
Abstract
Background:
Globally, 10% of all births are preterm. Access to human milk via manual breast expression is required to reduce the incidence of adverse outcomes related to prematurity. However, there is little evidence to recommend optimum timing to commence breast expression in mothers of preterm infants or the most effective method.
Research Aims:
(1) To test feasibility of recruitment and compliance to the protocol and (2) to determine influence of using hand expressing and breast massage on milk production, engorgement, mastitis, and breastfeeding status at 3 months.
Methods:
This study was an exploratory parallel two-group, pilot randomized controlled trial. Mothers of preterm infants at a metropolitan maternity hospital in Queensland Australia (N = 31) were randomized to receive either hand expressing and breast massage within the 1st hr of birth or standard care, hand expressing within 6 hr of birth, to determine the influence on milk production, engorgement, mastitis, and breastfeeding status at 3 months.
Results:
Feasibility targets were not met; however, valuable learning from this trial uncovered barriers facing midwives in the birth suite to commencing expressing in the 1st hr of birth. There was no difference in occurrence of secondary outcomes, although trends support future study.
Conclusions:
Overall, unpredictability of preterm birth influenced our ability to recruit participants. Important directions for future study design would benefit from incorporating expressing times up to 6 hr with a replicable breast massage.
Keywords
Key Messages
There is little evidence to recommend optimum timing or the most effective method to commence breast expression for mothers of preterm infants.
This pilot revealed important directions for future research, uncovered the barriers facing midwives in the birth suite to commencing expressing in the 1st hr of birth, and a larger cohort and a replicable breast massage may demonstrate stronger significance and confidence in recommendations for practice.
Background
Globally, 10% of all births are preterm, with most countries reporting an increase in the preterm birth rate over the last 20 years, making prematurity the leading cause of neonatal, infant, and child mortality (Liu et al., 2016; Pinto et al., 2019). Preterm babies are also at greater risk of health complications across the life course including respiratory, gastrointestinal, and infectious conditions; hearing, and vision problems, neurodevelopmental disabilities, and chronic diseases (Crump et al., 2020; Jacobi-Polishook et al., 2016; Magai et al., 2020).
The protective factors of human milk for both mother and baby are well documented for reducing adverse outcomes (Cortez et al., 2018; Feltner et al., 2018; Huang et al., 2019). Despite this, the rates of exclusive breastfeeding on discharge from hospital for preterm infants range from 20%–55% across a number of developed countries (Cuttini et al., 2019; Ericson et al., 2016; Pineda, 2011). However, there is little evidence on the optimal time to commence breast expression, or the most effective methods to support expression and breastfeeding success.
Previous researchers have suggested that expressing within 6 hr of birth is associated with early establishment of lactation (Becker et al., 2016; Furman et al., 2002). A randomized controlled trial (RCT) published by Parker et al. (2020), randomized 180 mothers into three groups: early (within 60 min), intermediate (61–180 min) and late (181–360 min). The authors reported that participants who express between 3 and 6 hr had increased milk production; all groups used an electric breast pump (Parker, Sullivan, Kruger, et al., 2020). The authors hypothesized that early initiation of expressing would be associated with increased milk production based on a previous pilot RCT and an observational study (Parker et al., 2012, 2015). However, neither was adequately powered to detect differences in milk volume. Their discussion highlighted the late group had 14% more expression sessions compared to the other groups, with further research needed (Parker, Sullivan, Kruger, et al., 2020). A 2016 Cochrane review (Becker et al., 2016), about methods of milk expression, recommended expressing be initiated soon after birth with the inclusion of low-cost interventions, for instance relaxation, massage, and hand expression. Hand expressing and electric pumping, as the first mode of expressing were both used; however, it has been suggested that hand expressing is more effective in the first 48 hr and that it provides an opportunity to teach massage techniques (Ohyama et al., 2010). In a systematic review about the effectiveness of breast massage, researchers reported that breast massage may enhance milk flow when combined with expressing and may reduce the incidence of engorgement and mastitis (Anderson et al., 2019). However, their review highlighted several methodological limitations and recommended further research, particularly in vulnerable groups, including mothers of preterm infants. This systematic review did not identify any previous studies that investigated hand expressing combined with massage in the 1st hr of birth. Our study was designed to address this gap. This study’s primary aims were (1) to test the feasibility of recruitment and compliance to the protocol and (2) to determine the influence of using hand expressing and breast massage on milk production, engorgement, mastitis, and breastfeeding status at 3 months.
Methods
Research Design
This study was an exploratory parallel two-group, pilot randomized controlled trial. A pilot was chosen to assess for the challenges of conducting a full RCT. This study was approved by the Mater Misericordiae Ltd, Mater Mothers’ Hospitals Human Research Ethics Committee (MM-HREC) in 2017 (HREC Protocol Number 17/MHS/83).
Setting and Relevant Context
This study was conducted in a large, metropolitan, tertiary maternity hospital in Queensland, Australia with over 500 babies born under 35 weeks’ gestation annually. The hospital is one of the largest in Australia, birthing over 10,000 babies per year and offering the highest level tertiary services to women, with approximately half having private insurance status. Specialist public services are provided for First Nations women, women from refugee backgrounds, and a large number of women from multiple ethnic backgrounds who live in the catchment area. The research was undertaken in four areas: birth suite, antenatal ward, postnatal ward, and neonatal critical care unit. The hospital provides lactation support from International Board Certified Lactation Consultants (IBCLC).
Sample
The inclusion criteria were women who were 28–35 weeks’ gestation, aged 16 years or older, who planned to breastfeed, and were expecting a preterm birth. The predictive criteria for preterm birth involved one or more of the following: preterm pre-labor rupture of membranes, evidence of cervical dilatation and/or effacement, history of preterm labor and birth, positive fetal fibronectin or actim partus test, planned preterm birth, or receiving magnesium sulphate infusion. We excluded mothers with history of breast surgery and admission to intensive care.
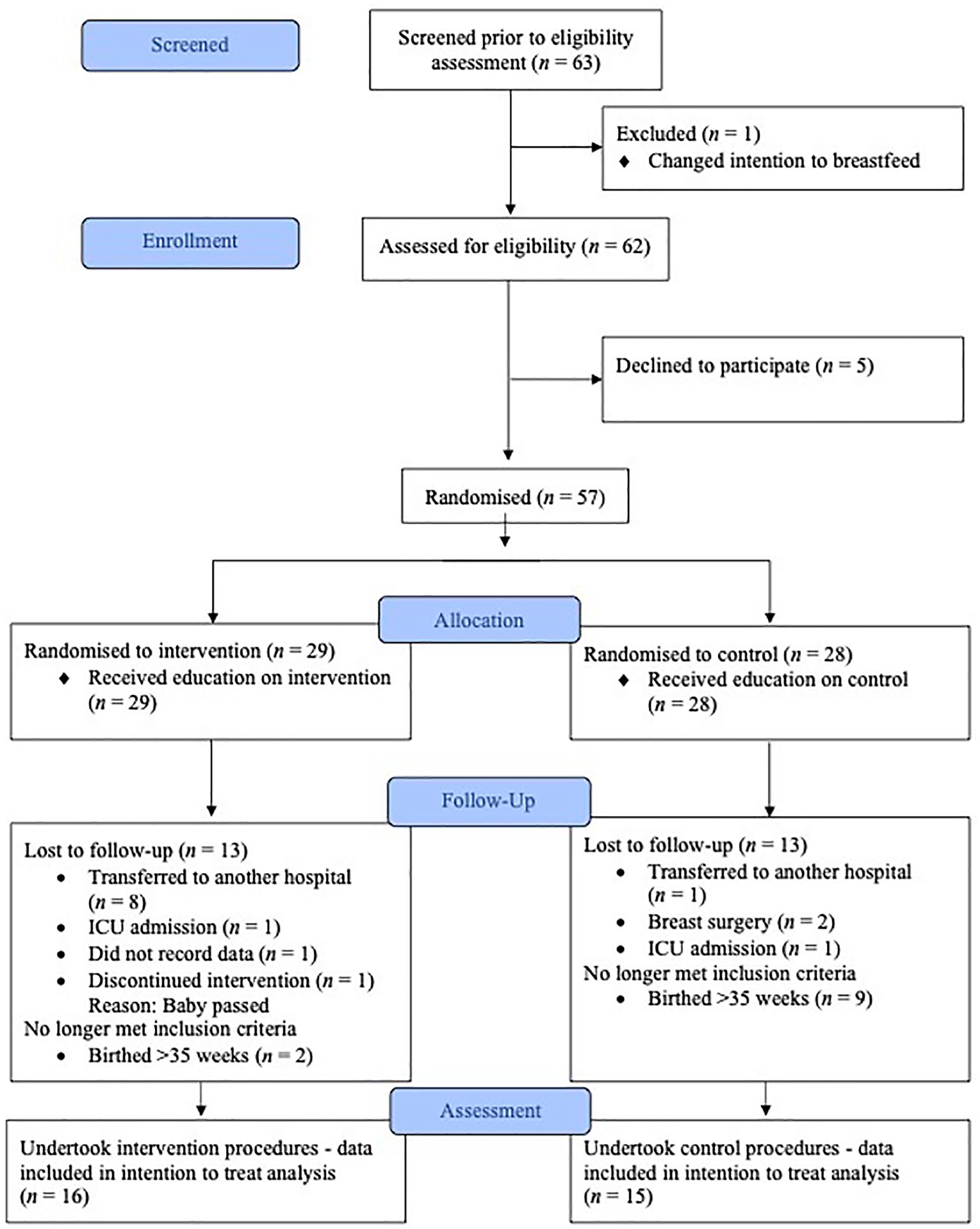
During 13 months of recruitment, there were 455 preterm births at the study facility who were potentially eligible to participate. Of note, randomization and education provision occurred on average 10.67 days prior to birth with the midwives education occurring over the first 6 months of recruitment. The number of preterm births meeting the inclusion criteria within the study period was 63, with six excluded, leaving 57 to randomize. Following randomization, almost half the participants (n = 26) were lost to follow up due to: transferred to another hospital (n = 9), Intensive Care Unit (ICU) admission (n = 2), did not record data (n = 1), breast surgery (n = 2), discontinued intervention (n = 1), and birthed > 35 weeks (n = 11). The remaining participants in the intervention (n = 16) and control (n = 15) groups all undertook the prescribed interventions (Figure 1).
Sample.
Sample size calculation was based on three areas: (1) general guidelines for pilot studies, including a general rule of at least 30 participants and a minimum sample size of 12 participants per group (Bell et al., 2018; Whitehead et al., 2016); (2) the estimated timeframe to complete the study; and (3) the number of preterm births at the research facility over 1 year. Allowing for attrition, we estimated a sample size of 30 participants, 15 in each arm, required to explore the feasibility outcomes with this total adequately representing the sample.
Measurement
Data about the feasibility of protocol compliance was collected at recruitment and extracted from participant logs and included number of preterm births meeting the inclusion criteria and compliance to trial interventions of expressing within the 1st hr with the use of breast massage. Data about the volumes of expressed milk were collected from participants’ expressing logs and a total daily measurement was documented from Days 1–7 and on Day 14. Participants were taught how to use a syringe to collect colostrum and shown how to read the measurements on the syringe to document. Each participant recorded the date and time of first expression, use of breast massage prior to expressing, method of expressing, and any breastfeeds. Data on signs of Lactogenesis II were recorded in the expressing log by the participant in line with the following criteria: maternal perception of swelling, fullness, physiological engorgement, and leaking of the breast daily (Chapman & Pérez-Escamilla, 2000; Parker, Sullivan, Cacho, et al., 2020). Occurrence of Lactogenesis II was recorded as the day when symptoms presented.
Participants were assessed daily either on the postnatal ward or, following participant discharge, in the neonatal critical care unit when visiting their baby from Days 1–7 and on Day 14 by the lead researcher for engorgement, characterized by hard, painful, tight breasts with difficulty expressing (Mangesi & Zakarija-Grkovic, 2016). Participants were assessed for mastitis each day, using the clinical definition of pain, redness, swelling with temperature of 38.5 °C or greater, chills, flu-like aching, and prescribed antibiotics (Amir, 2014).
Engorgement and mastitis were scored using a severity index and pain scale with the content examined by five Taiwanese experts including two nursing professors, two IBCLCs, and one obstetrician. The experts used a 4-point Likert scale from nonrelevant (1) to very relevant (4), with a content validity index calculated using the proportion of items given a rating of three or four by all experts. An index of 1.00 and Cronbach’s alpha of 0.83 was given as all items received a rating of three or four from all experts (Chiu et al., 2010). The scale has a total of three self-rated scores comprised of erythema (0–4), breast tension (0–5), and a visual analogue pain score (0–10). Participants were followed up at 3 months via a phone call with data collected about breastfeeding status, milk volume, and experience of engorgement and mastitis, as defined above.
Data Collection
This study conducted from February 2018 to March 2019. Potential participants were invited to take part in the study by the lead researcher following consultation and introduction from the clinical ward team leader and were provided with a Participant Information and Consent Form detailing the study purpose and procedures. Privacy was provided by the lead researcher for the potential participant to read the document; the lead researcher returned when the participant requested, and consent was signed. Each participant was assigned an identification number to maintain confidentiality with consent forms securely stored separately from the data. Additionally, the data collection forms were stored in a locked drawer within the lead researcher’s department.
Following informed consent, randomization was undertaken using sequentially numbered opaque envelopes prepared independently of the research team in permuted blocks of 2–4. Due to the nature of the intervention, blinding was not possible. The risk of contamination between participants was low due to single room occupancy, participants being spread over two floors, and the intervention being undertaken by the participant rather than the midwife. Furthermore, data for the primary outcomes was collected during recruitment and consent process. Notes about compliance with trial processes were also recorded, with all data stored in a specifically designed, password protected database.
Intervention Group
Participants were allocated to the intervention group prior to birth and received information about breast massage and hand expressing techniques to express colostrum within 1 hr following birth. Intervention participants also received both written and instructional information (see supplementary materials) about anatomy and the physiology of milk production, a breast massage technique including lifting the breast with one hand while using the middle three fingers on the other hand to rub in a circular motion around the entire breast for 1–2 min on each side, a demonstration of hand expressing using a breast model, as well as usual hospital standard care, described below. The breast massage technique was constructed with evidence and clinical experience (Anderson et al., 2019). The information provided to participants in the intervention group was designed to enable a mother-led approach supported by their midwives, rather than relying on midwives to initiate the expression and massage.
Control Group
Participants allocated to the control group received a hospital brochure outlining standard care, which included written information on expressing by hand and pump within 1–6 hr of birth, how to use a breast pump, and an expressing log. Participants were advised to read the information and shown how to fill in the expressing log. Following birth, both the intervention and control group were cared for by the midwives as per standard care and were visited by the lead researcher daily either on the postnatal ward or the neonatal critical care unit between Days 1–7 and on Day 14 and contacted by phone at 3 months to collect data. Additionally, education was provided by the lead researcher including six in-services over 6 months from March 2018 to July 2018 for birth suite midwives, and the continuity of care midwives group outlining the study. This included an overview of the research, the purpose of the research, and participant and staff involvement.
Data Analysis
The intention to treat (ITT) approach was used for analysis. To determine feasibility and proceed to a full RCT the following parameters were agreed: number of women approached and agreed to be recruited > 80%, number of participants who completed the intervention as planned > 80% and < 10% drop out or lost to follow-up. Differences between groups were compared using t tests for normally distributed continuous data and chi-square tests for nominal data with the use of Fisher’s Exact test for variables when any cell with an expected frequency < 5.
Simple descriptive stats were used to describe the primary outcomes. For the total expressed milk volume measured over the days in the same participant we used a multilevel model to control for the clustering effect. Expressed milk volume across 14 days are model predicted mean volumes. Treatment effects were presented as mean differences with its associated 95% CI between intervention and control group. To describe day of establishment of milk supply, engorgement, and mastitis, we used the chi-square test with Fisher’s Exact test. The chi-square test was used to compare breastfeeding status at 3 months between groups. The statistical significance was set at the p = .05 level.
Results
Characteristics of the Sample
Participants in both groups had demographics and characteristics at baseline that were similar (Table 1). Participants were on average 32.9 (SD = 5.3) years old. Participant age did not differ by condition.
Summary of Participant Characteristics (N = 57).
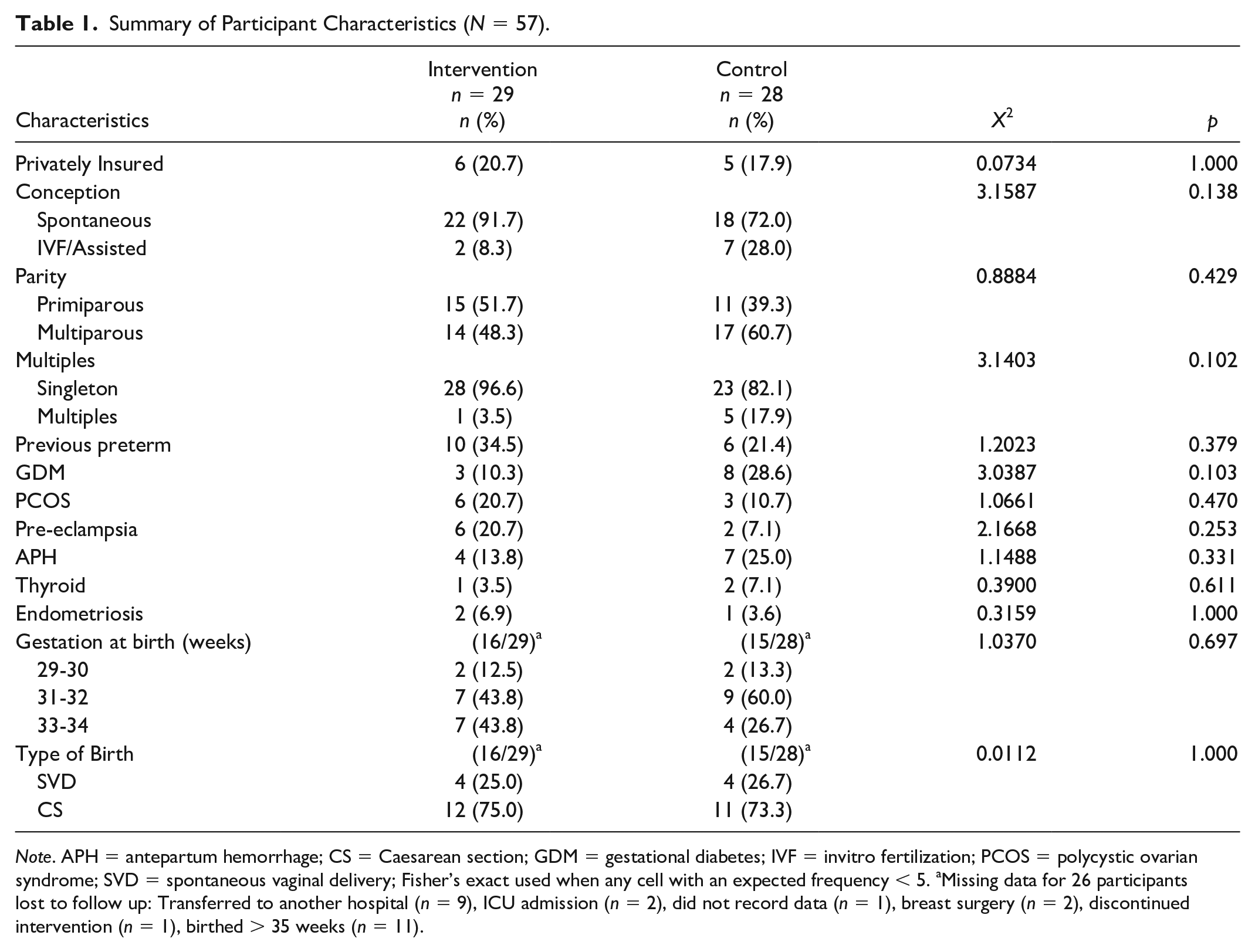
Note. APH = antepartum hemorrhage; CS = Caesarean section; GDM = gestational diabetes; IVF = invitro fertilization; PCOS = polycystic ovarian syndrome; SVD = spontaneous vaginal delivery; Fisher’s exact used when any cell with an expected frequency < 5. aMissing data for 26 participants lost to follow up: Transferred to another hospital (n = 9), ICU admission (n = 2), did not record data (n = 1), breast surgery (n = 2), discontinued intervention (n = 1), birthed > 35 weeks (n = 11).
Outcomes
Due to the small sample size, secondary outcomes are exploratory only. Compliance with trial interventions of initiating expressing within the 1st hr of birth was not met. Only three (19%) of the intervention group participants, and two (13%) of the control group, expressed within the 1st hr of birth. The mean (SD) time of first expression for participants in the intervention group was 5.4 (5.3) hr from birth and 5.9 (4.3) hr in the control with both groups having outliers (intervention 19 hr and control 16 hr). Compliance with breast massage prior to the first expression was low with seven (44%) participants in the intervention group performing breast massage as prescribed.
There was a significant difference in expressed milk volume favoring the control group on Days 6, 7, and 14 (Table 2); however, this was accompanied by a higher number of infants feeding directly at the breast for participants in the intervention group (Figure 2). Table 2 represents the model predicted expressed milk volume across 14 days, not the mean of observed volume. The multilevel mixed model assumed the expressed milk volume was normally distributed, therefore, with the milk volume in Day 1 and Day 2 in the intervention group very small, the model predicted a negative value, which is not statistically different from zero.
Total Daily Expressed Milk Volume (ml) Over Time Between Intervention and Control Group—Multilevel Mixed Model Analysis (N = 31).
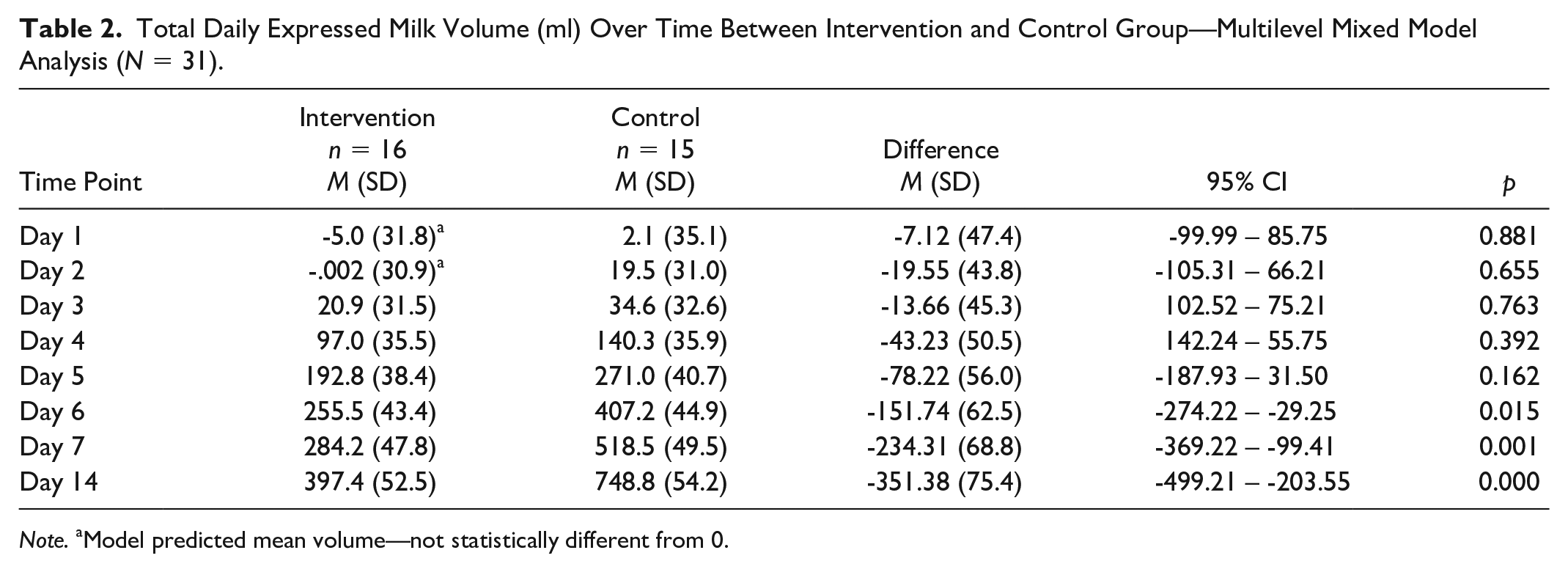
Note. aModel predicted mean volume—not statistically different from 0.
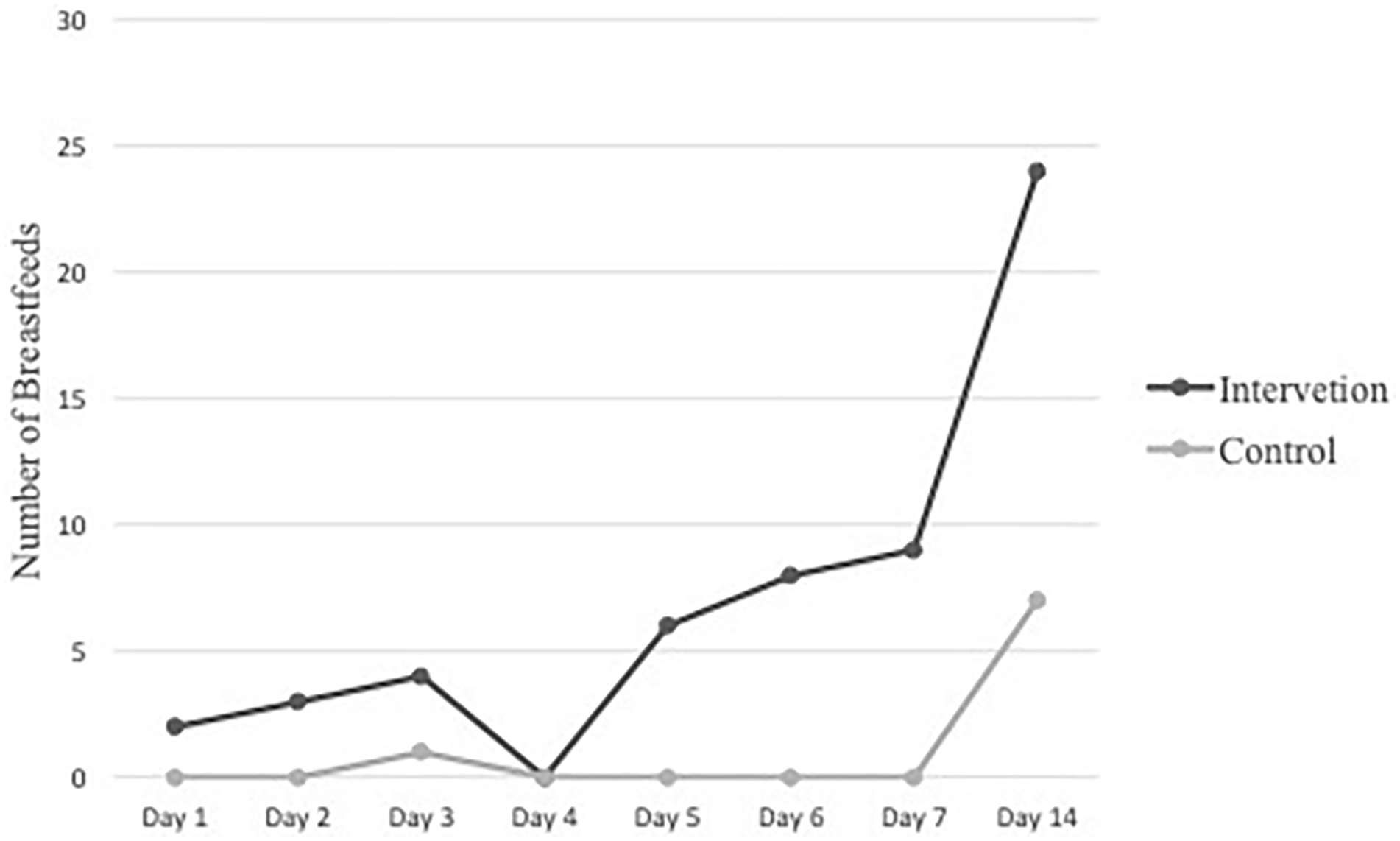
Total Daily Breastfeeding Occurrences for each Group.
Breastfeeding occurrences—that is, feeding directly at the breast—for participants in the intervention group was considerably more on Days 6 and 7 compared to the control group, which was zero on these days. Furthermore, on Day 14 the participants in the intervention group breastfed more than three times that of the control group. Any milk consumed via the breast was not measured in this pilot study but is may be the reason for the significant difference in milk volume (Figure 2).
The secondary outcome of Lactogenesis II results were similar in both groups. By Day 5 11 (74.4%) of the participants in the intervention group and 12 (81%) of the participants in the control group had reached Lactogenesis II (p = .879). Two participants in the intervention group and one in the control group did not establish lactation. Interestingly, the participants in the intervention group both suffered from high blood pressure and all three participants who did not establish lactation undertook their first expression between 8 and 19 hr.
There were no significant differences between the two groups for experiences of mastitis and engorgement. The control group experienced a 20% higher rate of engorgement compared to the intervention group, although the difference was not significant (p = .083). There was one case of mastitis in the control group over a 3-month period (Table 3).
Experience of Engorgement and Mastitis Any Time Over First 3 Months (N = 31).
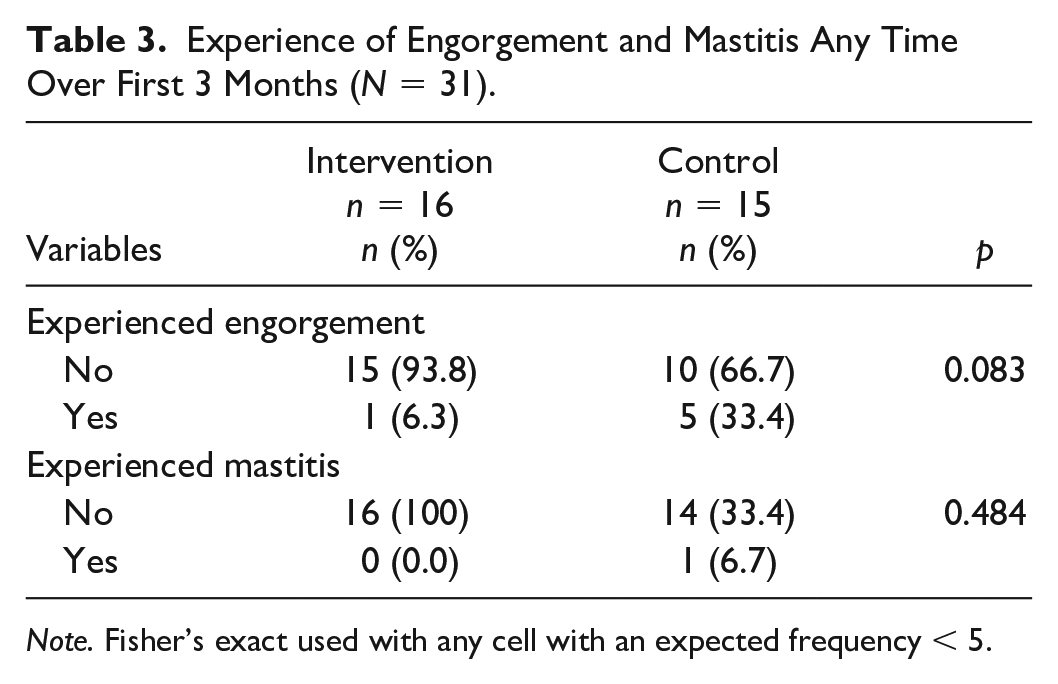
Note. Fisher’s exact used with any cell with an expected frequency < 5.
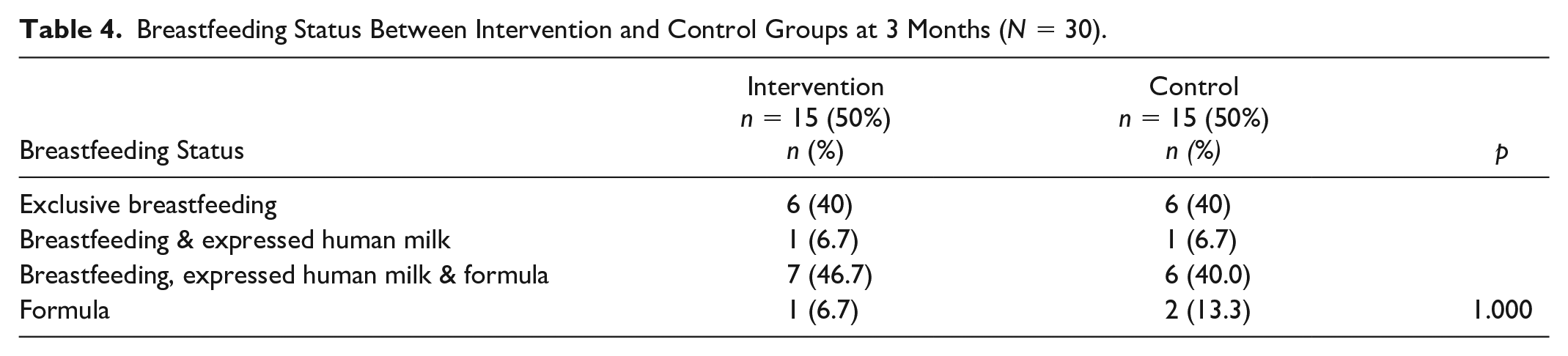
The participants were followed up at 3 months to enquire about breastfeeding status. At 3 months, almost 50% of both groups were providing human milk exclusively via direct breastfeeding or expressing, and over 85% of both groups were providing some human milk to their infant. The remaining participants fed their baby with a mix of breastfeeding, expressed human milk, and formula with 10% of the combined groups feeding with formula at 3 months (Table 4).
Breastfeeding Status Between Intervention and Control Groups at 3 Months (N = 30).
Discussion
Overall, feasibility targets were not met; however, valuable learning from this pilot study, and current literature, informed recommendations for a future RCT. Many potentially eligible participants were never approached due to the unpredictability of preterm birth and the limited availability of research staff. Almost half the participants randomized were no longer eligible, or lost to follow up, by the time they birthed. We had planned to randomize participants in early labor but were not given ethical approval, and thus relied on consent and randomization for participants prior to labor. Additional contributing factors were short stays for threatened preterm birth and difficult recruitment pathways for privately insured participants.
Compliance with the trial intervention of expressing within the 1st hr of birth was not met, with small numbers in both cohorts expressing in this time frame. In this study the intervention group relied upon memory recall of the education given and the ability of the participant to express independently so as not to influence existing clinical workloads. The reasons for non-compliance noted in field notes during data collection highlighted issues (e.g., forgot to express in the 1st hr, staff unavailable to help, did not have the information with them, and too tired).
During recruitment, participants in both groups were eager to ask questions about breastfeeding a preterm infant. As the lead investigator was a clinician and IBCLC there was a duty of care to answer the participants’ question and may have revealed information relevant to the intervention group, contributing to group contamination. Furthermore, our study intervention was purposefully led by the participant with guidance from the midwives, testing feasibility of the intervention in the clinical context (Olufunlayo et al., 2019).
There were a number of clinical and organizational barriers that affected compliance with the intervention. First, some of the participants were transferred between multiple wards and there was little consistent documentation between the wards detailing if and when breastfeeding education had been provided. This oversight may have contributed to the study’s low compliance rate for expressing within the 1st hr of birth. Midwives, as trusted health professionals, play a major role in educating mothers to breastfeed. A qualitative study on exploring health education with midwives, as perceived by participants, found information was highly appreciated and a more pro-active approach from midwives may be valuable (Baron et al., 2017). The intervention group may not have placed importance on expressing and not recalled their involvement in the study. Secondly, the “ownership” of the necessary expressing education was not clear within each department. The lack of awareness or pathway between each department may have contributed to the delay of the first expression. Midwives’ experiences of educating mothers of preterm infants will be further explored to address these barriers.
Compliance with breast massage prior to the first expression was not met within the intervention group. There are many breast massage techniques used for breastfeeding mothers which are individual to the person performing the massage and their skill level. A systematic review on breast massage and breastfeeding problems highlighted large variations of breast massage techniques and skill level (Anderson et al., 2019). At the study facility there is no guideline for providing breast massage as a technique to support the initiation of breastfeeding; however, it is used in varying degrees as recorded by the participants. Further research about a replicable breast massage technique may be useful to create uniformity, particularly as this study found a high proportion of participants with engorgement in the control group.
Both the intervention and control groups’ secondary outcome of milk supply were similar. Prior to our study, expressing within 6 hr of birth was achieved less than 50% of the time at the study facility. This study, however, did find that achieving expressing within 6 hr of birth in both groups is possible. The RCT by Parker (2020) measuring milk volume to 6 weeks reported the late expressing group (3–6 hr) produced more milk during the first 3 days only. Combining results from the earlier RCT by Furman (2002), together with the results of Parker’s (2020) study and our own, suggested that expressing within 6 hr of birth may be more achievable, highlighting the need to undertake further study (Furman et al., 2002; Parker, Sullivan, Kruger, et al., 2020).
There is a dearth of literature about the experience of engorgement and mastitis for mothers of preterm infants; however, we found a lower incidence in the intervention group. The intervention group and control groups’ experience of mastitis was well below the average, with the literature stating that approximately 33% of women experience mastitis (Cooper et al., 2020; Kvist, 2013). Additionally, breast engorgement and mastitis are two of the most common reasons for early cessation of breastfeeding. Preventing these issues is key to ensuring sustained breastfeeding in line with World Health Organization (2017) recommendations. Although our numbers are very small, they do encourage further research in this area.
In summary, the findings of our pilot trial suggested that a RCT investigating the benefits of expressing within the 1st hr of birth with breast massage would need considerable protocol adjustment to be feasible. Recruiting and randomizing participants after birth, to commence the intervention (massage and hand expression) within 3–6 hr may be a better approach. Extending the inclusion criteria to all women who have a baby in the neonatal intensive care and changing the primary outcomes to take the emphasis off milk volume, instead focusing on engorgement, mastitis, and breastfeeding outcomes at 3 months, may be more appropriate.
The results from this pilot RCT highlighted the barriers to expressing within the 1st hr with future direction focused on exploring expressing within 6 hr of birth. Moreover, it is important to assess the results of breast massage coupled with expressing, not only on milk supply but on incidence of engorgement and mastitis. All participants who experienced engorgement did not perform breast massage prior to the first expression within this study. Further qualitative research would provide additional information about the challenges that midwives face. Ideally, exploring expression coupled with breast massage within 6 hr of birth in a larger trial, may prove beneficia, if sufficient funding for adequate support during recruitment, and support from the entire study facility was available.
Limitations
This study aimed to address feasibility; therefore, it was not powered for inference in the clinical outcomes. Due to this, the study’s limitations include organizational issues (e.g., transfers between multiple wards and lack of, or inconsistent, documentation on expressing). Some aspects that may be pertinent in a full pragmatic trial of this complex intervention (e.g., sub-group analysis of massage vs. no massage and hand vs. mechanical expression) were not possible to include in this feasibility study due to limited resources and small sample size. Additionally, feedback from clinical staff about barriers to implementing the intervention and early initiating of expressing generally were not sought. A qualitative exploration of these issues is underway and will be important to the planning of a larger study.
Conclusions
The findings of our study suggested that for a full trial to be feasible a number of challenges would need to be addressed. Overall, the study’s primary outcomes of feasibility of expressing within the 1st hr of birth with breast massage were influenced by the unpredictability of preterm birth and the challenges of conducting research in a high flow, acute care area.
Supplemental Material
sj-docx-1-jhl-10.1177_08903344221088789 – Supplemental material for A Comparison of the Timing of Hand Expressing of Human Milk With Breast Massage to Standard Care for Mothers of Preterm Infants: An Exploratory Pilot Using a Randomized Controlled Design
Supplemental material, sj-docx-1-jhl-10.1177_08903344221088789 for A Comparison of the Timing of Hand Expressing of Human Milk With Breast Massage to Standard Care for Mothers of Preterm Infants: An Exploratory Pilot Using a Randomized Controlled Design by Loretta A. Anderson, Sue Kildea, Nigel Lee, Kathryn Kynoch and Yu Gao in Journal of Human Lactation
Supplemental Material
sj-docx-2-jhl-10.1177_08903344221088789 – Supplemental material for A Comparison of the Timing of Hand Expressing of Human Milk With Breast Massage to Standard Care for Mothers of Preterm Infants: An Exploratory Pilot Using a Randomized Controlled Design
Supplemental material, sj-docx-2-jhl-10.1177_08903344221088789 for A Comparison of the Timing of Hand Expressing of Human Milk With Breast Massage to Standard Care for Mothers of Preterm Infants: An Exploratory Pilot Using a Randomized Controlled Design by Loretta A. Anderson, Sue Kildea, Nigel Lee, Kathryn Kynoch and Yu Gao in Journal of Human Lactation
Supplemental Material
sj-docx-3-jhl-10.1177_08903344221088789 – Supplemental material for A Comparison of the Timing of Hand Expressing of Human Milk With Breast Massage to Standard Care for Mothers of Preterm Infants: An Exploratory Pilot Using a Randomized Controlled Design
Supplemental material, sj-docx-3-jhl-10.1177_08903344221088789 for A Comparison of the Timing of Hand Expressing of Human Milk With Breast Massage to Standard Care for Mothers of Preterm Infants: An Exploratory Pilot Using a Randomized Controlled Design by Loretta A. Anderson, Sue Kildea, Nigel Lee, Kathryn Kynoch and Yu Gao in Journal of Human Lactation
Supplemental Material
sj-docx-4-jhl-10.1177_08903344221088789 – Supplemental material for A Comparison of the Timing of Hand Expressing of Human Milk With Breast Massage to Standard Care for Mothers of Preterm Infants: An Exploratory Pilot Using a Randomized Controlled Design
Supplemental material, sj-docx-4-jhl-10.1177_08903344221088789 for A Comparison of the Timing of Hand Expressing of Human Milk With Breast Massage to Standard Care for Mothers of Preterm Infants: An Exploratory Pilot Using a Randomized Controlled Design by Loretta A. Anderson, Sue Kildea, Nigel Lee, Kathryn Kynoch and Yu Gao in Journal of Human Lactation
Footnotes
Authors’ Note
This pilot RCT was registered (ACTRN12617000769381) with Australian New Zealand Clinical Trials Registry on May 25, 2017.
Author contribution(s)
Disclosures and Conflicts of Interest
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: We would like to disclose that the first author undertook this study as a student of a Doctor of Philosophy degree through the University of Queensland.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant provided by The Mater Foundation under the Betty McGrath Fellowship Scheme.
Supplemental Material
Supplementary Material may be found in the “Supplemental material” tab in the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.