
Abstract
Marina Ferreira Rea is a Brazilian medical doctor. She has a masters and a doctorate degree in public health from the University of São Paulo (USP). She specialized in breastfeeding at Wellstart International, and completed post-doctoral research at Columbia University, New York, USA, focusing on working women and breastfeeding. She was a researcher at the Health Institute at Columbia University in New York, the Center for Population and Family Health, and at the postgraduate studies, Nutrition in Public Health, University of São Paulo, where she advised many students and published many articles and books (a few selected below). She was a Coordinator of International Breastfeeding Actions at the World Health Organization (Geneva), in the early 1990s, when actions like the Baby-Friendly Hospital Initiative, breastfeeding counseling, and other courses were started. During this same period, the World Alliance for Breastfeeding Action (WABA) and World Breastfeeding Week were initiated. In 1981 she participated in the launching of the International Code of Marketing of Breastmilk Substitutes. Marina Rea is a member of the International Baby Food Action Network and its Latin American policy committee, and is the founder of the International Baby Food Action Network (IBFAN) Brazil group. Since 2017, she has been a member of the IBFAN Global Council. She is now retired but continues to volunteer as an IBFAN member. She has two daughters and four grandchildren. A more detailed curriculum vitae in Portuguese can be found here: http://lattes.cnpq.br/8193850878281835 (MR = Marina Rea; MA = Maryse Arendt)
Keywords
Marina Ferreira Rea, MD, PHD

Maryse Arendt, IBCLC, BSEd, BLL

Interview
When did you come in contact with breastfeeding issues first?
When I finished the Medical School, my residence [internship] was in Preventive Medicine, where we had to go to a rural area to attend patients in a teaching hospital and at health centers. Although many children were malnourished, I saw mothers breastfeeding for long periods; those breastfed babies were less or not malnourished. From this experience came two decisions: to study nutrition in public health and to do research on breastfeeding. And then my first research was my Master’s dissertation about breastfeeding in rural areas of Vale do Ribeira, Sao Paulo (SP; Brazil)—a comparison of families with easy access to artificial milk with families living in more isolated rural villages.
Tell me more about your disserta-tion.
My research study was in a rural area called Vale do Ribeira, SP, one of the poorest area of Sao Paulo State, where the population used to live in “small villages,” and the women worked in tea crops; some villages were linked to the “main commercial village” by roads, but others not. My study was a comparison of these two types of villages, with and without easy access to shops where the powdered milk to prepare baby bottles was available. The results showed that mothers exposed to commercial milks breastfed less. Well. . . I should say that this was my first “realization” about the importance of availability of artificial milk and commercial promotion as a factor to wean babies!
So, you say that the babies were weaned earlier when mothers were in contact with easy access to commercial infant formula or did you find mothers who had not even started breastfeeding? What was the breastfeeding rate, approximatively, during those times?
All mothers started breastfeeding. The babies were breastfed and bottle-fed for long periods. Actually, this was another realization: mixed feeding is not an “obligatory” reason to wean, but it was possible in that environment to continue breastfeeding more than 2 years with a bottle of artificial milk. At least 50% of children were breastfed for 12 months.
As a medical doctor what did you learn about breastfeeding in your academic training?
My medical school, although considered the best in Brazil, did not provide almost any breastfeeding knowledge and training. On the contrary, the Pediatric Department used to get infant formula commercial representatives around, including sometimes breastmilk substitutes (BMS) company representatives were invited to give classes to us, besides offering “free lunch” in the last academic years. By the way, when the American Senator Kennedy did the important memorable hearing at USA Congress on formula feeding marketing and malnutrition in poor countries (Tanovic, 2014; Kennedy Hearings, US Senate Hearings, 1978) the BMS CEO in the film, that ashamed us, was exactly the one from Nestlé Brazil who used to give classes at the Pediatric Department of the School of Medicine I mentioned. . . very sad time.
You worked/served for the World Health Organization [WHO]. How long was this appointment? And what tasks did you have?
I worked in WHO, Geneva. I was hired as a medical officer in the Diarrheal Diseases Control Division (it seems this has another name today) from 1990 to 1992; although, since 1989 I was a consultant for them on breastfeeding and continued to be a consultant after leaving the headquarters [HQ] during subsequent years. I was responsible for the implementation of breastfeeding actions, in the HQ and in countries, particularly Kenya, Tanzania, Philippines, Viet Nam, Colombia.
You have drafted or were involved in the drafting of the Innocenti Declaration. Could you tell us more how this landmark document was born?
During the mid-1980s an important initiative took place called IGAB—Initiative on Global Action on Breastfeeding—with WHO and UNICEF [the United Nations Children’s Fund], as leaders, technical people, bilateral agencies (e.g., Swedish International Development Cooperation Agency [SIDA], United States Agency for International Development [USAID], Norwegian Agency for Development Cooperation [NORAD], etc.) and multilateral agencies, e.g., World Bank. IGAB seminars in different countries were structured/outlined, each one specific for one aspect of breastfeeding policy. The meeting in Florence, Italy on the 31st of July through the 1st of August, 1990, in the Hospedale del Innocenti, was organized to gather a few countries (around 30) with successful experience to share on breastfeeding implementation programs and very good breastfeeding experts. The reports of the previous IGAB meetings were important to stimulate specific discussion such as “breastfeeding by working mothers,” “rooming-in and other hospital routines to start breastfeeding well,” “training and educational materials,” “implementation of the Code,” etc. It was good to hear country cases with critique and come up with the excellent summary of operational targets and objectives for the protection, promotion, and support of breastfeeding (WHO & UNICEF, 1990; WHO & UNICEF, 2005; Table 1).
Innocenti Operational Targets (1990).
These targets are still valid today and should be implemented fully everywhere.
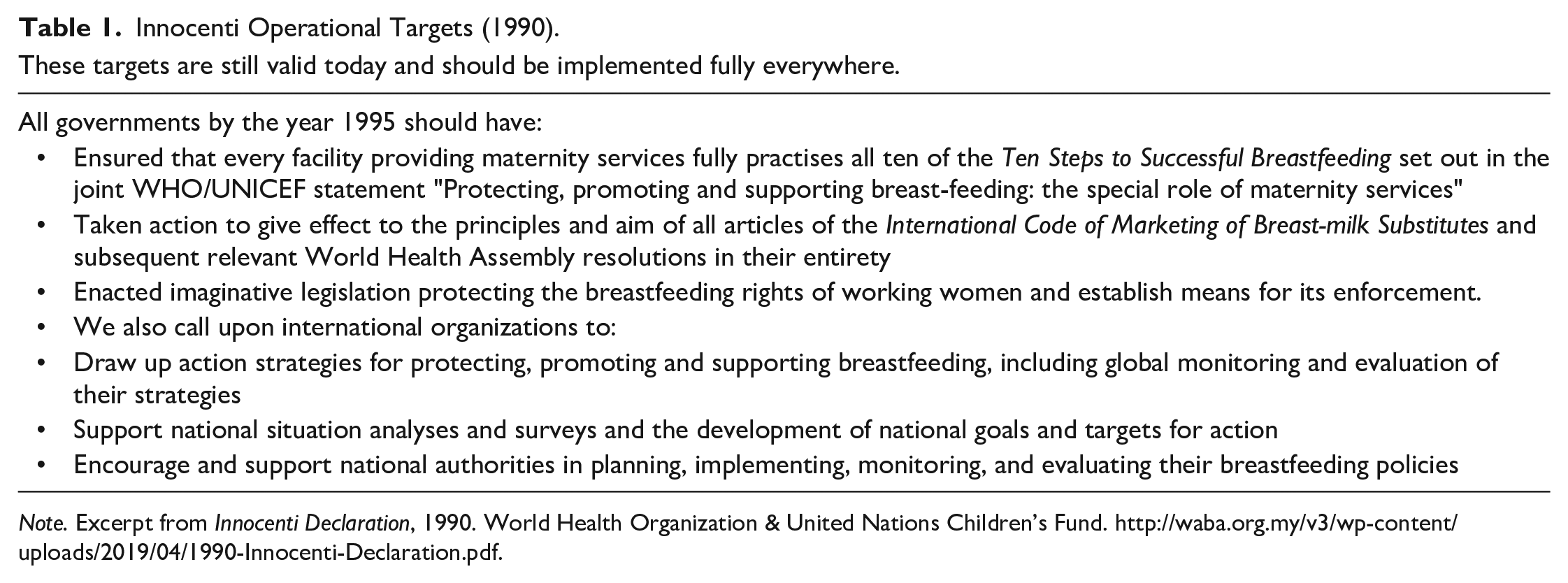
Note. Excerpt from Innocenti Declaration, 1990. World Health Organization & United Nations Children’s Fund. http://waba.org.my/v3/wp-content/uploads/2019/04/1990-Innocenti-Declaration.pdf.
Did you have an active role? And what other persons were involved?
As [a] WHO consultant, I have had an active role during the IGAB meetings, and I was there at the Innocenti meeting hired as a WHO Geneva member. But. . . certainly acting with two other “hats”: An IBFANer (I founded IBFAN Brazil in 1983) and a Brazilian doctor, who has had intense participation in the starting of the Brazilian Breastfeeding Promotion Program in 1981.
You are from Brazil, the country that has launched amazing breastfeeding policies and initiatives since the 1980s. Please tell us more.
In 1981, Brazil launched the Brazilian Breastfeeding Promotion Program (BBPP), supported mostly by UNICEF, with a huge social mobilization through mass media promotion using champions like TV novel artists and football players. UNICEF also hired external consultants like Derrick and Patrice Jelliffe to help the Ministry of Health (MoH) program coordinators. Then, these MoH leaders organized Working Groups on different themes (Education—pre and in service, Regulation, e.g., the Code, Communication, Mother Support, Working Women, Hospital practices—rooming-in, Human Milk Banks and so on) calling on different institutions related to infant and young child feeding (IYCF) to participate. They also suggested the reproduction of this model in universities and at state level (Brazil has 27 states), but only in a few this was well done, but the working groups were all very active. Now, in 2021, we are proudly celebrating 40 years of the BBPP. . . .1981—1988 was a period of ending of the dictatorship with people eager for democracy and free elections. Then, a new Constitution was approved in 1988; this shows why we also approved labor legislation including the extension of maternity leave and a paternity leave; the initiation of the Human Milk Bank Network; and the Brazilian Code! Very successful time! A well-organized breastfeeding program coordination and a support committee were instrumental for this, in my view.
You have done so much for breastfeeding in front of the scene and behind the scenes. Can you tell some of the achievements where you were involved?
The Brazilian Code, approved in 1988, was an important and the biggest achievement. I was the Code Working Group coordinator invited by MoH. I could interfere in the names/institutions of participants; although, the presence of the local milk companies’ representative was obligatory by MoH. The Code working group was strong, although difficult due to the industry representation and the Brazilian Pediatric Society delegate—normally with sponsorship by infant formula companies. Good support from UNICEF was definitive to fund my participation at the World Health Assembly [WHA] 1988 when I had opportunity to talk to MoH delegates and speed up their understanding for approval of the Brazilian Code. Besides, UNICEF also supported Jean-Pierre Allain as a consultant to the Code Working Group; he was a member of the International Code Documentation Centre (ICDC) at IBFAN. He knew well to build different national codes, and helped Brazil during final discussions on wording of articles and political analysis. It was necessary to decide: Should we submit the draft Code to the parliament to enact and publish it as a law or should we keep it at MoH level as a “sanitary” Health Resolution? So, although with good democratic panorama in the country we discussed and concluded that no parliament support was available, and our draft Code could be weakened, undermined by the agro-cattle farmers parliamentarian lobby. We decided to submit just as a national Health Resolution. It was a good decision, and the Code as a law was only approved in 2006, enforced by good articles like the scope that covers products till 36 months, inclusion of whole milk, and different types of warnings, among other achievements.
How do you see your professional trajectory from national to international and vice-versa?
I learned to work in breastfeeding advocacy in 1979–1980 when I got a fellowship at Columbia University, in New York, where I met the beginners of IBFAN and Nestle Boycott, Doug Clement and Leah Margulies. Besides, I met the sweet and strong feminist Elisabet Helsing with whom I worked in a multicentric study on Working Women and Infant Feeding Policies. This allowed my academic and advocacy sides to flourish. Since then, I joined IBFAN and all my professional activities, domestic and internationally, had this footprint leading to combine knowledge and operational implementation of it.
Another important experience was my participation in the International Labor Organization (ILO) meetings in 1999 and 2000 to discuss the Maternity Protection Convention. I was part of the Maternity Protection Coalition of IBFAN-WABA supported by the late Chris Mulford from the International Lactation Consultant Association (ILCA) and other NGOs. These were 2 years of discussions to come up with the Convention 183 and Recommendation 191 (ILO Convention 183, 2000; ILO Recommendation 191, 2000). I was not aware about the “tripartite” way of functioning the organization. It was amazing to follow the delegates of countries. Ministers of Labor were in the middle of the plenary, the employers on the right side, and the trade unions representatives of the employees on the left side. Clearly a very male body, where the discussions related to women’s needs as mothers were not clearly understood, not a priority. After a long initiation of the discussion to “define” what is a mother, I felt shocked with considerations I never listened to before. For example, some country’s Minister of Labour (MoL) proposed to “define” mothers as only those legally married, to apply this Convention! Then. . .it was necessary to lobby to convince some MoL about the unsanitary conditions of human milk expression during working hours in the bathroom, and the need to have adequate rooms for milk expression with paid breaks considered as working hours!
Another difficult agreement was about the weeks of maternity leave. When we realized that the “possible” would be 14 weeks, we worked to convince MoL and even the trade unionists to go for “vote” in favor of this possibility—although it was an insufficient duration for the practice of exclusive breastfeeding. And—terrible anxiety!—we almost lost this poll, as the Nordic countries were against it; they were in favor of “more than 1 year” of maternity leave (of course we were in favor but what was clearly impossible to win). To achieve an ILO Convention is really a lesson to be learnt! By 2021 the Convention was ratified by 39 countries, Brazil has not ratified it, but Luxembourg and many European Countries have done so! This means that all the provisions of the convention are now legal requirements in those countries.
Could you explain which improvements your team managed to get in the new Convention?
I am just naming the major ones! We managed to extend the paid leave for mothers from 12 to a minimum of 14 weeks and to define that the payment during the leave should be full or at least two-thirds of the woman’s previous earnings. We could get a better definition of one or more daily breaks or a daily reduction of hours of work to breastfeed her child and to be counted as working hours. We secured job security by awarding the women a guaranteed right to return to the same position or an equivalent position paid at the same rate at the end of her maternity leave; we could assure that the women can get the total leave after the birth, not obligatory in pregnancy.
What improvements were reached through the Recommendation?
The 2000 ILO recommendation 191 supplements the Convention and is a recommendation for countries with ideas to further improve maternity protection. It contains these main recommendations: (a) 18 weeks of fully paid maternity leave at the level of the previous earnings; (b) assessment of work place risks and if elimination of risks cannot be eliminated and no adaptation can be made than the woman should be put on paid leave; and (c) breastfeeding facilities at or near the workplace.
You were really active in many fields to protect breastfeeding; what would you recommend now to the readers as advocacy topics or as policy needs in their community or at national level?
We certainly learned a lot during these almost 5 decades of working pro-breastfeeding. It is always difficult to advise readers, as we should take into consideration the environment, the family and professional circumstances, the community, and cultural behavior of people, when working on infant feeding practices. But I will try:
1) There is a clear increase in the use and abuse of artificial foods, due to cheaper prices, and accessibility. Strong, fragile human beings should/must get the “golden” standard food—human milk. Therefore, we should continually advise this as our main advocacy flag. 2) There are clear pro-breastfeeding strategies that have been shown to be effective and appropriate. These are important advocacy tools and must be part of breastfeeding policies: a) The implementation of the International Code of Marketing of Breastmilk Substitutes and relevant WHA Resolutions, to counteract the aggressive marketing of BMS corporations (WHO, 1981–2020). b) The implementation of the Baby-Friendly Hospital Initiative (Rea, 2011), to start breastfeeding well immediately after birth and keep it exclusively for 6 months (WHO & UNICEF, 2018). c) The inclusion of “counseling” techniques and skills in the pre-service and in-service training of health workers on infant feeding, to be part of all ambulatory, out of hospital community care to support longer breastfeeding practice and duration. d) The implementation of adequate labor benefits for maternity protection to assist lactating working women (Rea & Morrow, 2004).
Footnotes
Disclosures and Conflicts of Interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Ms. Arendt is an JHL Assistant Editor for the WHO International Code for the Marketing of Breast-milk Substitutes and is ILCA’s Delegate to the Codex Alimentarius. Authors have no conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.