
Abstract
Background:
Human milk is the optimal food for newborns. Choices to feed preterm infants in neonatal intensive care units are mother’s milk, donor milk, or formula. Preterm infants have better tolerance for human milk, but the lower caloric density of donor milk might not meet preterm infant growth needs. Preterm infants have higher protein and energy requirements with a limited stomach capacity. Therefore, there is a need for human milk with increased nutrient density.
Research Aim:
To concentrate donor milk to have a higher caloric and protein density while avoiding side effects of high osmolality by precipitating lactose at low temperatures.
Methods:
We investigated the results of volume reduction and lactose removal processes on the lactose, protein, osmolality, and viscosity of human milk. Donor milk was obtained from WakeMed Mothers’ Milk Bank. Homogenization and evaporative condensation were applied to samples (N = 36) before they were stored frozen overnight, followed by refrigerated centrifugation for lactose removal at 0 °C. Supernatants were separated and compared to the composition of controls.
Results:
A significant reduction of lactose (SW = -262, p < .0001) and osmolality (SW = -211.5 p < .01) was achieved in the concentrated milk without a significant protein loss from centrifugation (SW = -44.5, p = .49). A 30%–40% volume reduction is within the American Academy of Pediatrics recommended osmolality for infant feeding.
Conclusion:
Concentrating human milk in a milk bank setting for feeding preterm infants might be a simple and low-cost process to achieve a product with higher nutrient density and no non-human components.
Key Messages
To meet the high nutrient requirements of preterm infants’ donor milk, it is often fortified with bovine milk-based formulas.
To increase exclusive human milk feedings and decrease the use of formula and fortifiers, we investigated a method to increase the protein and nutrient content of human milk, while preventing lactose content and osmolality increase at the same rate.
We showed that by chilled centrifugation we can crystallize lactose significantly and reduce osmolality while maintaining protein content.
Evaporation and chilled centrifugation are methods that can be used in donor milk banks.
Background
Human milk is the optimal nutrition and the recommended way to feed every newborn exclusively for 6 months, with the continuation of breastfeeding for 2 years and beyond (Agostoni et al., 2009; American Academy of Pediatrics [AAP], 2012; World Health Organization [WHO] & United Nations Children’s Fund [UNICEF], 2003). AAP, The European Society for Paediatric Gastroenterology Hepatology and Nutrition (ESPGHAN), and The WHO recommend that preterm infants receive human milk, and that it should be the mother’s own milk when possible (AAP, 2012; Lapillonne et al., 2019; WHO, 2011). Human milk banks aim to provide milk to preterm and sick infants when the mother’s own milk is not available. Human milk often needs to be fortified to meet the high nutritional demand of a preterm infant (AAP, 2012). An exclusive human milk diet decreases the risk for necrotizing enterocolitis ([NEC]; Delaney Manthe et al., 2019; Miller et al., 2018), which is one of the most common causes of preterm infant death (Schindler et al., 2017). However, commercial human milk-based fortifiers are very costly. The cost might be reduced if non-profit human milk banks could increase the nutrient density of human milk in their settings.
Globally, 14.84 million babies are estimated to be born prematurely every year and complications due to prematurity are the leading cause of death in children younger than 5 years of age (Chawanpaiboon et al., 2019). Compared to full-term infants, preterm infants are born with low nutrient storage (Justyna, 2020). Improved feeding practices have been decreasing the rates of growth failure; however, the risk is still high. Postnatal growth failure affected half of the very low birth weight infants due to insufficient nutrient supply at North American hospitals in the Vermont Oxford Network (Horbar et al., 2015). The focus on preterm infant nutrition has been shifting from energy alone to the protein-to-energy ratio (Agostoni et al., 2010). Weight gain of premature infants was positively correlated with both high daily total protein intake and protein concentration in human milk (Lin et al., 2020). Furthermore, increasing protein intake promotes growth, lean body mass, and long-term developmental outcomes (Hay, 2018).
Lactose is an osmotically active disaccharide. It can crystallize when lactose concentration exceeds the solubility constant for a given temperature (Jenness & Walstra, 1984). The concentration of lactose in human milk is a major contributor to osmolality (Choi et al., 2016). Hyperosmolar feeding is one of the proposed risk factors for necrotizing enterocolitis which is an inflammatory gastrointestinal tract disease that increases the mortality of preterm infants (Chandran et al., 2020; Siripattanapipong et al., 2019). Therefore, lactose removal from milk by crystallizing and precipitating would also result in osmolality reduction. Increasing the energy and protein content of the milk can be achieved by concentrating the milk by removing the water from it. Evaporation, freeze-drying, reverse osmosis, and nanofiltration are possible methods to concentrate the milk. The evaporation method is the least costly and retains non-volatile small molecules that may have functional importance so could be used in a milk bank with a smaller budget.
Mothers who donate their milk to the milk bank are often mothers of infants with a surplus milk supply. The composition of the term mother’s milk is different than preterm mother’s milk (Lawrence & Lawrence, 2016). Preterm mother’s milk is higher in protein and lower or similar in lactose compared to term mother’s milk, hence preterm mother’s milk is closer to the preterm infant nutritional requirement (Lawrence & Lawrence, 2016; Underwood, 2013). Therefore, human milk that is processed to have increased energy and protein density would be a preferable product for human milk banks to supply to hospital neonatal intensive care units (NICU) for preterm infants. The aim of this study was to concentrate donor milk to have a higher caloric and protein density while avoiding the side effects of high osmolality due to the high lactose concentration by precipitating lactose at low temperatures.
Methods
Research Design
In this true experimental research study with posttest-only control group design, we investigated the results of volume reduction and lactose removal processes on the lactose, protein, osmolality, and viscosity of human milk (Frey, 2018). The University Institutional Review Board reviewed the study (IRB protocol #23719) and determined that it did not meet the definition of human subjects’ research.
Setting and Relevant Context
Our research was completed at North Carolina State University. Donated human milk was obtained from the WakeMed Mother’s Milk Bank, Cary, NC. WakeMed Mother’s Milk Bank is a Human Milk Banking Association of North America (HMBANA) member milk bank and it dispenses approximately 17,000 oz of donor milk every month to the NICUs in North Carolina and the east coast of the United States (WakeMed Mother’s Milk Bank, n.d.).
Sample
Donor milk is provided to preterm infants in NICUs. Donor milk did not include data about mother’s identity, whether it was expressed at the beginning or end of the feeding, time of the day collected, infant’s age, maternal diet, or gestational age at birth (Allen et al., 1991; Hibberd et al., 1982; Lonnerdale, 1986) all of which can affect milk composition. Donated milk that was not suitable for infant feeding was accepted. Samples were pooled to achieve the required 200 ml volume. Thirty-six samples underwent different levels of homogenization, evaporation, and centrifugation to achieve a lactose-reduced human milk concentrate. Eighteen of these samples were homogenized, while the remaining 18 were not.
Measurement
We represented the volume reduction as condensation, which is a fixed treatment factor and has six categories (80%, 60%, 50%, 40%, 30%, and 0%). These reduction levels were selected based on the results of preliminary experiments, suggesting that an increase in lactose concentration might be necessary to initiate crystallization. Furthermore, the samples that were over-condensed might be too saturated to create lactose crystals. Thus, we decided to observe a variety of condensation levels.
Lactose, nitrogen, viscosity, and osmolality were measured. Three replicates were completed for each measurement. Lactose measurement was performed with a Lactose/D-galactose enzymatic kit (R-biopharma, Darmstadt, Germany; Kleyn, 1985). Measurements were taken at 340 nm wavelength with a spectrophotometer (Thermo Multiskan MCC Fisher Sci USA) in a 96-well plate with blanks and a standard curve. Total nitrogen analysis was performed to measure protein (Vario Macro cube CHN and Rapid N Exceed, Elementar Analysensysteme Germany). Osmolality (mOsm/kg) was measured with a freezing point depression osmometer (Advanced Micro Osmometer Model 3300, Advanced Instrument Inc., Norwood, MA, USA). The instrument was calibrated with standard solutions of 50 mOsm and 850 mOsm. Viscosity measurement was performed with an Anton Paar modular compact rheometer at 25 °C (MCR 302, Anton Paar GmbH, Austria). Parallel plate and double-gap concentric cylinder geometry were used. Most of our samples were non-Newtonian fluids, so we reported flow curves instead of a single value.
Data Collection
The study was conducted from 2017–2019. Donors provided consent that the milk not suitable for infant feeding could be used for research purposes. Milk and donors’ personal information were collected by HMBANA but not shared with investigators. The milk was frozen at -20 °C when received, and kept frozen until use. It was thawed in a shallow shaking water bath (Precision Model 2875, Thermo Scientific) at 27 °C for 30 min. A benchtop homogenization machine (Niro Soavi, Panda2K, Italy) was used for two-stage homogenization. Samples were condensed with a rotary evaporator (Buchi R-300 RotavaporTM). The water bath of the rotavapor was set to 40 °C to avoid protein denaturation. The rotation rate of the rotavapor was set to 30 rpm, and inner pressure was set to 33 mbar, which efficiently removed water from the milk. Six different levels of volume reductions were applied to the samples. There were three replicates for each combination of condensation and homogenization levels (N = 36). Volume reductions were specified as 80%, 60%, 50%, 40%, 30%, and 0%. The condensation levels were decided based on preliminary data and donated milk batches were randomized into treatment groups.
Samples from each level of condensation were aliquoted into two 50-ml conical centrifuge tubes: One tube was frozen at -20 °C overnight and centrifuged at 0 ± 2°C, 3500 rpm for 60 min for lactose removal, and the other tube was kept refrigerated as a control. During the centrifugation process, the samples thawed slowly, and lactose crystals precipitated at the bottom and formed a lactose pellet. The part that did not include the lactose pellet is called “supernatant.” Approximately 5 ml of fluid was left at the bottom in order not to disturb the lactose pellet and to prevent lactose from dissolving back into the supernatant fraction while removing the supernatant. The lactose pellet was discarded. All samples were aliquoted and stored at -20 °C until further analysis. The measurements of supernatants were compared to the controls.
Data Analysis
In our study, the datasets included 72 observations each for the lactose content, protein content, and osmolality levels. Thirty-six respondents’ milk donations were randomly assigned to six categories of condensation. Then, the lactose, protein, and osmolality measurements were taken from each sample before and after applying lactose removal. There are two repeated measurements on each sample. We used the GLM procedure in JMP Pro 14 (SAS Inc. Cary, USA) to perform the Mann-Whitney U test to evaluate the effects of homogenization, Wilcoxon signed-rank tests to evaluate the effects of the lactose removal process, and two-way mixed ANOVA to evaluate the interaction effect between condensation and lactose removal for lactose, protein, and osmolality measurements. Statistical significance was considered when p values were below .05.
Results
Lactose
In Figure 1, we show the variability in the lactose content of the milk samples before and after the lactose removal process, homogenization, and condensation were applied. Based on the comparison of the average lactose amount for each combination of homogenization and condensation, the results indicate that the supernatant group is lower than those for the control group. Moreover, the lactose amounts for the control and supernatant groups appear to vary between homogenized and non-homogenized milk, within each category of condensation.
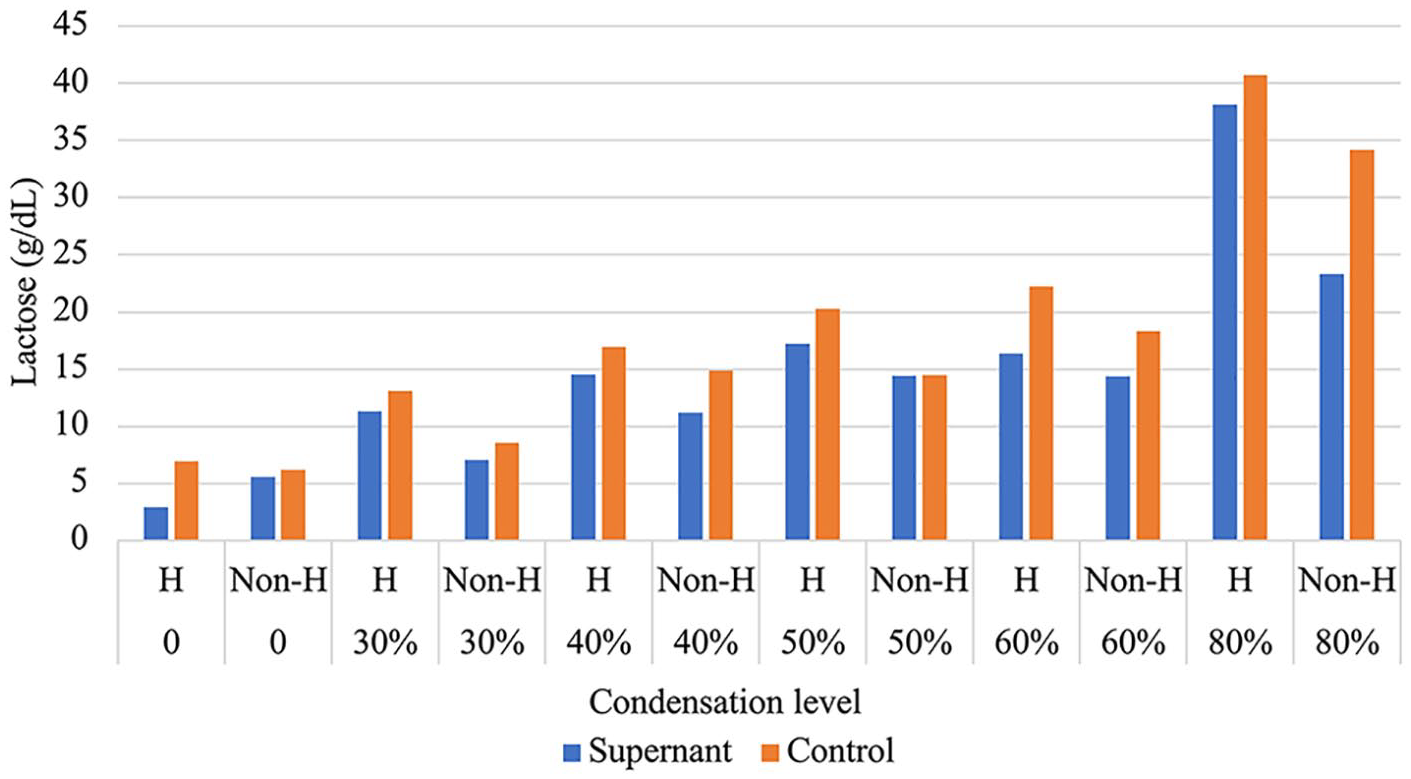
Comparison of Average Lactose Levels for Homogenized, Condensed, and Lactose-Removed Milk Compared to Control (N = 36).
In order to determine whether the differences are significant and if the homogenization has an effect on lactose precipitation, we compared the lactose content between the control-H and control-Non-H groups as well as the supernatant-H and supernatant-Non-H groups by applying the nonparametric Mann-Whitney U test. These test results were not significantly different in lactose amounts between homogenized and non-homogenized milk for the control group (SU = 370, p = .248) and supernatant group (SU = 360, p = .402). Hence, we can conclude that homogenization does not have a significant effect on the lactose removal process. In accord with these results, we pooled the data from these samples.
We investigated whether there was a difference in the lactose content before and after applying the lactose removal process. We used a related samples Wilcoxon signed-rank test to conclude that chilled centrifugation had a significant effect on lactose (SW = -262, p < .0001). The supernatant group had relatively lower lactose amounts (Mdn = 14.05) than those for the control group (Mdn = 16.31).
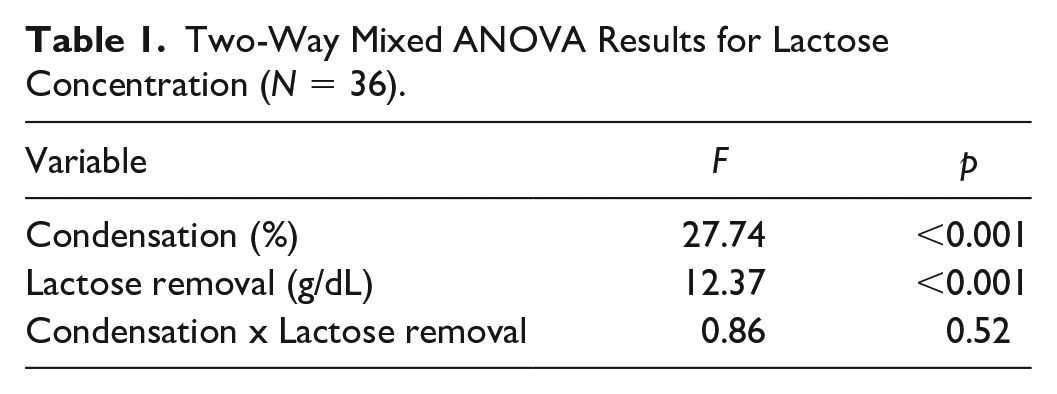
Two-Way Mixed ANOVA Results for Lactose
The correlation coefficient r for repeated measurements between control and supernatant is 0.85 with a p-value less than .001. This implies that the two-way mixed ANOVA is an appropriate analysis method for the lactose data set. According to the two-way mixed ANOVA results shown in Table 1, the condensation had a significant effect on lactose content. The result of the lactose removal process was also significant, suggesting that there was a significant decrease in lactose concentration when centrifugation was applied since the mean lactose contents for control and supernatant samples were 17.96 g/dl and 14.78 g/dl, respectively. The interaction effect between centrifugation and condensation was not significant, meaning that the effect of the chilled centrifugation procedure on the lactose content was consistent across different levels of condensation.
Two-Way Mixed ANOVA Results for Lactose Concentration (N = 36).
Protein
In Figure 2, we show the variability in the protein content of the milk samples before and after the lactose removal process, homogenization, and condensation were applied. The protein amounts for the supernatant and control groups were very similar to each other for almost all combinations of homogeneity and condensation. We also observed that the average protein content for samples increased as the condensation level increased.
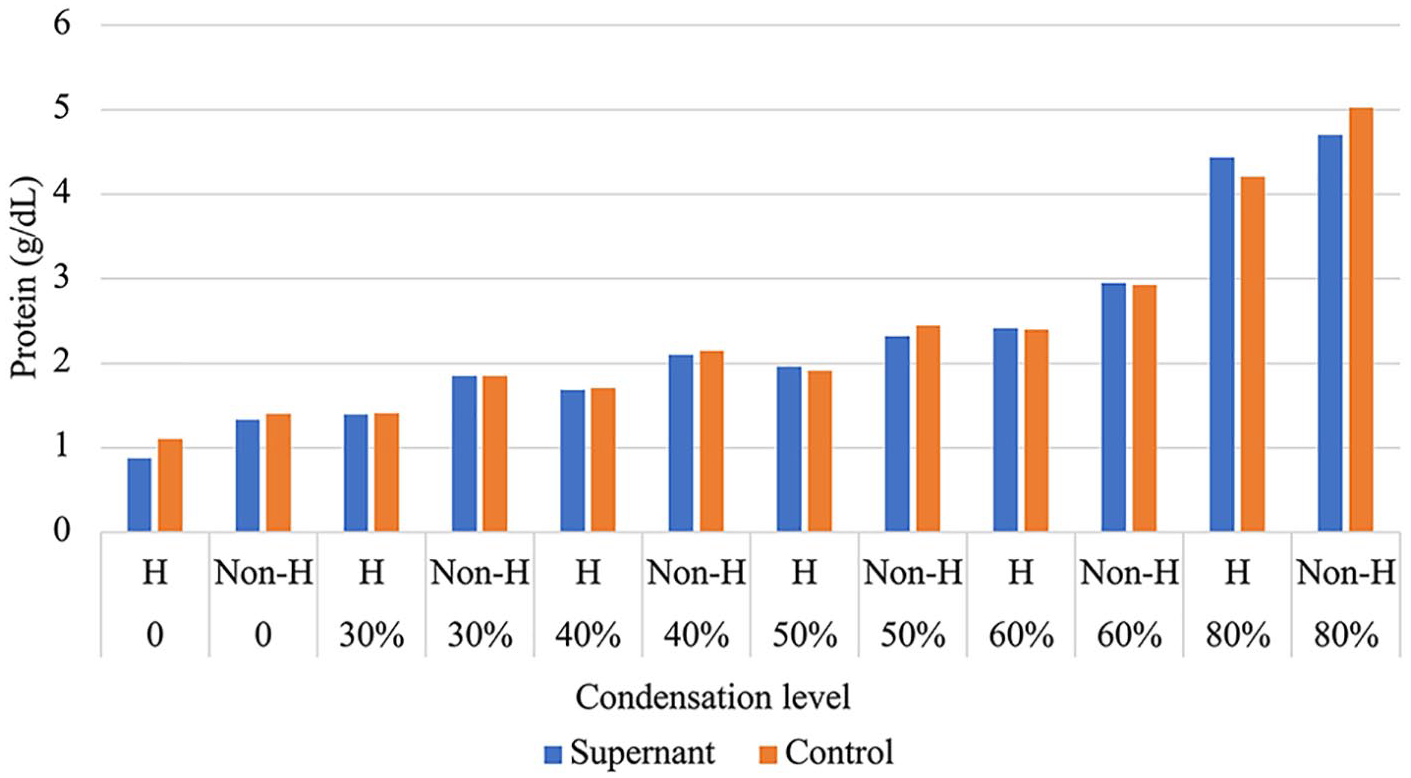
Comparison of Average Protein Levels for Homogeneity, Condensation, and Lactose Removal (N = 36).
We applied the Mann-Whitney U test to the control and supernatant groups to see whether the protein content differed between the Non-H and H categories. As expected, homogenization did not cause a noticeable change in the protein amount either in the control groups (SU = 281.5, p = .11) or the supernatant groups (SU = 285, p = .13). As in the lactose analysis, we used a related samples Wilcoxon Signed-Rank Test to determine whether there was a difference in the protein content before and after applying the lactose removal process. The protein contents for the control group were (Mdn = 2.03 g/dl) and the supernatant group (Mdn = 2.02). Hence, we conclude that lactose removal did not have a significant effect on the protein content of the milk samples (SW = -44.5, p = .49), which implies that lactose removal did not cause a significant protein loss between controls and supernatants. Therefore, we observed that the protein amount increased proportionally as the volume reduction increased.
Osmolality
In Figure 3, we show the variability in the osmolality of the milk samples before and after the lactose removal process, homogenization, and condensation were applied. We observed similar osmolality levels for the homogenized and non-homogenized milk. We investigated whether homogenization influences osmolality for the control and supernatant groups by applying the Mann-Whitney U test. This suggested that the homogenization process did not have a significant effect on osmolality either in the control group (SU = 346.5, p = .68) or the supernatant group (SU = 340.5 and p = .83). Osmolality increased gradually as the volume reduction increased. According to the Wilcoxon signed-rank test result, lactose removal had a significant effect on osmolality (SW = -211.5 and the p < .01), and the supernatant group (Mdn = 615.75) had lower osmolality than the control group (Mdn = 685).
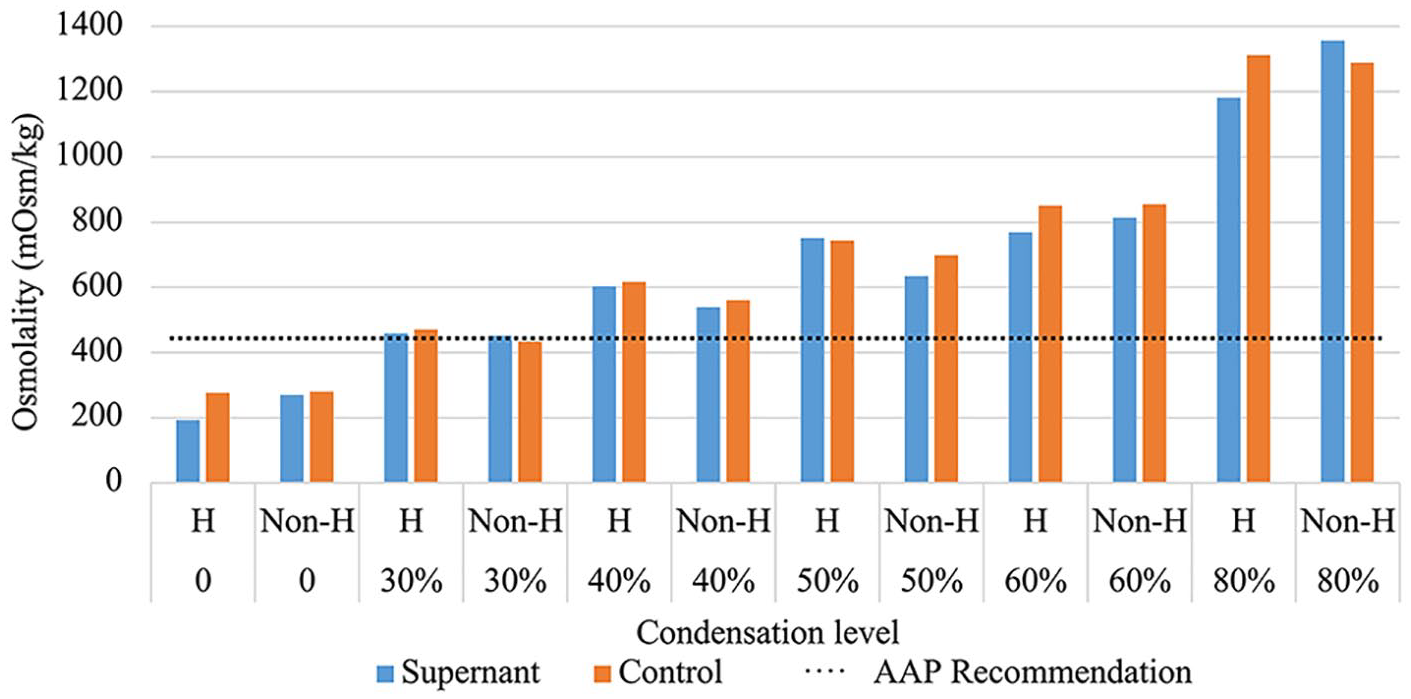
Comparison of Average Osmolality Levels for Homogeneity, Condensation and Lactose Removed Milk Compared to Control (N = 36).
The dotted line on the osmolality graph (Figure 3) indicates the AAP recommendation for the upper level of osmolality in feed for newborns (Barness et al., 1976). However, fortification applications that add powdered nutrients to human milk to meet the higher nutrient requirements of preterm infants often result in much higher osmolality in feed than this recommendation (Kreissl et al., 2013). The 30% volume reduction in our study had osmolality less than the AAP recommendation for maximum osmolality.
Two-Way Mixed ANOVA Results for Osmolality
The correlation coefficient between control and supernatant, r = 0.88 (p < .01), means that correlation between repeated measurements was significant. As shown in Table 2, the main result of condensation suggested a significant difference in mean osmolality between the condensation categories. We can see from Figure 3 that the mean osmolality levels were increasing as the condensation level of milk samples was increased.
Two-Way Mixed ANOVA Results for Osmolality (N= 36).
There is also a significant overall difference in osmolality at the control and supernatant groups, showing that the average osmolality changed after lactose removal was applied. The mean osmolality for control and supernatant was 709.58 (315.8) mOsm/kg and 638.26 (314.2) mOsm/kg, respectively, so a significant decrease in osmolality occurred when centrifugation was applied. There was no significant interaction effect between centrifugation and condensation. That is, mean osmolality contents do not change differently over centrifugation levels depending on different levels of condensation.
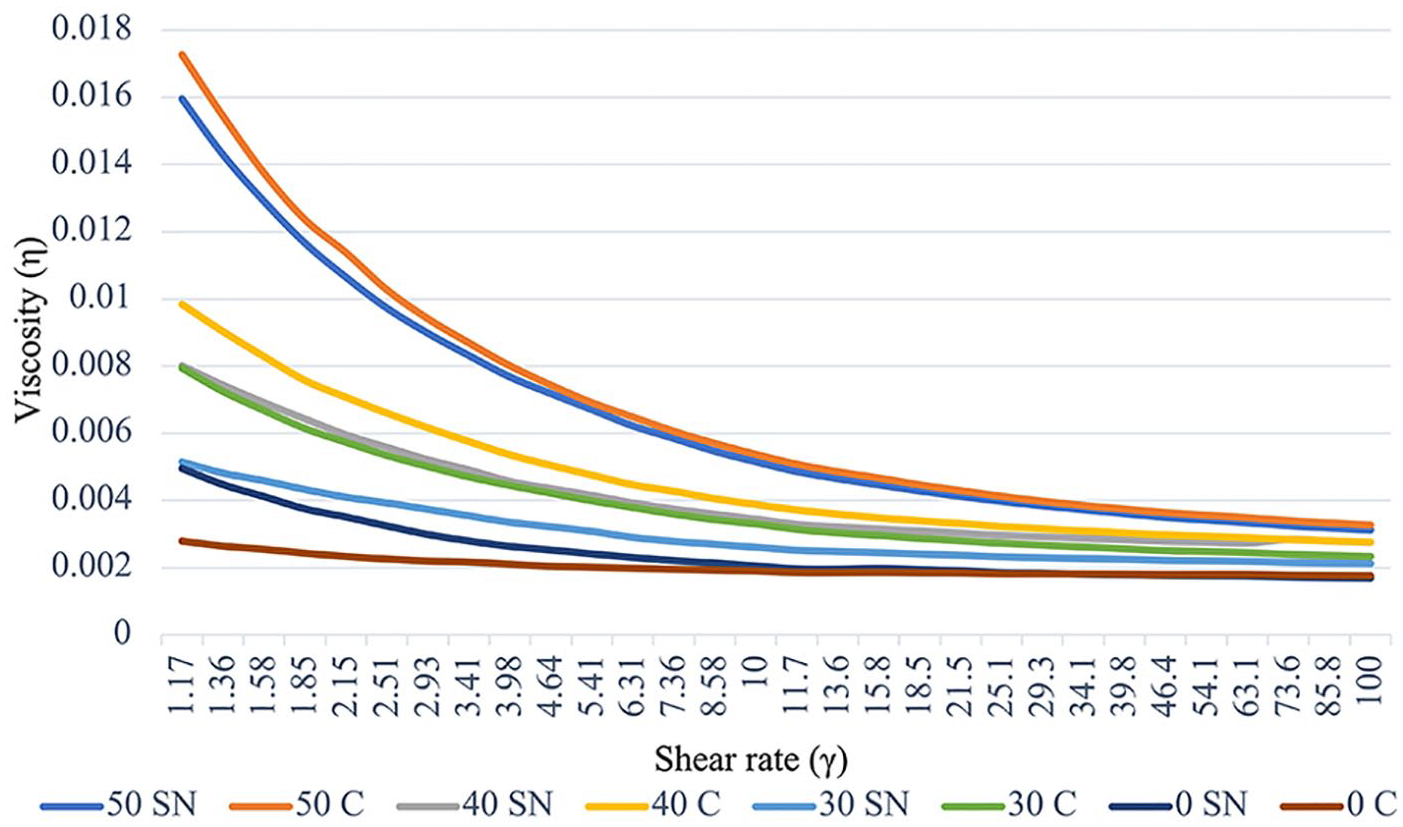
Viscosity
Figures 4–7 show the viscosity measurements. Flat flow curves represent Newtonian fluid, whereas a curve with a slope represents non-Newtonian behavior (Pollen et al., 2004). Concave curves that we observed for the homogenized and 80% condensed samples indicated a shear-thinning character. As shown in Figure 4 the flow curve for the 80% condensation level was dramatically higher than the rest of the condensation levels. Figure 5 represents 50%, 40%, 30%, and 0% flow curves separately to be able to observe flow curves of less condensed homogenized samples.
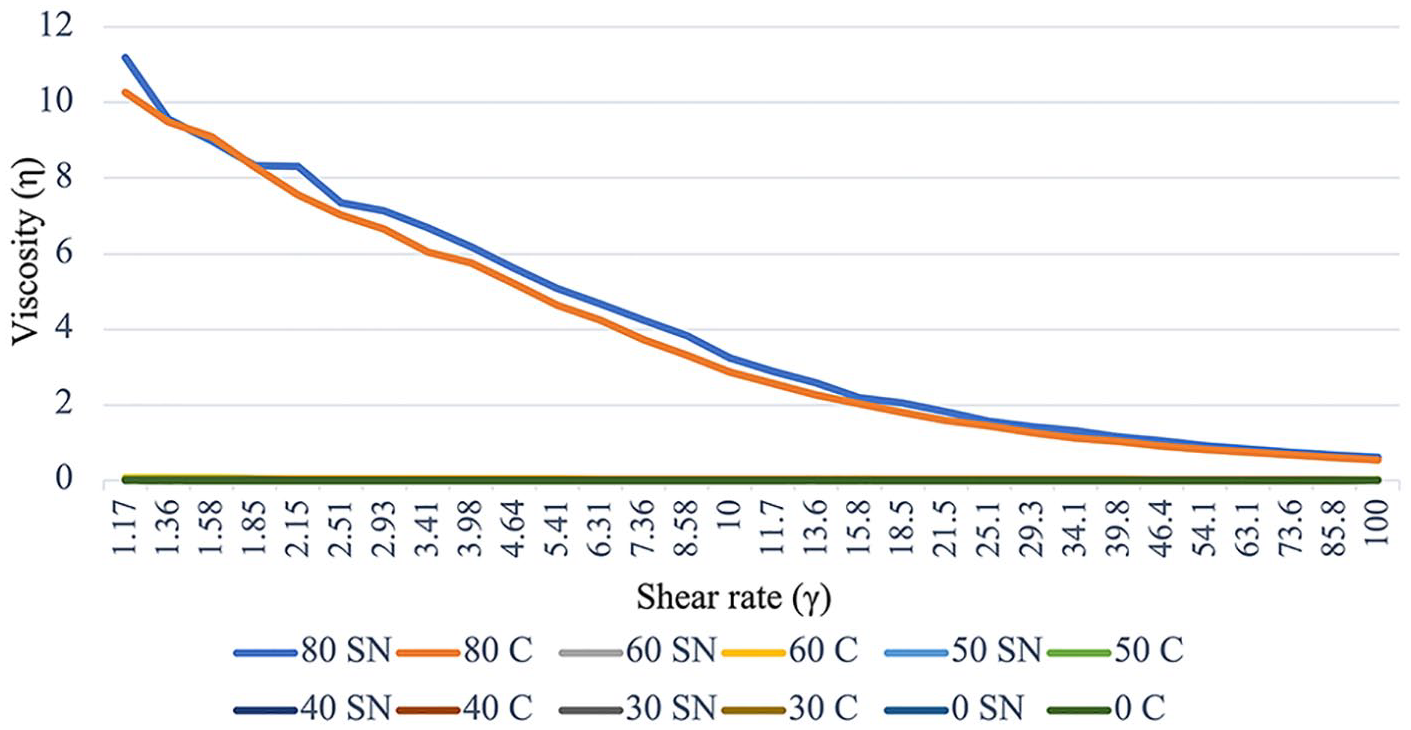
Flow Curves for Homogenized Samples (N = 36).
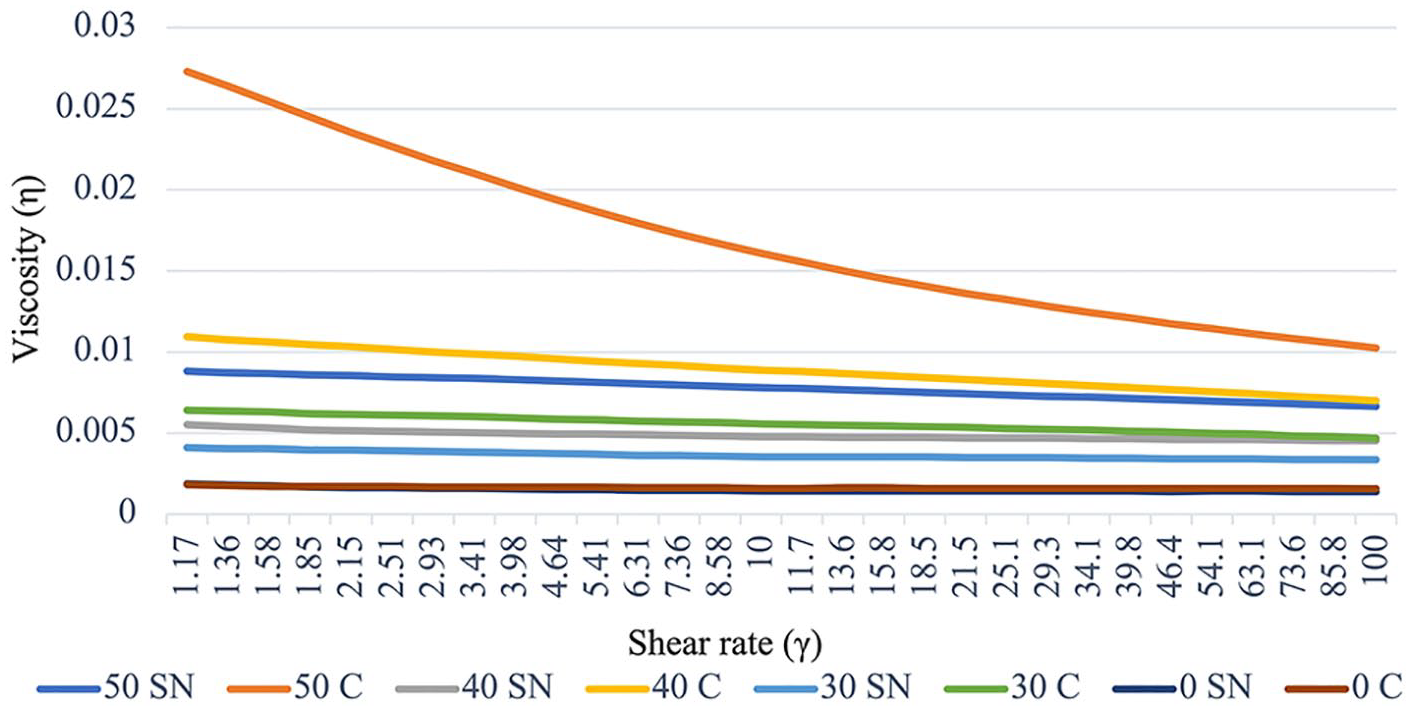
Flow Curves for Less Condensed Homogenized Samples (N = 36).
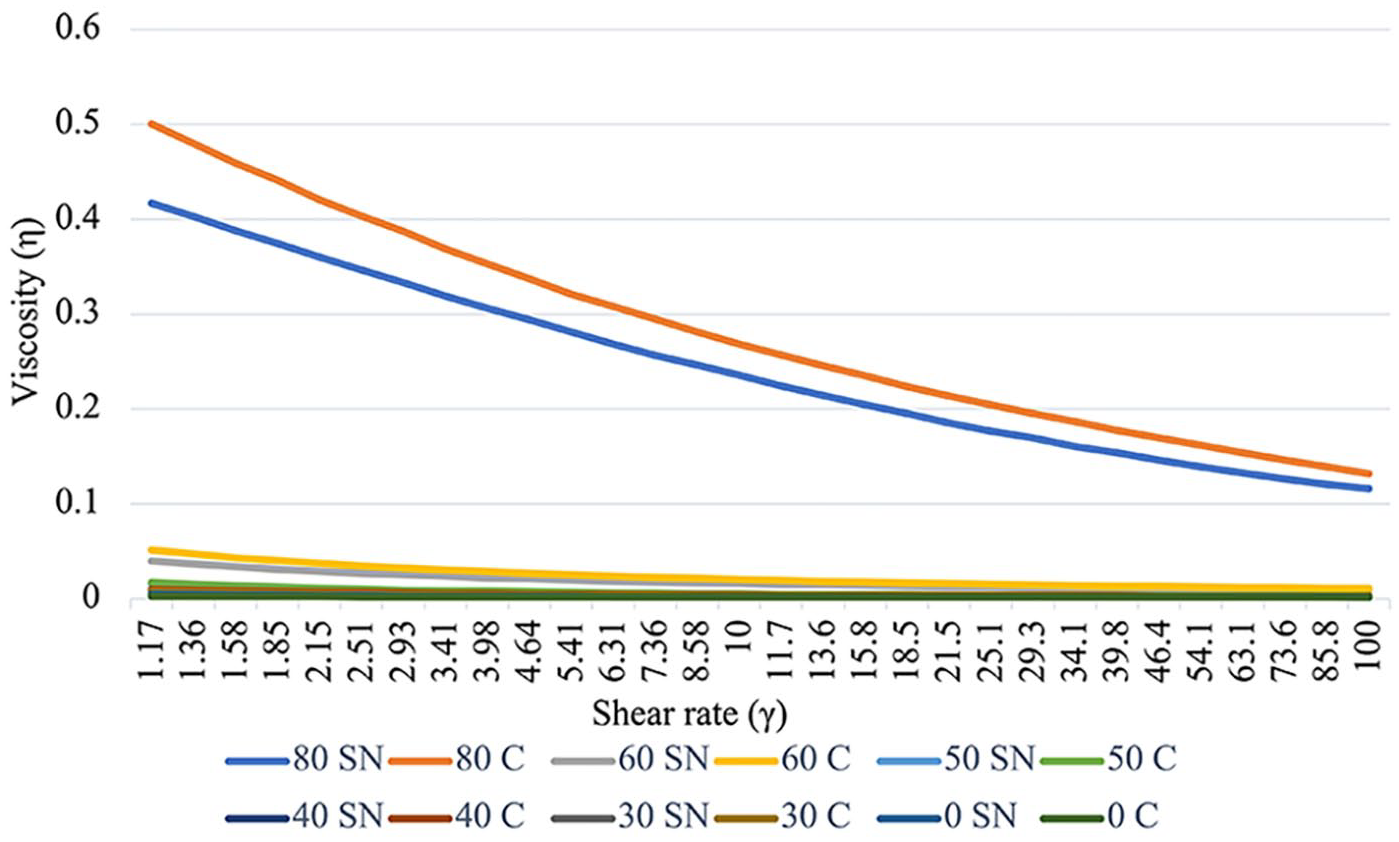
Flow Curves for Non-Homogenized Samples (N = 36).
Flow Curves for Less Condensed Non-Homogenized Samples (N = 36).
The flow rates for homogenized samples shown in Figures 4 and 5 indicated that lower condensation levels had lower viscosity. The 80% condensed samples had very high viscosity and non-Newtonian behavior. Also, apparent viscosity was higher in control for each pair, except for no condensation. It was also evident that non-Newtonian behavior was stronger in more condensed samples.
The flow rates for non-homogenized samples are shown in Figures 6 and 7. Similar to homogenized samples, the viscosity of 80% condensed samples was dramatically higher than all other condensation levels. Figure 7 shows 50%, 40%, 30%, and 0% flow curves separately to be able to observe flow curves of less condensed non-homogenized samples. Viscosity increased as volume reduction increased in non-homogenized samples as well. The apparent viscosity of control was to be higher than the supernatants for non-homogenized samples. Non-Newtonian behavior was stronger in more condensed samples. Also, the non-Newtonian character was more distinct in non-homogenized samples compared to the homogenized samples. Also, we observed a stronger non-Newtonian flow curve on non-homogenized samples.
Discussion
Preterm infants should receive human milk and it should be their mother’s own milk if possible, with proper fortification to meet high nutritional requirements. An exclusive human milk diet gives better outcomes for preterm infants for necrotizing enterocolitis (Delaney Manthe et al., 2019). Therefore, we aimed to find a method to process human milk to increase nutrient content by increasing the concentration of human milk nutrients while avoiding hyperosmolality by partially removing lactose. Our process can presumably increase the concentration of micronutrients as well as protein and lipid. Other volume reduction methods, for example, micro-filtration or ultra-filtration to remove water and lactose, could also lose other small bioactive molecules. We evaluated osmolality and rheological properties of human milk and condensed human milk, for which there is very limited research. In general, the protein amounts for the homogenized milk seemed to be lower than those for the non-homogenized milk. This observation could be due to greater loss of fat by adherence to processing equipment without homogenization, which slightly dilutes the protein.
The lactose removal process yielded a significant reduction in lactose and osmolality. The reduction rate for different condensation levels was not significantly different for lactose or osmolality. There was no significant difference in protein between control and supernatant, which indicated that protein loss did not occur during the lactose removal process and the amount of protein increased as condensation increased. These findings allow us to propose that this method could be used to increase protein and nutrient density while avoiding hyperosmolality. Our results are promising for the use of evaporation in human milk banks to increase human milk-based nutrient density for preterm infants.
Viscosity data showed that human milk has a non-Newtonian shear thinning character, and this character was more pronounced with non-homogenized samples. Viscosity dramatically increased in the over condensed samples (80% and 60% volume reduction). The viscosity of feed might interfere with the use of condensed human milk in a NICU. The high viscosity of feed may cause less fluidity in intragastric (IG) tubes (White & King, 2014). The accuracy of enteral feed pumps depends on the feed’s viscosity. Highly viscous feed lowers the flow rate (White & King, 2014). Feeding pumps set at different flow rates may be inaccurate with non-Newtonian fluids. Delivering fortified feeds with a pump should be done by taking viscosity into account (Howson et al., 2012). Current recommendations for newborn feeding do not discuss viscosity. Milk viscosity should be evaluated to determine the efficiency of nutrient delivery in a NICU. There is a need for further studies to evaluate the microbiological safety and rheological properties of the final product. Also, pasteurization should be incorporated into the method and optimized with further research. The processing method should be simple and inexpensive for it to be applicable in a human milk bank setting.
Limitations
The composition of human milk varies. We obtained the donor milk from an HMBANA milk bank and did not collect information about the donors, stage of lactation, or collection time. We accepted the donor milk collections that were denied use for infant feeding due to the HMBANA regulations. We did not measure the lipid content of our samples, which prevented us from accurately calculating caloric content. However, the lipid was not removed by any of the procedures so its concentration should increase in proportion to the amount of condensation.
Conclusion
Exclusive human milk feeding has many advantages, especially for preterm infants. However preterm infants need higher nutrient density than donor human milk can provide. We achieved significant osmolality and lactose reduction while avoiding protein loss with the lactose removal process. Thus, concentrating human milk in a milk bank setting for feeding preterm infants might be a simple and low-cost process to achieve a product with higher nutrient density and no non-human milk components.
Footnotes
Acknowledgements
April Fogleman, Josip Simunovic, Ruth Watkins, and the Department of Food, Bioprocessing and Nutrition Science at North Carolina State University, Fulbright Program
Disclosures and Conflicts of Interest
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Research was completed as a part of Hande Z. Ulus’s Master’s thesis. Jonathan C. Allen was the chair of her committee. Authors have no conflicts of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The researchers were funded by the Fulbright Scholarship and USDA Hatch funds. The research was funded through Departmental Academic Programs sources.