
Abstract
Introduction:
One of the obstacles to breastfeeding is the false beliefs in society about human milk and breastfeeding.
Research Aim:
The aim of this study is to develop the “Human Milk and Breastfeeding Myths Scale” and test its validity and reliability.
Methods:
This methodological study included 326 participants (individuals in the last trimester of pregnancy and breastfeeding individuals with infants aged 0–2 years) recruited from two public hospitals in Istanbul, Turkey. Data were collected using the Descriptive Participant Data Form and the Human Milk and Breastfeeding Myths Scale. Reliability analyses included internal consistency and a test–retest assessment conducted at a 2-week interval (n = 34). The study was reported in accordance with the STROBE guidelines, and a pilot test was conducted with 10 participants.
Results:
The draft scale initially consisted of 32 items and was evaluated by experts. Following exploratory factor analysis, eight items with low factor loadings were removed, and content validity was supported using the Lawshe technique. The final 24-item scale demonstrated a structure with two factors with eigenvalues greater than 1 and a dominant first factor, with good internal consistency (α = .86).
Conclusion:
The Human Milk and Breastfeeding Myths Scale demonstrated acceptable validity evidence and good reliability, and may be used to assess beliefs related to breastfeeding myths.
Keywords
Introduction
Human milk, the most suitable food for the healthy growth and development of the newborn, is a unique living substance owing to its antimicrobial, anti-inflammatory, and immunoregulatory features that support immune system development (Meek & Noble, 2022). Organizations such as the World Health Organization (WHO) and the United Nations International Children’s Fund (UNICEF) recommend initiation of breastfeeding within the first hour of life, exclusive breastfeeding with human milk for the first 6 months, and continued breastfeeding up to 2 years of age or beyond. In line with these recommendations, the WHO has identified its global nutrition target for 2025 as increasing the rate of exclusive breastfeeding during the first 6 months of life to at least 50% (Drohan & Faustini, 2019; WHO, 2014).
The reported global rate of exclusive breastfeeding for the first 6 months is approximately 38%, while in Turkey this rate is 41% (Turkey Demographic and Health Survey [TDHS], 2018). These figures indicate that exclusive breastfeeding rates in both global and national contexts remain below targeted levels. Breastfeeding is not only a common infant feeding practice but is also a social and cultural phenomenon. Historical evidence indicates that human milk has been the primary source of nutrition supporting healthy growth and development of newborns for centuries (Timurturkan, 2020). Archaeological findings suggest that breastfeeding held ritual significance in prehistoric societies and served as the sole source of infant nutrition, with female figurines frequently symbolizing fertility and breastfeeding (Dixson & Dixson, 2011; Yüksel & Yılmaz, 2021).
When barriers to breastfeeding are examined across historical and contemporary contexts, previous studies have identified, as major barriers, maternal beliefs, the influence of significant others on infant feeding decisions, and sociocultural factors (Balogun et al., 2015). In Turkey, misconceptions related to milk sufficiency, colostrum, breastfeeding frequency, and maternal diet are commonly reported and may contribute to early supplementation and discontinuation of exclusive breastfeeding. Consistent with this perspective, previous studies have reported a close association between breastfeeding barriers and myths that are widely prevalent in society (Gölbaşı et al., 2018).
In ancient Greece, the word myth referred to orally transmitted stories (Batuk, 2009), and societies used myths as values that protect and transmit culture. In prehistoric times, communities accepted myths as tools through which certain beliefs were established within society (Yılar, 2005). In the modern world, however, the word “myth” is used more often for negative behavior patterns (Batuk, 2009).
A study conducted in Turkey reported that myths are common among individuals who give birth, that educational level significantly influences belief in these myths, and that widespread beliefs about human milk and breastfeeding constitute barriers to exclusive breastfeeding, particularly during the first 6 months of life (Gölbaşı et al., 2018). Alongside this, beliefs, attitudes, and behaviors concerning breastfeeding may vary according to culture. Considering these findings, identifying prevalent breastfeeding myths and developing a culturally grounded scale were deemed necessary. This scale may inform future interventions aimed at addressing breastfeeding myths among breastfeeding participants.
Key Messages
Breastfeeding myths are a cultural phenomenon that impact breastfeeding success and sustainability.
The Human Milk and Breastfeeding Myths Scale assesses the myths held by pregnant women and breastfeeding mothers about breastfeeding and helps guide interventions targeting myth-related barriers to breastfeeding.
Psychometric analyses of the scale demonstrated that the Human Milk and Breastfeeding Myths Scale has good reliability and validity.
Methods
Research Design
This methodological study was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (Vandenbroucke et al., 2014). The study was approved by the University Ethics Committee (Approval number 46.2023fbu). Permission was obtained from the Health Directorate for the hospitals where the research would be conducted (dated June 20, 2023 and November 2023).
Aim
The purpose of this study is to develop the Human Milk and Breastfeeding Myths Scale and to test its validity and reliability.
Procedure
The study procedure is shown in Figure 1.
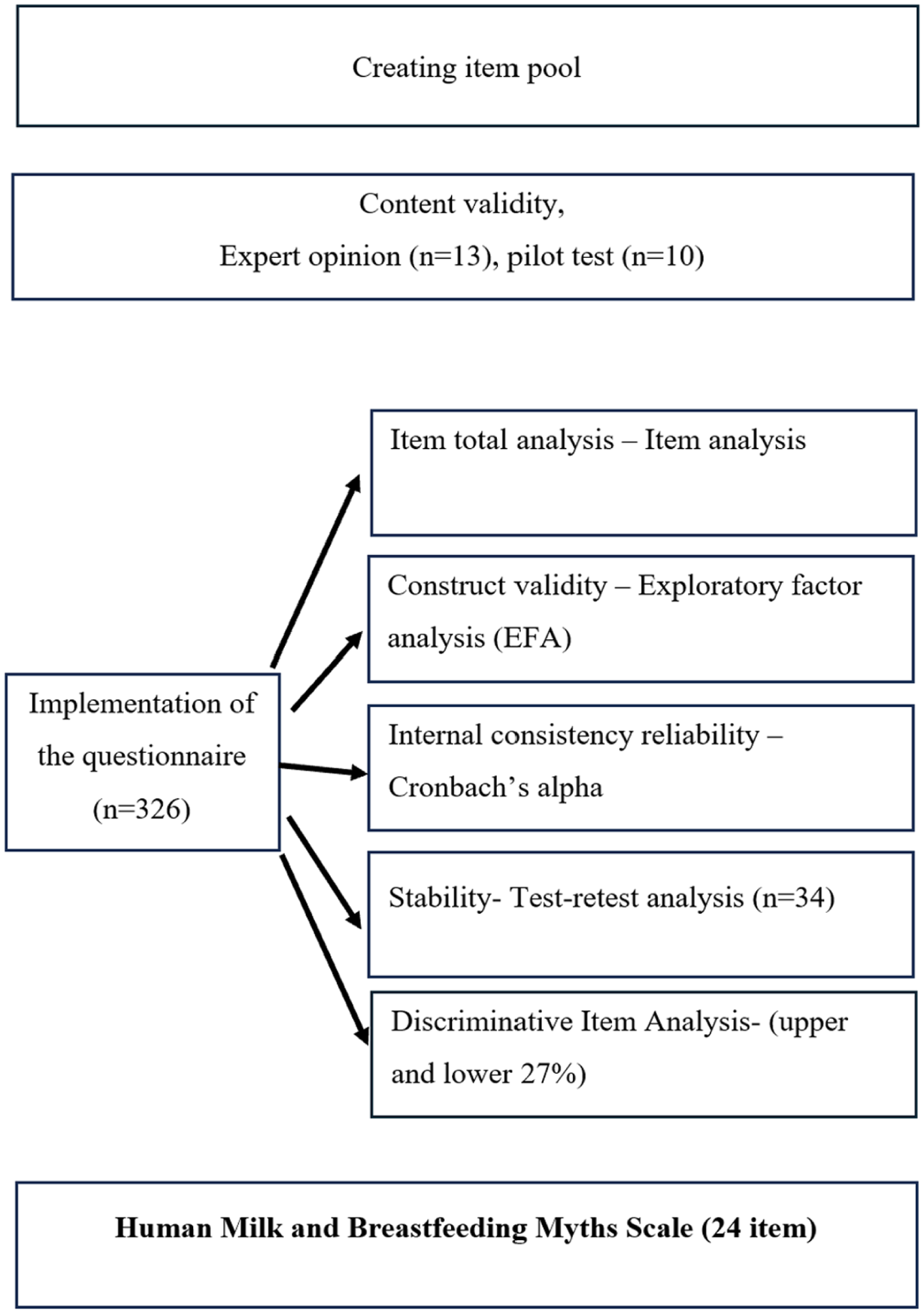
The study procedure.
Sample and Data Collection
The research population consisted of individuals who attended the child, antenatal, and postnatal clinics of Zeynep Kamil Women’s and Children’s Diseases Training and Research Hospital and Ümraniye Training and Research Hospital in Istanbul. Because the draft scale contained 32 items, it was targeted to reach a sample size amounting to five to 10 times the number of items in the draft scale (Boateng et al., 2018). The total sample reached was 326. Data were collected face-to-face by the researchers via questionnaire between February and May 2023. Inclusion criteria were being in the last trimester of pregnancy or currently breastfeeding an infant aged 0–2 years and being able to communicate in Turkish. Participants who had difficulty communicating in Turkish were excluded. All participants were Turkish-speaking and resided in Turkey.
The Scale Development Process
Creating the item pool
The item pool was created by the researchers on the basis of the previously published study entitled “Postpartum women’s beliefs about human milk and breastfeeding myths” (Gölbaşı et al., 2018 ) and other studies in the national and international literature on breastfeeding myths, false beliefs, and prejudices (Acheampong & Abukari, 2024; Aksu et al., 2011; Yelsouei & Taşğın, 2025; Yılmaz Sezer et al., 2024). As a result, the researchers independently created a pool of 32 items to be answered in a 5-point Likert-type manner.
Content Validity
The draft measurement scale was submitted for expert opinion to evaluate the relationship of the items with the intended concept, language, and meaning; the presence of similar expressions among items; and the suitability of the items to the purpose of the research. Thirteen experts were invited by e-mail to examine the draft scale, and all accepted. All experts were Turkish and fluent in Turkish. Expert opinions were obtained from academics in the fields of pediatric nursing (two experts), public health nursing (three experts), and women’s health nursing (eight experts). The Lawshe technique was used for content validity (Lawshe, 1975).
Pilot Test
After content validity, a pilot test was performed with 10 randomly selected participants in order to test the suitability and comprehensibility of the items. The participants who took part in the pilot test were not included in the main sample.
Measurement
Data were obtained by using the Participant Information Form (13 questions), which determines participants’ sociodemographic, obstetric, and breastfeeding characteristics, and the Draft Human Milk and Breastfeeding Myths Scale (32 items).
Validity and Reliability Analyses
Reliability Analyses
To determine the internal consistency of the items in the scale, Cronbach’s alpha coefficient was examined. Cronbach’s alpha generally ranges between 0 and 1, with higher values indicating greater reliability (Tavakol & Dennick, 2011; Ursachi et al., 2015). Item analysis was also conducted. According to the item–test total-score statistics, if the alpha coefficient rises when an item is removed, that item is considered to lower reliability and should be excluded. This ensures greater homogeneity of the scale (Tavakol & Dennick, 2011; Ursachi et al., 2015). In addition, item discrimination was examined by comparing the highest and lowest 27% scoring groups. Items that are correctly endorsed by high scorers and less frequently by low scorers are considered more discriminative. Test–retest reliability was assessed to show the stability of the scale over time. For intermittent measurement, it is recommended that the interval not be shorter than 2 weeks nor longer than 4 weeks (Ursachi et al., 2015).
Validity Analysis
To examine construct validity, exploratory factor analysis (EFA) was performed to observe how many sub-dimensions the scale would have and which items would cluster together.
Data Analysis
The data obtained in the study were analyzed using the SPSS (Version 28). Whether or not the scale items displayed a normal distribution was examined with the Shapiro–Wilk test, the Kolmogorov–Smirnov test, and a Q–Q plot, and it was observed that they displayed a normal distribution. Descriptive statistics, mean, and standard deviation were given for quantitative data, and frequency and percentage for qualitative data. Scale content validity was examined using the Lawshe method. For discrimination, item means for the lower and upper 27% of groups were examined. Scale reliability was evaluated using the test–retest method. An item–test total analysis was also carried out.
Results
Descriptive Findings
The Human Milk and Breastfeeding Myths Scale was administered to 326 participants, including individuals in the last trimester of pregnancy and breastfeeding participants with infants aged 0–2 years. Participants ranged in age from 18–47 years (M = 31.0, SD = 5.9). Most participants had completed primary education (63.5%), while 32.2% were university graduates. In addition, 73.3% of participants were not employed, and 85.0% reported previous breastfeeding experience.
Reliability Analyses
Item Analysis
Item–total correlations ranged from 0.22 to 0.59, and no item significantly altered the scale’s mean or variance when deleted. Therefore, no items were removed (Table 1).
Item–Total Correlations and Internal Consistency Indices of the Human Milk and Breastfeeding Myths Scale (N = 326).
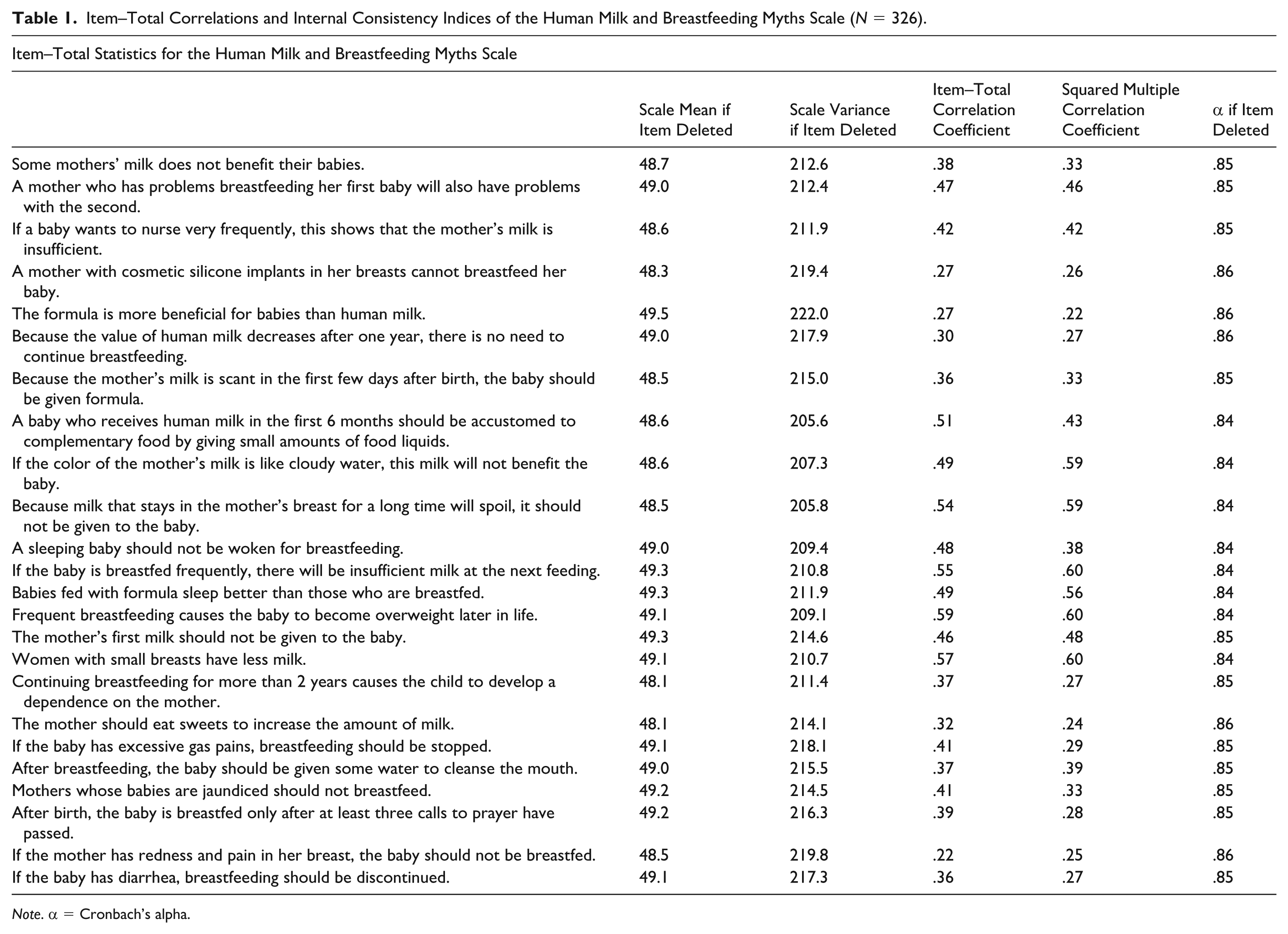
Note. α = Cronbach’s alpha.
Internal Consistency
Cronbach’s alpha was calculated to assess internal consistency. The scale was found to have a high reliability, with a total alpha of .86 (Table 2).
Internal Consistency of the Human Milk and Breastfeeding Myths Scale.
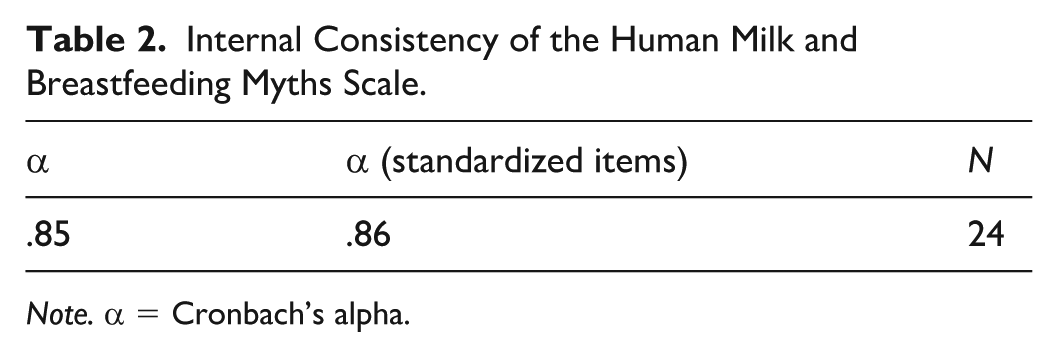
Note. α = Cronbach’s alpha.
Item Discrimination Index
Item discrimination was evaluated using the upper and lower 27% group method. Independent-samples t tests revealed statistically significant differences between the upper and lower 27% groups for all items, t(174) = 5.21–12.24, p < 0.01, indicating that the scale effectively distinguishes participants with high and low levels of belief in breastfeeding myths (Table 3).
Item Discrimination Results of the Human Milk and Breastfeeding Myths Scale Based on Upper and Lower 27% Groups
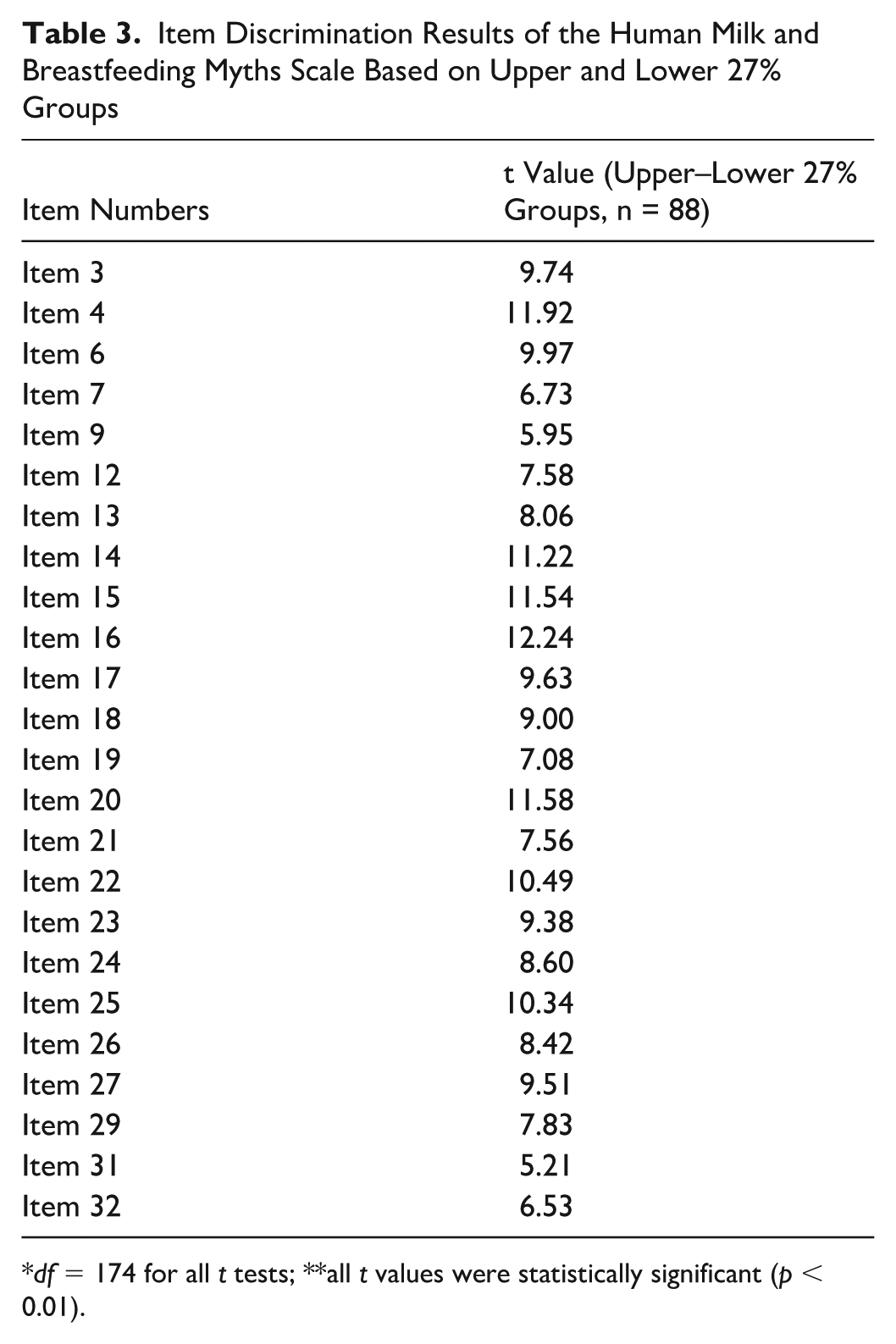
df = 174 for all t tests; **all t values were statistically significant (p < 0.01).
Stability
The stability of the scale was evaluated using the test–retest method with 34 participants over a 2-week interval. Mean scores were comparable between the test (M = 48.7, SD = 10.8) and retest (M = 49.2, SD = 10.6) administrations. Paired-samples t test results indicated no statistically significant difference between the two measurements, t(33) = −1.55, p = 0.13. Bland–Altman analysis demonstrated random scatter with no values exceeding the limits of agreement (−3.93–5.17), supporting the temporal stability of the scale (Table 4).
Test–Retest Reliability of the Human Milk and Breastfeeding Myths Scale.
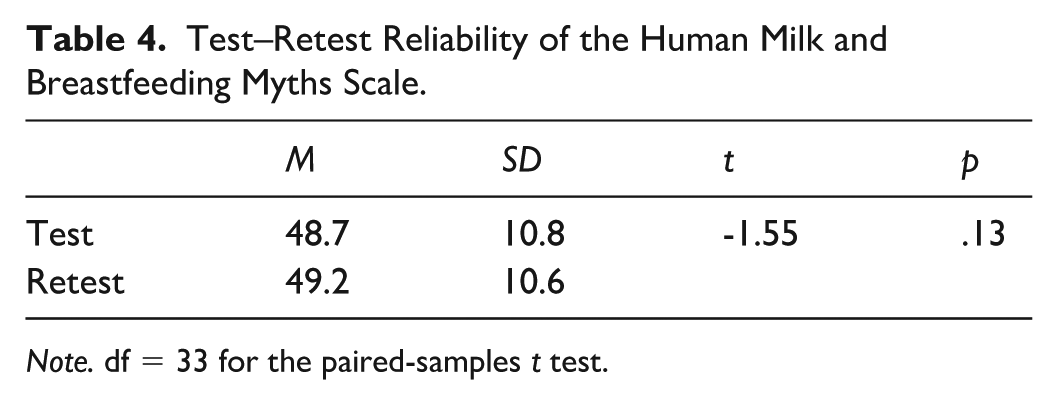
Note. df = 33 for the paired-samples t test.
Validity Analyses
Construct Validity
Exploratory factor analysis identified two factors with eigenvalues greater than 1. The first factor was dominant (eigenvalue = 5.96), explaining 24.8% of the total variance, whereas the second factor had an eigenvalue of 1.96 and accounted for an additional 8.2% of the variance (Table 5).
Exploratory Factor Analysis Results for the Human Milk and Breastfeeding Myths Scale.
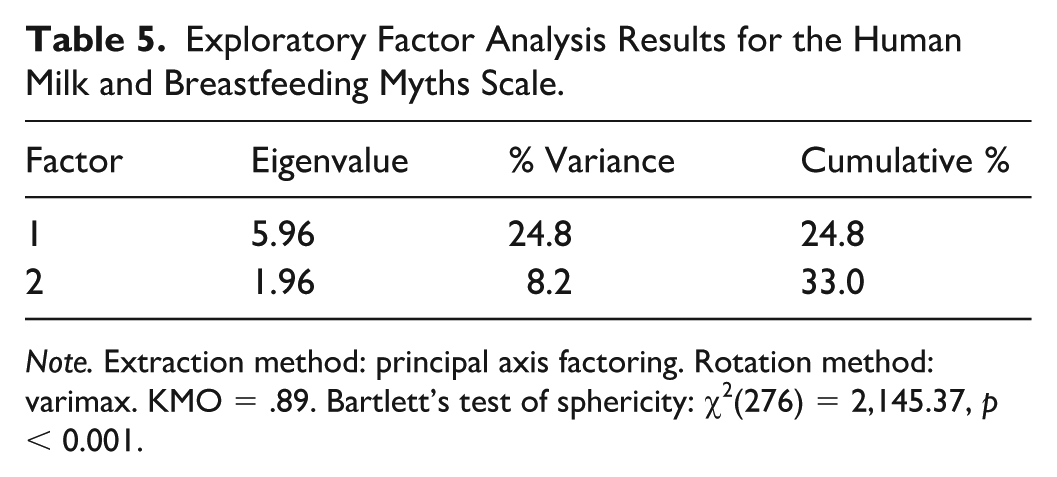
Note. Extraction method: principal axis factoring. Rotation method: varimax. KMO = .89. Bartlett’s test of sphericity: χ2(276) = 2,145.37, p < 0.001.
Content Validity
Following the exploratory factor analysis, eight items with low factor loadings were removed, resulting in a final scale consisting of 24 items. Content validity was assessed using the Lawshe method. The Content Validity Index (CVI) was .97, and the Content Validity Criterion (CVC) was .54. Because the CVI exceeded the CVC, the content validity of the scale was considered acceptable. In addition, a pilot study conducted with 10 participants indicated that the items were clear and comprehensible, and no further revisions were required.
Scoring
The final 24-item scale uses a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree). Possible scores range from 24 to 120, with higher scores indicating a higher level of belief in breastfeeding myths (see the online supplementary file).
Discussion
This methodological study, conducted among participants attending public hospitals, focused on the development and validation of the Human Milk and Breastfeeding Myths Scale.
In scale development studies, content validity is used to determine the extent to which items reflect the construct being measured. Expert opinions are typically consulted, with literature recommending a minimum of five and a maximum of 40 experts who have relevant subject matter expertise (Ayre & Scally, 2014; Tavşancıl, 2019). In the present study, 13 experts provided feedback on the draft items. The Lawshe technique was applied to assess content validity. According to this method, the number of experts indicating an item as “appropriate” is divided by the total number of experts, and one is subtracted; results equal to or below zero are considered unacceptable (Ayre & Scally, 2014). For the items evaluated by 13 experts, the Content Validity Index (CVI) was .97 and the Content Validity Criterion (CVC) was .54, indicating acceptable content validity (CVI > CVC). All items achieved content validity ratios above zero. A pilot test with 10 participants confirmed the comprehensibility of the scale items and their reflection of the intended construct.
Item analysis is a critical step in scale development, as items are expected to show adequate correlations with the total score. In this study, item–total correlations were examined, showing coefficients ranging from 0.22 to 0.59, which exceeds the recommended minimum of 0.20 (DeVellis, 2017). No items were removed from the final scale.
Discriminative power was evaluated by comparing the means of the lower and upper 27% of participants. Item discrimination analysis indicated that all items effectively differentiated participants with higher versus lower levels of belief in breastfeeding myths.
Construct validity was assessed using exploratory factor analysis (Brown, 2015; Thompson, 2008). The results supported a structure with two factors with eigenvalues greater than 1, with a clearly dominant first factor explaining a substantially larger proportion of the total variance. This pattern suggests that the scale may be considered essentially unidimensional in practice, supporting the use of a total score when assessing overall belief in breastfeeding myths. Overall, these findings provided evidence supporting the construct validity of the 24-item scale.
Stability was supported by test–retest findings showing no statistically significant difference between administrations, t(33) = −1.55, p = 0.13. Bland–Altman analysis further supported temporal stability, with no values exceeding the limits of agreement.
Internal consistency was evaluated using Cronbach’s alpha, which measures the extent to which items consistently assess the intended construct. Cronbach’s alpha values between 0.61 and 0.80 indicate moderate reliability, while values between 0.81 and 1.00 indicate high reliability (Baykul, 2015; Kılıç, 2016). The total scale demonstrated good internal consistency (α = .86), providing additional support for the reliability of the scale and its use in assessing beliefs about human milk and breastfeeding myths.
This study contributes to the breastfeeding literature by providing a culturally grounded measure of myths related to human milk and breastfeeding in Turkey. The scale may be useful for identifying prevalent misconceptions in clinical practice and for evaluating the effectiveness of educational interventions aimed at reducing myth-based barriers to breastfeeding.
Limitations
The study sample consisted of participants in their last trimester of pregnancy and participants breastfeeding infants aged 0–2 years who were recruited from public hospitals in Turkey. Therefore, the findings may not be generalizable to individuals receiving care in private settings or to populations from other regions and cultural contexts. In addition, the scale items use gendered language (e.g., “mother”), which may limit inclusivity for individuals who breast/chestfeed but do not identify as women. Future studies may adapt the wording to be more inclusive and evaluate measurement invariance across diverse populations.
Conclusion
This study evaluated the psychometric properties of the 24-item Human Milk and Breastfeeding Myths Scale among participants in the last trimester of pregnancy and breastfeeding participants with infants aged 0–2 years. The present study provides initial evidence that the 24-item Human Milk and Breastfeeding Myths Scale demonstrates acceptable validity evidence and good reliability. The scale may serve as a useful measure for assessing beliefs related to common myths about human milk and breastfeeding in Turkey and for supporting future breastfeeding intervention research and educational initiatives.
Supplemental Material
sj-docx-1-jhl-10.1177_08903344261434720 – Supplemental material for Human Milk and Breastfeeding Myths Scale: Development, Validity, and Reliability Study
Supplemental material, sj-docx-1-jhl-10.1177_08903344261434720 for Human Milk and Breastfeeding Myths Scale: Development, Validity, and Reliability Study by Sinem Güven Dinmez, Zehra Gölbaşi, Kafiye Eroğlu and Müge Coşkun Yıldırım in Journal of Human Lactation
Footnotes
Acknowledgements
The authors would like to thank all expert panel members and the pregnant women and mothers who responded to the survey.
Author Note
This study was presented as an oral presentation at the 2nd International Gulhane Human Milk and Breastfeeding Congress. (06.10.2024, Ankara-Turkey).
Kafiye Eroğlu is now affiliated to İstanbul Atlas University, İstanbul, Türkiye.
Ethical Considerations
The ethics committee approved the study (Fenerbahçe University Ethics Committee, Approval number 46.2023fbu-18.01.2023). Institutional permission for the hospitals where the research would be conducted was obtained from the Istanbul Provincial Health Directorate with the decision dated 20 June 2023 and numbered 2023/11. This research was conducted in accordance with the Declaration of Helsinki.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author [SGD], upon reasonable request.
Supplemental Material
Supplementary Material may be found in the "Supplemental material" tab in the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.