
Abstract
Background:
Physical distancing associated with the COVID-19 pandemic may lead to suboptimal maternal mental health, social support after birth, and infant feeding practices.
Research Aims:
To compare breastfeeding prevalence in participants who were pregnant at a time when strict physical distancing measures were imposed in Fortaleza, the capital of Ceará state, Brazil, with the pre-pandemic breastfeeding levels, and to assess the association of breastfeeding prevalence with maternal common mental disorders, and sociodemographic and health predictors.
Method:
A cross-sectional prospective two-group comparison design using two population-based surveys was carried out in Fortaleza before and after the pandemic. Participants (n = 351) who had a live birth in Fortaleza in July or August 2020, and participants (n = 222) who had a child younger than 12 months in 2017 were surveyed. Crude and adjusted multinomial logistic regressions with robust variance were used to estimate risk ratios and 95% confidence intervals (CI).
Results:
Similar prevalence of exclusive breastfeeding were observed in 2021 (8.1%) and 2017 (8.5%; p = .790). An increase in predominant (2.2% vs. 13.4%; p < .001) and a decrease in complementary breastfeeding (64.0% vs. 48.4%; p = .037) was observed in 2021, compared to 2017. The prevalence of maternal common mental disorders also increased in 2021 (17.6% vs. 32.5%, p < .001). No statistically significant associations were found between breastfeeding patterns, maternal common mental disorders, and other predictors in 2017 or 2021.
Conclusions:
Participants who delivered during the COVID-19 pandemic delayed solid foods introduction and breastfed predominantly longer than participants during the pre-pandemic period. While common mental disorders significantly increased, they were not associated with differences in breastfeeding.
Keywords
Key Messages
Little is known regarding the influence that the COVID-19 pandemic has had on breastfeeding patterns, especially in developing countries.
In Fortaleza, Northeastern Brazil, no difference between pre and during the pandemic exclusive breastfeeding prevalence was observed.
There was a decrease in complementary breastfeeding, and predominant breastfeeding increased during the COVID-19 pandemic.
Maternal postpartum common mental disorders increased during the COVID-19 pandemic.
Background
Coronavirus disease (COVID-19) is caused by a novel virus, SARS-CoV-2 (Severe Acute Respiratory Syndrome Coronavirus 2), first detected in China in late 2019. Although the first COVID-19 case in Brazil was officially reported in February 2020, there is evidence that SARS-CoV-2 had been circulating undetected in the country since December 2019 (Stringari et al., 2021; Kerr et al., 2020). The virus rapidly spread through Brazil (Candido et al., 2020; Castro, Gurzenda et al., 2021), triggering varied local responses that included some form of physical distancing, with few locations imposing lockdowns (Barberia et al., 2020).
As of January 10, 2022, 22 months after COVID-19 was declared a pandemic, there have been 305,914,601 confirmed cases of COVID-19, with 5,486,304 deaths reported worldwide (World Health Organization [WHO], 2021). Brazil, one of the countries most affected by the pandemic, accounts for over 7% of the global COVID-19 cases and 11% of global COVID-19 deaths (WHO, 2021), although its population represents 2.7% of the worldwide total (United Nations, 2019). Among the social and health consequences of COVID-19 in Brazil are the reduction of life expectancy (Castro, Kim et al., 2021), disruption of primary care (Lotta et al. 2020), deterioration of health conditions (Barone et al., 2020), and an increase in mental health disorders (Ornell et al., 2020; Pfefferbaum & North, 2020).
Common mental disorders (CMD) associated with pregnancy and the postpartum period include depression and anxiety (WHO, 2017). Before the COVID-19 pandemic, the prevalence of CMD increased in low- and middle-income countries, reaching 16% to 30% during pregnancy (Jha et al., 2018). Maternal mental health has been associated with impaired child care and has been linked to reduced breastfeeding initiation and early cessation (Dias & Figueiredo, 2015; Pope & Mazmanian, 2016). Breastfeeding (BF) has known beneficial effects on an infant’s development and health and has been associated with decreased morbidity, hospital admissions, and mortality due to infectious diseases (Victora et al., 2016; WHO, 2000). Thus, an increase in maternal mental disorders, as a result of the COVID-19 pandemic, could lead to negative consequences for both maternal and infant health. In fact, being pregnant and delivering an infant during the pandemic has been associated with increased anxiety in women in Italy (Saccone et al., 2020), with a growing number of authors showing similar associations in their studies (Mappa et al., 2020; Nowacka et al., 2021; Preis, 2020).
Researchers who conducted a review of the influence of COVID-19 on breastfeeding practices and maternal mental health showed contrasting results based on the experience reported in six countries in Europe, North America, Western Asia, and Australia (Pacheco et al., 2021). On the one hand, positive BF outcomes were associated with participants having more time at home due to pandemic-related closings. On the other hand, negative BF outcomes were associated with participants who reported having low social and professional support for breastfeeding (Pacheco et al., 2021).
Our study contributed to this discussion and aimed to compare breastfeeding prevalence in participants who were pregnant at a time when strict physical distancing measures were imposed in Fortaleza, the capital of Ceará state, Brazil, with pre-pandemic levels, and to assess the association of breastfeeding prevalence with maternal common mental disorders, and sociodemographic and health predictors.
Methods
Research Design
A cross-sectional prospective two-group comparison design using two population-based surveys was conducted before and during the COVID-19 pandemic, respectively, facilitating the comparison of BF prevalence during both periods. The analyzed data were collected prospectively by the authors both before and during the pandemic. Both surveys were approved by the National Research Ethics Committee in Brazil (Numbers 31190420.4.0000.5054 and 73516417.4.0000.5049).
Setting and Relevant Context
We chose Fortaleza, the fifth largest city in Brazil and capital of the northeastern state of Ceará (CE), because it was one of the few cities in Brazil that imposed a strict lockdown (from March 15 to May 5, 2020) as a measure to contain the spread of COVID-19, and since data from before the pandemic were available for the city. Fortaleza is located in the northeastern region of Brazil. In 2020 it had an estimated population of approximately 2.7 million inhabitants, and a human development index (HDI) of 0.754 (Instituto Brasileiro de Geografia e Estatística, 2020). The city is divided into 121 neighborhoods, distributed in six administrative districts numbered 1 to 6 (Supplementary Figure 1) (Instituto de Planejamento de Fortaleza [IPLANFOR], 2020). These administrative districts have distinct socioeconomic characteristics. For example, nine out of the 10 neighborhoods with the highest HDIs in Fortaleza are located in Administrative District 2. In contrast, Districts 6 and 5 comprise neighborhoods with the lowest HDI (six out of the 10 lowest HDI are in District 5; IPLANFOR, 2020 ; Prefeitura de Fortaleza, 2014).
In Brazil, the public health care system offers universal and free of charge coverage for the whole population. All women can access the health care services during the pre- and postpartum period, where BF is encouraged and recommended. According to the National Study of Infant Food and Nutrition (Estudo Nacional de Alimentação e Nutrição Infantil [ENANI]), from 2019 the prevalence of exclusive breastfeeding (EBF) in the Northeast region of Brazil was 57.3% in the first 4 months and 39.0% in the first 6 months of infants’ lives (Universidade Federal do Rio de Janeiro, 2019).
Sample
Women who lived in Fortaleza and had a child aged 12 months or less were eligible to participate. For the COVID period, we used data from the Iracema-COVID, a longitudinal study, was designed to evaluate the health status of mothers who were pregnant during the COVID-19 pandemic and their offspring, and to be representative of Fortaleza at the administrative district level. Mothers who lived in Fortaleza, gave birth at public hospitals (which included 75% of all births) in July and August 2020, and had complete address information were eligible. In the present study, we used data from participants at the 6 months’ postpartum interview. Women who gave birth in private hospitals were deemed ineligible due to not having their contact information available in public records. Survey participants were sampled from the Live Birth Information System (Sistema de Informações sobre Nascidos Vivos [SINASC]).
For the Iracema-COVID survey, the sample size (n = 352) was calculated to detect a prevalence of 46% of maternal CMD (Machado et al., 2021), with a margin of error of 5%, and a 95% confidence interval (CI). Out of 4,840 mothers who gave birth in July and August 2020, 3,567 were eligible for the study. Of those, 352 women were randomly selected using the GSAMPLE module in Stata (Version 16) and 351 participants started and completed this survey.
The second study data used for our pre-COVID comparison group was the Maternal and Child Health Survey in Ceará (Pesquisa de Saúde Materno Infantil do Ceará [PESMIC]), a state-wide, repeated, cross-sectional survey that has been carried out in Ceará roughly every 5 years since 1987 (Correia et al., 2019). The 2017 PESMIC recruited women aged 18–49 and children aged 0–72 months (only households with children were included). A cluster sampling approach was used based on the Brazilian Institute of Geography and Statistics (IBGE) census tracts, with stratification between Fortaleza (the state capital) and the rural areas (Correia et al., 2019). PESMIC’s original sample size calculations considered infant mortality rates of 10% at the time of the first survey in 1987 and a level of significance of 5%, aiming to find 4,000 children, which would provide an absolute precision of 1 (Correia et al., 2019). Of the 3,200 families included in the 2017 PESMIC, 900 were representative of Fortaleza, and 222 (24.7%) mothers aged 18–49 years had children under 12 months of age at the time of the interview. To facilitate comparisons with the Iracema-COVID survey, those 222 mothers were included in the present analysis.
Measurement
To assess possible factors associated with BF practices, maternal and child characteristics were selected through a conceptual model (Figure 1) elaborated from a review of the current literature (Boccolini et al., 2015; Cohen et al., 2018; Santana et al., 2018). The model has four levels that indicate the hierarchical association of the included predictors with breastfeeding. Supplementary Table 1 describes the instruments used to collect the predictor variables at each survey.
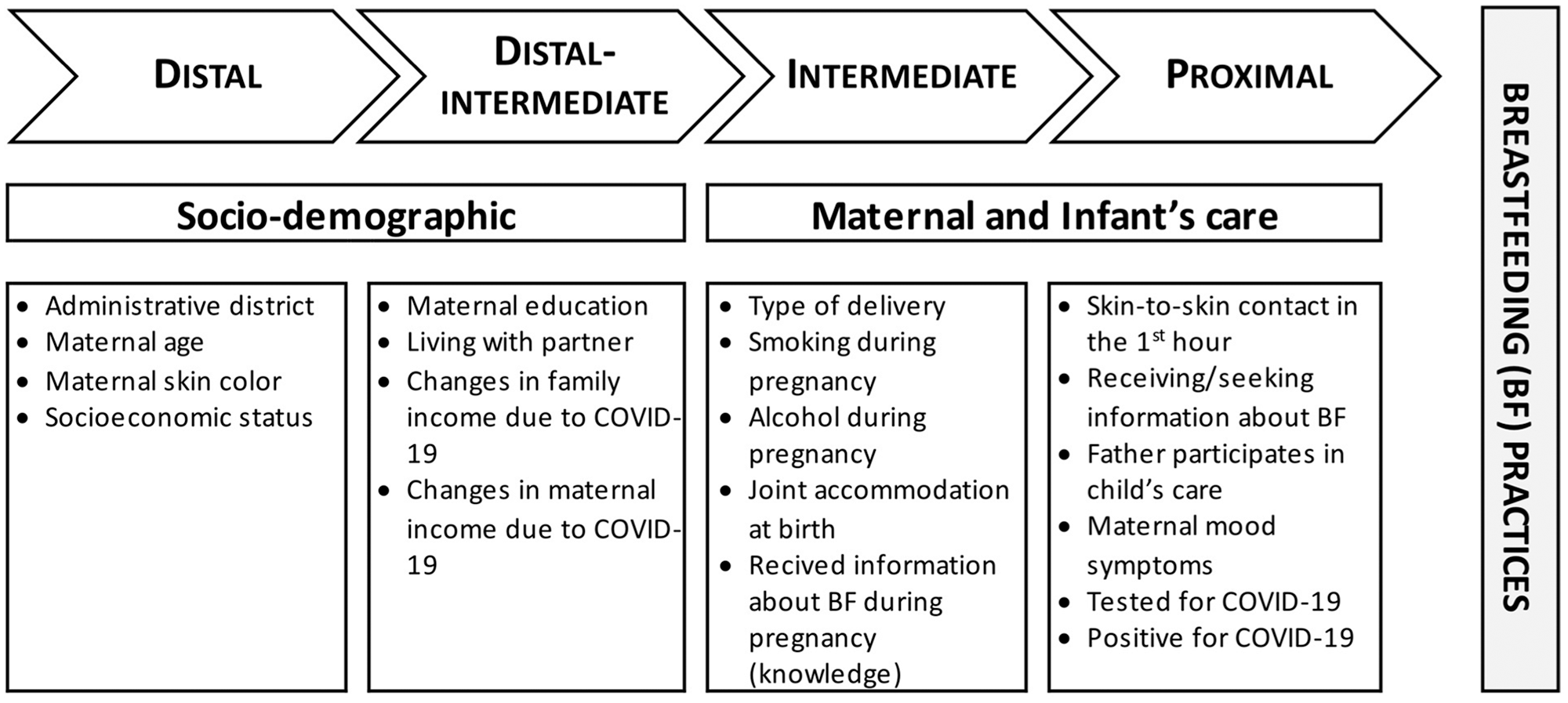
Hierarchical Theoretical Model of Breastfeeding and its Possible Predictors.
Socioeconomic status was constructed based on the Brazilian Economic Classification Criteria (Critério de classificação econômica Brasil [(CCEB]; Associação Brasileira de Empresas de Pesquisa [ABEP], 2021). This index is summarized into five socioeconomic strata and an estimate of the monthly household income has been provided for each (monthly income in U.S. dollars was calculated using the exchange rate of January 4, 2022: 1 US$ dollar = 5.68 Reais). The five categories were: A (monthly income of US$ 4,004.15), B1 (US$ 1,899.39), B2 (US$ 1,007.35), C1 (US$ 562.38), C2 (US$ 333.62), and D/E (US$ 151.83; ABEP, 2021). For the analyses conducted here, we grouped those into three categories: A/B, C, D/E. Administrative Districts of Residence 3 and 4 were grouped together given their similar socioeconomic characteristics and considering the lower numbers of mothers.
Maternal CMD were assessed by the Self Report Questionnaire (SRQ-20), a 20-item self-report screening tool developed by the WHO aimed at detecting psychological distress (Beusenberg & Orley, 1994). The SRQ-20 has been validated for application with the Brazilian population, using a cut-off point of eight or more as an indicator of morbidity with an 83% sensitivity and 80% specificity (Mari & Williams, 1986).
Both the 2020 and 2017 surveys collected information about BF practices. The Iracema-COVID asked whether the child was being breastfed and/or if any other food or liquid was being offered. PESMIC gathered information about BF and the age of the child when liquids, formula, and solid foods were introduced. We adopted the WHO (2009) definition to categorize BF patterns: (i) exclusive BF: no other food or drink (not even water) being administrated to the child, other than human milk, except for medications and vitamins; (ii) predominant BF: human milk and water, water-based drinks, and fruit juice; (iii) complementary BF: human milk and any food or liquid including non-human milk and formula; and (iv) bottle feeding: any food or liquid including non-human milk and formula. Since a small number of participants had exclusive and predominant BF, we combined these two categories. Therefore, the analyses in this study utilized three infant feeding patterns: (1) exclusive/predominant BF (EPBF); (2) complementary BF (CBF); and (3) bottle-feeding.
Data Collection
Iracema-COVID survey data were collected by trained researchers between January 8 and June 30, 2021. Due to restrictions imposed by the COVID-19 pandemic, all data were collected remotely through telephone interviews. In the PESMIC survey, data were collected between August and November, 2017. All interviews were performed by field researchers working in pairs. Verbal informed consent was obtained from all participants. Data from both studies were stored in encrypted format, maintaining participants’ confidentiality, as only anonymized data were analyzed.
Data Analysis
Descriptive statistics of maternal characteristics were obtained from each survey. Tests of differences between the characteristics of the two surveys were carried out using a chi-square test. For each survey, crude and adjusted multinomial logistic regressions with robust variance were performed to estimate risk ratios, and their respective 95% CI, for the associations of BF patterns with the investigated predictors. Multicollinearity was assessed through the Variance Inflation Factor (VIF) with a cut-off value of 10. The final multivariable model was selected based on the Log-likelihood and the Akaike information criterion (AIC). Statistical significance was considered at p value < .05. Statistical analyses were performed in STATA (Version 16.1).
Results
Characteristics of the Sample
In 2017, 44.3% (n = 98) of the participants were aged 18–24, over 90% came from socioeconomic classes C, D, and E, and 58.1% (n = 129) had 1–9 years of formal education (Table 1). Compared to the year 2017, in 2021 there was an increase in the proportion of participants aged 25–29 (p < .001) and a reduction in those aged 18–24 (p < .001). In 2021, participants had a higher prevalence of alcohol consumption compared to 2017 (p < .001). Our analysis did not find an association between income variations due to COVID-19 and drinking habits. In the 2021 sample, a lower prevalence of having received information about BF (p < .001) was found. In 2021, 34.5% (n = 121) participants reported avoiding seeking medical help during pregnancy, and 47.9% (n = 168) had at least one medical appointment canceled during the pandemic. Even though 85% (n = 299) of this sample had the recommended six or more prenatal appointments.
Participants’ Characteristics Grouped by Pre/Post COVID Periods (N = 573).
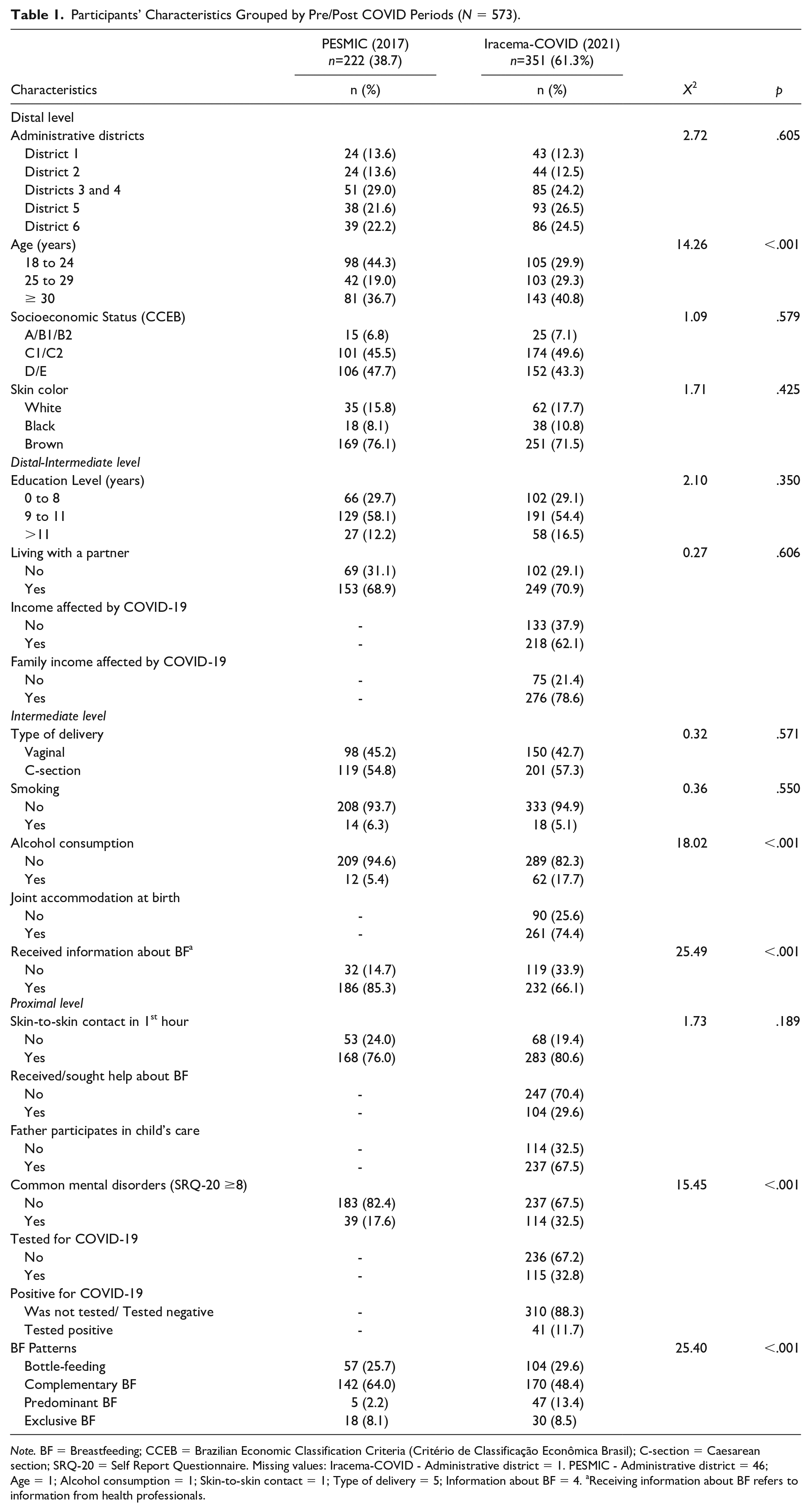
Note. BF = Breastfeeding; CCEB = Brazilian Economic Classification Criteria (Critério de Classificação Econômica Brasil); C-section = Caesarean section; SRQ-20 = Self Report Questionnaire. Missing values: Iracema-COVID - Administrative district = 1. PESMIC - Administrative district = 46; Age = 1; Alcohol consumption = 1; Skin-to-skin contact = 1; Type of delivery = 5; Information about BF = 4. aReceiving information about BF refers to information from health professionals.
Common Mental Disorders
The frequency of CMD was 17.6% (n = 39). In 2021, 40.8% (n = 143) of the participants were aged 30 years or older, and most were from the lower socioeconomic classes (C, D, and E) and had 9–11 years of education (54.4%, n = 191). CMD frequency was 32.5% for participants who delivered during the pandemic. In addition, 62.1% (n = 218) and 78.6% (n = 276) of interviewed participants in 2021 observed a decline in their income and overall family income, respectively, due to the COVID-19 pandemic. A third of our sample had previously been tested for COVID-19 and 12% (n = 41) of those had positive results (Table 1).
The prevalence of maternal CMD increased substantially from 2017 to 2021 (p < .001). However, there was an increase in PBF in 2021 (p < .001), and a decrease in CBF (p = .037; Table 1). Similar results were found when modeling the combined data from both studies using wave as an independent variable (Supplementary Table 2).
Participants who were pregnant during the period of lockdown in Fortaleza, and who delivered their babies in 2020, had a decrease of about 15% in the prevalence of CBF and an 11% increase in PBF prevalence compared to participants who had delivered babies 4 years earlier. We observed an increase of 16 percentage points in the prevalence of CMD 6 months to a year after delivery between 2017 and 2021.
Breastfeeding
Regarding feeding patterns, EBF frequency was 8.1% in 2017 and 8.5% in 2021. No significant differences in EBF were observed between the two surveys (p = .790). We had a reduction in the proportion of participants who offered supplementary milk or food to their infants and an increase in those offering EPBF. In the univariable (Tables 2 and 4) and adjusted (Tables 3 and 5) multinomial logistic regressions no statistically significant differences between BF patterns and the predictors, both before and during the COVID-19 pandemic, were observed. Although no association was found among CMD measured by the SRQ-20 scale, we performed analyses individually including each of the 20 items on the questionnaire (Supplementary Tables 3 and 4). In 2021, BF patterns were only associated with the “daily work suffering” item (EPBF RR 3.08, 95% CI [1.18, 8.06]), while in 2017 no statistically significant associations were observed.
Univariable Association of Breastfeeding Patterns and Possible Risk Factors (Iracema-COVID -2021).
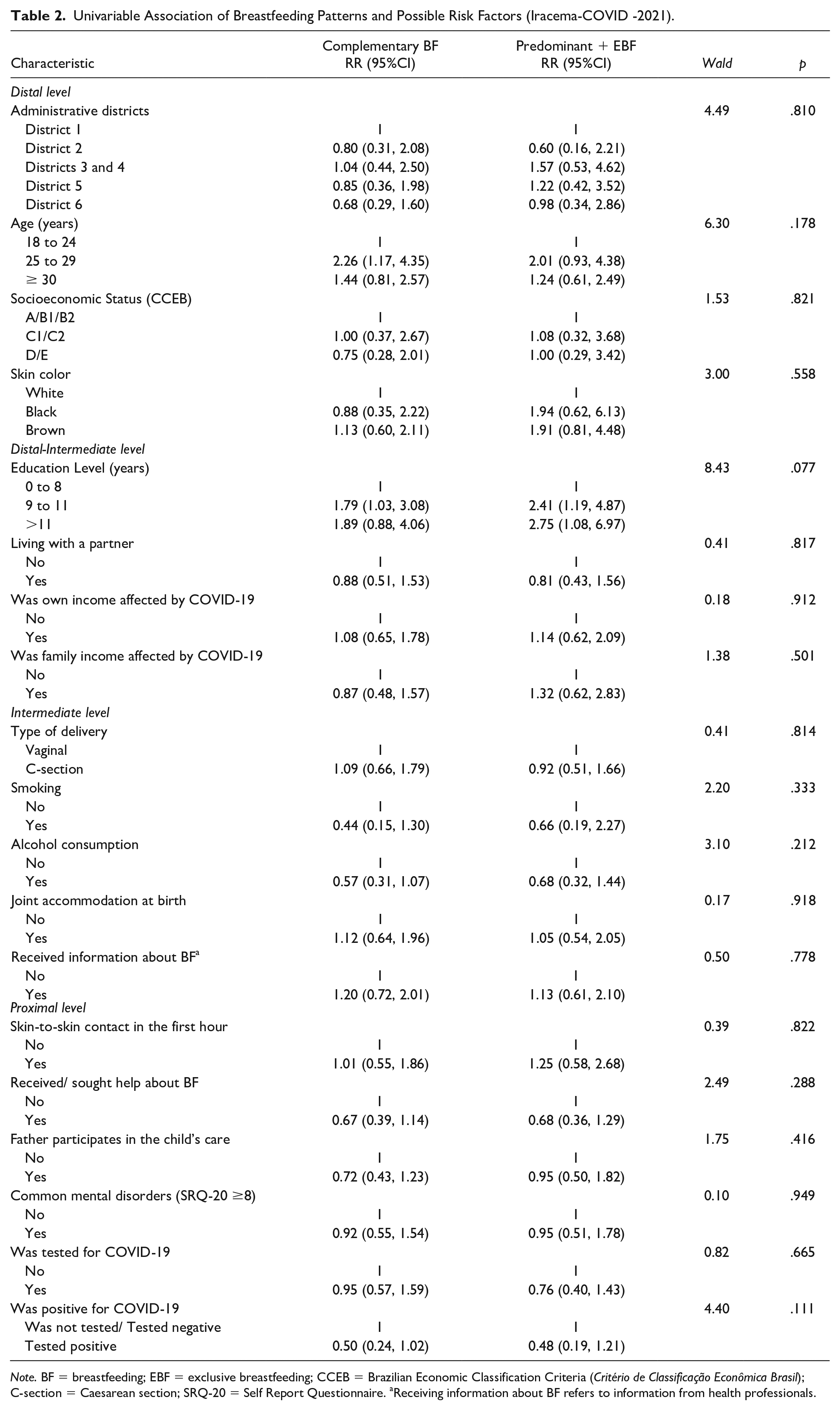
Note. BF = breastfeeding; EBF = exclusive breastfeeding; CCEB = Brazilian Economic Classification Criteria (Critério de Classificação Econômica Brasil); C-section = Caesarean section; SRQ-20 = Self Report Questionnaire. aReceiving information about BF refers to information from health professionals.
Multivariable Association of 2021 Breastfeeding Patterns and Possible Risk Factors (Iracema-COVID -2021).
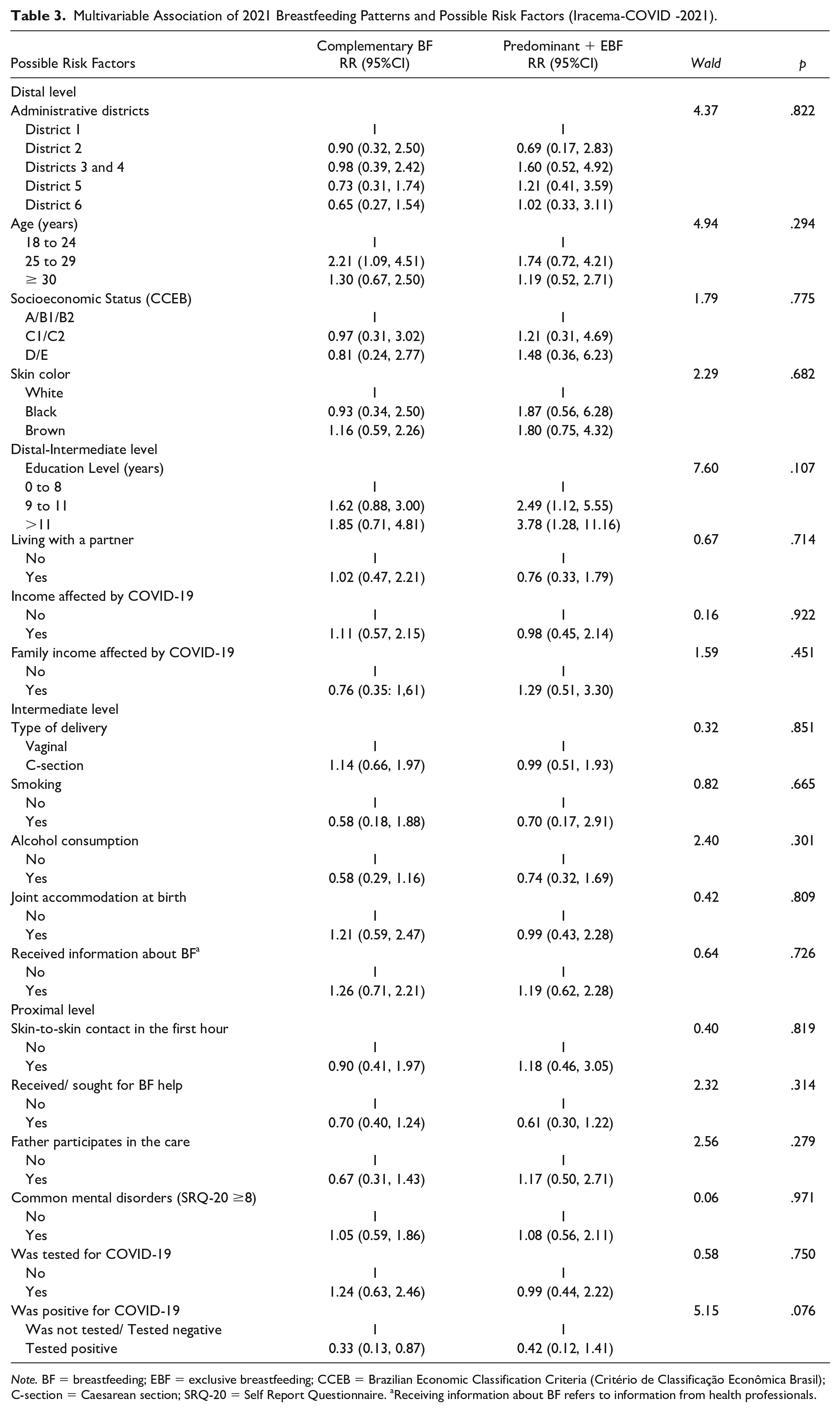
Note. BF = breastfeeding; EBF = exclusive breastfeeding; CCEB = Brazilian Economic Classification Criteria (Critério de Classificação Econômica Brasil); C-section = Caesarean section; SRQ-20 = Self Report Questionnaire. aReceiving information about BF refers to information from health professionals.
Univariable Association of Breastfeeding Patterns and Possible Risk Factors (PESMIC-2017).
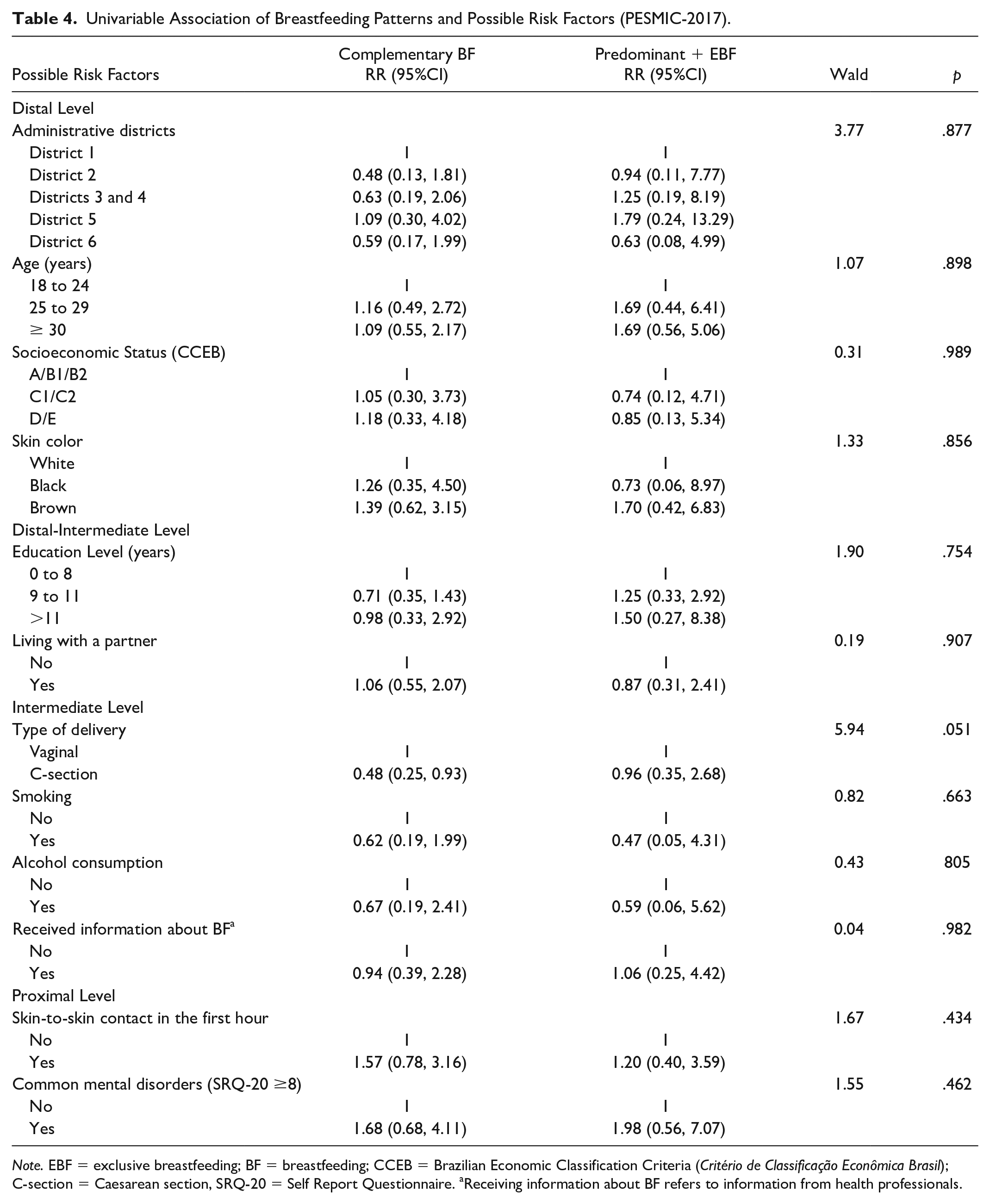
Note. EBF = exclusive breastfeeding; BF = breastfeeding; CCEB = Brazilian Economic Classification Criteria (Critério de Classificação Econômica Brasil); C-section = Caesarean section, SRQ-20 = Self Report Questionnaire. aReceiving information about BF refers to information from health professionals.
Multivariable Association of Breastfeeding Patterns and Possible Risk Factors (PESMIC-2017).
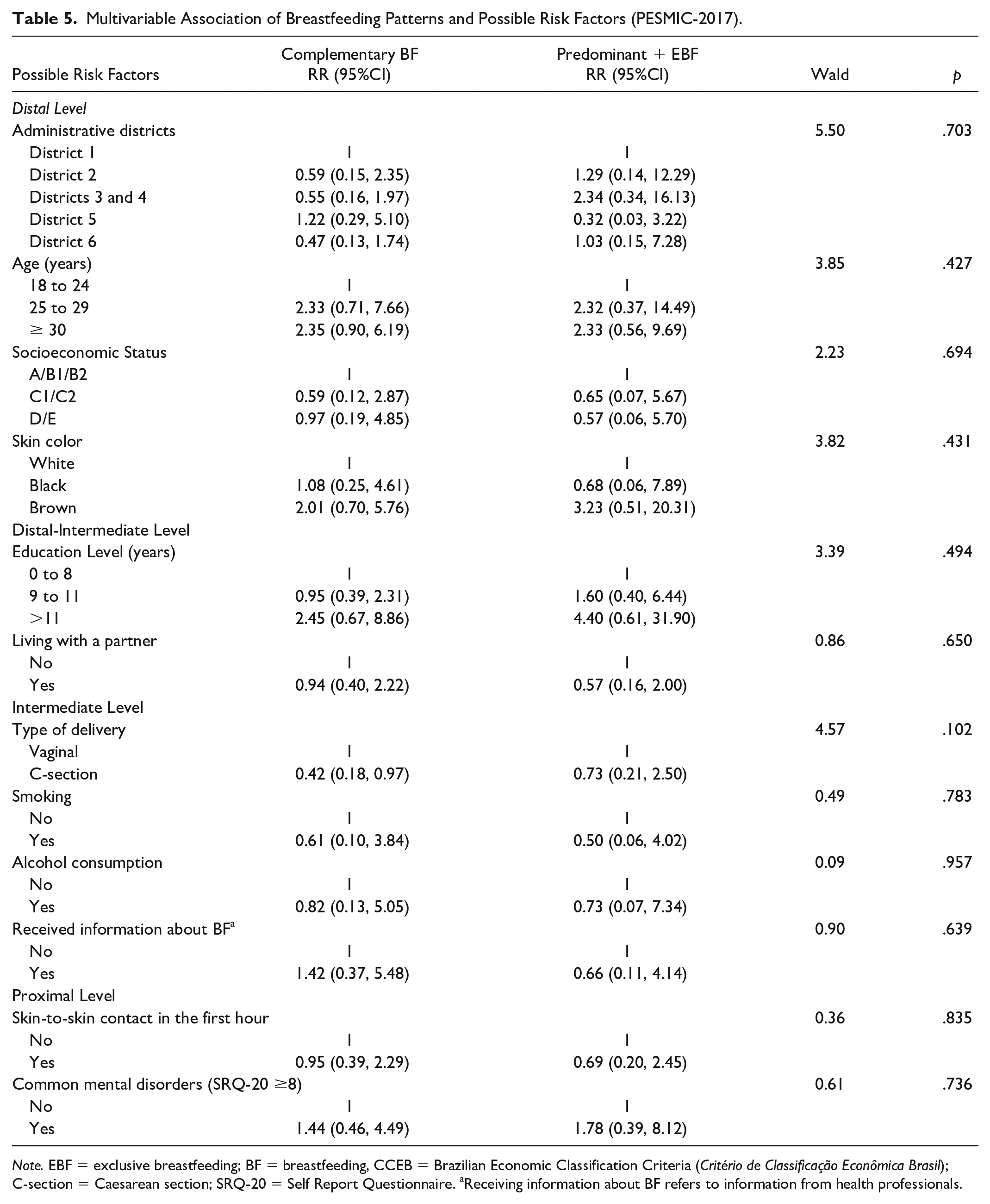
Note. EBF = exclusive breastfeeding; BF = breastfeeding, CCEB = Brazilian Economic Classification Criteria (Critério de Classificação Econômica Brasil); C-section = Caesarean section; SRQ-20 = Self Report Questionnaire. aReceiving information about BF refers to information from health professionals.
Discussion
Despite conflicting information about the risks and benefits of BF in the context of COVID-19, which was publicized at the beginning of the pandemic (Vu Hoang et al., 2020), we found no evidence that participants in our study changed patterns of BF initiation during the COVID-19 pandemic. Our results differed from previous researchers who reported a decrease in the proportion of EBF 90 days to a year after delivery during the COVID-19 pandemic (Latorre et al., 2021; Pacheco et al. 2021; Zanardo et al., 2021). However, those studies were exclusively from high-income countries. In Fortaleza, we showed that over three-quarters of families had their income reduced during the pandemic, which could have resulted in dietary restrictions. Indeed, food insecurity in the state of Ceará increased by 15% during the COVID-19 pandemic (Rocha et al., 2021). Therefore, food insecurity may have overcome the eventual fear of disease transmission through human milk and influenced participants to postpone the introduction of solid foods into their infant’s diet. In Brazil, a higher prevalence of BF has been found among food-insecure families of children aged 12–24 months (Gomes & Goubert, 2012). However, this result has not been observed in developed countries where inverse or no associations between food insecurity and breastfeeding initiation and duration were reported (Dinour et al., 2020; Orr et al., 2018). Similar to previous findings (Pacheco et al., 2021), no association of BF patterns with COVID-19 related exposure was found.
Even though participants included in the Iracema-COVID survey were older than those interviewed in 2017 and older maternal age has been associated with higher breastfeeding prevalence (Santana et al., 2018), we observed a reduction in any breastfeeding in the sample of participants who delivered during the COVID-19 pandemic compared to those who gave birth in 2017 (74.3% [n = 165] in 2017 vs. 70.4% [n = 247] in 2021).
In 2021, our participants received less information about BF while pregnant. The quality of the consultations might have been affected due to pandemic protocols to avoid or reduce the risk of infection while attending health facilities.
The increase in the prevalence of maternal CMD in 2021, compared to 2017, could reflect physical distancing measures associated with the stress of going through a pandemic. Only a few researchers have focused on the influences of physical distancing on maternal health; they have reported a substantial increase of almost six times in maternal depression and two times in anxiety risk during the COVID-19 restrictions (Davenport et al., 2020; Loret de Mola et al., 2021). Childbearing is a major life event with a profound influence on mental health (Geller, 2004). Combined with the after-birth changes caused by a rapid hormonal alteration (Trifu et al., 2019), and all adaptations needed to care for a newborn child, the gestational and puerperium periods are of high vulnerability for women to develop CMD, and that could have been exacerbated during the pandemic.
Participants who reported suffering feelings towards their work were three times more likely to be exclusively/predominantly breastfeeding their infants. Work-related challenges during the COVID-19 pandemic included adapting to home office practices that could make them more available for BF, but also more stressed during the day, having to manage work and house chores at the same time. Working from home has been associated with higher stress and mental suffering when there is no organizational support from companies (Oakman et al., 2020), which is likely to be the case for many companies in Brazil.
The main strength of this study was the use of data representative for the city of Fortaleza, before and during COVID-19, enabling a comparative analysis. Also, to the best of our knowledge, this was the first study in Brazil to assess the possible influence of the COVID-19 pandemic on breastfeeding patterns. In the future, researchers should investigate the long-term influence of the COVID-19 pandemic on breastfeeding patterns and how maternal mental health might have influenced breastfeeding initiation and continuation.
Limitations
Given that only records from public hospitals were included, participants with higher incomes may have been underrepresented in the sample. The higher prevalence of alcohol consumption observed in 2021 might be due to methodological differences in data collection between the two surveys. While in 2017 the survey specifically asked about drinking alcohol during pregnancy, in 2021 the participant was asked whether she drank and when she had started (before or during the pandemic). Thus, higher proportions of alcohol consumption could reflect current consumption rather than consumption during pregnancy. Also, the COVID-19 pandemic has been associated with an increase in occasional alcohol consumption in Latin American countries, including Brazil (Garcia-Cerde et al., 2021). The evaluation of CMD through a self-report instrument could have introduced self-report and social desirability biases. Lastly, the cross-sectional design does not allow the assessment of causality.
Conclusion
Our findings suggested that participants who were pregnant and delivered babies during the COVID-19 pandemic chose to delay solid foods introduction and offered human milk exclusively or predominantly for longer, compared to the pre-pandemic period. While maternal CMD had an important increase during the same period, no significant association with breastfeeding practices was found. These findings highlight the need for public policies and clinical protocols that provide updated infant feeding guidelines during the COVID-19 pandemic as well as mental health monitoring after delivery.
Supplemental Material
sj-docx-1-jhl-10.1177_08903344221101874 – Supplemental material for Breastfeeding Practices Before and During the COVID-19 Pandemic in Fortaleza, Northeastern Brazil
Supplemental material, sj-docx-1-jhl-10.1177_08903344221101874 for Breastfeeding Practices Before and During the COVID-19 Pandemic in Fortaleza, Northeastern Brazil by Simone Farías-Antúnez, Luciano Lima Correia, David Augusto Batista Sá Araújo, Ana Luiza Penna, Geziel dos Santos de Sousa, Anamaria Cavalcante e Silva, Jocileide Sales Campos, Hermano Alexandre Lima Rocha, Camila Machado de Aquino, Marcia C. Castro and Márcia Maria Tavares Machado in Journal of Human Lactation
Footnotes
Author contribution(s)
Disclosures and Conflicts of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Iracema-COVID was funded by Fundação Maria Cecilia Souto Vidigal, and by the Medical School of the Federal University of Ceará. SFA received support from the David Rockefeller Center for Latin American Studies, Harvard University
Supplemental Material
Supplementary Material may be found in the “Supplemental material” tab in the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.