
Abstract
Background:
Because of its many benefits, exclusive breastfeeding for 6 months is a common public health goal. However, only 44% of infants aged 0–6 months are exclusively breastfed worldwide and, in the United States, only 26% of infants are exclusively breastfed for 6 months. The restrictions imposed during the COVID-19 pandemic may have reduced these rates even further.
Research Aim:
To examine the differences in breastfeeding exclusivity and satisfaction before and during the COVID-19 pandemic.
Methods:
A cross-sectional, two-group survey design was used. Parents (N = 110) of infants born April 1 to December 31, 2019 (pre-pandemic; n = 69), or April 1 to December 31, 2020 (during the pandemic; n = 41), who received lactation support services from an urban academic breastfeeding clinic were surveyed.
Results:
Respondents who gave birth in 2020 (pandemic year) were no less likely to exclusively breastfeed for the first 6 months of their infant’s life compared to respondents who gave birth in 2019 (pre-pandemic year). After multivariable logistic regression, the odds of high breastfeeding satisfaction were 73% lower in respondents with infants born in 2020 than in respondents with infants born in 2019 (OR = 0.27, 95% CI [0.08, 0.89]). The strongest contributor to high breastfeeding satisfaction was a prenatal breastfeeding visit with an International Board Certified Lactation Consultant.
Conclusions:
Future research is needed to identify the specific pandemic-related factors that led to the difference in breastfeeding satisfaction between the two groups and to confirm the impact of prenatal International Board Certified Lactation Consultant visits on breastfeeding satisfaction.
Keywords
Key Messages
The influence of the COVID-19 pandemic on exclusive breastfeeding rates and breastfeeding satisfaction in the United States is unknown.
While respondents who gave birth during the pandemic were no less likely to exclusively breastfeed for 6 months compared to those who gave birth in the year prior, they were much less likely to report high levels of breastfeeding satisfaction.
The strongest contributor to high breastfeeding satisfaction overall was a prenatal visit with an International Board Certified Lactation Consultant.
A society’s exclusive breastfeeding rate—the proportion of infants fed only human milk with nothing else given except medications or vitamins up to a designated age—is a measure of its success in supporting parents to establish and maintain breastfeeding. Due to its many benefits, 6 months of exclusive breastfeeding is a public health goal in many areas of the world (Centers for Disease Control and Prevention [CDC], 2021; World Health Organization [WHO], 2019). From 2015 to 2020, only 44% of infants aged 0–6 months were exclusively breastfed worldwide, and in the United States, only 25.6% of infants born in 2017 were exclusively breastfed for 6 months (CDC, 2020; WHO, 2020). The Healthy People 2030 goal for 6 months of exclusive breastfeeding in the United States is 42.4% of infants, a 66% increase from 2017 data (Office of Disease Prevention and Health Promotion [ODPHP], 2020).
Multiple factors, like parity, separation, intention to work outside the home, and breastfeeding education, contribute to the likelihood of breastfeeding (Cohen et al., 2018; Moimaz et al., 2017; Thomas-Jackson et al., 2016). Because previous maternal satisfaction with breastfeeding is related to the likelihood of breastfeeding subsequent infants, breastfeeding satisfaction during the COVID-19 pandemic has the potential to affect future breastfeeding rates and may affect the United States’ attainment of the Healthy People 2030 exclusive breastfeeding goal (Moimaz et al., 2017; ODPHP, 2020). On an individual level, breastfeeding satisfaction is a factor in the integration of breastfeeding into maternal identity and promotes maternal well-being and bonding (Avilla et al., 2020; Edwards, 2018; Kuswara et al., 2021). The effects of the COVID-19 pandemic on breastfeeding exclusivity and satisfaction are largely unknown. This study contributes to the growing body of knowledge surrounding COVID-19 and breastfeeding.
The COVID-19 pandemic changed the breastfeeding experience of families worldwide (Figure 1). Across the United States, hospitals largely limited the birthing parent to one support person with no other visitors. Having visitors is a barrier to skin-to-skin contact, an important facilitator of frequent and exclusive breastfeeding following birth that has also been linked to increased breastfeeding satisfaction (Alenchery et al., 2018; Hongo et al., 2015; Linares et al., 2017; Singh et al., 2017). Visitor restrictions may have facilitated a decrease in early supplementation, as successful breastfeeding initiation is more likely with frequent skin-to-skin contact (Lau et al., 2018).
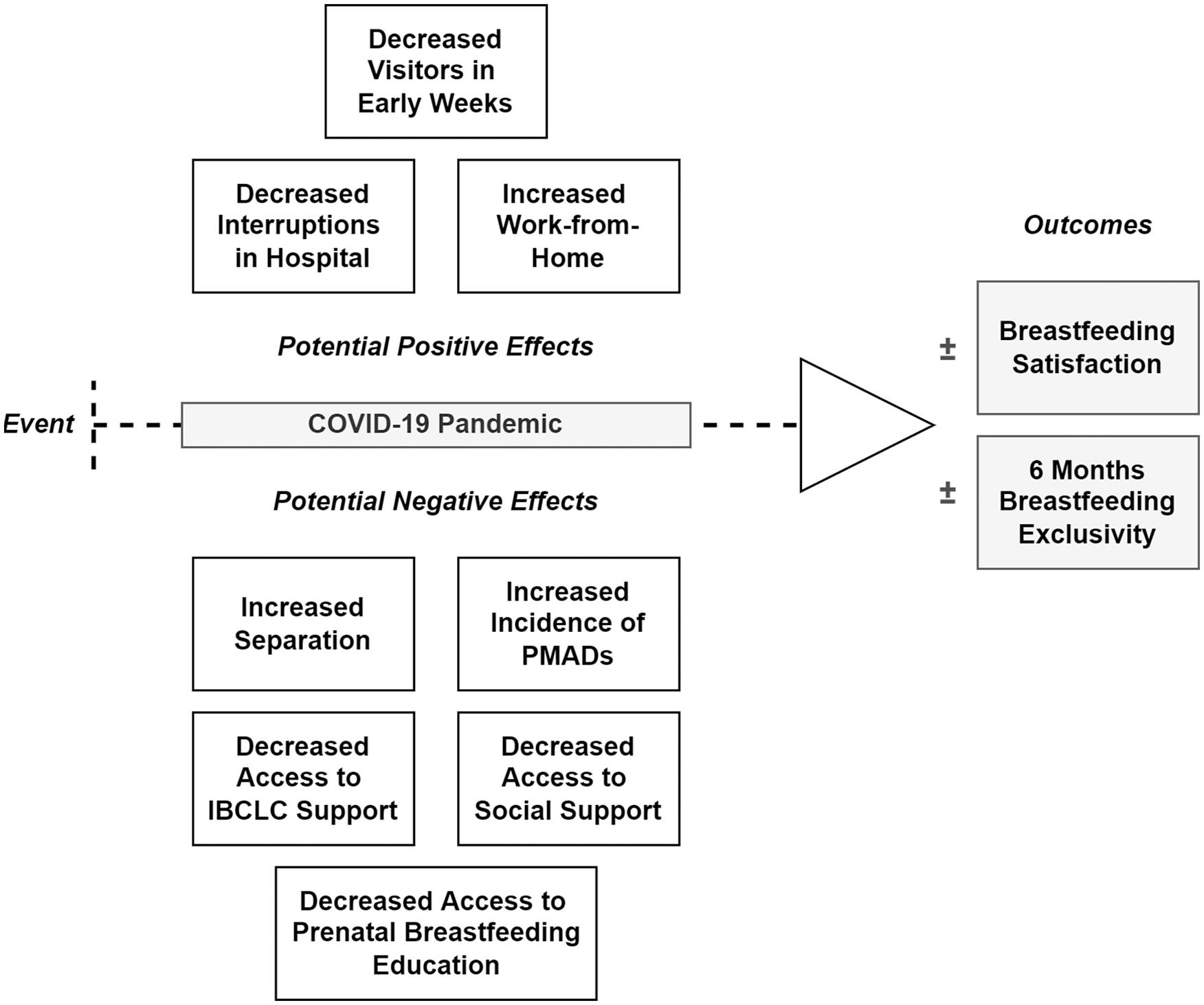
Process of Changes Related to COVID-19 Pandemic Influencing Breastfeeding Exclusivity and Satisfaction.
To reduce personal protective equipment use, staff minimized the number of times they entered patient rooms; consequently, interruptions may have been reduced (Grimm, 2020). Reducing interruptions by hospital staff gives families more continuous time with their infants, increases the percent of breastfeeding infants, and increases exclusive breastfeeding rates (Grassley et al., 2018; Lawrie et al., 2021).
Additionally, in the United States, breastfeeding parents commonly return to work 6–12 weeks postpartum, relying on breast pumps to express milk. By working from home during the pandemic, parents avoided workplace barriers, like a lack of private space and insufficient break time, potentially increasing breastfeeding exclusivity (Burns & Triandafilidis, 2019; Snyder et al., 2018).
Conversely, parent–infant separation due to COVID-19 infection decreased exclusive breastfeeding in the first 3 months (Bartick et al., 2021). Distancing the mother and infant precluded the proximity of the dyad that facilitates breastfeeding, thereby reducing rates of exclusivity (Patterson et al., 2019; Ward et al., 2017).
Breastfeeding exclusivity rates are significantly higher when families have access to lactation support before hospital discharge (Bonuck et al., 2005; Castrucci et al., 2006). Decreased contact with staff during the pandemic may have reduced the breastfeeding support that families received from International Board Certified Lactation Consultants (IBCLCs) and other staff.
Visitor restrictions may have also limited new parents’ support from relatives or friends with breastfeeding experience. Lack of family help was identified as a significant risk factor for decreased exclusivity of breastfeeding in Thailand during the COVID-19 pandemic and may have had a similar effect in the United States (Piankusol et al., 2021). Additionally, parents may have been unwilling to have breastfeeding-knowledgeable friends or family members in their homes due to fear of contracting COVID-19.
Out of concern for safety, parents may not have sought in-person assistance from an IBCLC. Likewise, an unknown percentage of community-based IBCLCs opted for virtual visits over in-person appointments. Although previous researchers have shown high satisfaction with lactation support provided via telehealth, no researchers have examined differences in breastfeeding exclusivity or satisfaction among participants who received lactation support via telehealth (Oggero et al., 2021; Uscher-Pines et al., 2020).
Awaliyah et al. (2019) found that a major factor in breastfeeding satisfaction was breastfeeding self-efficacy, which can be enhanced by prenatal breastfeeding education (Chan et al., 2016; Noel-Weiss, 2006). Prenatal breastfeeding education also was associated with increased rates of exclusive breastfeeding. Access to prenatal breastfeeding education and types of education offered may have been affected by changes during the COVID-19 pandemic.
Symptoms of perinatal mood and anxiety disorders (PMADs), particularly those related to anxiety, may have led to decreased breastfeeding satisfaction and exclusivity among new parents during the pandemic (Avilla et al., 2020). Researchers conducting studies of the incidence of PMADs related to isolation and social restrictions during the COVID-19 pandemic have yielded mixed results; however, anxiety appears to be significantly more common than depression (Wu et al., 2020; Zanardo et al., 2020).
Bartick et al. (2021) found a significant difference in breastfeeding exclusivity at 3 months between mothers with COVID-19 who were separated from their infants and those who were not. However, researchers have not compared breastfeeding exclusivity between those who gave birth before versus during the COVID-19 pandemic. Additionally, to our knowledge, no one has compared breastfeeding satisfaction among parents of infants born before and during the COVID-19 pandemic. Understanding the relationship of pandemic-related changes to breastfeeding exclusivity and satisfaction is important for policy development in case of ongoing or future widespread communicable illness. Therefore, the aim of this study was to examine the differences in breastfeeding exclusivity and satisfaction before and during the COVID-19 pandemic.
Method
Research Design
This study was conducted using a prospective, cross-sectional design with two-group comparison. The Committee for the Protection of Human Subjects at The University of Texas Health Science Center at Houston (UTHealth) granted Institutional Review Board exemption before data collection commenced.
Setting and Relevant Context
The setting was a breastfeeding clinic located in Houston, Texas, and affiliated with a nearby medical school’s department of pediatrics. The clinic is co-funded via a Title V Maternal/Infant Health grant and the Texas Women, Infants, and Children (WIC) Supplemental Nutrition Program. All clinic services are free, regardless of income or WIC participation. The clinic is also a lactation training facility for medical residents, other healthcare professionals, and WIC staff. The clinic providers are IBCLCs who conduct approximately 1,800 in-person visits annually. Additional services include telehealth visits, phone counseling, classes, and a weekly support group.
Eligible participants resided in Houston and surrounding communities when they received services. Houston is the fourth-largest city and one of the most ethnically diverse areas in the United States (City of Houston, 2020). The Greater Houston metropolitan area, comprised of Houston itself and numerous suburban communities, has a total population of nearly 7 million people (Greater Houston Partnership, 2019).
According to the CDC’s (2020) most recent Breastfeeding Report Card, only 23.9% of babies in Texas are exclusively breastfed for 6 months. This rate is similar to the national rate of 25.6%. Texas did not achieve the Healthy People 2020 goal of 25.5% of infants exclusively breastfed for 6 months and is ranked 34th of 50 states in exclusive breastfeeding rates (CDC, 2020).
Currently, there are approximately 35 hospitals with maternity services within a 75 km radius of central Houston (Texas Department of State Health Services, 2022). Of these, 10 are designated as Baby-Friendly (Baby-Friendly USA, 2022). Additionally, there are over 1,200 IBCLCs in the state of Texas (International Board of Lactation Consultant Examiners, 2019). As in many other major cities in the United States, Houston-area IBCLCs routinely serve patients in the hospital and in community settings through clinic-based visits, home visits, and at local WIC agencies. During the pandemic’s early months in Houston, many community-based IBCLCs limited or stopped in-person visits, WIC agencies were closed to clients, and in-person breastfeeding support groups were not meeting.
Sample
The target population was all postpartum patients seen at the clinic with infants born from April 1 to December 31 in both 2019 and 2020. Infants born from January 1 to March 31 of 2020 were excluded, as this was a time of transition while COVID-19 cases emerged in the Houston area. Respondents were excluded if they did not have an infant born in the selected time period, were younger than 18 years, or if the infant was born prior to 37 weeks gestation, from a multiple gestation, or admitted to the neonatal intensive care unit (NICU; except if only to separate the infant from a COVID-positive or suspected positive parent).
A total of 1,241 patients were eligible to receive an invitation to complete an online survey in English (Figure 2). Five patients did not provide an email address, resulting in 1,236 patients who were invited to participate. With a target sample size of 150, a logistic regression model would have 80% power when the effect size for a categorical independent variable is an odds ratio (OR) = 2.83. This is equivalent to those with a characteristic having 2.83 times the odds of achieving the outcome of interest (e.g., exclusive breastfeeding to 6 months of age or high breastfeeding satisfaction).
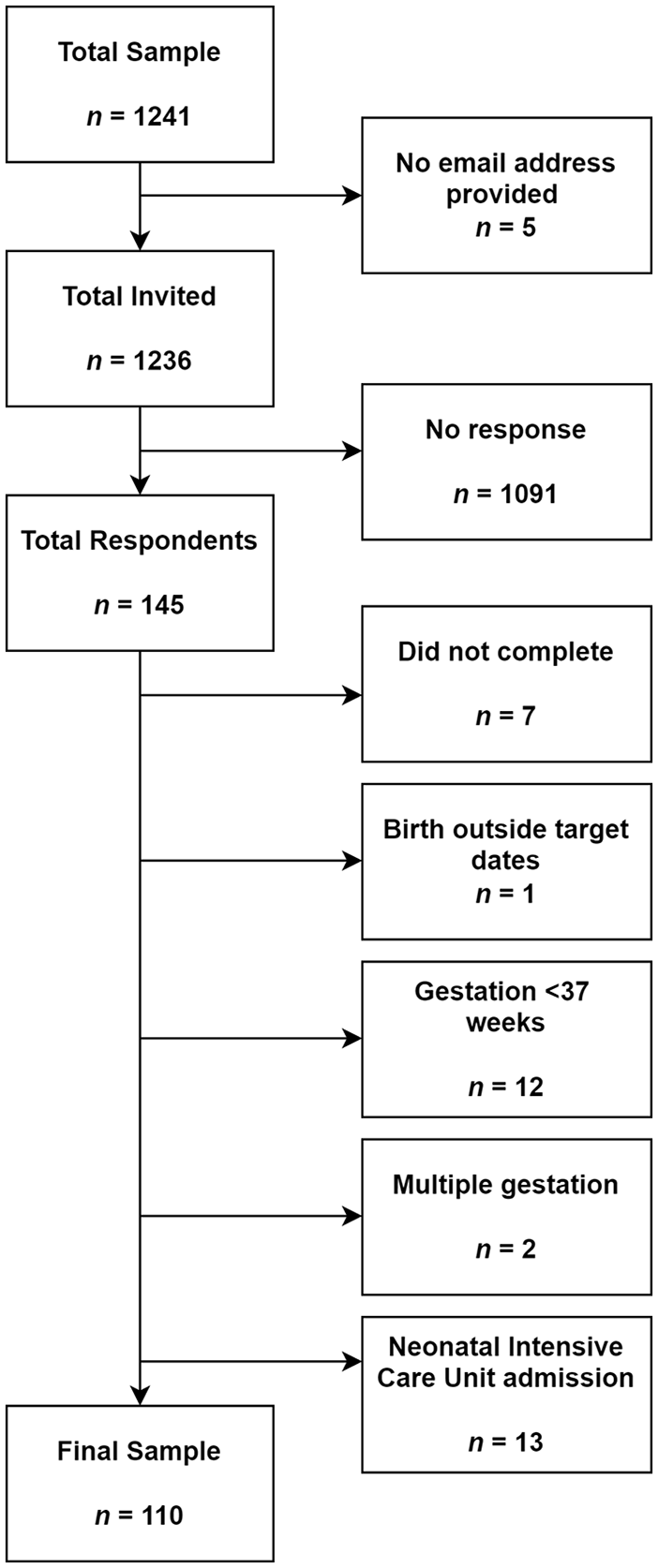
Sample Selection Diagram.
Of 145 respondents who attempted the survey (11.7% response rate), 35 were excluded: one due to birth occurring outside of the target dates, 12 due to gestation less than 37 weeks, two due to multiple gestation, 13 due to NICU admission, and seven who began but did not complete the survey. The total number of completed, eligible surveys was 110. Although the targeted sample size was not met, the resulting sample was sufficient to detect large effects.
Measurement
Dependent Variables
Exclusive breastfeeding at 6 months was assessed using three survey items about the timing of infant feeding practices (see Supplementary Materials). Respondents were not considered to have exclusively breastfed for 6 months if their infant received any formula while in the hospital following birth or received infant formula, water, liquids (other than human milk or medicine), and/or solid foods in the first 6 months of life. Respondents who indicated that none of the aforementioned items were fed in the first 6 months were asked how old their infant was (in months) when first fed anything other than human milk or medications/vitamins. Any respondent who answered less than 6 months was not considered exclusively breastfeeding at 6 months.
Breastfeeding satisfaction was measured by a single item, which asked: “How would you rate your overall breastfeeding experience?” The responses ranged from 0 (“absolutely awful”) to 10 (“absolutely wonderful”). For the purposes of analysis, the variable was dichotomized so that scores of 8, 9, and 10 (the top quarter of possible scores) indicated high levels of satisfaction, and scores of 0–7 did not.
Independent Variable
The primary independent variable was year of birth for determining exposure to the pandemic. Infants born April 1, 2019, to December 31, 2019, were already at least several months old when pandemic-related changes began to occur in the Houston area. Infants born April 1, 2020, to December 31, 2020, were born during the initial three waves of the COVID-19 pandemic and experienced many changes designed to limit the spread of disease.
Covariates
Several covariates were selected based on their previously reported associations with breastfeeding exclusivity and satisfaction, including maternal age, race, and ethnicity (Xiang et al., 2019). Other variables included birth location and firstborn status (Buckman et al., 2020; Quigley et al., 2016). Gestation at birth was included as a combination of weeks and days (Noble et al., 2019). Additional questions ascertained the infant’s age in weeks at the first lactation clinic visit and WIC enrollment status at the time of any of their lactation clinic appointments (Bookhart et al., 2021).
Respondents were asked to indicate any prenatal education they received from the following options: in-person class, online class, books, online research, consultation with a non-IBCLC healthcare professional, information from a WIC peer counselor or WIC class, and prenatal breastfeeding visit with an IBCLC (Dueñas-Espín et al., 2021). They were also asked to indicate any breastfeeding issues they experienced—for example, difficulty latching, trouble feeding due to the infant’s sleepiness, nipple pain and/or damage, low milk supply, oversupply, mastitis, plugged milk ducts, inadequate infant weight gain, or jaundice (Gianni et al., 2019). Respondents were asked if they had a positive or presumed positive COVID-19 status near their infant’s birth or at any point while breastfeeding or providing human milk (Bartick et al., 2021).
Face validity of the questionnaire was evaluated and confirmed by experts in lactation practice and nursing research. The two co-authors are academics, one a women’s healthcare nurse practitioner (WHNP) and the other a family nurse practitioner and IBCLC. One additional outside reviewer is a practicing neonatal nurse practitioner and IBCLC, and another is a WHNP and IBCLC. Minor changes were made based on their recommendations.
Data Collection
Initial survey invitations were sent by email through the Qualtrics online survey platform in late June 2021 to all eligible patients who had provided email addresses. A reminder email was sent the following week. The email included the study details and a link to the survey, which was open for 5 weeks. Documentation of consent was waived due to the anonymous nature of the survey, and all respondents viewed the study details before beginning the survey. Participants were not compensated for completing the survey. No identifying details or internet protocol addresses were collected in the survey process. Data were kept on a secure drive at the authors’ home institution, and only the authors maintained access.
Data Analysis
Data analysis was performed in JMP Pro (Version 15.2.0). All continuous variables were analyzed for a normal distribution. Bivariate analyses compared each variable by year to determine which variables were significantly different between families of infants born before and during the COVID-19 pandemic. Chi-square (variables with all counts ≥ 5) and Fisher’s exact (variables with any counts < 5) tests were used to examine differences in proportions of all categorical independent variables by year. For continuous variables, t tests for independent samples were used to examine differences in means by year. The Chi-square test was used to evaluate the difference in the proportion of respondents who reached 6 months of exclusive breastfeeding by birth year and to evaluate the difference in the proportion of respondents with high breastfeeding satisfaction by birth year. Pairwise deletion was used to exclude participants with missing data from applicable analyses (n = 3).
Additional analysis using logistic regression examined the effect of maternal and infant characteristics, birth year, breastfeeding education, and breastfeeding characteristics on the odds of high breastfeeding satisfaction. Variables related to high breastfeeding satisfaction in bivariate analyses were evaluated for inclusion in the logistic regression model using an initial p value cutoff of .25 (Bursac et al., 2008). Significance was then evaluated for each variable at the 0.1 alpha level following the initial model run, and variables above this threshold were removed from the model in order of largest p value one at a time until all remaining variables had p values less than .1. At this point, any variable not selected for the original model was added back individually to identify those that were not significantly related to high breastfeeding satisfaction alone but may have contributed to its increase or decrease in the presence of other variables. None of the originally excluded variables were significant at the 0.1 alpha level when added back to the model; therefore, no additional variables were retained. The final logistic regression model resulted. Variance inflation factor values were used to assess for multicollinearity. None of the variables included in the final model had missing values.
Results
Characteristics of the Sample
The characteristics of the pre-pandemic and pandemic groups were similar (Tables 1 and 2). The age distribution and racial and ethnic breakdown of the sample reflected the clinic’s general patient population. None of our participants reported being COVID-positive or presumed positive near the time of birth. Only one participant reported testing positive while breastfeeding and indicated that she was neither advised nor chose to stop breastfeeding or change her feeding practices as a result.
Characteristics of the Sample Grouped by Year: Continuous Variables (N = 110).
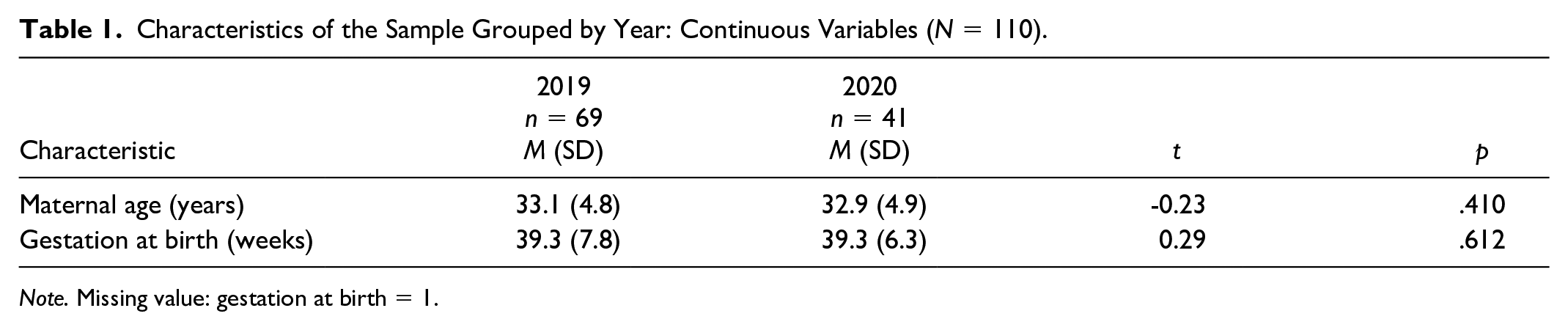
Note. Missing value: gestation at birth = 1.
Characteristics of the Sample Grouped by Year: Categorical Variables (N = 110).
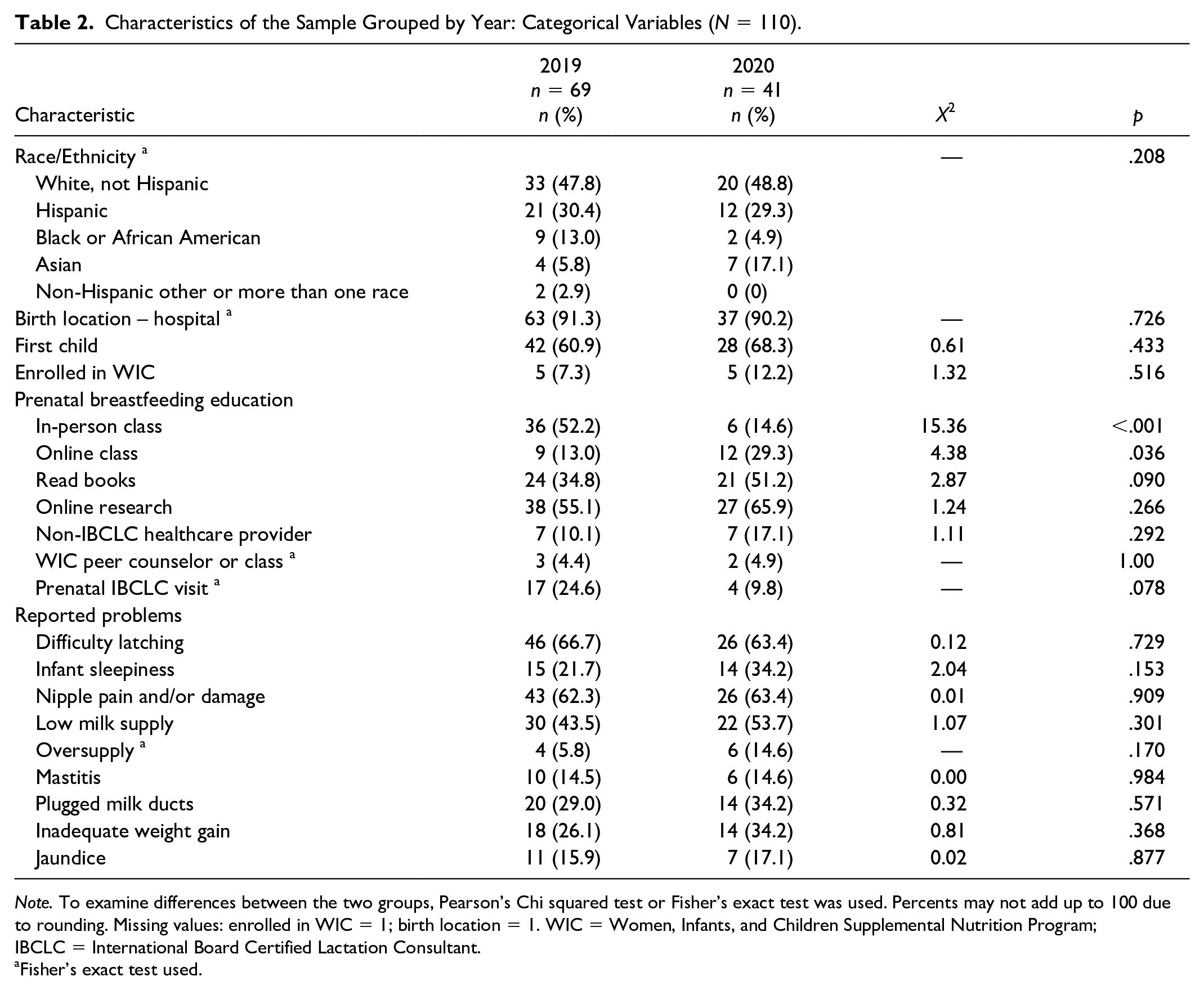
Note. To examine differences between the two groups, Pearson’s Chi squared test or Fisher’s exact test was used. Percents may not add up to 100 due to rounding. Missing values: enrolled in WIC = 1; birth location = 1. WIC = Women, Infants, and Children Supplemental Nutrition Program; IBCLC = International Board Certified Lactation Consultant.
Fisher’s exact test used.
Difference in Breastfeeding Exclusivity
Respondents (n = 41) who gave birth in 2020 were no less likely than those who gave birth in 2019 (n = 69) to exclusively breastfeed for the first 6 months (Table 3).
Comparison of Exclusive Breastfeeding for 6 Months by Year (N = 110).
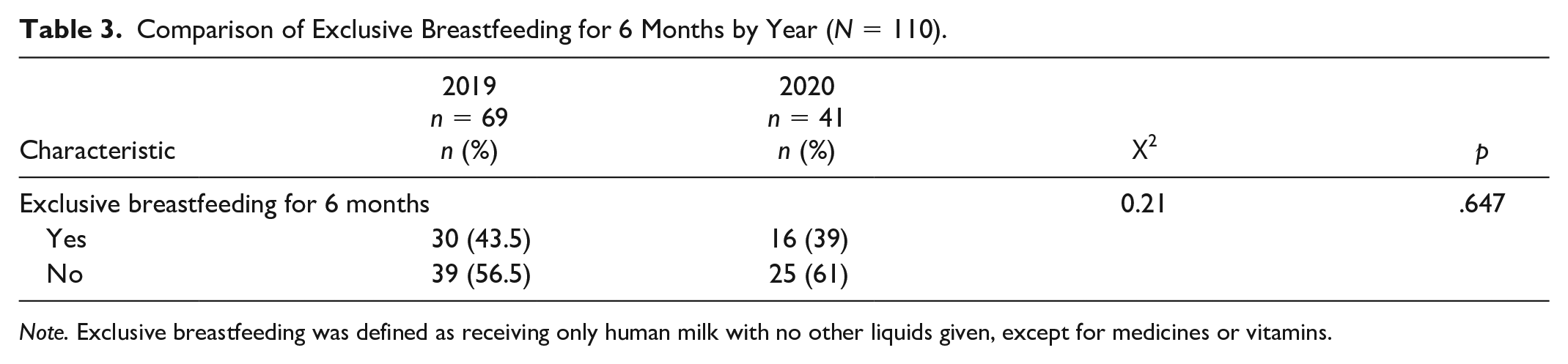
Note. Exclusive breastfeeding was defined as receiving only human milk with no other liquids given, except for medicines or vitamins.
Difference in Breastfeeding Satisfaction
Respondents who gave birth during the pandemic were significantly less likely than those who gave birth pre-pandemic to report high breastfeeding satisfaction (Table 4). After multivariable logistic regression including several covariates, the odds of high breastfeeding satisfaction were 73% lower in respondents with infants born in 2020 than in respondents with infants born in 2019 (OR = 0.27, 95% CI [0.08, 0.89]; Table 5). The log-likelihood Χ2 statistic for this model was 65.32 (p < .0001). Variance inflation factor values for applicable variables were all less than 1.2, ruling out problems associated with multicollinearity.
Comparison of Highly Positive Breastfeeding Experience by Year (N = 110).
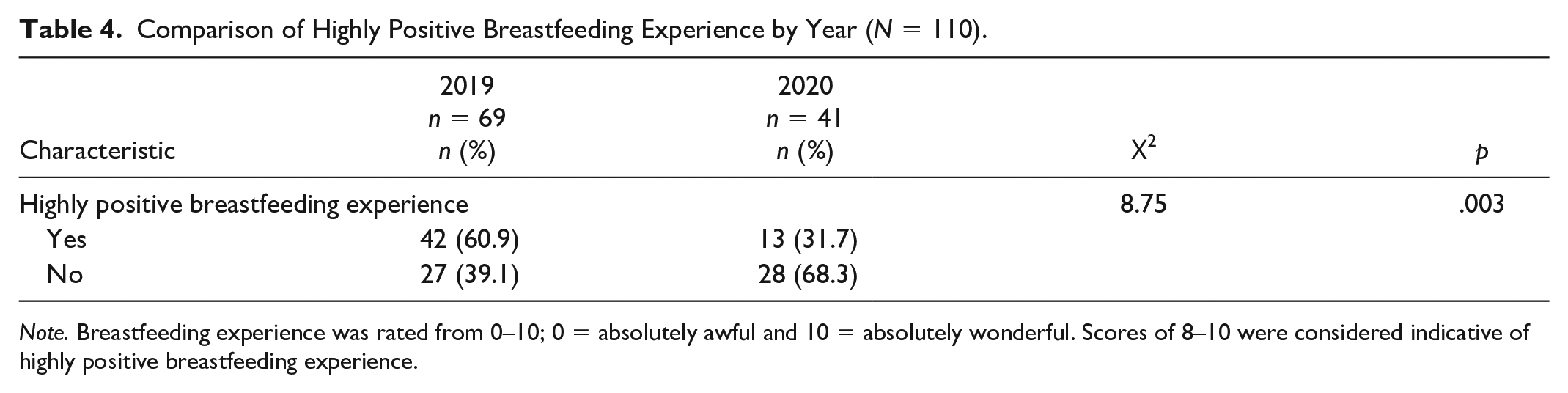
Note. Breastfeeding experience was rated from 0–10; 0 = absolutely awful and 10 = absolutely wonderful. Scores of 8–10 were considered indicative of highly positive breastfeeding experience.
Odds Ratios for Highly Positive Breastfeeding Experience Using Logistic Regression (N = 110).
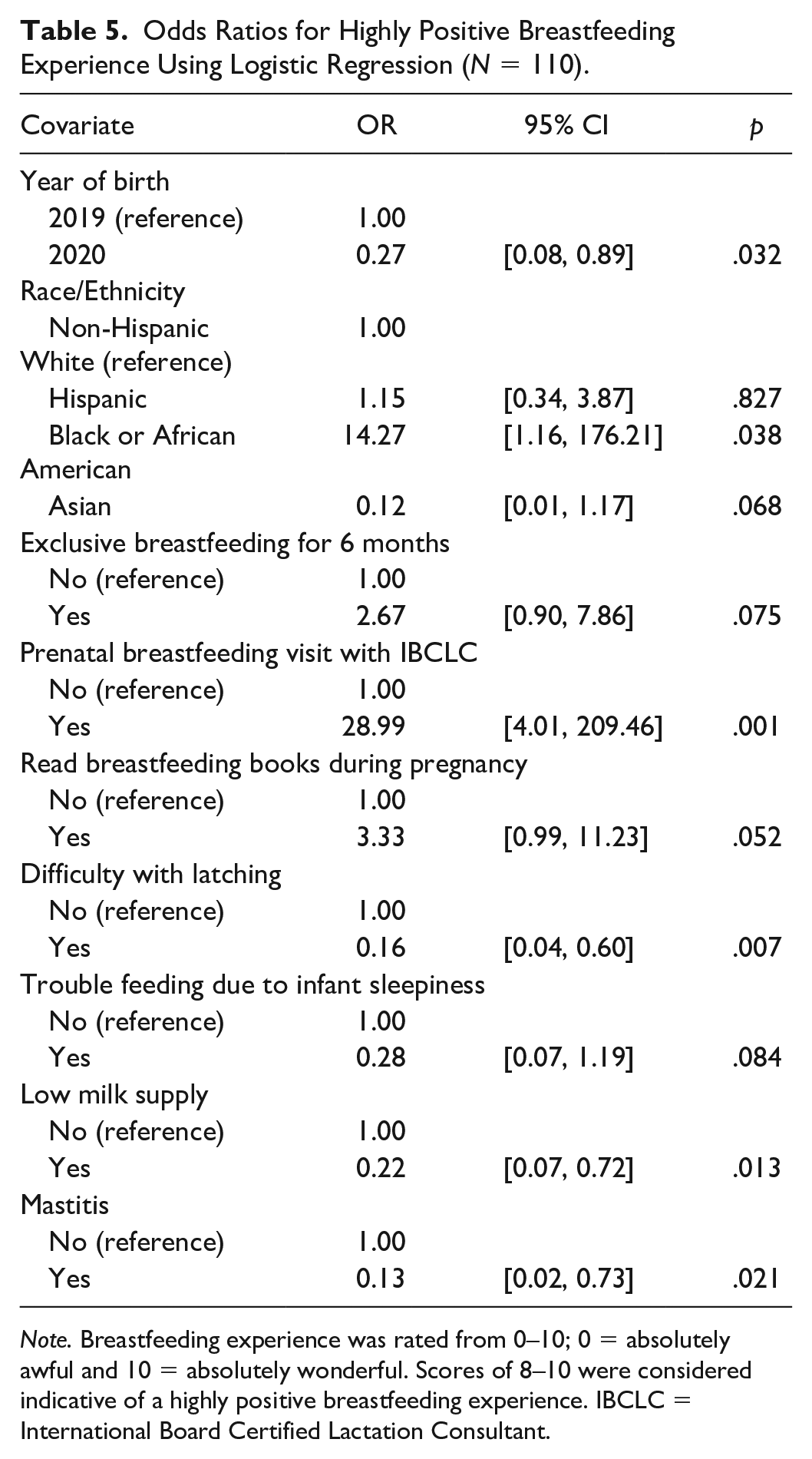
Note. Breastfeeding experience was rated from 0–10; 0 = absolutely awful and 10 = absolutely wonderful. Scores of 8–10 were considered indicative of a highly positive breastfeeding experience. IBCLC = International Board Certified Lactation Consultant.
The most significant contributor to high breastfeeding satisfaction in this model was a prenatal breastfeeding visit with an IBCLC. The odds of high breastfeeding satisfaction were 29 times higher in those who had a prenatal IBCLC visit than in those who did not (OR = 29.0, 95% CI [4.01, 209.47]). The odds of high breastfeeding satisfaction were 84% lower in those who experienced difficulty latching (OR = 0.16, 95% CI [0.04, 0.60]). The odds of high breastfeeding satisfaction were 78% and 87% lower in respondents reporting low milk supply or mastitis, respectively (OR = 0.22, 95% CI [0.07, 0.72]; OR = 0.13, 95% CI [0.02, 0.73]). While Black/African American parents appear to have higher odds of high breastfeeding satisfaction in this model (OR = 14.3, 95% CI [1.16, 176.2]), this result should be interpreted with caution given the small group size.
Discussion
Our results provide preliminary evidence of the influence of the COVID-19 pandemic on breastfeeding exclusivity and satisfaction. While respondents who gave birth during the COVID-19 pandemic were no less likely to exclusively breastfeed for 6 months than respondents who gave birth pre-pandemic, a small but significant difference might be detectable with a larger sample; therefore, further research is recommended. However, the finding that breastfeeding exclusivity was not drastically affected by COVID-related changes in this sample remains reassuring.
Despite the lack of difference in breastfeeding exclusivity, the odds of high breastfeeding satisfaction were much lower in those who gave birth during the pandemic than in those who gave birth pre-pandemic. Decreased access to social support and heightened anxiety related to the fear and uncertainty of a worldwide health crisis likely contributed, at least partially, to this difference. Limited support from hospital staff and community-based IBCLCs may have also played a role. Further research is needed to identify the specific factors that led to this difference in breastfeeding satisfaction.
The most significant contributor to high breastfeeding satisfaction was having a prenatal breastfeeding visit with an IBCLC. Although this finding should be interpreted cautiously owing to the lack of precision related to the small sample, even the low end of the CI predicted that the odds were at least four times higher in those with a prenatal IBCLC visit. Although prior research has examined various breastfeeding education interventions and their impact on breastfeeding exclusivity and satisfaction, little research focused on the impact of prenatal IBCLC visits on breastfeeding satisfaction. In this study, several types of prenatal education, including in-person and/or online classes, self-education by reading books and/or researching online, and education received from a non-IBCLC healthcare professional and/or a WIC peer counselor were included, but only the prenatal IBCLC visit was significantly associated with breastfeeding satisfaction. Future research should explore this relationship to verify and expand upon this study’s finding.
Strengths of this study include its setting in a major metropolitan area with a diverse population. Additionally, including only full-term infants who were not from a multiple pregnancy or admitted to the NICU reduced the impact of the related stressors accompanying premature, multiple infants, and/or NICU admission on breastfeeding exclusivity and satisfaction, although future research is recommended in these areas as well. With a wide initial selection of potential variables, the iteratively constructed multivariable logistic regression model subsequently focused on the variables that most strongly impacted breastfeeding satisfaction in this sample and ultimately highlighted the potential impact of prenatal IBCLC visits on the mitigation of pandemic-related changes.
Limitations
The primary limitation of this study is its relatively small sample size. The total sample of 110 respondents did not meet the original goal of 150 respondents, resulting in lower power than anticipated, increasing potential for Type II errors, and decreasing the likelihood of detecting small but significant effects. With only 69 respondents in the pre-pandemic group and 41 in the pandemic group, an actual difference in breastfeeding exclusivity could have been undetected. The small sample size also contributed to reduced precision of the estimates based on the somewhat wide 95% CIs for the ORs.
Potential non-response bias is another limitation, as the extent to which those who did and did not respond differed is not known. The population from which this sample resulted, patients of an urban, academic breastfeeding clinic in the United States, may not be widely generalizable, although the diversity of the Houston area may mitigate this to some extent. Additional limitations include the measurement of breastfeeding satisfaction with a single question rather than an established scale and the unknown effects of recall bias on the answers given by the pre-pandemic participants.
Additionally, each prenatal IBCLC visit was conducted to meet the individual patient’s needs and was not standardized, although covered content is largely the same for each patient. This factor precludes identifying particular characteristics of the visit that may be especially impactful. Further research aimed at identifying these characteristics could benefit future practice.
Conclusions
While breastfeeding exclusivity was not significantly different between infants born during the COVID-19 pandemic and infants born pre-pandemic, the odds of high breastfeeding satisfaction were significantly lower for parents of infants born during the pandemic. Additionally, having a prenatal breastfeeding visit with an IBCLC was the most significant contributor to high breastfeeding satisfaction. Future research is needed to identify the specific pandemic-related factors that led to the difference in breastfeeding satisfaction between the two groups and to confirm the impact of prenatal IBCLC visits on breastfeeding satisfaction.
Supplemental Material
sj-pdf-1-jhl-10.1177_08903344221086974 – Supplemental material for Changes in Breastfeeding Exclusivity and Satisfaction During the COVID-19 Pandemic
Supplemental material, sj-pdf-1-jhl-10.1177_08903344221086974 for Changes in Breastfeeding Exclusivity and Satisfaction During the COVID-19 Pandemic by Megan K. Oggero and Diane W. Wardell in Journal of Human Lactation
Footnotes
Acknowledgements
Special thanks to Stanley Cron, MSPH of the Cizik School of Nursing at UTHealth for statistical consultation.
Author contribution(s)
Disclosures and Conflicts of Interest
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Megan Oggero completed this student research, and Diane Wardell was the faculty advisor on this project.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplementary Material may be found in the “Supplemental material” tab in the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.