
Abstract
Background:
Human colostrum has been used in a number of investigations when preterm human infants cannot, for any reason, breastfeed directly from their mothers. One of the growing fields in these investigations is colostrum therapy, which consists of exposing the oropharyngeal mucosa of these preterm newborns to small amounts of raw colostrum.
Research Aim:
To critically review the scientific evidence about colostrum therapy in premature infants and to explore its influences on the immune system.
Methods:
This systematic review was performed according to the preferred reporting items for systematic reviews and meta-analyses (PRISMA statement). The following databases were searched for potentially eligible studies up to March 10, 2021: Medline, Scopus, Web of Science, Cochrane Library, Embase. Two reviewers independently screened all titles, abstracts, and full texts for eligibility.
Results:
A total of 12 studies with 996 participants were included. A significant difference in lactoferrin levels in the urine was found (SMD 0.70; 95% CI [0.03,1.36]; p = .04; I² = 65% two studies, 112 participants, very low-quality evidence).
Conclusion:
Colostrum seems to result in increasing lactoferrin levels in the urine of premature newborns after 1 week of intervention.
Clinical Trial Registration:
The study was registered at PROSPERO with the number CRD42017073624, submitted on August 9, 2017.
Keywords
Key Messages
Breastfeeding is very important for the development of the newborn, including strengthening the immune system.
Despite the scarcity of evidence about colostrum therapy and its influence on the immune system of premature newborns, our findings do point in the direction of benefits for those who receive colostrum.
This systematic review is important because it synthesized the current published data in this area, helping in the decision-making process and planning of future studies about colostrum therapy for premature newborns.
Background
Preterm delivery is defined as babies born alive before 37 weeks of pregnancy. There are sub-categories of preterm birth, based on gestational age: (1) extremely preterm (less than 28 weeks), (2) very preterm (28–32 weeks), and moderate to late preterm (32–37 weeks; World Health Organization [WHO], 2018). Although immune systems of all infants are immature at birth, premature infants are particularly vulnerable to disease due to the immaturity of nearly all organ systems. Prematurity causes 70% of neonatal deaths, 36% of child deaths, and represents about 25% of neurological problems that affect children in the long term (Di Renzo et al., 2017). About 15 million premature births occur each year (5%–18% of all deliveries) and, globally, preterm birth and its complications are the most common cause of death among children less than 5 years (Chawanpaiboon et al., 2019; WHO, 2016).
Postnatally, lactation is part of the continuum of the reproductive process as mother’s milk contains essential factors that promote the development of the neonate’s systems. Human milk provides a source of innate and passive immunity until the infant’s own immune response matures. However, prematurity may limit the infant’s suckling ability, and so colostrum may need to be administered via the oropharyngeal route (Diniz et al., 2014). Colostrotherapy is a painless and safe therapy that exposes the baby’s oropharyngeal mucosa to small amounts of raw colostrum, contributing to immune system absorption that stimulates the development of the child’s immune system (Martins et al., 2020).
Human milk is composed of macro- and micronutrients, for example: proteins, fat, carbohydrates, vitamins, and minerals. Besides that, colostrum—the first human milk secreted after birth—has bioactive components that contribute to the maturation of the infant’s immune system (Ballard et al., 2013). Among these substances, there are high levels of secretory Immunoglobulin A, lactoferrin, proinflammatory, and anti-inflammatory cytokines, besides growth factors (Martín-Álvarez et al., 2016).
When mature human milk—milk produced about 10–15 days after birth—is compared to colostrum, it is richer in antimicrobial peptides, immunoregulatory compounds and growth factors. The main functions of colostrum are to provide essential nutritional components, strengthen the natural defense system, modulate the immune response, balance the intestinal microbiota, increase growth, and repair tissues (Menchetti et al., 2016). In general, preterm newborns are more susceptible to infections since their immune system functions are immature. This can lead to worsening conditions and even systemic dissemination of infection (Collins et al., 2018). The administration of colostrum is hypothesized to improve immune markers, like IgA levels, which would lead to a healthier immune system (Martín-Álvarez et al., 2016). Thus, through a systematic review and meta-analysis, the aim of this study was to critically review the scientific evidence about colostrum therapy in premature infants and to explore the results on the immune system
Methods
Research Design
This study was a systematic review with meta-analysis, performed according to a prospective protocol using PRISMA guidelines (preferred reporting items for systematic reviews and meta-analyses; Page et al., 2021). A systematic review represents the study design with the highest level of scientific evidence.
Sample
The inclusion criteria for this review derived from the PICOS acronym, which stands for patient, intervention, comparison, outcomes and study type. Studies were included that (1) had our target population: premature newborns with gestational age lower than 38 complete weeks, admitted to the neonatal intensive care unit (NICU); (2) used any administration of colostrum as intervention; (3) compared the colostrum therapy with a placebo (sterile water or saline water), formula, or standard care; (4) analyzed immune system laboratory markers; and (5) were controlled trials. The exclusion criteria were (1) uncontrolled clinical trials; (2) animal studies; and (3) mature newborns included in the population.
Two independent investigators (IF and PF) reviewed study titles and abstracts using the Rayyan software (https://www.rayyan.ai). Studies that potentially fulfilled the inclusion criteria were retrieved for full-text assessment, and were independently screened by the investigators (IF and PF) to identify studies for inclusion. Any disagreements were resolved by discussion or by referring to a third review author (AJG) when required.
Through database searching, we identified 4671 records. We did not identify any additional records through other sources. Of these, 1113 studies were excluded by duplication, leaving for reading titles and abstracts 3558 studies. We screened the titles and abstracts of these 3558 records, excluding 3518 records. We screened 40 full-text articles and excluded 28. We included 12 studies in the qualitative synthesis and seven studies in meta-analysis since they analyzed the same outcomes. The selection process of relevant studies retrieved from databases is shown in a PRISMA-compliant flowchart (Figure 1).
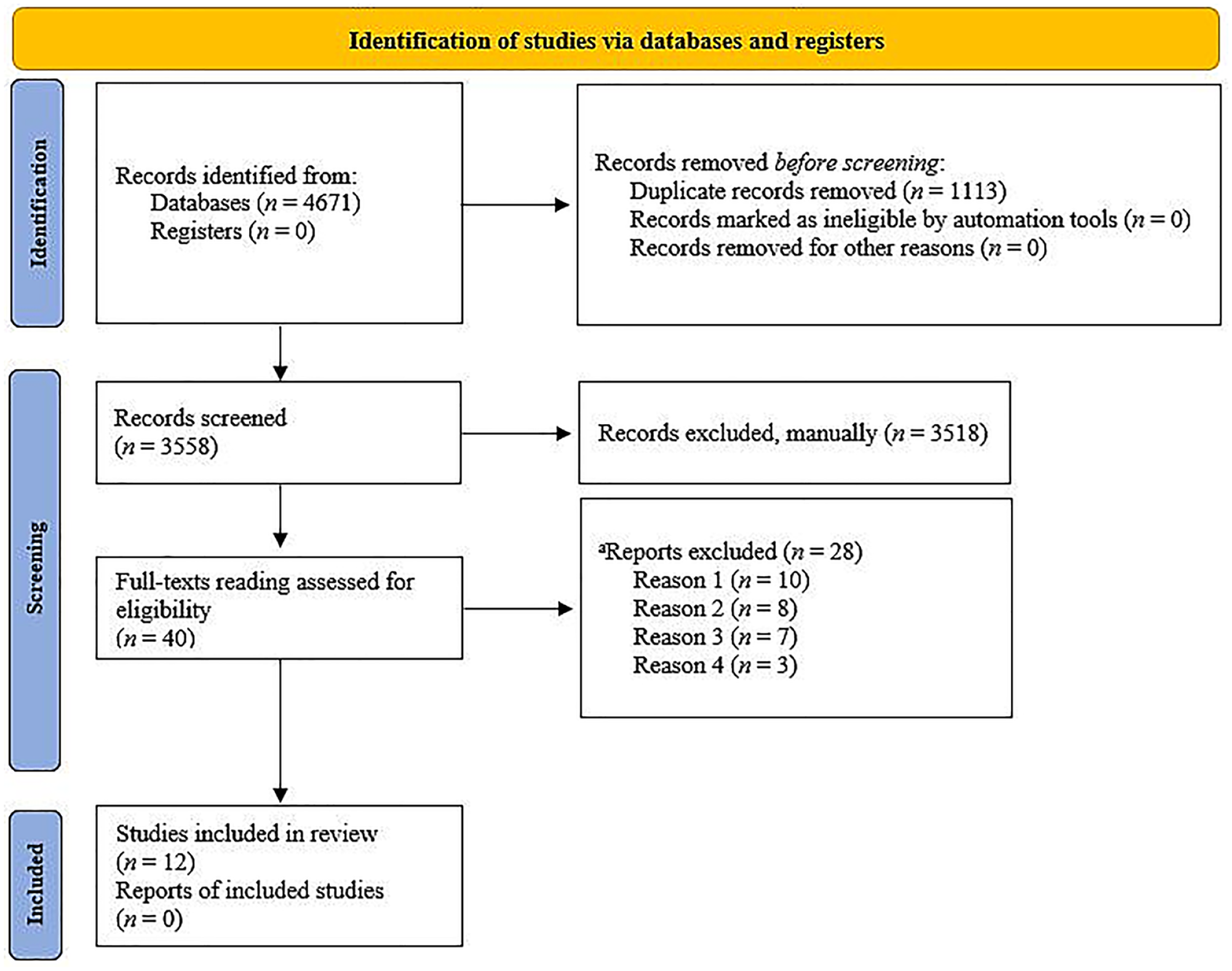
PRISMA Flow Chart: Selection Process of Relevant Studies Retrieved From Databases.
In our systematic review, we included 12 complete studies from the literature, but there is a study protocol for an ongoing randomized clinical trial (Rodriguez et al., 2015) on the oropharyngeal administration of the mother’s colostrum and the influence on the health of premature babies, with a 5-year analysis, has not been published. In addition to this, four more studies are underway in several countries on this topic, but at the time of writing there were no partial results released.
Measurement
The processes for data extraction of the included studies were performed by two reviewers (IF and PF), independently and blinded. The reviewers analyzed the risk of bias and independently performed data extraction into a standardized form, prepared by the authors and standardized for all studies, with the following titles: Study type, participant characteristics, information demographics, type, and time of intervention and placebo. After they were obtained, the data were compared and, when there was a conflict, the studies were again analyzed, and a third reviewer (AJG) gave his opinion. When the information was not obtained, the authors were contacted by email.
To assess the risk of bias, we used the Cochrane Collaboration’s Tool for Assessing the Risk of Bias in Randomized Trials (RoB 2; Higgins et al., 2011). To grade the quality of evidence, we used the Grades of Recommendation, Assessment, Development, and Evaluation (GRADE) approach (Iorio et al., 2015; Yang et al., 2017; Supplementary Table 2). The variables defined for study comparison are specified in Table 2, as well as the methodologies used for the dosage.
Data Collection
The following databases were searched from their inception up to March 10, 2021, for potentially eligible studies without language restrictions: Medline, Scopus, Web of Science, Cochrane Library, Embase. We also manually checked all references from the included studies for other studies to include. A search strategy was developed (Supplementary Table 1). We also performed searches for unpublished, ongoing trials and grey literature using the System for Information on Grey Literature in Europe (SIGLE), Google Scholar, and the International Clinical Trials Registry Platform. Before completing this review, we performed an additional search of each database and registration platform to guarantee that the most recent studies were included.
Data Analysis
The primary outcomes analyzed were salivary IgA levels and IgA urine levels. The secondary outcomes analyzed were lactoferrin urine levels post-intervention; lactoferrin urine levels after 1 week; sepsis positive culture and suspected clinical sepsis (Table 2). The descriptive analysis of the included studies was carried out in a narrative form, in which the data from the studies (for example outcomes, intervention, sample, and application) were presented in tables and in the text of the results. The data of interest presented as continuous, salivary IgA levels, IgA urine levels, lactoferrin urine levels post-intervention, and lactoferrin urine levels after 1 week (M and SD) were used to perform a meta-analysis to obtain the standardized mean difference (SMD) when standardization of data were required. For sepsis positive culture and suspected clinical sepsis, Risk Ratios (RR) and 95% confidence intervals (CI) were calculated.
The number of participants/events was calculated based on the total sample size for the colostrum and control groups. All analyses were cross-checked, and discrepancies were resolved by discussion. The results of the meta-analysis are presented in forest plots. The significant differences of the colostrum and control for all outcomes were obtained by a two-sided p value less than p < .05 and a 95% CI that did not cross 1 for RR or 0 for mean difference (mean difference or standardized mean difference).
We assessed heterogeneity using the I2 statistic to describe the percentage of variability in effect. We classified heterogeneity as: I2 = 0%–40% might not be important; 30%–60% may represent moderate heterogeneity; 50%–90% may represent substantial heterogeneity; and 75%–100% represents considerable heterogeneity.
Results
Characteristics of the Sample
The included studies were conducted in Iran (Ghaemi et al., 2014), the United States (Glass et al., 2017; McFadden, 2012; Rodriguez et al., 2011; Romano-Keeler et al., 2017; Sohn et al., 2016), Korea (Lee et al., 2015), Spain (Martín-Álvarez et al., 2016, 2020), China (Zhang et al., 2017), Egypt (Abd-Elgawad et al., 2019), and Brazil (Ferreira et al., 2019). The smallest study had 12 participants (Sohn et al., 2016), and the largest 268 (Ghaemi et al., 2014). Of the 12 studies included in this systematic review, two evaluated preterm infants less than 28 weeks of gestational age, four less than 32 weeks, one 26–34 weeks, one less than 34 weeks, and four did not specify the gestational age of the newborns. In addition, seven studies included only infants with very low body weight (VLBW, less than 1,500 g) and one study with an extremely low birth weight (ELBW, less than 1,000 g). The characteristics of included studies are summarized in Table 1. Table 1 also includes the aims and design of these studies, Table 2 the variables measured, and Table 3 the characteristics of these studies. The assessment of risk of bias is displayed in Figure 2.
Characteristics of Included Studies (N = 12).
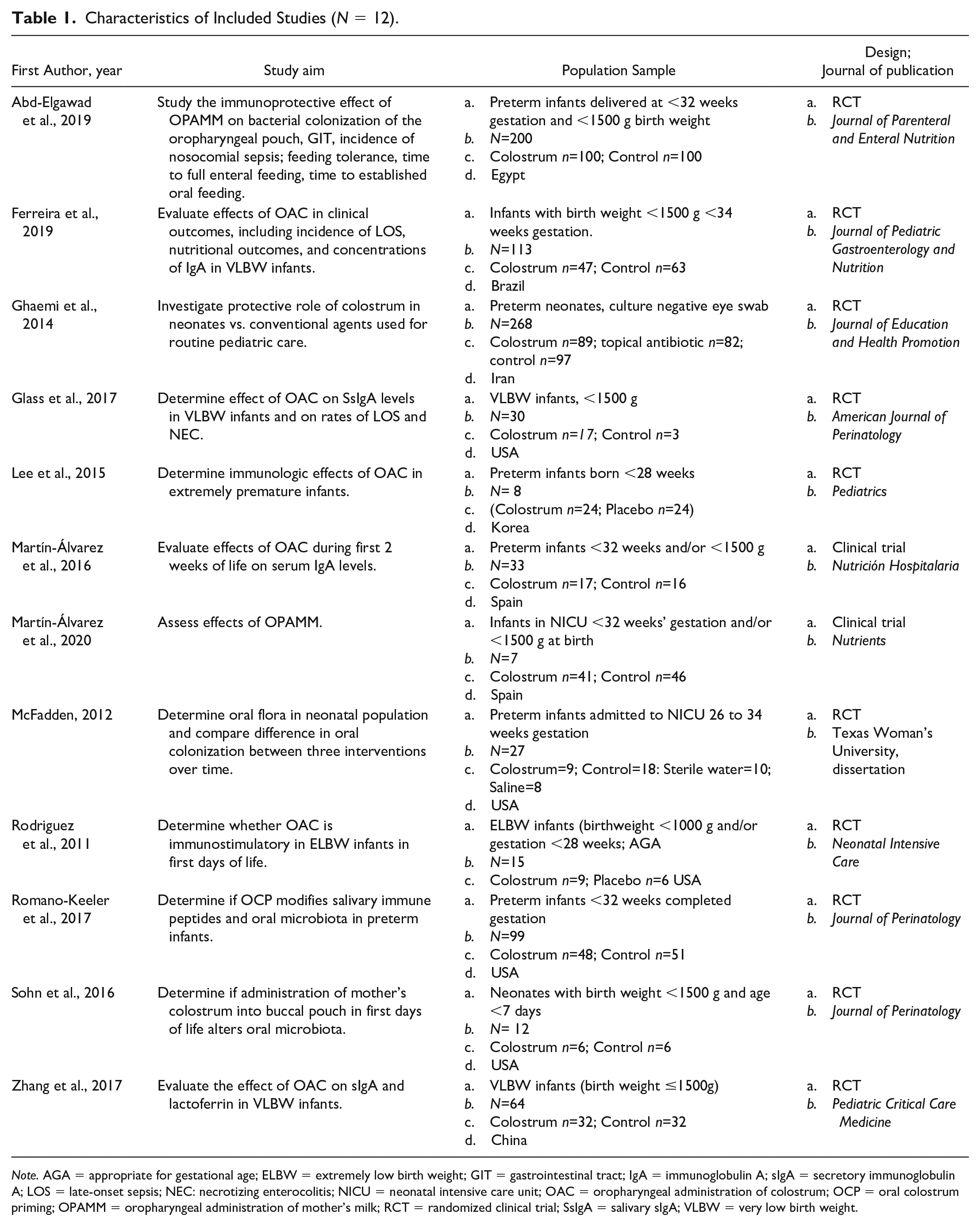
Note. AGA = appropriate for gestational age; ELBW = extremely low birth weight; GIT = gastrointestinal tract; IgA = immunoglobulin A; sIgA = secretory immunoglobulin A; LOS = late-onset sepsis; NEC: necrotizing enterocolitis; NICU = neonatal intensive care unit; OAC = oropharyngeal administration of colostrum; OCP = oral colostrum priming; OPAMM = oropharyngeal administration of mother’s milk; RCT = randomized clinical trial; SsIgA = salivary sIgA; VLBW = very low birth weight.
Variables Measured and Instruments Used, and Their Reliability and Validity in Included Studies (N = 12).
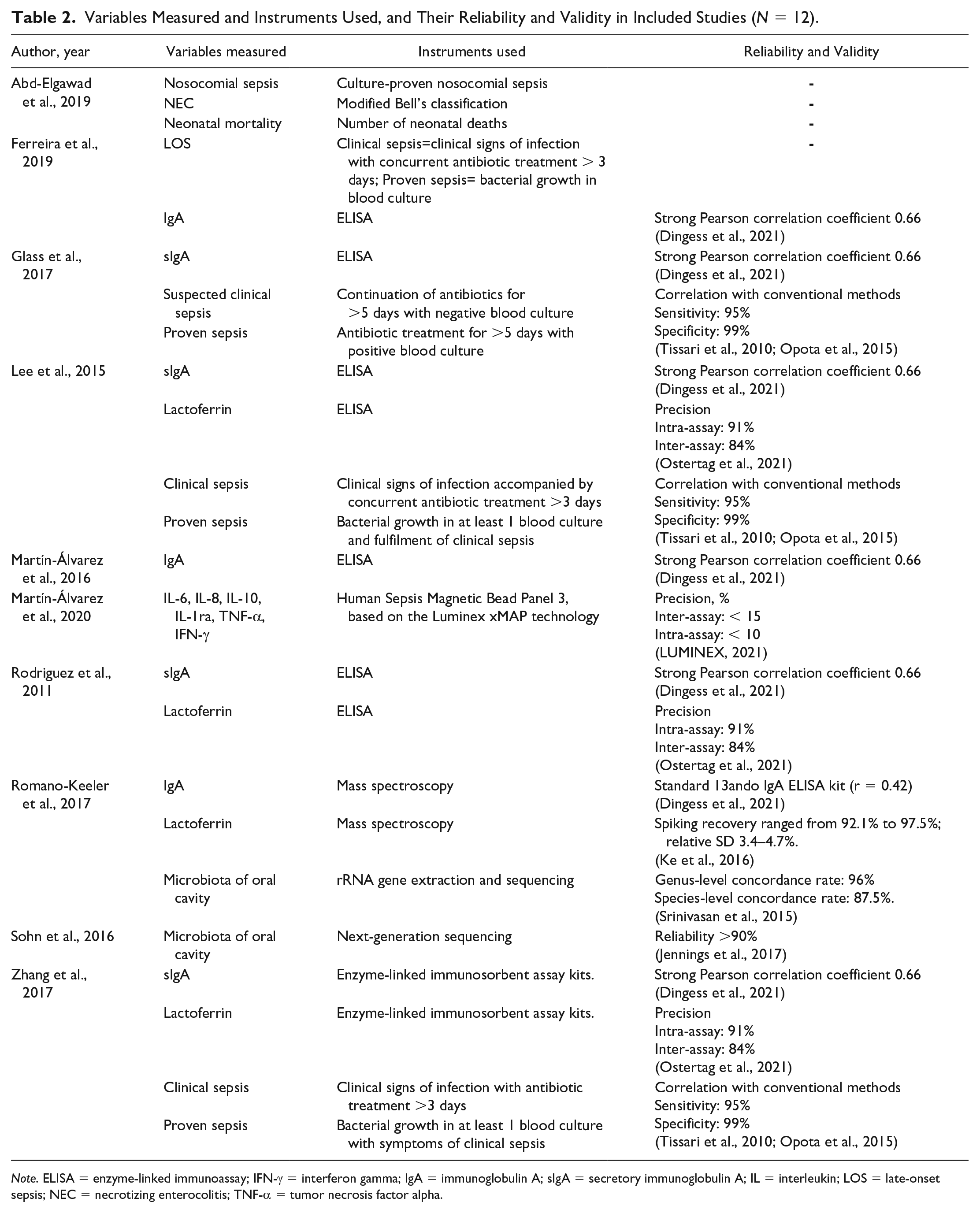
Note. ELISA = enzyme-linked immunoassay; IFN-γ = interferon gamma; IgA = immunoglobulin A; sIgA = secretory immunoglobulin A; IL = interleukin; LOS = late-onset sepsis; NEC = necrotizing enterocolitis; TNF-α = tumor necrosis factor alpha.
Treatments and Outcomes of Included Studies (N = 12).
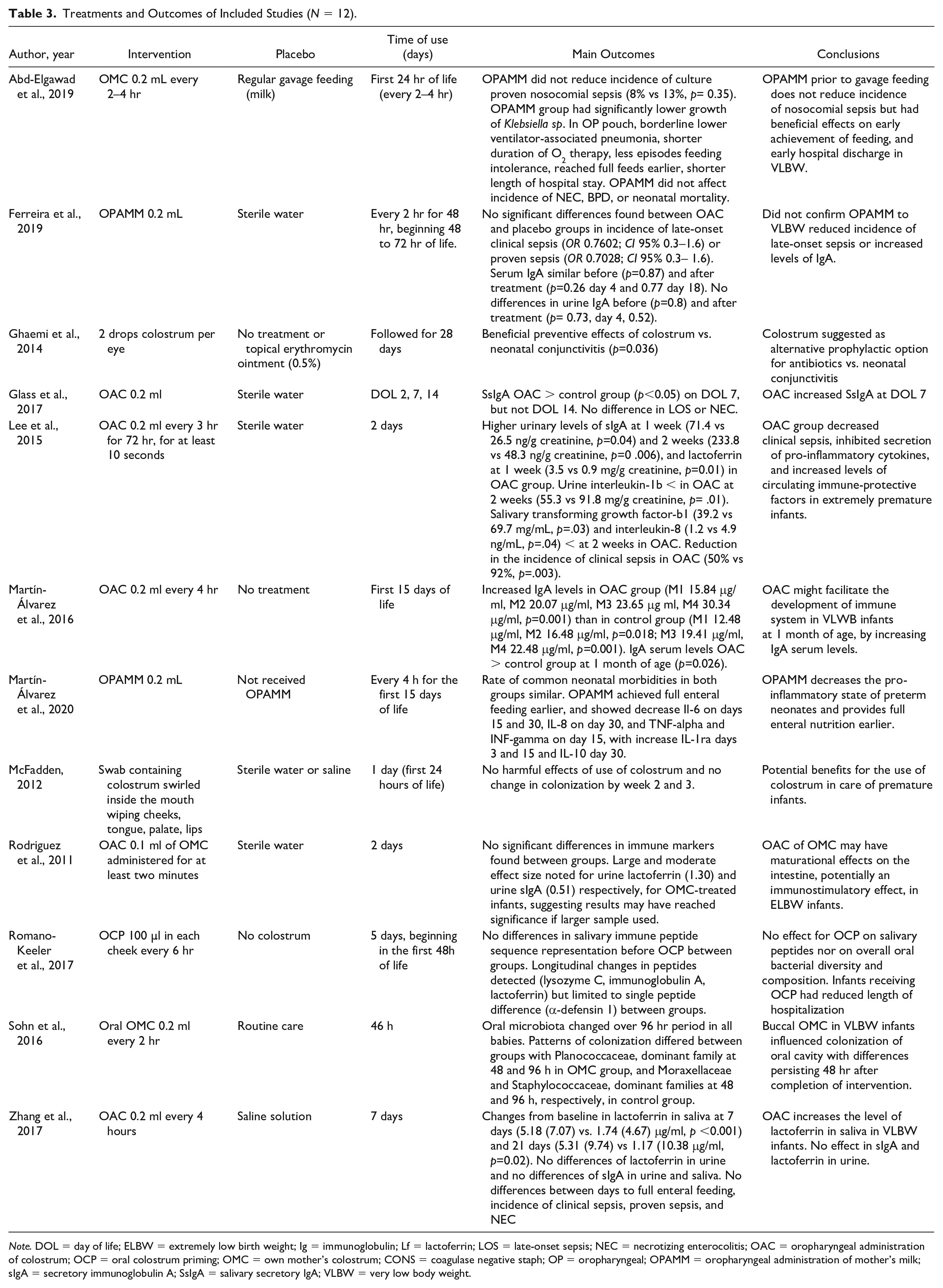
Note. DOL = day of life; ELBW = extremely low birth weight; Ig = immunoglobulin; Lf = lactoferrin; LOS = late-onset sepsis; NEC = necrotizing enterocolitis; OAC = oropharyngeal administration of colostrum; OCP = oral colostrum priming; OMC = own mother’s colostrum; CONS = coagulase negative staph; OP = oropharyngeal; OPAMM = oropharyngeal administration of mother’s milk; sIgA = secretory immunoglobulin A; SsIgA = salivary secretory IgA; VLBW = very low body weight.
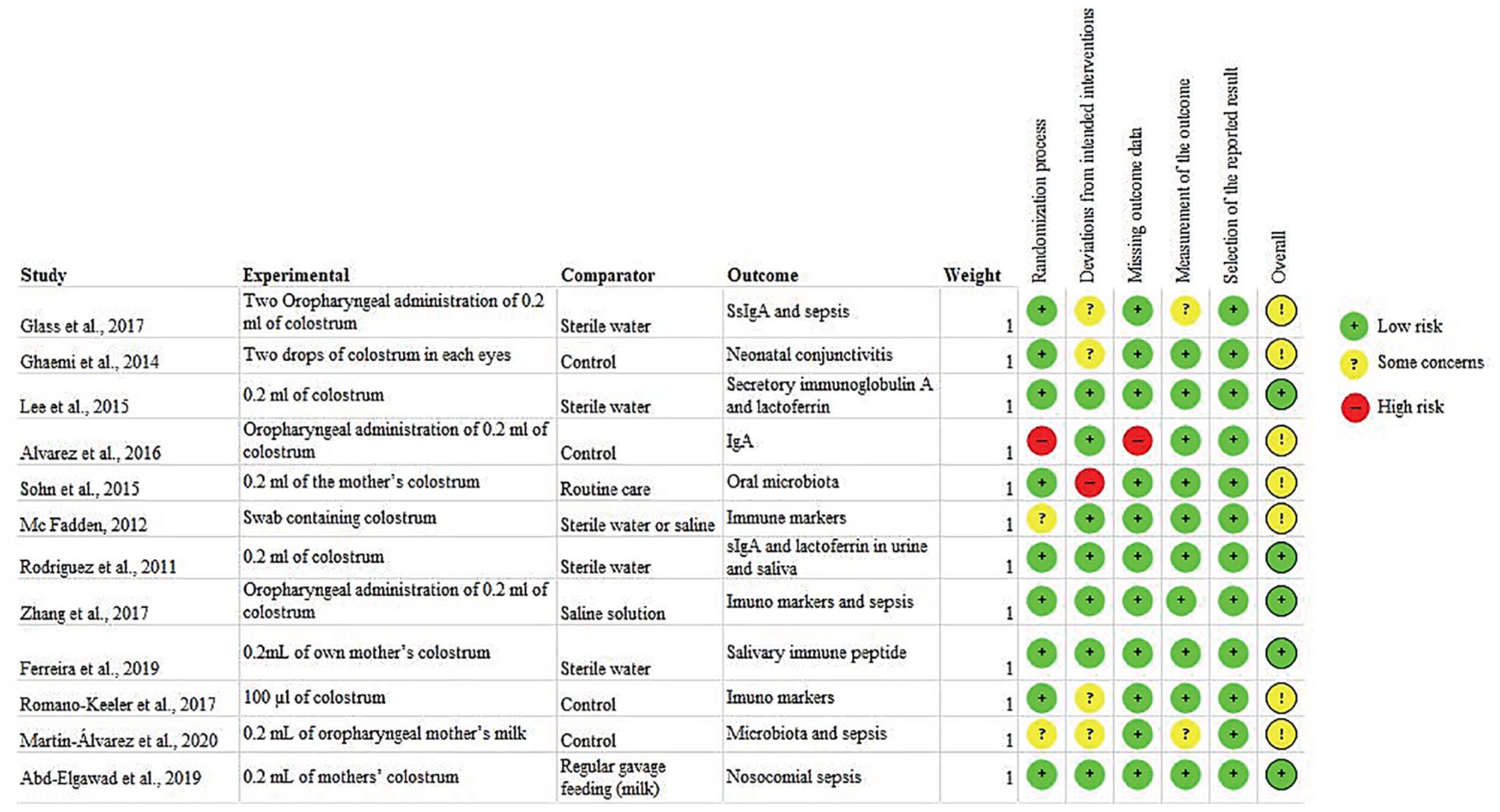
Risk of Bias Risk Table for Each Included Study.
Participants’ immune system laboratory markers were reported in all studies presented assessments of immunoglobulin A (IgA) levels and lactoferrin in patient’s saliva and urine. Sohn et al. (2015) and Romano-Keeler et al. (2017) included data analyzing the natural microbiota of the oral cavity. Zhang et al. (2017), Lee et al. (2015), and Glass et al. (2017) addressed suspected sepsis, and its confirmation in their results. Ferreira et al. (2019) evaluated sepsis and concentrations of IgA in VLBW infants. Abd-Elgawad et al. (2019) evaluated nosocomial sepsis, incidence of necrotizing enterocolitis and neonatal mortality. Finally, Martín-Álvarez et al. (2020) evaluated the serum concentrations of interleukin (IL) IL-6, IL-8, IL-10, IL-1ra, tumor necrosis factor alpha, and interferon gamma.
Intervention Protocols
From the 12 studies included in this review, in nine the colostrum was administered via the oropharyngeal route, in two the colostrum was administered in the newborn’s oral cavity, and in only one study it was used in the eyes of newborns. Regarding the control group, in six studies the control was sterile water or saline solution, and in one study the authors mentioned no treatment. In two studies the authors did not use colostrum/human milk, in one study human milk was used as the control, and in one study erythromycin ointment or no treatment was used.
Regarding the doses used in the studies, nine studies used 0.2 ml of colostrum, two studies 0.1 ml of colostrum, one study two drops in each eye of colostrum, and in one study the authors did not mention doses. The administration time and the frequency with which the colostrum administration occurred varied greatly between the studies, with the application time varying between 1–28 days, as well as the number of applications per day/period also varying from 1–12 times a day (Table 3).
Primary Outcomes
Salivary IgA Levels
In four studies in this review a total of 241 participants were included, of which 121 were in the colostrum group and 120 were in the control group. Salivary IgA levels were measured 1 week after the interventions. A significant difference was shown in the forest plot in salivary IgA levels in the newborns in the group receiving oropharyngeal colostrum, shown in Figure 3A (SMD 0.71; 95% CI [0.25, 1.17]; p = .002 I2=64%, two studies, 241 participants, low-quality evidence). We downgraded the quality of evidence due to (-1) serious inconsistency and (-1) imprecision.
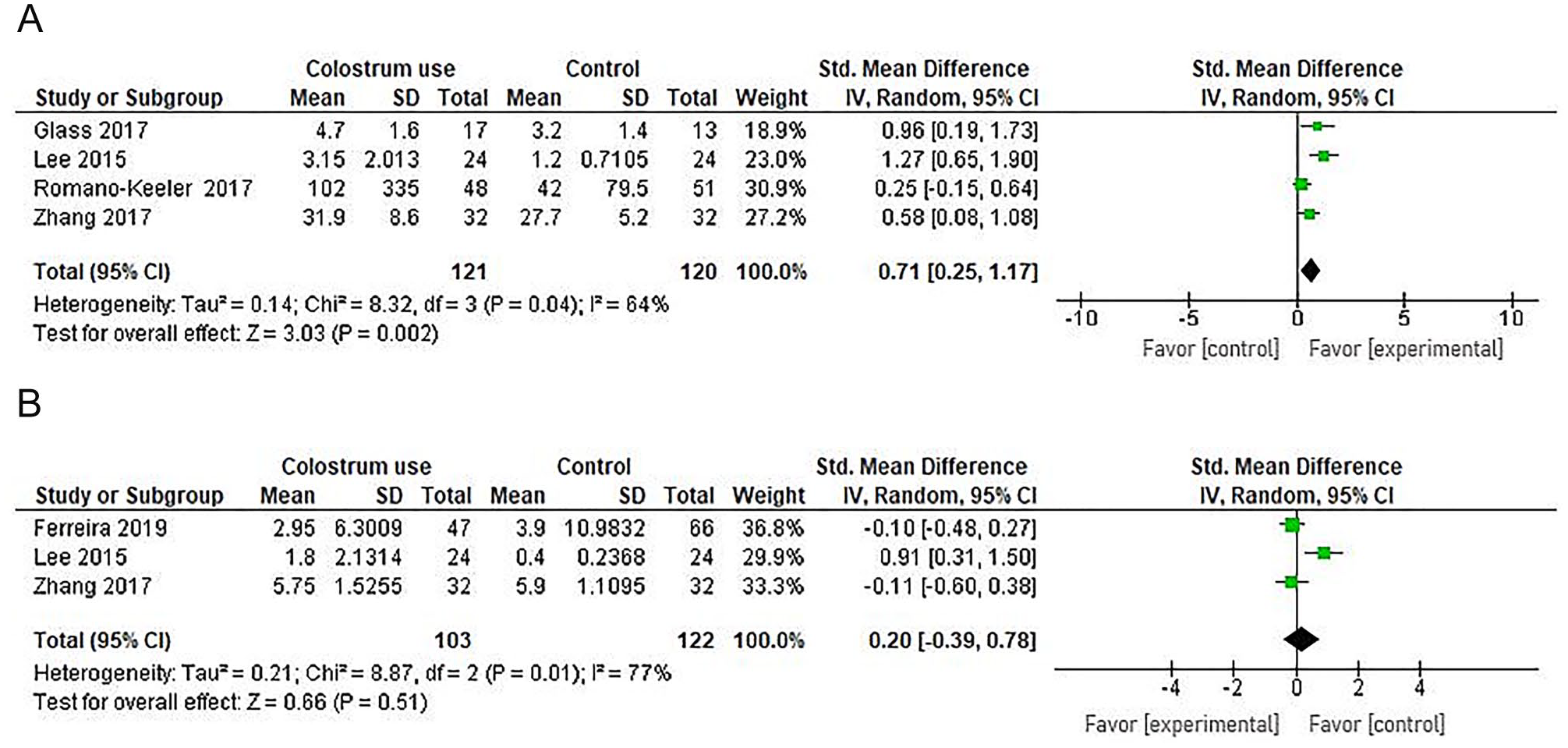
A. Comparison of Salivary IgA Levels After Intervention: Colostrum Versus Control. B. Comparison of Urinary IgA Levels After Intervention: Colostrum Versus Control.
Urinary IgA Levels
After extracting all data from the primary studies, we observed that three studies, with a total of 225 participants reported urine IgA levels in the colostrum (n =103) x control groups (n = 122) after intervention. No difference was shown in the continuous data forest plot in urinary IgA levels in newborns in the group receiving oropharyngeal colostrum compared with the placebo group, shown in Figure 3B (SMD 0.20; 95% CI [-0.39, 0.78]; p = .51; I2=77%, three studies, 225 participants, very-low quality evidence). We downgraded the quality of evidence due to (-2) very serious inconsistency and (-1) serious imprecision.
Secondary Outcomes
Suspected Clinical Sepsis
Regarding the secondary outcome of suspected sepsis with clinical signs between the control and intervention group, with dichotomous data, four studies were included, totaling 427 participants, 194 in the colostrum group and 233 in the control group. In the meta-analysis there was no significant difference between the occurrence of suspected clinical sepsis between both groups (RR 0.98; 95% CI [0.69, 1.39]; p = .90; I2 = 0%, four studies, 427 participants, low quality evidence). We downgraded the quality of evidence due to (-1) serious inconsistency and (-1) serious imprecision. Figure 4A presents the forest plot for suspected clinical sepsis comparison of colostrum x control.
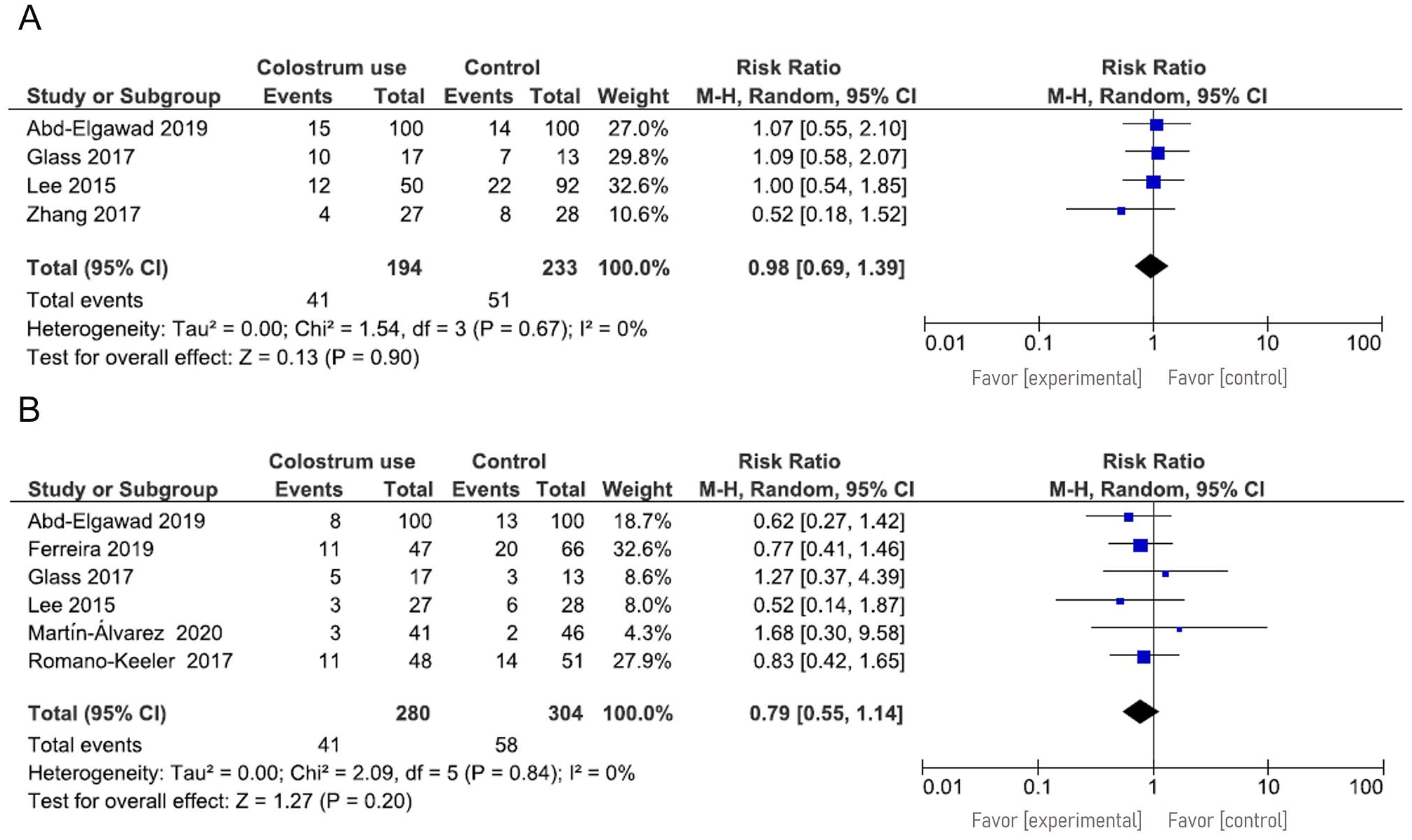
A. Suspected Clinical Sepsis: Colostrum Versus Control. B. Occurrence of Positive Sepsis: Colostrum Versus Control.
Sepsis Positive Culture
In the comparison regarding the occurrence of positive culture sepsis between the control group and those receiving colostrum, six studies were included, totaling 584 participants, 280 in the colostrum group and 304 in the control group. In the meta-analysis, with dichotomous data, there was no significant difference between the occurrence of positive culture sepsis between both groups (RR 0.79; 95% CI [0.55, 1.14]; p = .20 I2 = 0%, six studies, 584 participants, low quality evidence). We downgraded the quality of evidence due to (-1) serious inconsistency and (-1) serious imprecision, as shown in Figure 4B.
Lactoferrin/Urine Levels After 1 Week
The comparison of lactoferrin levels in the urine after 1 week of intervention was evaluated in two studies. Between the colostrum group (56 participants) x control groups (56 participants), totaling 112 participants, there was a significant difference in the forest plot (SMD 0.70; 95% CI [0.03, 1.36]; p = .04; I2 = 65%, two studies, 112 participants, very low-quality evidence). We downgraded the quality of evidence due to (-2) very serious inconsistency and (-1) serious imprecision, as shown in Figure 5A.
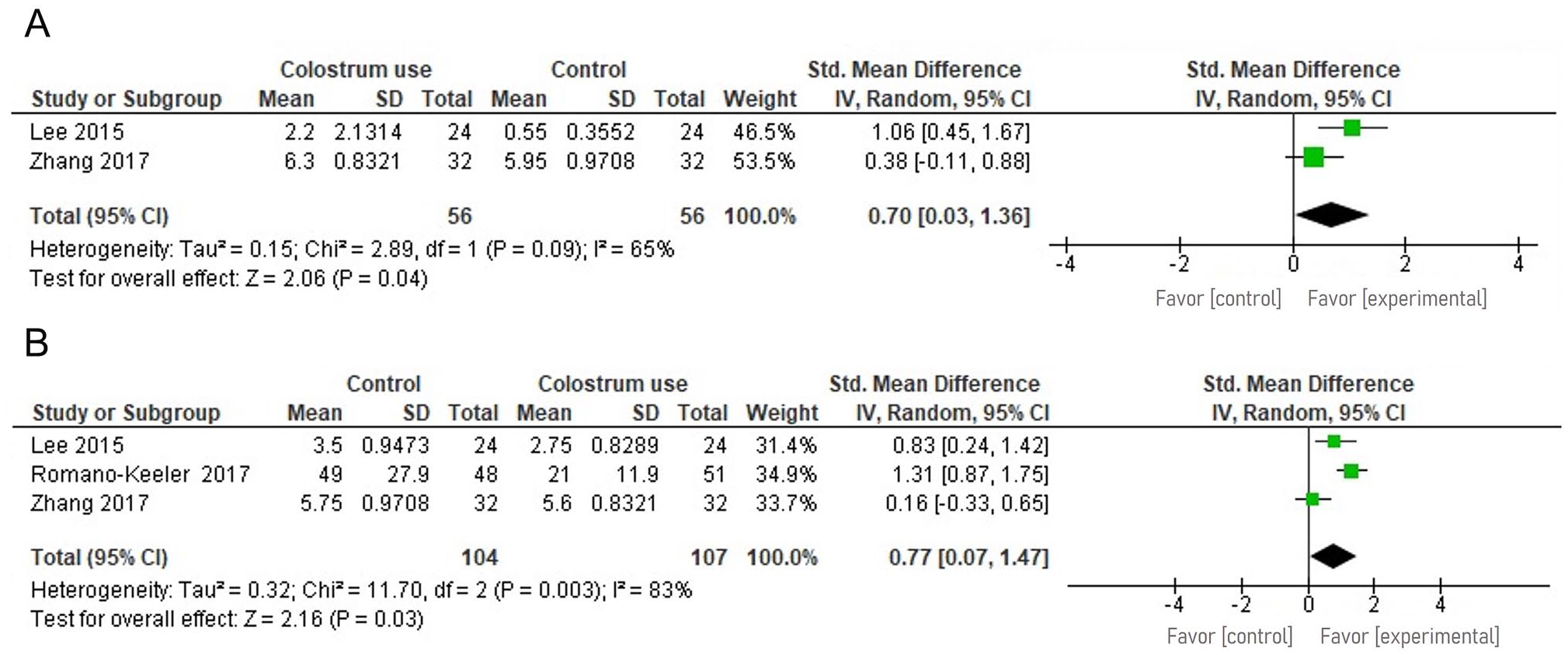
A. Comparison of Lactoferrin Urine Levels After 1 week of Intervention: Colostrum Versus Control. B. Comparison of Lactoferrin Urine Levels Post-Intervention: Colostrum Versus Control.
Lactoferrin/Urine Levels Post-Intervention
Regarding the comparison of post-intervention lactoferrin levels in the urine between the colostrum group (107 participants) and the control group (104 participants), three studies, totaling 211 participants, were included. In the meta-analysis, with continuous data, there was a significant difference in lactoferrin/urine levels post-intervention (SMD 0.77; 95% CI [0.07, 1.47]; p = .03; I2 = 83%, three studies, 211 participants, very low-quality evidence). We downgraded the quality of evidence due to (-2) very serious inconsistency and (-1) serious imprecision, as shown in Figure 5B.
Discussion
In this systematic review we comprehensively assessed the administration of maternal colostrum in preterm newborns. We have demonstrated that colostrum therapy improved lactoferrin levels in urine after 1 week of intervention. RCT studies with sufficient power are needed to investigate the effects of administering maternal colostrum in preterm newborns, allowing for a more in-depth and reliable analysis of the outcomes. The use of correction of the outcomes analyzed (Lee et al., 2015) that performed the correction of urine (diluted vs. concentrated) expressing creatinine per unit helps standardize the data. It is noteworthy that this review has international relevance, as infant mortality and morbidity are associated with preterm birth; therefore, studying interventions and mechanisms will help to understand and perhaps reduce the risks.
Lactoferrin is a glycoprotein that is present in colostrum and milk. It has the quality of binding to iron and is considered a molecule with antimicrobial, antioxidant, anti-inflammatory, anticancer, and immune system regulatory properties (Haschke et al., 2016). Previous researchers have reported that lactoferrin levels in preterm milk have shown significantly higher values than in term milk (Pammi & Abrams, 2015). One possible explanation is that as lactation starts, every hour counts and milk composition changes; for instance, lactoferrin decreases substantially on the 3rd day of lactation (McClelland et al., 1978). Due to its high affinity towards ferric iron, it not only acts as a carrier of iron in human milk but also deprives harmful microbes of iron that is key for their growth. Additionally, lactoferrin not only has antimicrobial properties but also modulates the innate and adaptive immune responses (Tomita et al., 1991).
Increased lactoferrin levels appear to improve neonatal outcomes. The systematic review by Pammi and Abrams (2015) evaluated the use of oral lactoferrin to prevent sepsis in premature infants. Their results showed oral lactoferrin supplementation decreased late-onset sepsis, and all-cause mortality. Oral lactoferrin supplementation with a probiotic decreased late-onset sepsis. They summarized that oral lactoferrin with or without probiotics decreased fungal sepsis, but not chronic lung disease or length of stay.
Immunoglobulin A (IgA) is the main immunoglobulin in colostrum and milk and its concentrations decrease from the 4th week postpartum and during the 1st year of lactation; however, significant levels of IgA are maintained in milk (Riordan et al., 2010). Demers-Mathieu et al. (2019) analyzed mother’s own milk and donor human milk. These samples were collected from 20 mothers of premature babies (gestational age 26–36 weeks). Milk and gastric samples (1–2 ml) were collected on Days 8–9 and 21–22 postnatal age. The samples were analyzed by ELISA for the concentration of secretory IgA (SigA), total IgA (SigA/IgA), total IgM (SigM/IgM), and IgG. The concentrations of total IgA, SigA, total IgM, and IgG were 55.0%, 71.6%, 98.4%, and 41.1% and were similar to donor milk (49.8%, 32.7%, 73.9%, and 39.7%), which showed the importance of colostrum and milk intervention, despite the source. The higher concentration of antibodies suggested lower risk of enteric pathogens in newborns (Demers-Mathieu et al., 2019).
We showed an increase in salivary IgA, but no difference in urinary IgA excretion compared to the control group. Secretory IgA is an antibody that inhibits the binding of pathogens to the respiratory system and the intestinal mucosal epithelial barrier, maintains intestinal mucosal integrity, and provides barrier protection against pathogens that cause respiratory and gastrointestinal tract infections (Hurley et al., 2011). As IgA is absorbed from human milk by the neonatal intestinal mucosa, with subsequent excretion in the urine, it could perhaps be explained that in these infants this absorption was altered or the half-life of IgA may have been shorter than the collection time.
Researchers reporting studies with colostrum samples corroborate and emphasize the importance of human milk, which protects against the oral invasion of a large number of microorganisms (Andreas et al., 2015). However, there is a gap in the literature on evidence in preterm and underweight neonates. As colostrum administration is easy, inexpensive, and well-tolerated, future research should continue to examine the optimal procedure for measuring the direct immunological results of this therapy, as well as clinical outcomes (e.g., infections). Additionally, some very low birth weight infants cannot initiate enteral feeding due to clinical instability, so oropharyngeal colostrum administration may be indicated (Rodriguez et al., 2010).
In our results, there was no significant difference between the occurrence of suspected clinical sepsis, nor in the occurrence of sepsis confirmed with culture between colostrum administration compared to standard care. Ferreira et al. (2019) presented the following incidences in percentage on the occurrence of late-onset clinical sepsis and proven sepsis in the intervention and control groups, respectively: 45% and 23% (colostrum) and 51% and 30% (control). However, their results did not reach statistical differences, which may have been hampered by all newborns in the study, in both groups, being fed with human milk in a volume of at least 100 ml/kg/day. Enteral feeding with human milk itself can influence the serum concentrations of various nutrients and immunoglobulins, as is widely known.
The review by Panchal et al. (2019) evaluated randomized and nonrandomized clinical trials, with a total of 10 articles, with six and four articles in each group, respectively. They determined that there was no scientific significance regarding the outcomes: occurrence of late sepsis, necrotizing enterocolitis Stage 2, mortality from other causes, time to complete feeding, and length of hospital stay. A cited result that agrees with our study is that the concentrations of IgA immunoglobulin increased, as well as lactoferrin.
The challenges in carrying out these studies would be to explain and consider confounders in the analysis as medications are used concomitantly. A well-designed randomized controlled trial would provide more reliable evidence. However, we must ask: Would it be ethical to forbid a mother from giving colostrum to a baby randomly? Perhaps quasi-experimental studies would be the best design to measure the post-intervention effect. There is a growing interest in this subject and new studies are being conducted. Thus, we believe that future studies will make the evidence stronger and more reliable, enabling a greater assessment of the outcomes of the use of colostrum.
Limitations
There were limitations in the process of this systematic review: (1) lack of reporting to permit a non-subjective risk of bias assessment for some domains; (2) clinical and methodological variability in classification in the reviewed studies made the synthesis a challenge due to lack of consistent criteria; and (3) most trials were not registered, presenting another potential source of bias.
One of the limitations was the absence of a protocol about colostrum administration within the reviewed studies. In addition, there was a lack of standardization in the collection of human milk, form of storage, storage time, and colostrum temperature and quantity. The investigators of these studies showed mainly a variation in the application of colostrum and the time of follow-up of the newborns, making it impossible to carry out a specific analysis of dose, time, and effects. Another limiting factor was that only one of the reviewed studies analyzed newborns up to 28 weeks separately from the those 28–32 weeks old (Abd-Elgawad et al., 2019), which would be important data to be analyzed in subgroups.
Conclusion
We suggest that colostrum appears to have an effect in increasing lactoferrin levels in the urine after 1 week of intervention. The magnitude of the effect was large. However, the quality of evidence was very low, indicating that future studies may change the estimates of the intervention.
Supplemental Material
sj-docx-1-jhl-10.1177_08903344221087967 – Supplemental material for Colostrum Use and the Immune System of Premature Newborns: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-jhl-10.1177_08903344221087967 for Colostrum Use and the Immune System of Premature Newborns: A Systematic Review and Meta-Analysis by Tamy Colonetti, Isabela de Carvalho Florêncio, Pâmela Figueiredo, Laura Colonetti, Maria Laura Rodrigues Uggioni, Maria Inês da Rosa, Luciane B. Ceretta, Leonardo Roever and Antonio Jose Grande in Journal of Human Lactation
Supplemental Material
sj-docx-2-jhl-10.1177_08903344221087967 – Supplemental material for Colostrum Use and the Immune System of Premature Newborns: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-2-jhl-10.1177_08903344221087967 for Colostrum Use and the Immune System of Premature Newborns: A Systematic Review and Meta-Analysis by Tamy Colonetti, Isabela de Carvalho Florêncio, Pâmela Figueiredo, Laura Colonetti, Maria Laura Rodrigues Uggioni, Maria Inês da Rosa, Luciane B. Ceretta, Leonardo Roever and Antonio Jose Grande in Journal of Human Lactation
Footnotes
Authors’ Note
Author contribution(s)
Disclosures and Conflicts of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplementary Material may be found in the “Supplemental material” tab in the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.