers, including nurse practitioners, nurse midwives, residents, and attending physicians, during prenatal care. Consequently, the answers to questions may have been subject to differences in interpretations resulting in possible differences in scores. We suspect this impact to be minimal as all providers were instructed to record problems and successes as directly reported by the participant. More importantly, this study is unable to account for breastfeeding counseling or education received by these women in their routine prenatal care. The tool is merely a scoring system, and we were unable to track any additional meaningful counseling that occurred as a result of the integration of the BAP questionnaire into clinical practice. Secondly, the BAP questionnaire was not administered or recorded in approximately 10% of cases. It is unclear what impact, if any, the inclusion of this population would have on our results. Additionally, our cohort has an overall formula supplementation rate that is significantly higher than that reported in the literature for Baby-Friendly Hospitals. The reasons for this are unclear, although the exclusion of primiparous women may have falsely inflated the overall formula supplementation rate. Lastly, participants in this study were considered to have exclusively breastfed when their infants did not receive non-medically indicated formula supplementation. This outcome was chosen to be consistent with the definition of exclusive breastfeeding utilized in the original publication by Burns et al. (2018). The instances of medically-indicated formula supplementation were not recorded, and, as such, are unable to be further commented upon.
Conclusion
This study confirms prior retrospective literature on the use of a women’s breastfeeding history to predict future breastfeeding success. Future studies are warranted to determine the applicability of this tool in widespread clinical practice as a means of increasing breastfeeding initiation, exclusivity, and duration.
Footnotes
Authors’ Note
Findings of this paper were presented as a poster at SMFM’s 38th Annual Pregnancy Meeting in Dallas, TX on February 1, 2018.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.