
Abstract
Background:
Only 61% of Malawian women exclusively breastfeed to the recommended 6 months. Paternal support is predictive of exclusive breastfeeding, and significantly related to paternal breastfeeding self-efficacy, defined as fathers’ confidence in their ability to assist mothers with breastfeeding.
Research Aims:
To (1) examine the psychometric properties of the Paternal Breastfeeding Self-Efficacy Scale-Short Form (BSES-SF) in Malawian fathers, including internal consistency reliability, test-retest reliability, construct validity using Confirmatory Factor Analysis (CFA), and convergent validity; and (2) assess the relationship between the BSES-SF and paternal demographic and health factors.
Methods:
A cross-sectional study was conducted at a maternity hospital in Lilongwe, Malawi, and 180 fathers whose partners had delivered a singleton infant were included. Participants completed the Breastfeeding Self-Efficacy Scale and Quality of Life with confirmatory factor analysis performed to assess the construct validity. The internal consistency reliability and test-retest reliability were evaluated using Cronbach’s alpha coefficient and intra-class correlations. Convergent validity was also assessed.
Results:
A unidimensional factorial structure of the Malawian Paternal BSES-SF was identified using confirmatory factor analysis. The scale had an excellent Cronbach’s alpha of .90 and a test-retest reliability of .93. Participants’ breastfeeding self-efficacy was significantly correlated with the Quality of Life domains of psychological health (r = .23; p < .01), social relationships (r = .28; p < .001), and environmental health (r = .30; p < .001). Participants who were older, married, and with ≥ two children had significantly higher breastfeeding self-efficacy and were more confident in their ability to support their partner’s breastfeeding.
Conclusion:
The Paternal Breastfeeding Self-Efficacy Scale-Short Form was a valid and reliable measure to assess fathers’ confidence in their ability to assist mothers with breastfeeding in Malawi.
Keywords
Key messages
A prior study that psychometrically evaluated the Paternal Breastfeeding Self-Efficacy Scale-Short Form confirmed a unidimensional factor structure, but its psychometric properties among African fathers remain unknown.
Our psychometric study confirmed the Malawian version of this instrument to be a valid and reliable tool for assessing Malawian fathers’ confidence in providing breastfeeding support.
Our findings will aid in the identification of high-risk fathers with low breastfeeding self-efficacy levels and thus support Malawian breastfeeding families.
Background
In Malawi, breastfeeding exclusivity to 6 months postpartum, as recommended by the World Health Organization (WHO) and the Malawi Ministry of Health, remains a clinical problem despite the implementation of the Baby-Friendly Hospital Initiative (BFHI) into national breastfeeding programs (Kavle et al., 2019). A recent national Malawian survey found that 76.9% of women initiated breastfeeding, and 79% continued to 6 months postpartum, but only 61% did so exclusively (National Statistical Office/Malawi & ICF, 2017). This 6-month breastfeeding exclusivity rate is significantly lower than the 90% recommended by the WHO (Cai et al., 2012). A new approach to this long-standing clinical problem for Malawian mothers is needed. Paternal breastfeeding self-efficacy has been highly associated with their ability to provide breastfeeding support, which is a critical factor for sustaining breastfeeding exclusivity (Abbass-Dick et al., 2015). While most fathers want to support their partner with breastfeeding, many lack confidence in their ability to do so and are unable to engage in breastfeeding promotion activities (Al Namir et al., 2017). Thus, the prompt assessment of paternal self-efficacy and the provision of targeted interventions that increase both maternal and paternal breastfeeding self-efficacy should become a health priority in breastfeeding programs (Abbass-Dick et al., 2015). The Paternal Breastfeeding Self-Efficacy Scale-Short Form (BSES-SF) was developed and evaluated in Canada (Dennis et al., 2018), but its psychometric properties have not been evaluated among fathers in Africa, including those in Malawi.
The original Paternal BSES-SF was developed to measure a father’s confidence in his ability to assist his partner with breastfeeding (Dennis et al., 2018). The English version of the BSES-SF has been tested for psychometric properties, including internal consistency reliability, concurrent validity, and predictive validity, and a unidimensional factor structure was reported (Dennis et al., 2018). Whether a similar factor structure of Paternal BSES-SF exists in African samples remains to be investigated. This scale is a translated version of the internationally validated Maternal BSES-SF (Dennis, 2003). Investigation of the paternal version of the BSES-SF among African fathers will ensure the cultural relevance of breastfeeding measures that can be used to reliably identify at-risk breastfeeding families and evaluate the results of supportive interventions aimed at increasing duration and exclusivity rates.
Identifying factors associated with breastfeeding self-efficacy is important in establishing the validity of the paternal version of the Breastfeeding Self-Efficacy Scale. Researchers have suggested that factors (e.g., age, parity, and childbirth experience) are positively associated with breastfeeding self-efficacy scores (Dennis, 2006). Modifiable variables (e.g., depression and anxiety) are negatively related to breastfeeding self-efficacy, while Quality of Life (QoL) measures, including the physical well-being, psychological health, social relations, and environmental domains, are positively related to breastfeeding self-efficacy (Mirghafourvand et al., 2018). These factors have only been examined in maternal samples, and it is unknown if they influence paternal breastfeeding self-efficacy. Therefore, the study aimed to: (1) examine the psychometric properties of the Paternal BSES-SF in Malawian fathers, including internal consistency reliability, test-retest reliability, construct validity using Confirmatory Factor Analysis (CFA), and convergent validity; and (2) assess the relationship between the BSES-SF and paternal demographic and health factors.
Methods
Research Design
A cross-sectional, prospective study was conducted. This study design allowed us to collect the breastfeeding self-efficacy information of eligible fathers in the hospital. Ethical approval for this study was obtained from the Institutional Review Board and the National Health Sciences Research Committee of the study hospital (No: N201906063).
Setting and Relevant Context
The study hospital is designated as a Baby-Friendly Hospital that serves a population of almost 2 million and has over 12,000 deliveries a year (Chisenga et al., 2015). One of the largest maternity hospitals in Malawi, it is located in Lilongwe, the capital of Malawi (Chisenga et al., 2015). In low-income countries, such as Malawi, the length of hospital stay for postpartum is 48 hr for those who underwent a normal delivery and 5 days for those who delivered via caesarian delivery (Campbell et al., 2016). Postpartum women receive breastfeeding support and health instruction from nurses during their hospital stay and the hospital follows the Malawi Infant and Young Child Nutrition (IYCN) policy to promote and support exclusive breastfeeding (Ministry of Health and Population, 2020). A population-based study indicated that Malawian mothers who delivered in the hospital setting were more likely to exclusively breastfeed until 6 months postpartum compared to mothers who delivered at home (Chipojola et al., 2020), suggesting beneficial results of this national nutritional program.
Sample
A convenience sample of fathers whose partners had delivered at a district hospital in central Malawi were recruited. In total 200 fathers were approached to participate in the study, of which 180 were eligible and agreed to participate. The inclusion criteria were fathers who were 20 years of age and above, could understand and read Chichewa, and whose partner had had a singleton live birth. We focused on singleton pregnancies because the psychometric properties of the original English version of the BSES-SF were examined in fathers whose partners had delivered a singleton birth (Dennis et al., 2018) and we wanted to provide comparable results. Fathers were excluded if their infant had congenital fetal anomalies or a significant illness that could influence breastfeeding, or their partner had a significant obstetric complication (e.g., postpartum hemorrhage). A sample estimation of 140 participants was calculated based on the traditional rule of 10 participants for each item (Tinsley & Tinsley, 1987). Considering a 20% possible incompletion and attrition rate (Nukpezah et al., 2018), a sample of 168 participants was determined as adequate for this study.
Measurement
The Translation Process of the Paternal BSES-SF
We followed standard translation and back-translation procedures (Wild et al., 2005). Translation of the English version of the Paternal BSES-SF to the Chichewa language was carried out by a professional translator who was a native Chichewa speaker and fluent in English. The Malawian Paternal BSES-SF version was then back-translated into English by an independent bilingual expert with clinical child health and breastfeeding expertise, who was not aware of the original scale wording. To ensure clarity and semantic equivalence, the original English version of the Paternal BSES-SF was compared to the back-translated version by a panel of three clinical experts, which included a pediatric specialist, a breastfeeding specialist, and a maternity head nurse, all with over 10 years’ experience in their clinical area. The Malawian Paternal BSES-SF version was considered an accurate translation of the original English Paternal BSES-SF version by the expert panel, and no modifications were required. The Malawian version of the Paternal BSES-SF was then pilot tested and surveyed with 20 fathers whose partners were breastfeeding to determine face validity, clarity, and cultural relevance. They reported that the Malawian version was easy to understand and applicable to their breastfeeding experience, and no revisions were requested.
Paternal Breastfeeding Self-Efficacy Scale–Short Form
This measure is a self-report 14-item questionnaire that assesses a father’s confidence in his ability to assist his partner with breastfeeding (Dennis et al., 2018). The items are rated on a 5-point Likert scale where 1 = not at all confident and 5 = very confident, with a total score ranging from 14–70. A higher score indicates higher breastfeeding self-efficacy. In the original Canadian study that validated the paternal version, a Cronbach’s alpha of .91 was found in hospital and .92 at 6 weeks’ postpartum, and predictive validity of exclusive breastfeeding was reported (Dennis et al., 2018).
Quality of Life (QoL)
QoL was measured using the 26-item Chichewa version of an abbreviated Quality of Life scale developed by the WHOQoL-BREF (Colbourn et al., 2012b). This measure includes two items that assess overall QoL and overall health related QoL, and 24 items that measure the following four QoL domains: (1) physical well-being, (2) psychological well-being, (3) social relations, and (4) environment health (Colbourn et al., 2012b). Each item was rated using a 5-point Likert scale, generating the domain scores. The sum scores of the four domains scores were then transformed to a linear scale of 0–100, in which a higher score indicates a higher QoL (WHO, 1996). In this study, the Cronbach’s alphas were .70, .73, .71, and .74 for the physical health, psychological health, social relationships, and environmental domains, respectively, and the overall Cronbach’s alpha for the entire QoL scale was .77.
Paternal Demographic and Health Characteristics
A structured demographic questionnaire based on prior studies was developed to collect potentially important covariates of breastfeeding self-efficacy, including paternal age (15–49 years old), marital status (never married, divorced, or married), occupational status (unemployed or employed), and education level (illiterate or primary education and above; Dennis et al., 2018). Health variables, for example, delivery mode (vaginal or cesarean delivery), and parity (primiparous or multiparous), were also included (Dennis et al., 2018).
Infant Feeding Practice
A self-reported questionnaire was used to examine the infant feeding method at hospital discharge. The infant feeding method was assessed using the WHO (2008) definition, which included: (1) exclusive breastfeeding (infants who were given human milk only, with no other additional supplements, e.g., powdered milk, infant formula milk, or solids); (2) predominant breastfeeding (infants who received human milk as the primary source of nutrition, but were also given liquids, e.g., formula, water, water-based drinks, or juice); and (3) bottle feeding (infants who received some liquids or semisolid food from a bottle with a nipple). Fathers were instructed to choose the infant feeding indicator that best represented how they had fed their infant in the past 24 hr. We then combined the predominant breastfeeding and bottle-feeding practices as non-exclusive breastfeeding for the subsequent analysis.
Data Collection
Participants were enrolled in our study between August and September 2019. Following informed consent procedures, the eligible participants who agreed to participate completed a study questionnaire in hospital. Among the 180 participants, a sub-group (n = 30), whose partner returned for a postpartum check-up, completed a second Paternal BSES-SF questionnaire at 2 weeks’ postpartum to assess test-retest reliability. A sample size of 22 was needed to detect the intra-class correlation coefficient (ICC) of 0.50 with 80% power and alpha = 0.05 (Bujang & Baharum, 2017). Considering an attrition rate of 20%, the estimated target sample size for test-retest reliability was 28. To ensure data quality, data collectors were trained in all study and data collection procedures. Participants who were able to read and understand the Chichewa language completed the study questionnaire on their own. On average, each participant spent 30–45 min filling out the questionnaires. Illiterate fathers were assisted by the data collectors to fill in the questionnaires. Upon completion, all questionnaires were checked to catch any missing data. All collected information or data were entered and stored in a secured (i.e., password protected) computer. The questionnaires were stored in a locked cabinet in the principal investigator’s office.
Data Analysis
SPSS (Version 21) and AMOS (Version 25) were used for this analysis. Continuous data were expressed as the mean (M) and standard deviation (SD), and categorical variables were described using frequencies and percentages. Descriptive statistics were used to examine any missing items, and no missing items were found. An assumption of a normal distribution was assessed using the index of skewness (recommended range: -3 to +3) and kurtosis (recommended value: < 7; Jennings et al., 2002). A Cronbach’s alpha value of ≥ .70 (Tavakol & Dennick, 2011), inter-item correlation, and corrected-item total correlation were used to assess the internal consistency reliability of the Paternal BSES-SF. The test-retest reliability, an estimate of test consistency over a short period of time, was analyzed using the intra-class correlation (ICC) based on the procedure outlined by Koo and Li, with a suggested value of ≥ .75 (Koo & Li, 2016).
To examine the construct validity of the Paternal BSES-SF scale for the Malawian sample, CFA was carried out using the maximum-likelihood estimation method. The CFA was carried out to determine the unidimensional factor structure of the Paternal BSES-SF (Dennis et al., 2018). The model fit of the scale was determined using the following goodness-of-fit indices and their recommended values: χ2/df ( ≤ 3; Simon et al., 2010), Tucker-Lewis index (TLI; ≥ 90), comparative fit index (CFI; ≥ 90), root mean square residual (RMR) ≤ .08; Black et al., 2010), and the Akaike information criterion (AIC [the smaller the better] Kline, 2011). A factor loading of ≥ 0.30 indicated that an item adequately represented its factor (Swisher et al., 2004). Convergent validity was examined by calculating Pearson’s correlation coefficient between the Paternal BSES-SF scores and QoL domains. In the present study, we adopted a QoL scale instead of related measures of self-efficacy because of the lack of validated instruments (i.e., general self-efficacy scale) in Malawi. As with a prior study (Mirghafourvand et al., 2018), we hypothesized that the Paternal BSES-SF would be positively correlated with the four QoL domains. Independent-sample t tests were used to examine the relationships of the Paternal BSES-SF with baseline demographic and health variables. A p-value of < .05 was set for statistically significant results.
Results
Study Sample
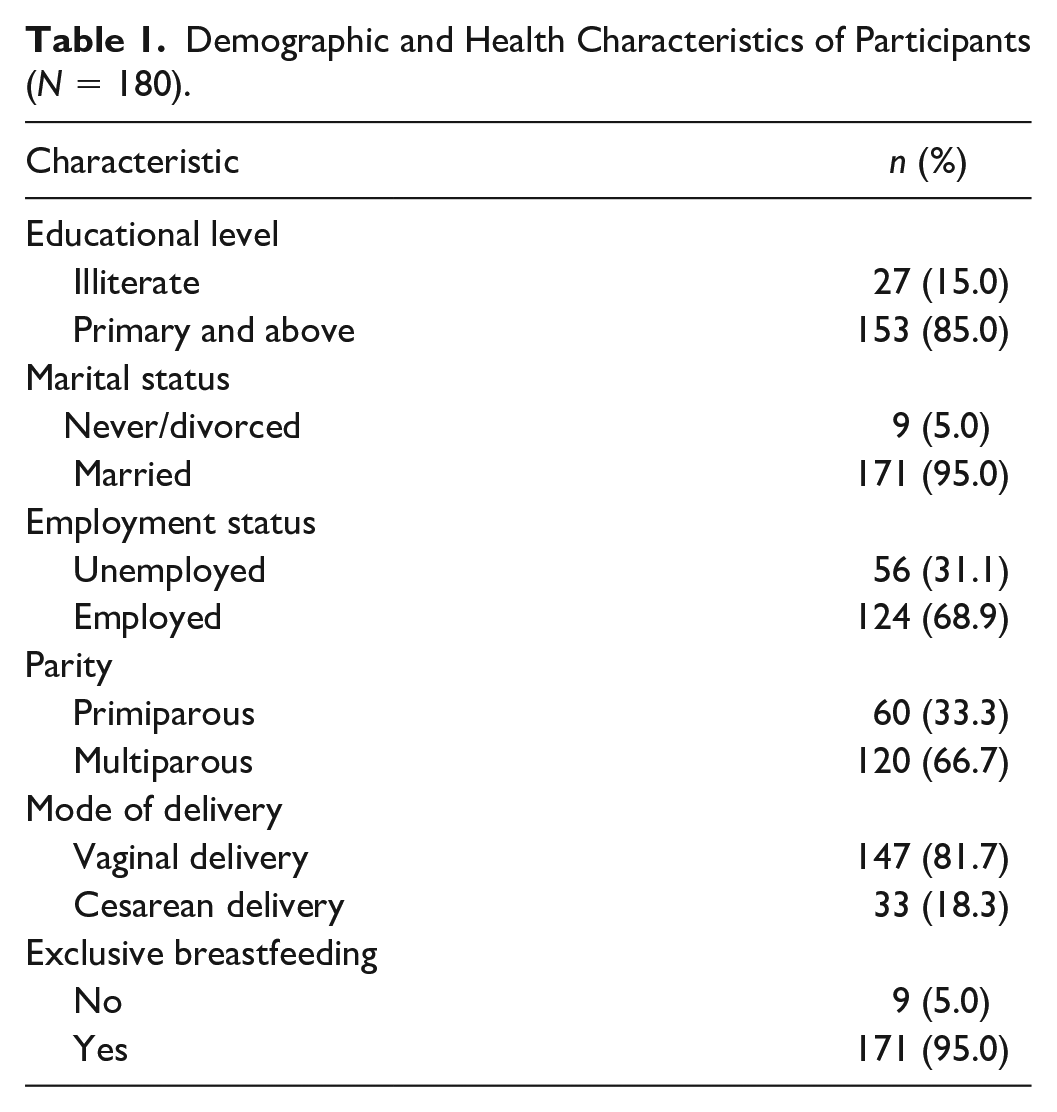
The average age of the participants was 30.4 (SD = 6.7) years and the majority of whom were married (n = 171; 95.0%), literate (n = 153; 95%), had a multiparous partner (n = 120; 66.7%), and infants who were born vaginally (n = 147; 81.7%). The majority of participants’ partners were exclusively breastfeeding (n = 171; 95.0%). Tables 1 and 2 display their demographic information.
Demographic and Health Characteristics of Participants (N = 180).
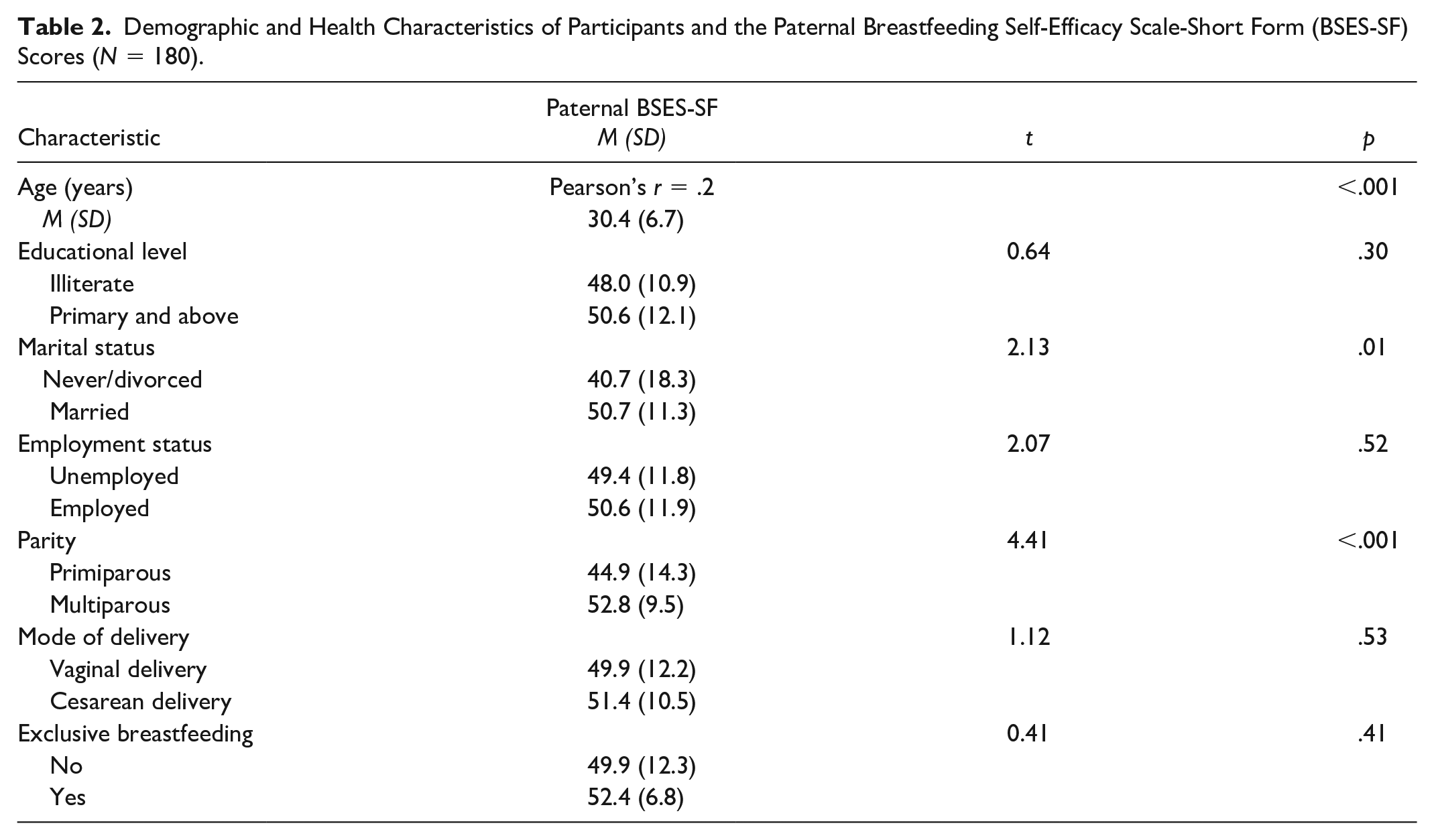
Demographic and Health Characteristics of Participants and the Paternal Breastfeeding Self-Efficacy Scale-Short Form (BSES-SF) Scores (N = 180).
Internal Consistency and Test Re-Test Reliability of the Paternal BSES-SF
The Paternal BSES-SF scale had a mean total score of 50.2 (SD = 11.9). Each Paternal BSES-SF item had mean values ranging from 2.9 to 4.0 (SD = 1.0–1.6). The data indicated a normal distribution, with a skewness value range of -.1 to -1.4, and a kurtosis value range of -.1 to 2.9 (Table 3). According to Table 3, all corrected item-total correlations had positive values and were within an acceptable range of .40–.80 (Tabachnick & Fidell, 2001). The Paternal BSES-SF had a Cronbach’s alpha of .90 and deleting any item of the Paternal BSES-SF did not increase the overall Cronbach’s alpha by more than 0.10, indicating that all items measured the construct of breastfeeding self-efficacy. Additionally, the Paternal BSES-SF had a test-retest reliability (i.e., intra-class correlation, ICC) value of .93, suggesting excellent reliability.
Descriptive Statistics and Internal Consistency of the Paternal Breastfeeding Self-Efficacy Scale-Short Form (N = 180).
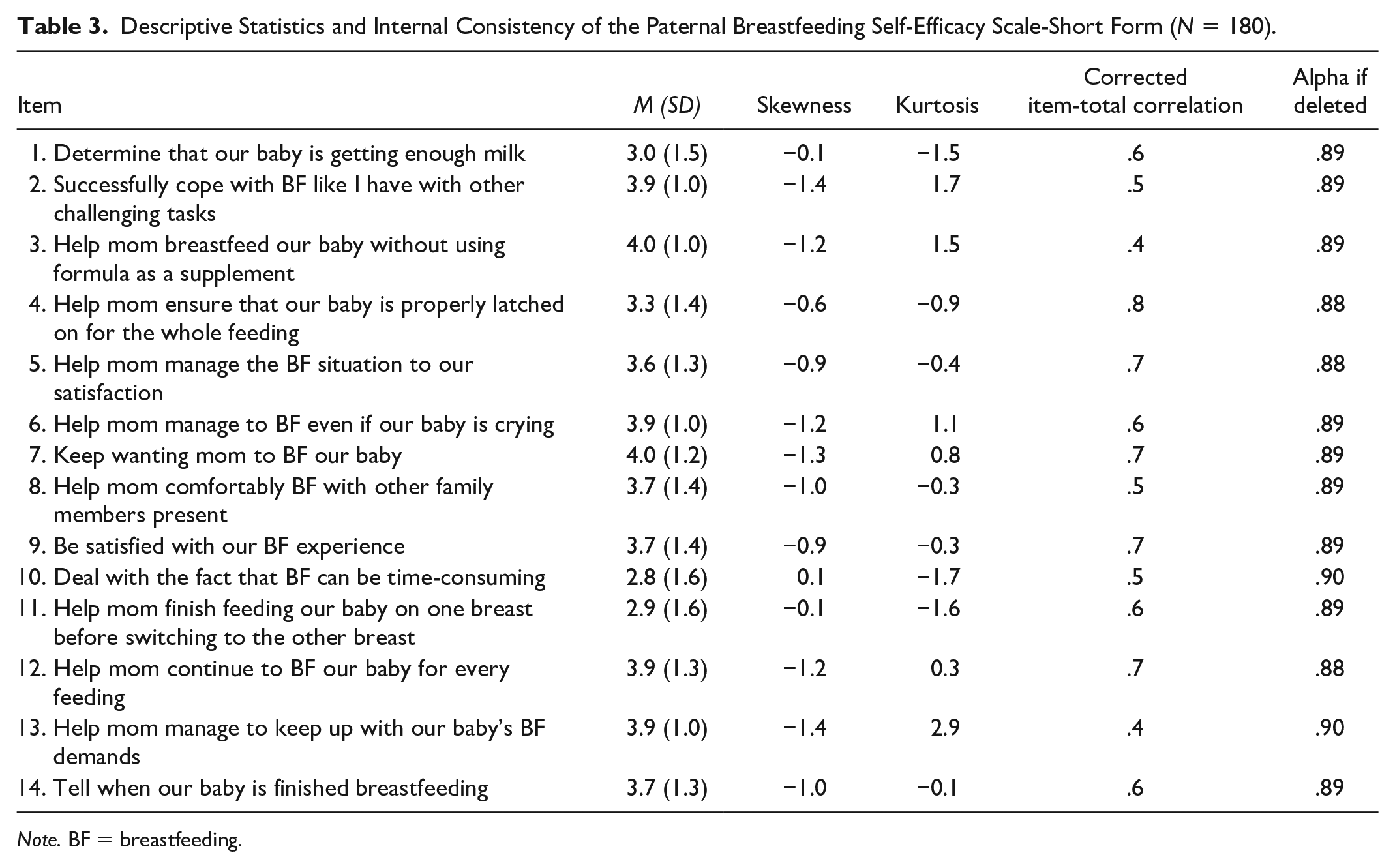
Note. BF = breastfeeding.
Construct Validity
A one-factor structure of the scale was examined using confirmatory factor analysis based on prior evidence (Dennis et al., 2018). The initial results of the model fit indices for a one-factor structure were not optimal (χ2/df = 3.89; RMR = .17; CFI = .80; TLI = .77). We inspected the item inter-correlations and found that Items 2 and 3, 2 and 6, 4 and 5, 10 and 4, 10 and 11, and 1, 2, 4, 8, and 11 were strongly correlated with each other. Accordingly, the covariance of the correlated items was modeled, and improvements in the model fitting indices were observed in the Paternal BSES-SF factor structure (χ2/df = 1.59; RMR = .08; TLI = .95; CFI = .97; Table 4). The factor loadings of each item to the common factor were all > .30, suggesting that each item was highly relevant for the factor identified (Table 5).
Confirmatory Factor Analysis (CFA) Goodness-of-Fit Statistics of the Paternal Breastfeeding Self-Efficacy Scale-Short Form Items (N = 180).
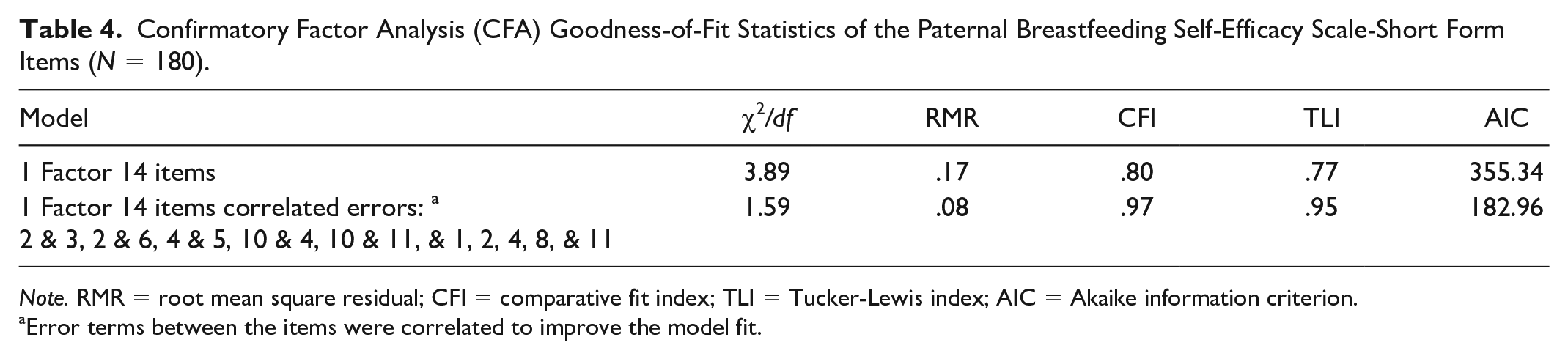
Note. RMR = root mean square residual; CFI = comparative fit index; TLI = Tucker-Lewis index; AIC = Akaike information criterion.
Error terms between the items were correlated to improve the model fit.
Factor Loadings of Paternal Breastfeeding Self-Efficacy Scale-Short Form.
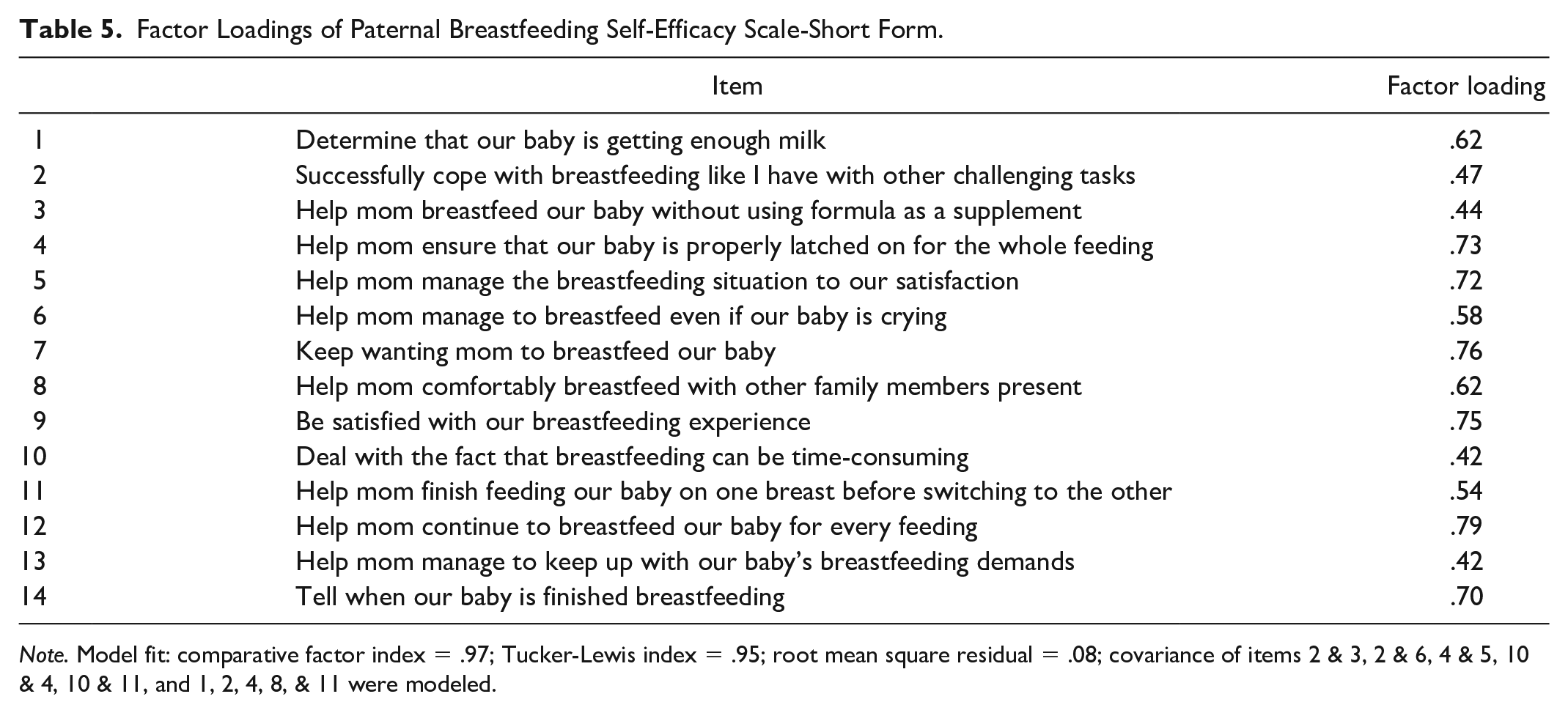
Note. Model fit: comparative factor index = .97; Tucker-Lewis index = .95; root mean square residual = .08; covariance of items 2 & 3, 2 & 6, 4 & 5, 10 & 4, 10 & 11, and 1, 2, 4, 8, & 11 were modeled.
Convergent Validity
The Paternal BSES-SF scores were significantly correlated to the following three Quality of Life domains scores: psychological well-being (r =.23, p < .01), social relations (r =.28, p < .001), and the environment (r =.30, p < .001). The Paternal BSES-SF had no significant correlation with the physical well-being domain (r =.01, p =.13).
Paternal BSES-SF and its Relationships With Demographic and Health Variables
Table 2 indicated a significant positive correlation between Paternal BSES-SF scores and paternal age (r = .2; p < .001). Married participants reported a higher score on the Paternal BSES-SF (M = 50.7, SD = 11.3) than those who were not married (M = 40.7, SD = 18.3; t [178] = 2.13; p < .05). Paternal breastfeeding self-efficacy mean scores were also significantly higher among multiparous fathers who had two or more children (M = 52.8, SD = 9.5) compared to those who had only one child (M = 44.9, SD = 14.3; t [178] = 4.41; p < .001). There were no significant differences in the paternal breastfeeding self-efficacy scores between those whose partner was exclusively breastfeeding (M = 52.4, SD = 6.8) and those whose infant was not exclusively breastfed (M = 49.9, SD = 12.3; t [178] = .12, p = .41).
Discussion
We examined the psychometric properties of the translated Malawian version of the Paternal BSES-SF. This was the first study to examine breastfeeding self-efficacy among fathers in Africa. Our results suggested a unidimensional structure using a confirmatory factor analysis, which was similar to the original Paternal BSES-SF version. Both the internal consistency and test-retest reliability index were excellent. Regarding convergent validity, we found that there was a significant positive correlation between the Paternal BSES-SF scores and the QoL domains of psychological well-being, social relations, and the environment, but not the physical wellbeing domain. We also found that the Paternal BSES-SF scores were strongly related to older age, marital status, and the number of children. Overall, our results demonstrated that the Malawian version of the Paternal BSES-SF was a reliable and valid measure in the Malawian context and can be used to assess a father’s confidence in providing breastfeeding support to his partner while in-hospital soon after birth and at 2 weeks’ postpartum.
The CFA findings provided empirical support for the unidimensional Paternal BSES-SF structure, which was consistent with the original Paternal BSES-SF study (Dennis et al., 2018). So far, researchers have conducted limited studies exploring the BSES-SF in paternal samples. Our study provided initial evidence that it may be appropriate for health professionals to use the Paternal BSES-SF to assess African fathers’ confidence in their ability to support their partner with breastfeeding. Future researchers need to explore the factor structure of the Paternal BSES-SF at different postpartum periods and in different countries in Africa.
The Cronbach’s alpha coefficient value of the present analysis was similar to that of a previous Canadian study of the Paternal BSES-SF (Dennis et al., 2018). It exceeded the minimum acceptable standard of .80, suggesting good internal consistency (Taber, 2018). Further, our study demonstrated a high value of test-retest reliability, which signified the temporal stability of the Paternal BSES-SF and ensured that the scores obtained in-hospital were both representative and stable over time. This finding is clinically important in the identification of fathers with low breastfeeding self-efficacy levels who may benefit from future self-efficacy enhancement interventions.
In our study, paternal breastfeeding self-efficacy was significantly positively correlated with the psychological health, social relationships, and environmental domains of QoL, which were consistent with our study hypothesis and in line with a recent Iranian study involving a sample of mothers (Mirghafourvand et al., 2018). In the African setting, men perceive their life to be meaningful by raising children and heading a family, which symbolizes lineage continuation (Mlungwana, 2020). Increased paternal breastfeeding self-efficacy assists fathers in achieving their family responsibilities. However, the overall QoL physical domain was not correlated with the Paternal BSES-SF. This domain consists of physical pain, sleep, dependence on medical aids, fatigue, and energy (Colbourn et al., 2012a). In this African setting, the expression of physical discomforts, for example, physical pain, is culturally unacceptable among men. It is regarded as a sign of weakness so it is not surprising that the majority of the participants may have underreported their physical discomfort resulting in this finding (Nortjé & Albertyn, 2015). Future studies examining convergent validity among Malawian paternal samples is recommended and may improve the clinical utility of the measure with this population.
Paternal breastfeeding self-efficacy was related to several demographic variables. Consistent with researchers who have examined maternal breastfeeding self-efficacy (Dennis, 2006), fathers with more than two children were more efficacious than those with one child. Thus, it is important to screen breastfeeding self-efficacy among young first-time fathers to identify those requiring additional support from professionals so that they, in return, can provide effective breastfeeding support to their partners. Additionally, we found a positive correlation between marital status and paternal breastfeeding self-efficacy. In Africa, marriage is regarded as a sign of a more stable and committed relationship (Phillips, 2018) and may highlight an opportunity to enhance not only breastfeeding duration but also exclusivity rates. These families may be more receptive to utilizing a coparenting approach at home (i.e., parents working together as a team), which would increase their likelihood of having better breastfeeding outcomes (Abbass-Dick et al., 2015). Lastly, it is important to note that the majority (66.1%) of our sample was living in an urban area, where coverage of healthcare facilities was at 70% (Palk et al., 2020). This gave the majority of our families access to breastfeeding-related knowledge, which could have increased their breastfeeding self-efficacy. Understanding the relationship between demographic variables and breastfeeding self-efficacy assists health care professionals in their ability to effectively target high-risk families that require additional breastfeeding support to achieve recommended breastfeeding outcomes, such as exclusivity to 6 months’ postpartum.
In the original Paternal BSES-SF study (Dennis et al., 2018), Paternal BSES-SF scores were associated with exclusive breastfeeding rates at 6 weeks’ and 12 weeks’ postpartum. In the present analysis, the Paternal BSES-SF scores were not correlated to exclusive breastfeeding rates while in hospital. However, it is important to note that the majority of participants’ partners were exclusively breastfeeding so there was insufficient variability to detect a relationship. Further research is warranted to explore the relationship between paternal breastfeeding and breastfeeding outcomes to 6 months’ postpartum.
Limitations
There were some limitations to the present study. First, despite the fact that this research was conducted in the largest maternity facility located in an urban area, it provided less accessibility to fathers residing in rural areas; this limits the generalizability of our study findings. Second, the predictive validity was not evaluated in our study. Future studies are thus warranted to examine the Paternal BSES-SF’s predictive validity. Third, the Paternal BSES-SF scale was only used at hospital discharge and 2 weeks’ postpartum, when most women remain exclusively breastfeeding. Further studies with repeated infant feeding assessments at postpartum 6 weeks and 12 weeks would be helpful to determine if the Paternal BSES-SF scores within the first 2 weeks’ postpartum are associated with breastfeeding outcome, as we see with maternal breastfeeding self-efficacy.
Conclusions
Our research provided appropriate reliability and validity of a one-dimensional Paternal BSES-SF in measuring the breastfeeding confidence of fathers in Malawi. Healthcare professionals can adopt this tool to screen fathers for further breastfeeding interventions in order to achieve adequate support for their partners to successfully breastfeed during the first 6 months after their child’s birth. In the future, Malawian researchers can use this instrument as a reference for promoting sustained exclusive breastfeeding.
Footnotes
Disclosures and Conflicts of Interest
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Roselyn Chipojola completed this manuscript as part of her PhD dissertation. Professor Shu-Yu Kuo was the student’s advisor and she served as a committee member during the dissertation defense. The authors declare that they do not have conflicts of interest. Professor Cindy-Lee Dennis is the creator of the Paternal Breastfeeding Self-Efficacy Scale-Short Form.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Ministry of Science and Technology, Taiwan (MOST 107-2314-B-038-034, MOST 106-2314-B-038-012, and MOST 104-2314-B-038-008). The contents are solely the responsibility of the authors and do not necessarily represent the funders. The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.