
Abstract
Background:
Mothers with flat or inverted nipples may have inadequate nipple protrusion, leading to infant latch difficulties and breastfeeding challenges. Although several approaches exist, their effectiveness varies.
Objective:
This randomized controlled study evaluated the effect of a newly developed Device for Flat or Inverted nipples (DFIN) on nipple length, the time for the infant to achieve latch, the duration of a single breastfeeding session, exclusive breastfeeding rates, and scores on the LATCH Assessment Tool.
Methods:
The study included 63 mother–infant pairs (DFIN group: n = 31; injector group: n = 32). The DFIN was applied in the experimental group, and the modified injector technique was applied in the control group. Measurements included nipple length, time taken to achieve latch, duration of a single breastfeeding session, and LATCH scores. Exclusive breastfeeding rates were monitored at birth and at 1, 2, 3, 4, 5, and 6 months postpartum.
Results:
Nipple length increased by 3.58 ± 2.06 millimeters in the DFIN group and 1.64 ± 1.17 millimeters in the injector group. The time taken to achieve latch decreased significantly in the DFIN group. LATCH scores increased by 2.10 ± 3.00 in the DFIN group, whereas they decreased by 1.38 ± 4.72 in the injector group. Exclusive breastfeeding rates were consistently higher in the DFIN group at birth and the 1st, 2nd, 4th, 5th, and 6th months postpartum (p < 0.05).
Conclusion:
The findings indicate that the DFIN improves nipple protrusion, shortens latch achievement time, enhances breastfeeding effectiveness, and supports sustained exclusive breastfeeding during the first 6 months postpartum.
Background
Breast milk alone provides all necessary nutrients for infants during the first 6 months. However, some problems prevent breast milk from being taken, including concern about milk insufficiency, hyperlactation, clogged milk ducts, engorgement, mastitis, painful, injured/cracked nipples, and flat or inverted nipples (Babakazo et al., 2022; Fitriyati et al., 2025).
As there is insufficient nipple projection in mothers with flat or inverted nipples, it has been reported that babies have difficulty latching on to the breast and have problems breastfeeding (Australian Breastfeeding Association, 2019). A study reported that 8.9% of mothers had breastfeeding problems, and 69% of mothers with this problem had flat nipples and 7.8 % had inverted nipples (Pradhan et al., 2025). However, some studies and reviews cite higher prevalence rates, up to 23% or even 34.5 % large-scale research (Maastrup et al., 2019; Suresh et al., 2014). Flat or inverted nipples are usually present from birth, but can also develop later in life due to breast surgery, cancer, or mastitis. The severity of nipple depression is categorized into three grades based on whether the nipple can be manually retracted while preserving its projection, and the degree of underlying fibrosis. Grade 1: minimal fibrosis; easily removed by hand. Grade 2: moderate fibrosis beneath the nipple; the nipple can be removed by hand, but its projection cannot be preserved. Grade 3: Severe fibrosis and indentation; not removable by hand (Nabulsi et al., 2022). Loss of tissue elasticity in the nipple–areolar complex can impair nipple protrusion during infant suckling, primarily due to increased subareolar fibrosis and reduced skin pliability. This mechanical limitation can hinder effective breastfeeding by restricting nipple extension and milk transfer (Douglas, 2022).
A study examining the relationship between nipple length and breastfeeding success reported that mothers with nipples of 7 mm or more were more successful at breastfeeding (Puapornpong et al., 2013). Also, it has been found that mothers with nipples shorter than 7 mm need more support (Intarasirisawat et al., 2019). Many interventions are recommended to solve flat or inverted nipple problems, including the modified injector technique (Nabulsi et al., 2022), vigorous sucking by the woman’s husband (Jain et al., 2013), the rubber band method (Dash, 2017), using silicone nipple shields (Maastrup et al., 2019; Santos et al., 2023), using breast shields (Chanprapaph et al., 2013), using electric breast pump (Chowdhry et al., 2024) and the Hoffman exercise (Thurkkada et al., 2022; Youssef Ahmed Abd-Ella & Fouad Mohammed 2021).
Key Messages
Flat or inverted nipples make breastfeeding difficult, affecting latching and exclusive breastfeeding.
This study found that using a specially developed breastfeeding device significantly increased nipple length and reduced the time taken for babies to latch on. It also improved LATCH scores and duration of baby’s single breastfeeding session, compared to the traditional syringe method .
Mothers using the device had higher rates of exclusive breastfeeding rates for 6 months.
This device may be a useful tool for improving breastfeeding outcomes by addressing specific challenges such as inverted nipple and latch difficulties.
Current approaches used to manage flat or inverted nipples—such as the modified injector technique, silicone nipple shields, Hoffman exercises, and breast shells—have important limitations. The modified injector method creates negative pressure but cannot provide controlled warmth prior to application. Silicone nipple shields are typically used to create a barrier between the infant and the nipple in mothers who experience pain or have nipple trauma; however, prolonged use has been associated with reduced milk production and may increase the risk of nipple irritation by keeping the skin moist (Coentro et al., 2020). Hoffman’s exercises rely on maternal adherence and do not produce immediate nipple protrusion. Breast shells can increase pressure and warmth on the breast but must be worn for long periods, which may limit skin ventilation, cause discomfort, or lead to skin irritation (Cecilio et al., 2022). Overall, these methods offer only partial or temporary improvement and do not address the combined need for controlled warmth, immediate negative pressure, and anatomical compatibility. This gap represents the specific rationale for the design and development of the DFIN.
In our study, different from these interventions, a device developed for flat or inverted nipples (DFIN) was used by researchers. This DFIN was developed by researchers based on their experience and literature. Studies show that applying heat to a mother’s breasts before breastfeeding or expressing milk significantly increases milk production and let-down reflex compared to before the intervention (Dencik, 2024; Ertugral Mollaahmetoglu & Guvenc, 2025). Applying a warm compress to the breasts increases blood circulation, relaxes breast tissue and stimulates oxytocin production. Oxytocin is responsible for milk letdown. This makes breastfeeding easier and more effective by facilitating the flow of milk to the nipple (Wahyuwihayanti et al., 2024). It is evident that methodologies such as the modified injector technique, silicone nipple covers, breast shields, and the Hoffman exercise do not permit direct application of heat. Inside the DFIN, however, there is a 150–200 ml hot water (39–41°C) reservoir, which allows the application of heat. DFIN was designed to fit the breast anatomy and be placed on breasts. DFIN is placed on the mother’s breast and kept on the breast for 10 minutes as stated in the literature. Then the piston in the DFIN is pulled, with the mother’s maximum comfort. With this step, it is aimed to correct/extend the flat/inverted nipple.
This study was designed to evaluate the effects of the DFIN for a mother just giving birth on nipple length, time taken to achieve latch and single breastfeeding session duration, LATCH scores and the duration of exclusive breastfeeding time in the first 6 months. The hypotheses of the study are as follows: H1: The nipple length of mothers using DFIN is longer; H2: Babies in the DFIN group will take less time to achieve latch; H3: Babies in the DFIN group will have a longer single breastfeeding session duration; H4: The LATCH score of the DFIN group will be higher higher; and H5: Babies in the DFIN group will have a longer exclusive breastfeeding time.
Methods
Research Design
This study employed a randomized controlled experimental design to evaluate the effectiveness of the DFIN in mothers with flat or inverted nipples. The study compared the impact of the DFIN with the modified injector technique on nipple length, time taken to achieve latch, single breastfeeding session duration, LATCH Breastfeeding Assessment Tool scores, and exclusive breastfeeding rates.
Research Setting
The research was conducted in the Obstetrics and Gynecology Clinic of Tekirdag Namık Kemal University Hospital, a clinical environment where breastfeeding is strongly promoted. In this region, breastfeeding is widely supported both culturally and through Baby-Friendly Hospital practices, with midwives and nurses routinely providing postpartum breastfeeding counseling. Despite these structures, mothers with flat or inverted nipples remain at increased risk of early latch difficulties and decreased exclusive breastfeeding, making this group particularly important for targeted interventions.
The study was conducted between November 2020 and November 2021, and data collection continued through the 6-month postpartum follow-up period for each mother–infant pair. The inclusion criteria required mothers to be aged 18 years or older, to have delivered at term (via vaginal or Cesarean birth), to have had an uncomplicated pregnancy and birth, and to have a nipple length of 7 mm or less. Mothers with any health condition that could interfere with breastfeeding were excluded. For mothers with uneven or asymmetric nipple shapes, nipple measurements were taken from both breasts, but the breast with the shorter nipple length—considered clinically more at risk for latch problems—was used for analysis. This approach was recommended by the independent statistician to ensure consistency and avoid measurement bias. To prevent potential confounding related to infant feeding difficulties, mothers with preterm or multiple births and infants with conditions known to affect latch or breastfeeding—such as congenital anomalies, tongue-tie, cleft palate, low birth weight, or any neonatal health problem—were excluded.
Research Sample
The G*Power program (Version 3.1.9.2.) was used to determine the required sample size. The power analysis of a study in which a breastfeeding support program was implemented and evaluated using LATCH scores found an effect size of .98 (Eksioglu, 2016). The aim of this study was to create a target change of .98 at a large effect level, with a two-sided alpha margin of error of 5% and a power of 90%. It was determined that there should be 29 mothers and babies per group.
Considering the potential for data loss during follow-up, the sample size was increased by 20%, resulting in 72 planned participants (36 per group). During follow-up, four mothers from both the DFIN and injector groups were excluded for non-participation in interviews, and one baby from the DFIN group died. Thus, 31 mothers–infant pairs in the DFIN group and 32 in the injector group completed the study. The effect size for nipple length was 1.784, with 99.5% power, and for the LATCH score, it was 0.841, with 90.7% power. A CONSORT flow diagram was used to present the participant flow (Figure 1).
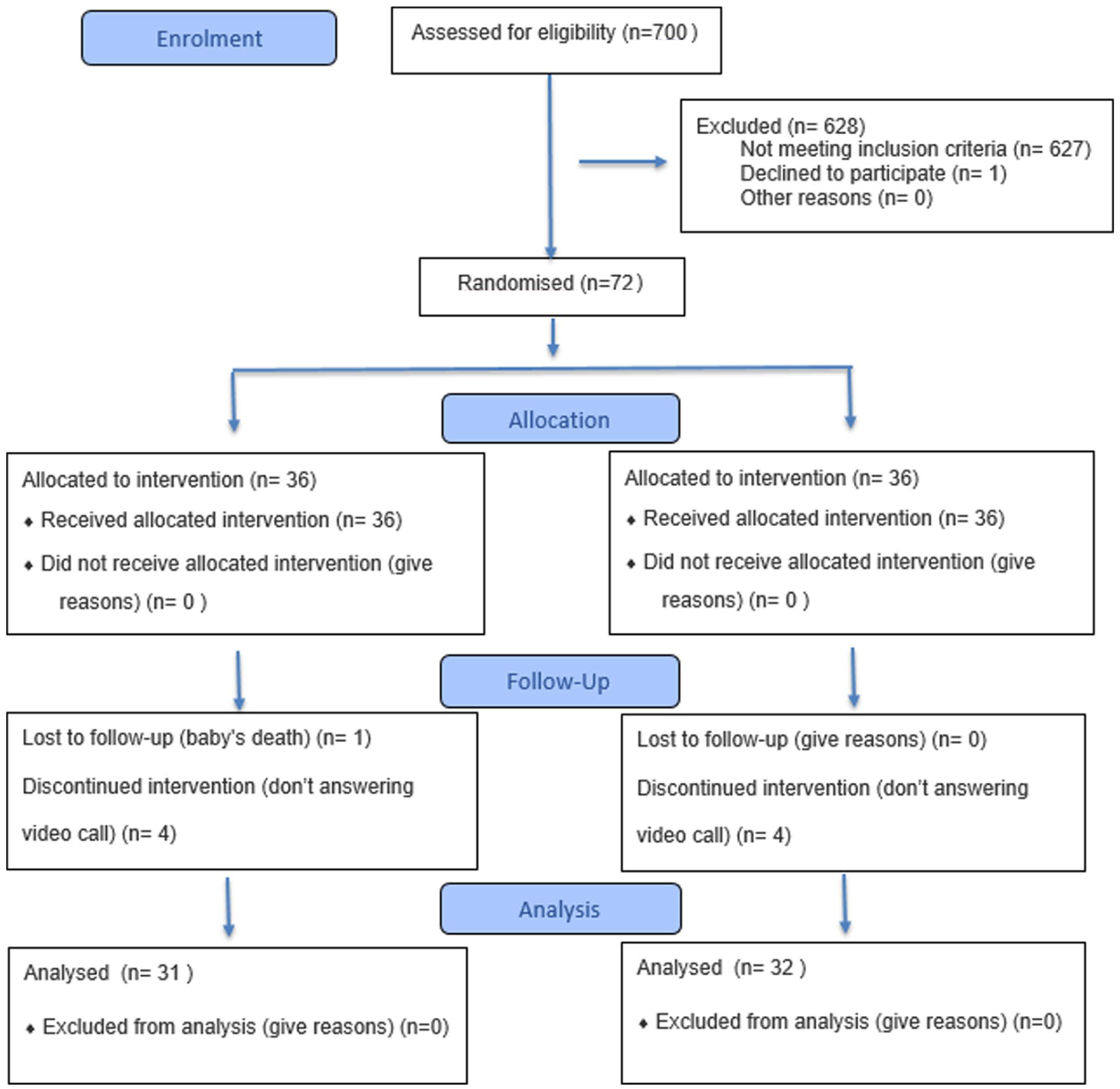
CONSORT 2025 flow diagram.
Randomization
Randomization was conducted using the URN method (Clark et al., 2021). To ensure allocation concealment and reproducibility, a set of sequentially numbered, identical, sealed opaque envelopes containing group assignments generated according to the URN procedure was prepared by an independent researcher not involved in data collection. When a mother–infant pair met the inclusion criteria, a ward nurse who was not part of the research team opened the next envelope in sequence to determine group allocation.
Research Measurements
Information and follow-up form
This form included information such as mothers’ age, education level, occupation, family income and type, pregnancy, and newborn’s sex, birth weight, and height, and APGAR score. The form was also used to record nipple sizes, time taken to achieve latch, and single breastfeeding session duration. The nipple length of the mothers was measured by the method used in the study by Puapornpong et al. (2013) titled “The Relationship of Nipple Length with Breastfeeding Success.” The researchers cut the ajutage off the 10 ml injectors and glued a millimetric transparent adhesive ruler on the cut. Next, the prepared injector was placed on the nipple and the value seen on the transparent ruler was recorded as the nipple length. A paper ruler was used to measure the diameter of the nipples and areola of the mothers. The diameter of the nipple and areola was measured for each mother’s a breast (Figure 2).

Nipple length, nipple and areola diameter measurement.
LATCH breastfeeding diagnosis and evaluation scale form
The LATCH scale is a diagnostic tool developed based on the Apgar score assessment model (Jensen et al., 1994). Its validity and reliability study was conducted, demonstrating its reliability. The scale’s Cronbach’s alpha coefficient was reported as 0.95 in previous studies, while in our study, it was found to be 0.95, confirming its internal consistency.
Nutrition form
This form recorded the infant’s feeding type—exclusive breastfeeding, breastmilk and formula, or formula only—at birth and at the 1st, 2nd, 3rd, 4th, 5th, and 6th months postpartum.
All data collection procedures, including follow-up assessments, LATCH scoring and completion of the nutrition form, were performed by the same lactation consultant nurse with 10 years of experience who had been trained by the researchers, thus ensuring consistency and preventing inter-rater variability.
Data Collection
Before the procedure
The purpose of the study was explained to the pregnant women who met the sample selection criteria by the researcher, and written consent was obtained from those who agreed to participate (n = 700). After consent, eligibility was confirmed immediately postpartum—before the first breastfeeding attempt—by measuring nipple length, and only mothers with a nipple length of 7 mm or less were included in the study (n = 72). Following eligibility confirmation, participants were randomly allocated to the DFIN or injector groups by a nurse in the clinic who was not part of the research team. Demographic information was then collected. Immediately after delivery (pre-application measurement), nipple length and diameter and areola diameter were measured by the same trained clinical nurse and recorded on the information and follow-up form.
Application to the DFIN group
Immediately after birth and before the first breastfeeding attempt, the DFIN was applied by the researcher to mothers in the DFIN group. Warm tap water (39–41°C) was added to the reservoir, and the device was placed on the breast for 10 minutes. During this period, the breast temperature and internal water temperature were monitored at 2–3 minute intervals. Before removing the device, suction was applied using the piston at the mother’s maximum comfort level. After removal, nipple length was measured by the same trained nurse and recorded as the first post-application measurement. Immediately afterwards, the same trained nurse positioned the infant at the breast and used a smartphone stopwatch to measure the time taken to achieve latching on and the duration of the single breastfeeding session. The same nurse assessed breastfeeding success using the LATCH Breastfeeding Assessment Tool, ensuring consistency across all evaluations. Changes in nipple length were photographed in mothers who provided consent—see Figure 3, which presents images taken before (A–C), after (B–D), and during (E) DFIN use. There were no adverse events during the intervention.

Before (A-C), After (B-D) and During (E) Use of DFIN.
Application to the injector group
Immediately after birth and before the first breastfeeding attempt, the researcher applied the modified injector method, which is routinely used in the clinic. Following the standard procedure (Arsenault, 1997), the narrow tip of the injector was removed and the plunger inserted from the cut end. The injector barrel was then placed over the flat or inverted nipple to create suction at the mother’s maximum comfort level. After removing the injector, the same trained nurse measured and recorded the nipple length as the first post-application measurement. Immediately afterward, the same trained nurse positioned the infant at the breast and used a smartphone stopwatch to measure the time taken to achieve latch and the duration of the single breastfeeding session. Breastfeeding success was assessed simultaneously by the same nurse using the LATCH Breastfeeding Assessment Tool, ensuring consistency across all evaluations. No adverse events occurred during the application of the injector.
Second and third applications
Intervention procedures were conducted within the first 12 postpartum hours. Because the hospital schedules breastfeeding every 2–3 hours, the second and third applications and measurements for both groups were conducted just before the subsequent two feeding sessions. This resulted in all three applications being completed within the first 12 hours after birth. This timing was necessary to ensure consistency and prevent inter-rater variability, as all assessments had to be performed by the same trained nurse, who was available only between 8 am and 8 pm.
Follow-up
After discharge, the same trained nurse contacted mothers in both groups at 1, 2, 3, 4, 5, and 6 months postpartum to determine whether their babies were being exclusively breastfed. This information was recorded on the Feeding Form. Although the short-term postpartum intervention consisted of three applications, both the DFIN and the modified injector device were provided for continued home use. Mothers reported routine use of their assigned method, usually at least twice daily. Therefore, the 6-month follow-up focused on evaluating the sustained impact of these techniques on exclusive breastfeeding rather than ongoing anatomical nipple changes.
Data Analysis
Number Cruncher Statistical System (NCSS) was used for statistical analysis. The Shapiro-Wilk test and graphs were used to test the normality of quantitative data. Descriptive statistical methods (mean, standard deviation, median, frequency, percentage, minimum, maximum) and Student’s t-test were used for quantitative variables with normal distribution, repeated measures analysis of variance with Bonferroni correction and Mann-Whitney U test, Kruskal-Wallis test and Dunn-Bonferroni test, Friedman test and Wilcoxon signed-ranks test with Bonferroni correction were used for quantitative variables without normal distribution. Pearson chi-squared test, Fisher’s exact test, and Fisher-Freeman-Halton test were used to compare qualitative data. Statistical significance was set at p < 0.05.
Ethical Considerations
Institutional permission was obtained from the hospital. Ethical permission was obtained from the Clinical Research Ethics Committee of Istanbul University – Cerrahpaşa, Cerrahpaşa Faculty of Medicine (Number: 54496, Date: September 10, 2020). Verbal and written consent was obtained from the parents for the mothers and babies to be included in the study. For the use of the LATCH Scale used in the research, permission was obtained. Clinical Registration: This study was registered with the U.S. National Library of Medicine Clinical Trials (code: NCT06978543).
Results
There were no significant differences in maternal sociodemographic characteristics and infant baseline variables, including delivery mode, gestational age, birth weight, birth length, head circumference, Apgar scores and infant sex, between the DFIN and injector groups (p > 0.05), as shown in Table 1.
Comparison of Sociodemographic and Infant Characteristics
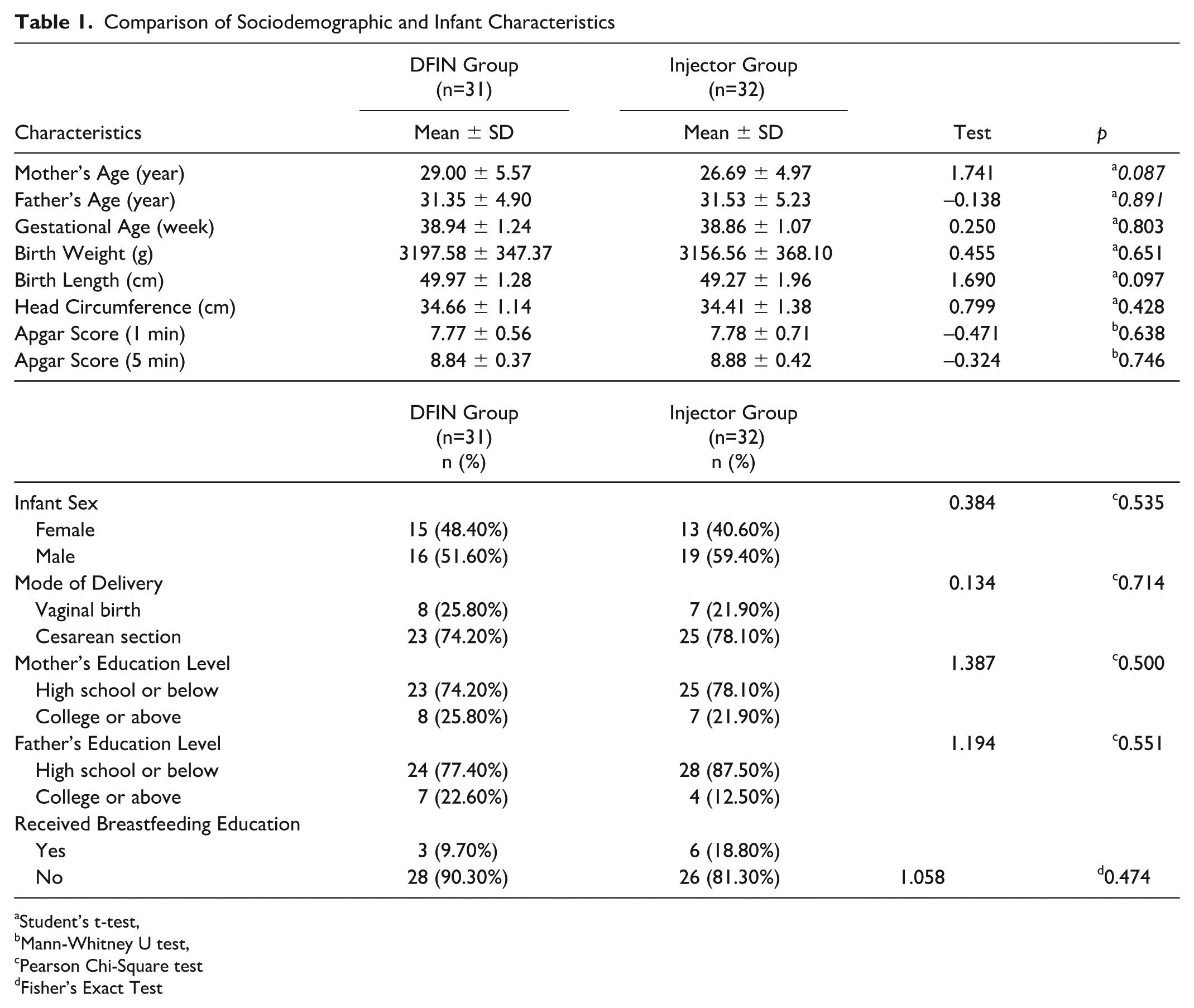
Student’s t-test,
Mann-Whitney U test,
Pearson Chi-Square test
Fisher’s Exact Test
The comparison of nipple lengths, time taken to achieve latch, single breastfeeding session duration, and LATCH scores between the groups is presented in Table 2. Both groups demonstrated significant increases in nipple length from pre- to post-application; however, the magnitude of improvement was significantly greater in the DFIN group than in the injector group (p < 0.001). Infants in the DFIN group achieved latch significantly faster than those in the injector group at the third post-application measurement, and the reduction in latch time across measurements was significantly greater in the DFIN group based on the change scores (p < 0.001). Although both groups showed increases in single breastfeeding session duration, the DFIN group exhibited a significantly larger improvement compared with the injector group based on the change score analysis (p < 0.05). LATCH scores increased significantly in the DFIN group but decreased in the injector group, resulting in a significantly greater overall improvement in the DFIN group from pre- to post-application measurements (p < 0.01).
Comparison of moms’ nipple length, time taken to achieve latch, single breastfeeding session duration, and LATCH scores between groups
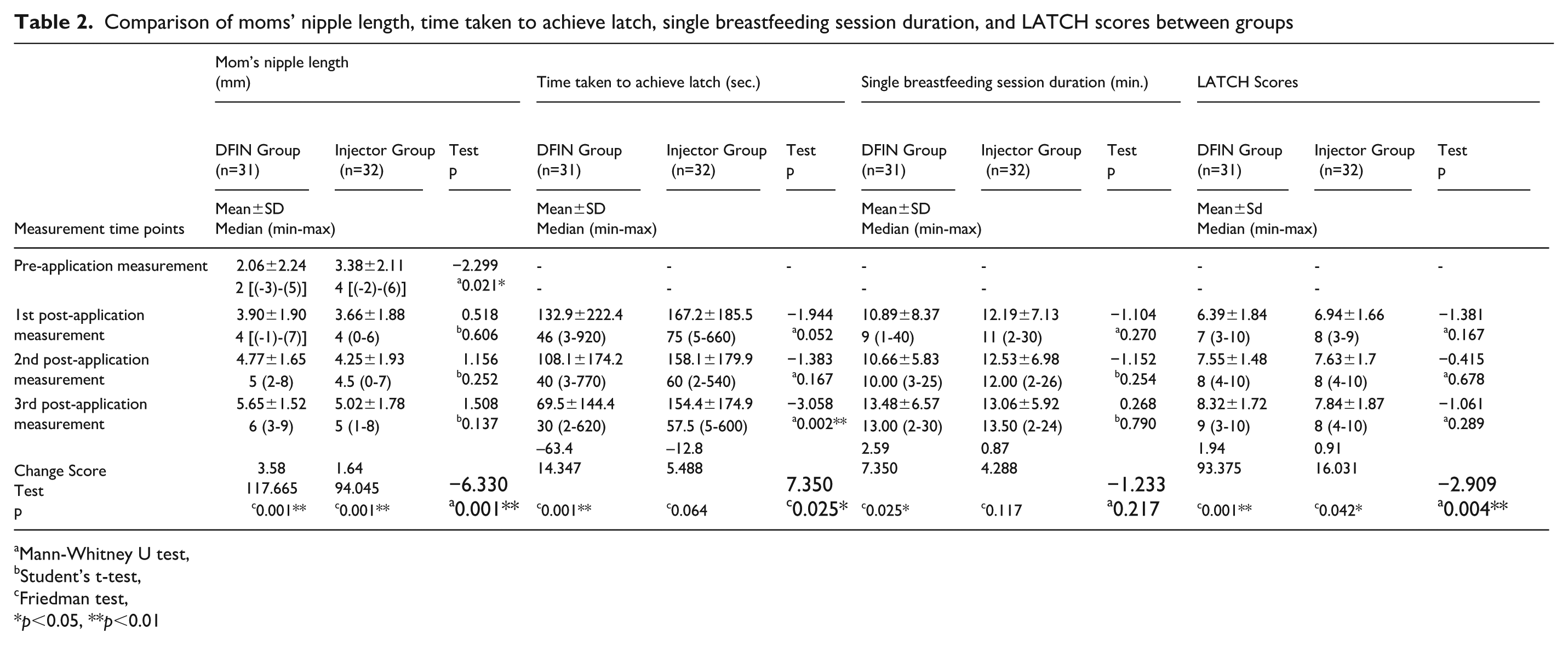
Mann-Whitney U test,
Student’s t-test,
Friedman test,
p<0.05, **p<0.01
Table 3 compares the babies feeding types at birth and during the 6-month follow-up. A significant difference favoring the DFIN group was observed at the 1st, 2nd, 4th, 5th, and 6th months (p < 0.05), while no difference was found between the groups at the 3rd month (p > 0.05).
Comparison of Feeding Types of Babies by Groups
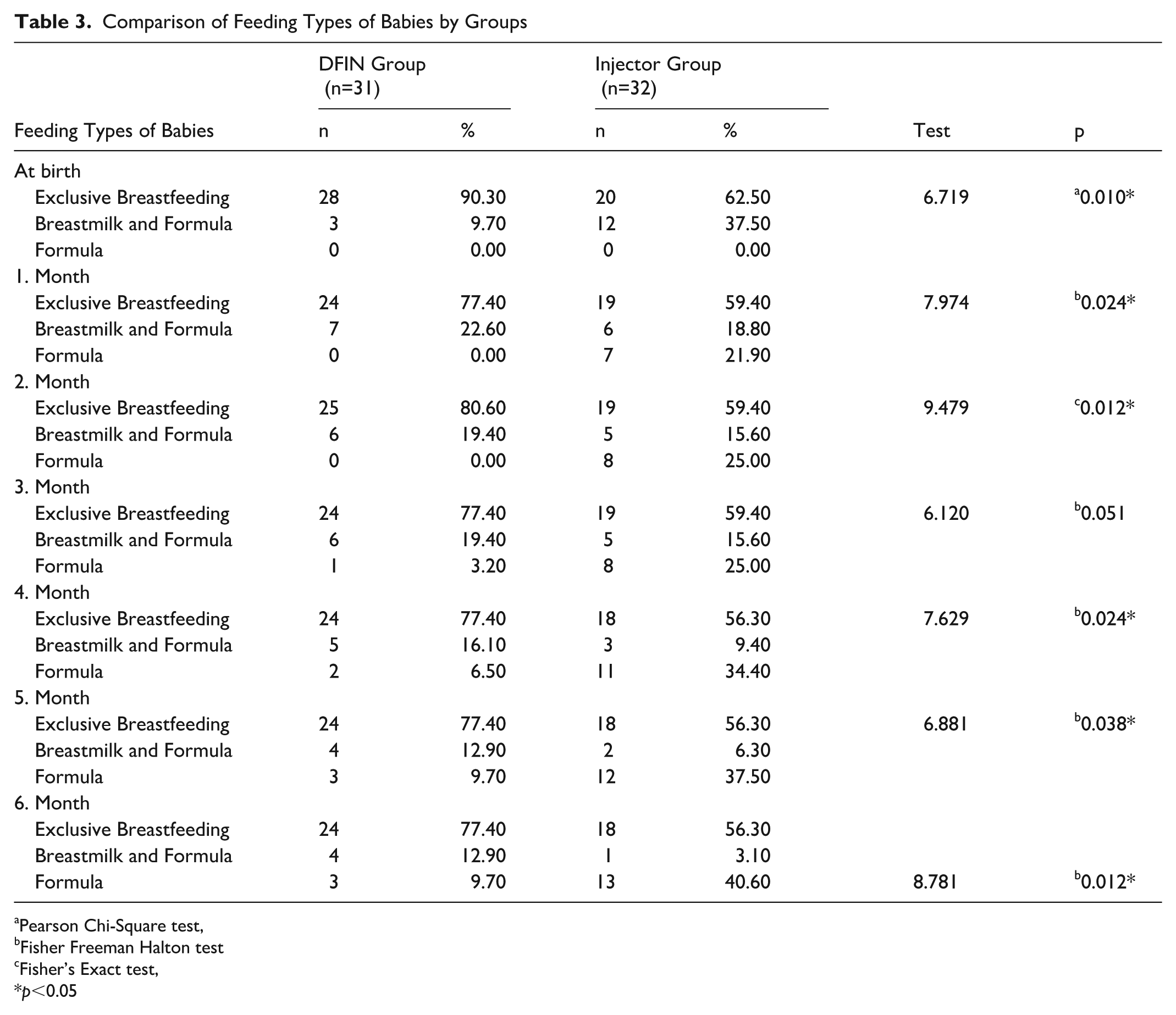
Pearson Chi-Square test,
Fisher Freeman Halton test
Fisher’s Exact test,
p<0.05
Discussion
In the study, nipple length was found to increase significantly in both groups in both intra- and inter-group assessments. The difference between the first and last measurements was 3.58 ± 2.06 mm in the DFIN group and 1.64 ± 1.17 mm in the injector group and was found to be significant in favor of the DFIN group (p < 0.05; Table 2). As a result of these findings, the H1 of the study was proven. There is no study in the literature measuring the length of nipples after birth.
However, in the study by Chanprapaph et al. (2013), breast shields were used 8 hours a day in pregnant women with a nipple length shorter than 7 mm, and the authors reported a significant increase in nipple length compared with the control group in their study (women who did not use breast shields). The change in nipple length was 2.37 ± 1.29 mm in the breast shield group and 1.84 ± 0.98 mm in the control group in their study. The use of breast shields resulted in increased nipple length compared with the non-intervention group, which is similar to the findings of the present study. Although both interventions were effective when compared with their own comparison groups in their respective studies, the increase observed in the DFIN group in the present study (3.58 mm) was greater than the increase reported in the breast shield group in the study by Chanprapaph et al. (2.37 mm). This result shows that the device is superior and more effective than both the breast shield and the injector method. It is thought that this difference of the DFIN was affected by both the mechanism, which provides a vacuum, and the ability to apply warmth. It is difficult for colostrum to come from the breast, especially immediately after birth. Temperature facilitates the flow of milk by stimulating milk ducts and milk pools (Wahyuwihayanti et al., 2024). When combined with gentle negative pressure, this warmth helps the nipple extend more easily, which may explain the superior outcomes observed with the DFIN. In terms of feasibility, the DFIN requires only warm tap water and manual suction, which makes it suitable for routine postpartum use in both hospital and home environments. Mothers reported no difficulty preparing the device or continuing its use after discharge, suggesting that the method is practical even in real-world settings with limited resources. Because this study did not isolate the effects of heat and suction, it remains unclear which component contributes most to the observed improvements. Future trials comparing heat-only and suction-only applications are needed to determine their independent and combined effects.
Time taken to achieve latch in the third evaluation of the babies in the DFIN group was found to be statistically significantly shorter than for babies in the injector group (p < 0.01; Table 2). According to this evaluation, it was observed that the babies of mothers who used the DFIN settled on the breast faster. Although many women with flat or inverted nipples want to breastfeed, they may be disappointed and stop breastfeeding after the baby is unable to attach or after multiple unsuccessful attempts (Dash, 2017). Although it is stated that babies do not need the nipple for sucking and that they should fully attach the areola, it has been stated in many studies that babies have difficulty in attaching to the breast and problems in breastfeeding because there is no protrusion of the flat or inverted nipple (Australian Breastfeeding Association, 2019; Bulbuli et al., 2018; Dash, 2017). However, in these studies, the time taken to achieve latch was evaluated through observation only. We did not find a study in the literature that measures the time taken to achieve latch. In our study, the time taken to achieve latch was also evaluated. In the first evaluation, it was seen that babies in the DFIN group attached to the breast in 132.94 seconds and babies in the injector group attached in 167.28 seconds. The time taken to achieve latch in the DFIN group was found to be remarkably short. In the third evaluation, babies in the DFIN group attached to the breast in 69.52 seconds, whereas babies in the injector group took 154.13 seconds; a significant difference was found in favor of the DFIN group (p < 0.05). As a result of these findings, H2 of the study was proven. Because nipples lengthened more in mothers who underwent intervention with the DFIN, it was much easier for babies to attach and hold the breast. Accordingly, babies in the DFIN group spent less time attaching to the breast.
After the interventions in the groups, no significant difference was found between the single breastfeeding session duration (p > 0.05; Table 2). However, when the groups were compared within themselves, it was observed that the babies in the DFIN group had an average increase of breastfeeding time of 2.60 ± 7.28 minutes between the first evaluation and the third evaluation, and this increase was significant (p < 0.05). In the injector group, the increase was not significant. In the literature, there is no research that we could find on the single breastfeeding session duration of mothers with flat or inverted nipples. The inability to attach to the breast due to flat or inverted nipples may cause delayed breastfeeding, infrequent breastfeeding, and breast enlargement/engorgement. As a result, babies may be prevented from receiving colostrum (Bulbuli et al., 2018; Dash, 2017). In our study, it can be interpreted that there may be an increase in the amount of milk as the babies in the DFIN group attach to the breast faster, and, for this reason, the babies stay at the breast longer to take the colostrum in the breast.
The breastfeeding success was evaluated using LATCH (Table 2). Studies on mothers with flat or inverted nipples show that interventions such as the injector method (Nabulsi et al., 2022), breast shields (Chanprapaph et al., 2013), and multiple care approaches (Bulbuli et al., 2018) significantly improve LATCH scores. In the first three breastfeeding sessions, LATCH scores showed no significant difference between the groups (p > 0.05). However, the increase in LATCH scores from the first to the third session was significantly higher in the DFIN group (p < 0.01). According to these results, breastfeeding success increased in both hospital practices, but more breastfeeding success was achieved in the DFIN group. The fact that a healthcare professional was always available while both methods were being used may have contributed to the effective results of both methods.
Exclusive breastfeeding rates at birth and at 1, 2, 4, 5, and 6 months were significantly higher in the DFIN group. In contrast, the injector group showed a decrease in exclusive breastfeeding and an increase in formula feeding (Table 3). Flat or inverted nipples can hinder breastfeeding by making it difficult for the baby to latch and obtain colostrum, leading to shorter breastfeeding durations and increased use of bottles (Belal et al., 2024). Studies on the impact of this condition on exclusive breastfeeding show mixed results. Suzuki et al. (2015) found no significant difference in exclusive breastfeeding rates at 7-day and 1-month follow-ups. Chakrabarti and Basu (2011) reported 68% exclusive breastfeeding at 28 days. Chanprapaph et al. (2013) demonstrated that the rubber band method increased exclusive breastfeeding rates by the 12th week. In our study, before the mothers were discharged, both methods (the injector and the DFIN) were taught to the mothers by the researcher, and they were informed about their use at home when needed. The mothers stated that the DFIN was more comfortable, easier, and more usable, with the feature of being able to apply warmth, unlike the injector. They reported that only 10 minutes of use before breastfeeding facilitated the descent of breast milk and relieved their breasts. By contrast, mothers in the injector group reported that the injector method was sometimes painful. It may be concluded that the DFIN is superior to the injector method in the long-term effect of exclusive breastfeeding rate.
Limitations
Although the data for this study were collected between 2020 and 2021 as part of a doctoral thesis, the findings remain valid. No significant clinical or technological changes have occurred in the management of flat or inverted nipples during this period. Therefore, the observed physiological responses and the effectiveness of the DFIN are still applicable to breastfeeding support today.
Because of the low normal birth rate, mothers were not selected only from those who gave birth normally. It was observed that the nipple lengths of the mothers in the DFIN group were shorter than in the injector group before any application was made. Because the mothers in each group were determined randomly, the shorter nipple length of the mothers in the DFIN group was completely coincidental, and homogeneity was not achieved in terms of this feature before.
Conclusions
The findings of this study demonstrate that the DFIN provides meaningful benefits for mothers with flat or inverted nipples by improving key early breastfeeding indicators. The device effectively increased nipple length, reduced the time taken to achieve latch, lengthened single breastfeeding session duration, and improved LATCH scores—factors known to support successful milk transfer and maternal breastfeeding confidence in the immediate postpartum period. Mothers continued to use the device at home, which likely reinforced these early gains. Accordingly, a higher proportion of infants in the DFIN group remained exclusively breastfed during the first 6 months. While these results suggest that early mechanical improvement of nipple protrusion may contribute to sustained exclusive breastfeeding, further research is warranted to confirm the underlying mechanisms and causal pathways.
Footnotes
Acknowledgements
This article is produced from the PhD thesis of Zeynem YILDIRIM BALKAN. The authors are grateful to the babies and their mothers who participated during the study.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.