
Abstract
Background:
A longer second stage of labor has been associated with increased likelihood of perinatal morbidity and mortality, but associations with the initiation of early and exclusive breastfeeding has not been explored.
Research Aims:
The objective of this study was to examine the relationship between second stage of labor duration and lactation outcomes in the first 7 days after birth.
Methods:
A secondary cross-sectional analysis was performed using electronic health record and survey data from a subset of primiparous participants from a longitudinal randomized control trial. Participants were included in the analysis if they intended to exclusively or near-exclusively breastfeed, had a vaginal birth, and they and their infants were discharged in the first 7 days after birth. Lactation outcome measures were timing of the first feed after birth, infant formula feeding frequency, direct chest/breastfeeding frequency during the 24 hours before discharge, and delayed onset of Lactogenesis II. Negative binomial, Poisson, and binary logistic regression models were applied for analyses.
Results:
The final cohort included 163 participants. The mean second stage of labor duration was 1.58 hours. Nearly half (46%) of participants used infant formula during hospitalization but second stage of labor duration was not significantly associated with the measured lactation outcomes.
Conclusion:
Longer second stage of labor duration was not associated with the defined lactation outcomes, thus did not impair attainment of early and exclusive breastfeeding in the first 7 days after birth.
Background and Introduction
Breastfeeding—a term that encompasses feeding an infant maternal/parental milk via direct chest/breastfeeding (C/BF) or other modalities (Labbok & Starling, 2012)—has dose-dependent and long-term benefits for lactating parents and their infants (Lande et al., 2020). Exclusive breastfeeding (no infant formula or other liquids) is recommended for the first 6 months of life, after which it is advised that complementary solid foods be introduced (Kuehn, 2018; Lande et al., 2020). Successful attainment of early and exclusive breastfeeding in the first few days after birth corresponds with longer breastfeeding duration and exclusivity (Bryanton et al., 2020; Fan et al., 2020; Lande et al., 2020). In the United States, 21% of breastfed infants also receive infant formula within the first 48 hours of life, and less than 30% of infants are exclusively breastfed at 6 months (Kuehn, 2018). Long-term milk production can be inhibited if lactation is not well-established in the first few days after birth (Bryanton et al., 2020; Fan et al., 2020). Therefore, to reach optimal public health targets and parents’ own goals for breastfeeding duration and exclusivity, it is important to understand how intrapartum and immediate postpartum (< 7 day after birth) factors impact lactation outcomes in the first few days after birth.
Labor characteristics have been associated with decreased breastfeeding duration and exclusivity during the first year of life. Specifically, use of epidural anesthesia, Cesarean delivery, and administration of induction agents (i.e., Pitocin, misoprostol) are correlated with increased infant formula use during birth hospitalization and with shorter duration of breastfeeding exclusivity (Bryanton et al., 2020; Chantry et al., 2014; Fan et al., 2020). The second stage of labor is the period from complete dilation of the cervix to the birth of the infant. The second stage of labor has high potential for parental and fetal stress that can necessitate invasive monitoring and intervention (Infante-Torres et al., 2019). There is evidence that prolonged second stage of labor—defined as pushing for greater than 3 hours for primiparas (2024)—is related to perinatal morbidity and mortality, although data are conflicting (Infante-Torres et al., 2019; Zipori et al., 2019).
Maternal exhaustion, stress, and pain during labor—all associated with longer labor duration—have been identified as barriers to establishing lactation (Türkmen et al., 2020). Further, some labor interventions also have potential to inhibit onset of copious milk production—referred to as Lactogenesis II—and impede lactation efforts (Peng et al., 2024). There have been no studies investigating the association between second stage of labor duration and immediate postpartum (≤ 7 days after birth) lactation outcomes. The objective of this study was to examine the relationship between second stage of labor duration and lactation outcomes in the first 7 days after birth (immediate postpartum lactation outcomes). We hypothesized that a longer second stage of labor duration would be associated with the infant’s first feed occurring greater than 1 hour after birth, increased use of infant formula during birth hospitalization, decreased frequency of direct C/BF before discharge, and delayed onset of Lactogenesis II.
Methods
Research Design
This is a secondary analysis of data collected during a longitudinal randomized control trial (RCT) that examined the efficacy of text-message based breastfeeding support (Mobile, semi-automated text message-based intervention to prevent perceived low or Insufficient miLK supply, MILK Trial; ClinicalTrials.gov registration: NCT02724969). Participants of this RCT were recruited between February 2017 and May 2018. Enrollment occurred at 13–25 gestational weeks during pregnancy and participants were followed through 6 months postpartum. Participants were pregnant with their first child, had a singleton pregnancy, intended to exclusively or near-exclusively breastfeed, and received care at a regional birth hospital in Pittsburgh, Pennsylvania (Demirci et al., 2020). Near-exclusive breastfeeding was defined by the researchers as planning on feeding their infant mostly via breastfeeding with a small amount of formula use. Each participant was randomized to one of two groups; the treatment group received text message breastfeeding support and education, while the control group were referred to text-based general perinatal education (Demirci et al., 2020). In both groups, text support began at 25 weeks of pregnancy and continued through at least 8 weeks postpartum. Other MILK Trial procedures, conceptualization of lactation variables (i.e., onset of Lactogenesis II), and results are reported in the publication for the primary study (Demirci et al., 2020). Ethical approval was received from the University of Pittsburgh Human Research Protection Office (Study #19050021) and informed consent was obtained before implementation of study procedures.
Keys Messages
The duration of the second stage of labor has been associated with morbidity and mortality among birthing parents and their infants, but the impact on lactation outcomes in the immediate postpartum period has not been explored.
Increased second stage duration was not associated with the defined lactation outcomes in the immediate postpartum period in this cohort of primiparous participants who intended to breastfeed exclusively or near-exclusively.
Despite prenatal intention to breastfeed exclusively or near exclusively and independent of second stage duration, the majority of participants fed formula to their infants during the birth hospitalization.
Setting and Relative Context
The site of the primary study serves approximately 10,000 pregnant and birthing families each year and, at the time of the study, employed several International Board-Certified Lactation Consultants (IBCLCs) who conducted prenatal and postnatal inpatient and outpatient visits. The hospital also offered in-person birthing, lactation, and newborn care classes for a fee at the time of the RCT. Double electric multi-use breast pumps are available for use at the bedside and for rent upon discharge. Nurses on the perinatal care floors take introductory breastfeeding support classes and can pursue breastfeeding counselor certification. The hospital is pursuing the state-based Baby-Friendly Hospital designation (Keystone 10) but has not yet met the requirements of all 10 steps. Pasteurized donor human milk is available for infants that meet criteria at this facility.
Sample
Participants who had Cesarean sections (C/S) were excluded for this secondary analysis. Those who were hospitalized or whose infants were hospitalized for > 7 days postpartum were also excluded because we intended to capture immediate postpartum in-hospital feeding data only. The final cohort consisted of 163 participants who gave birth vaginally. Most self-reported as White and non-Hispanic (72%), married (65%), and had an associate degree or higher (73%).
Measurement
The focal predictor, second stage of labor duration, was measured in hours from 10 cm cervical dilation to birth of the infant (ratio) and was abstracted from the electronic health record (EHR). Lactation outcomes in the first 7 days after birth were dependent variables and included: (a) timing of first feed after birth, (b) direct C/BF frequency 24 hours before discharge, (c) infant formula feeding frequency, and (d) onset of Lactogenesis II. Timing of first feed after birth (direct C/BF ≤ 1 hr or > 1 hr after birth) was measured as a binomial variable (Parker et al., 2020). Direct C/BF frequency in the 24 hours before discharge and infant formula feeding frequency for the entire birth hospitalization were continuous lactation outcome measures that were analyzed as count data. Onset of Lactogenesis II was measured as a binomial variable, with onset > 3 days after birth representing “delayed onset” and onset ≤ 3 days being “expected” (Chantry et al., 2014).
Covariates included in all analyses were maternal/parent age, partner status (single, living with partner, married), education level (< associates degree or >/= associates degree), racial identity (“White non-Hispanic” or “Black, Indigenous, or Person of Color [BIPOC] and/or Hispanic”), gestational age at birth, synthetic oxytocin used in labor, anesthesia (epidural) in labor, neonatal intensive care unit (NICU) admission, and randomization grouping within the larger trial (intervention vs. control group; Fan et al., 2020; Gomes et al., 2018). These covariates were included as they are known predictors of lactation outcomes (Fan et al., 2020).
Data Collection
Demographic and pregnancy data were collected from the EHR and via self-report at study enrollment between 13 and 25 weeks of gestation. Lactation, infant feeding, and birth data (e.g., second stage of labor duration) were collected via birth hospitalization EHR review for birth-parent infant pairs that were hospitalized for less than 7 days after birth. Two research assistants independently abstracted all EHR data and resolved differences through EHR re-review. Onset of Lactogenesis-II was assessed via a remote electronic survey at 1 week postpartum with a single question that asked, “How long did it take for your milk to come in after your baby was born?” with the following answer options: 1 day or less, 2 days, 3 days, 4 days, more than 4 days, my milk never came in, and I don’t remember (Chapman & Pérez-Escamilla, 2000).
Data Analysis
SPSS (Version 28) was used for statistical analysis. Descriptive statistics were generated for demographic, pregnancy, birth, and lactation data. Mean, standard deviation, median, and interquartile range were generated to describe ratio variables; frequencies and percentages were used for categorical variables. Correlation analyses were performed to identify potential confounders.
To examine the relationship between second stage of labor duration and the immediate postpartum lactation outcomes, we used binary logistic, negative binomial, and Poisson regression models according to the data type of the outcome assessed (e.g., binary vs. count data). Binary logistic regression was used to examine second stage of labor duration as a predictor of timing of the first feed after birth and onset of Lactogenesis II. To analyze the relationship between second stage of labor duration and the outcomes of infant formula feed frequency and direct C/BF frequency, negative binomial regression and Poisson regression were applied, respectively. Both are non-parametric analysis techniques applied for outcome variables that are count data. Negative binomial regression is used when count data is over dispersed with values of zero. Assumptions and the presence of outliers were assessed visually with histograms and boxplots. Models report main effects between independent and dependent variables.
In three models (dependent variables: infant formula feed frequency, direct C/BF frequency 24 hr before discharge, onset of Lactogenesis II), we included the remaining defined lactation outcomes as covariates (as relevant) given a known or hypothesized association. For example, there is an inverse relationship between infant supplementation and direct CF/BF, thus formula percentage was used as a covariate for the model evaluating the relationship between second stage of labor duration and number of direct C/BF during birth hospitalization. First stage of labor duration—defined as admission to the labor and delivery unit until complete dilation of the cervix in hours—was evaluated in early models. Inclusion of first stage of labor duration did not improve model fit and was not significantly associated with outcomes, and thus was excluded from final analyses. Assumptions were met for analyses. Data for all participants were included without transformations, as sensitivity analyses revealed outliers did not affect model fit.
Missing Value Analysis
Multiple imputation was used to attenuate missing data. Overall, 122 (75%) of participants had complete data. The variable with the largest amount of missing data was onset of Lactogenesis II (17% missing). Little’s MCAR test with Estimated Marginal (EM) Means indicated that missing values were not missing completely at random: X2(17) = 39.05, p = 0.002; Enders, 2010; Sterne et al., 2009. Five datasets with imputed values for missing data were created (Sterne et al., 2009). Pooled (original and imputed) odds ratios and p values are reported for binary logistic regression models. For Poisson and negative binomial regression models (outcome: infant formula feeding frequency, C/BF frequency), original dataset incidence response rates (IRR) from are reported in results and all imputed IRR are included in tables.
Results
The mean second stage of labor duration was 1.58 hours (SD = 1.4), with 19 (12%) experiencing clinically prolonged second stage of labor (> 3 hr). Eleven (7%) experienced forceps or vacuum assisted delivery. About half reported onset of Lactogenesis II less than 3 days after birth (54%). All birth parents were discharged from the birth hospital by 3 days postpartum. Additional demographic characteristics and clinical data are summarized in Table 1.
Cohort Demographics and Birth Hospitalization Characteristics With Original Data (N = 163).
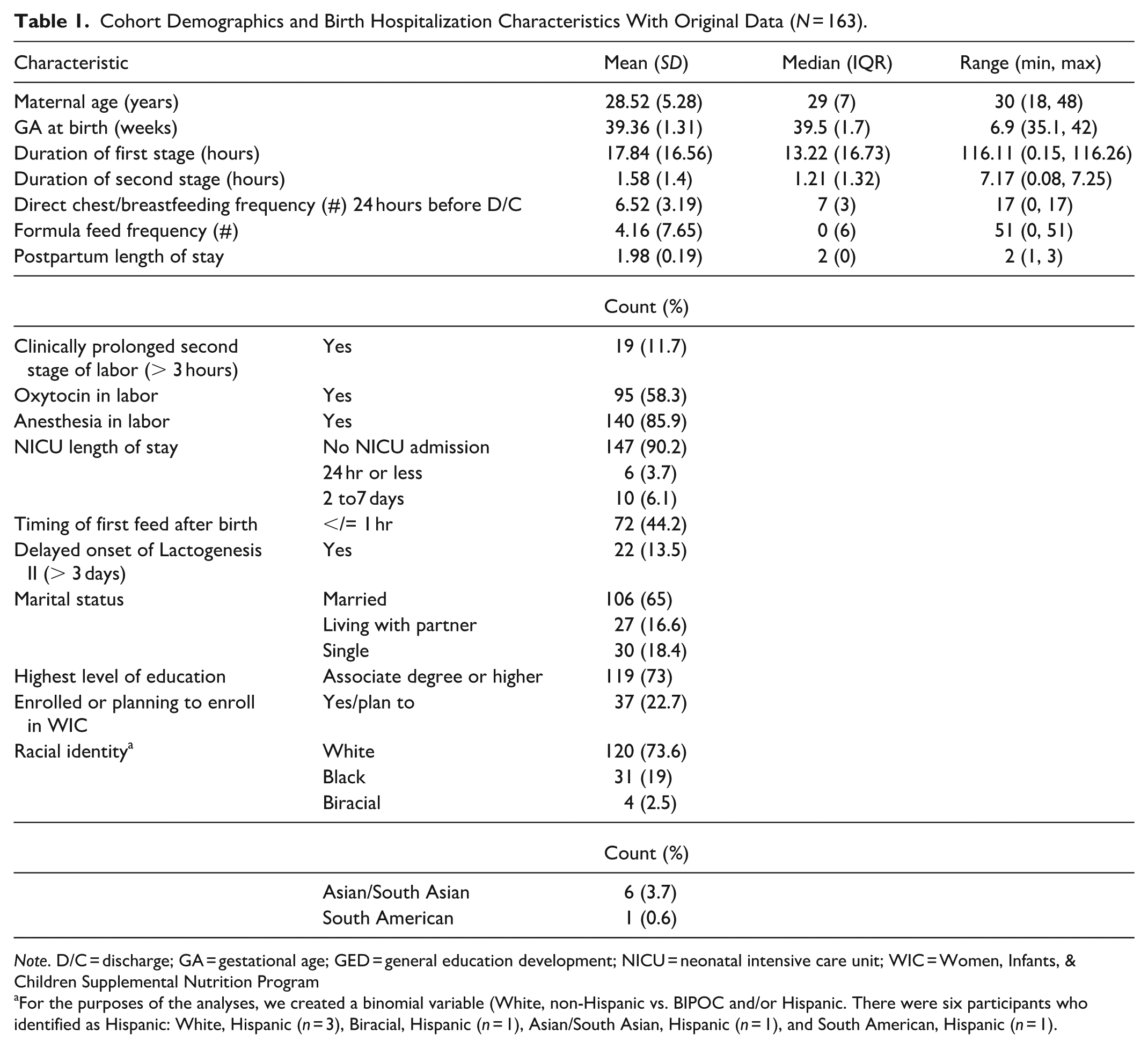
Note. D/C = discharge; GA = gestational age; GED = general education development; NICU = neonatal intensive care unit; WIC = Women, Infants, & Children Supplemental Nutrition Program
For the purposes of the analyses, we created a binomial variable (White, non-Hispanic vs. BIPOC and/or Hispanic. There were six participants who identified as Hispanic: White, Hispanic (n = 3), Biracial, Hispanic (n = 1), Asian/South Asian, Hispanic (n = 1), and South American, Hispanic (n = 1).
Relationship Between Duration of Second Stage of Labor and Lactation Outcomes
The second stage of labor duration only (without interaction terms or other covariates) did not significantly predict any lactation outcome measures.
The second stage of labor duration was not associated with the timing of the first feed after birth in the final binary logistic regression model (Table 2). Oxytocin use during labor was associated with lower odds of the first feed occurring later than 1 hour after birth (pooled p = 0.021), whereas NICU admission was associated with higher odds (pooled p = 0.015).
Associations Between Second Stage Duration and Timing of First Feed After Birth (N = 163).
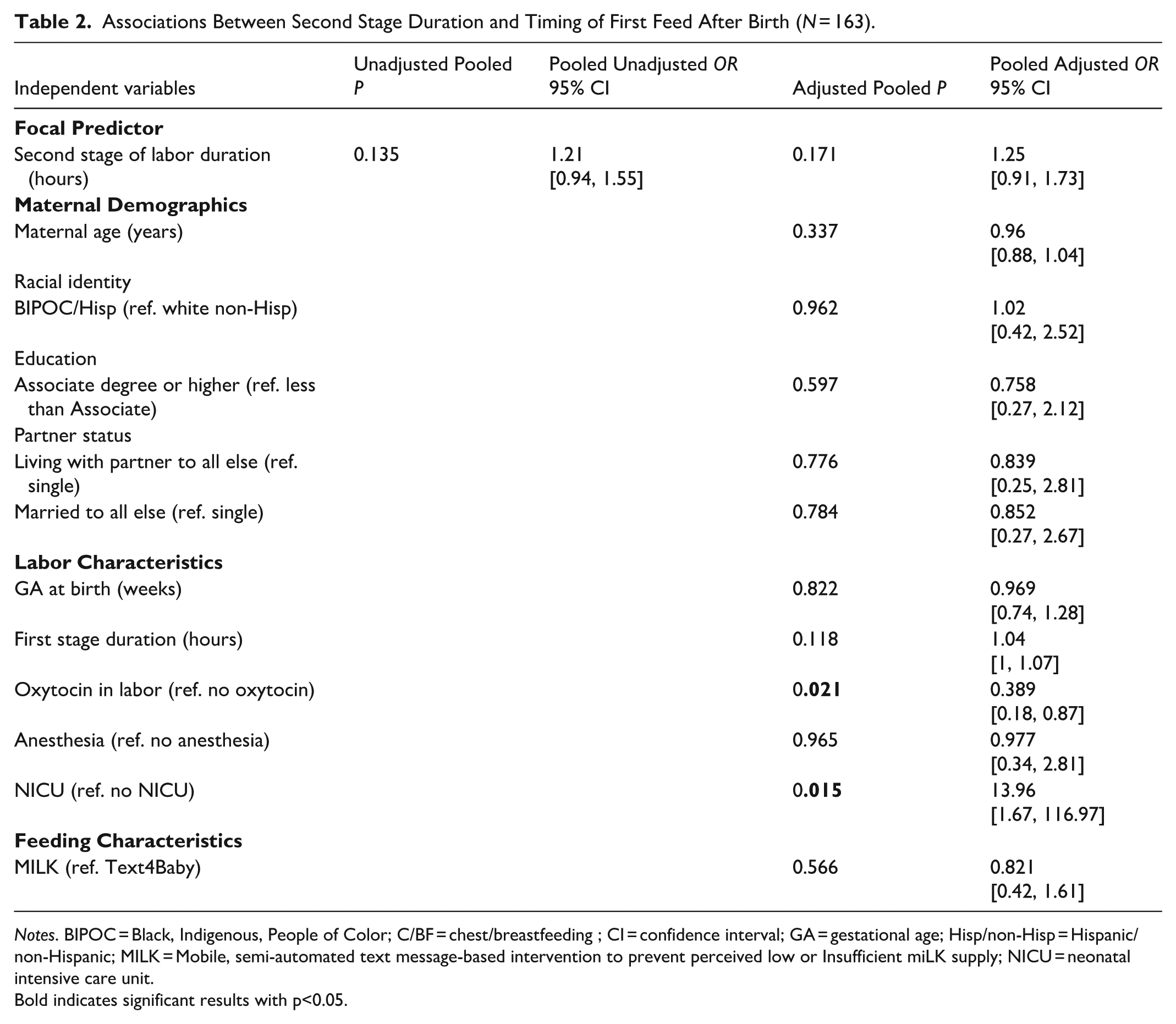
Notes. BIPOC = Black, Indigenous, People of Color; C/BF = chest/breastfeeding ; CI = confidence interval; GA = gestational age; Hisp/non-Hisp = Hispanic/non-Hispanic; MILK = Mobile, semi-automated text message-based intervention to prevent perceived low or Insufficient miLK supply; NICU = neonatal intensive care unit.
Bold indicates significant results with p<0.05.
The second stage of labor duration was not a significant predictor of infant formula feed frequency during birth hospitalization in a negative binomial regression model that included covariates, timing of the first feed after birth, and direct C/BF frequency in the 24 hours before birth hospitalization discharge (Table 3). Participants who identified as BIPOC and/or Hispanic had higher rates of infant formula use across original and imputed datasets (Original IRR = 2.52, 95% CI [1.45, 4.37], p = 0.003). Higher incidence rates of infant formula use were also associated with anesthesia during labor (IRR = 4.33, 95% CI [0.97, 19.35], p = 0.008) and NICU admission (IRR = 6.94, 95% CI [3.6, 113.36], p < 0.001), whereas higher direct C/BF frequency 24 hours before discharge was associated with fewer infant formula feeds (Original IRR = 0.764, 95% CI [0.71, 0.83], p < 0.001).
Associations Between Second Stage Duration and Formula Feeding Frequency During Birth Hospitalization (N = 163).
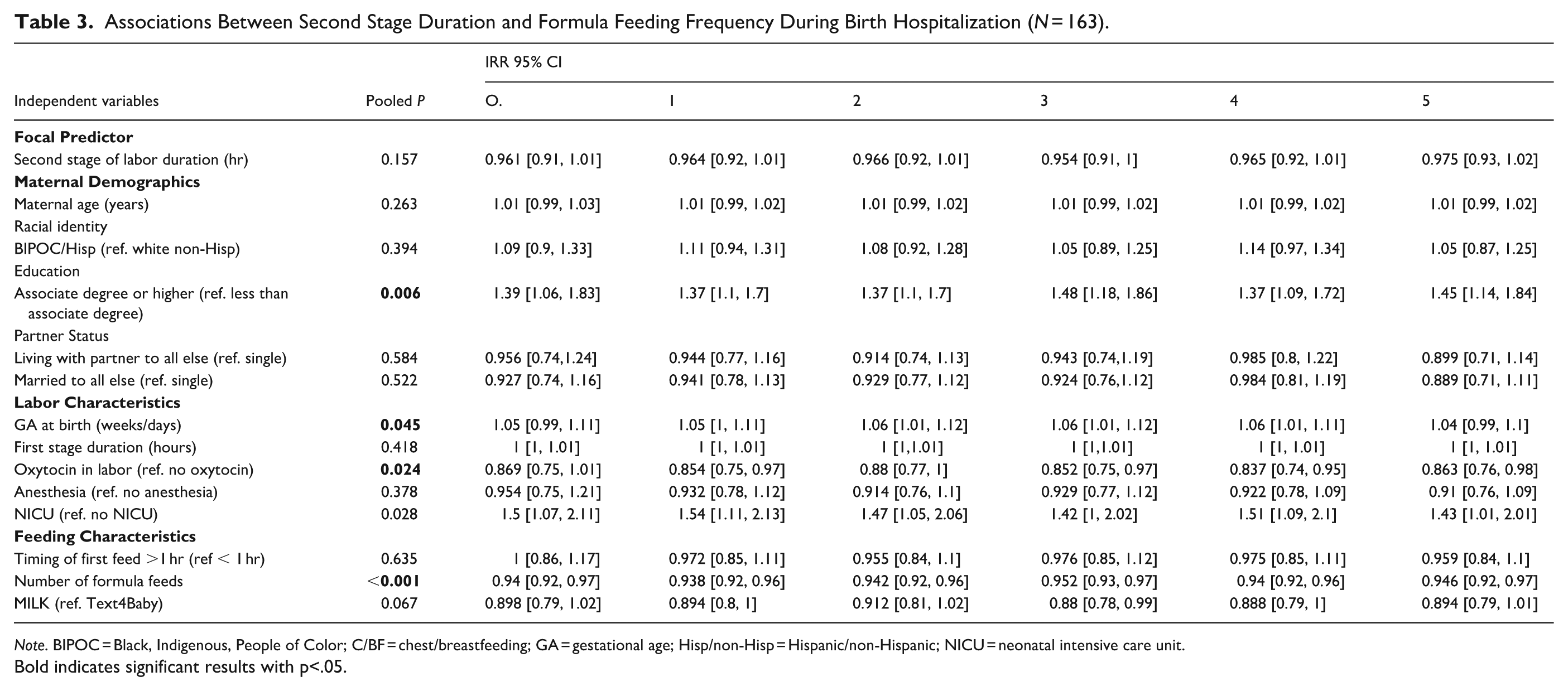
Note. BIPOC = Black, Indigenous, People of Color; C/BF = chest/breastfeeding; GA = gestational age; Hisp/non-Hisp = Hispanic/non-Hispanic; NICU = neonatal intensive care unit.
Bold indicates significant results with p<.05.
The second stage of labor duration was not a significant predictor for frequency of direct C/BF frequency in the 24 hours before birth hospitalization discharge in the Poisson regression model that included covariates, timing of the first feed after birth, and infant formula feed frequency (p = 0.191; Table 4). Lower frequency of direct C/BF was associated with oxytocin use in labor, higher infant formula feed frequency, and NICU admission. Having an associate degree or higher was associated with greater frequency of direct C/BF (Original IRR = 1.39, 95% CI [1.06, 1.83], p = 0.003).
Associations Between Second Stage Duration and Frequency of Direct Chest/Breastfeeding 24 Hours Before Birth Hospitalization Discharge (N = 163).
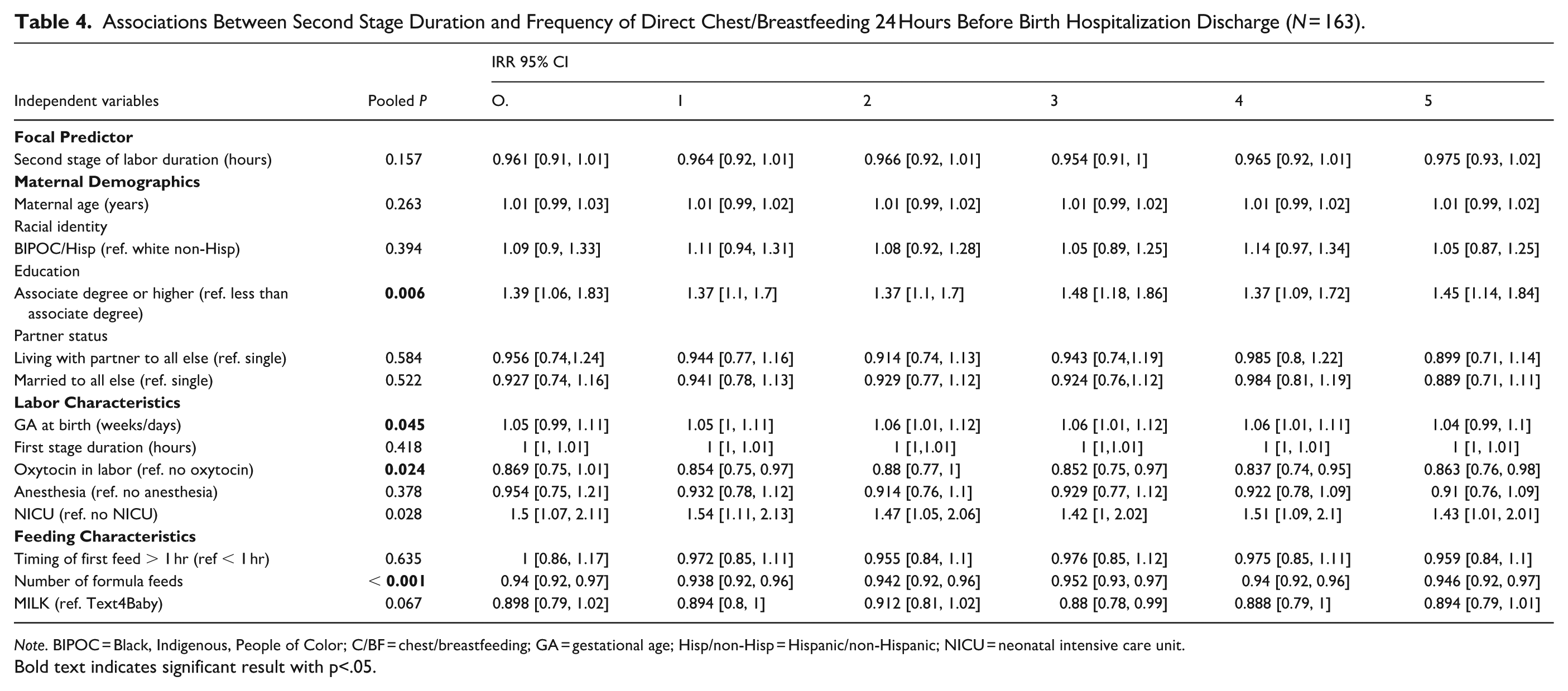
Note. BIPOC = Black, Indigenous, People of Color; C/BF = chest/breastfeeding; GA = gestational age; Hisp/non-Hisp = Hispanic/non-Hispanic; NICU = neonatal intensive care unit.
Bold text indicates significant result with p<.05.
Longer second stage of labor duration was not associated with onset of Lactogenesis II in an unadjusted binary logistic model (pooled unadjusted OR = 0.899, 95% CI [0.7, 1.15], p = 0.405) or in an adjusted model including covariates, timing of first feed after birth, formula feeding frequency, and direct C/BF frequency in the 24 hours before discharge (pooled unadjusted OR = 0.724, 95% CI [0.52, 1.01], p = 0.06). No other covariates were significant predictors of delayed onset of Lactogenesis II.
Discussion
Overall, the results of the analysis did not support our hypothesis that a longer second stage of labor duration is associated with decreased rates of early and exclusive direct C/BF. Participant demographics and labor characteristics appeared to be stronger predictors of some measures of early and exclusive direct C/BF, as was number for infant formula feedings as a predictor for number of direct C/BF in the 24 hours before discharge. The results are consistent with existing evidence demonstrating that a significant proportion of parents who intend to exclusively feed their infants via direct C/BF also supplement with infant formula during birth hospitalization.
Early Direct Chest/Breastfeeding
The second stage of labor duration was not associated with the timing of the first feed after birth. Clinically prolonged second stage of labor (> 3 hours) can contribute to maternal exhaustion, which could delay immediate infant feeding efforts (Türkmen et al., 2020). More notable differences in timing of the first feed may be evident between those who experience clinical prolonged labor compared to those who do not.
We found that when participants received oxytocin in labor, they were more likely to initiate feeding in the first hour after birth. Although oxytocin use has been associated with adverse lactation outcomes in other cohorts (Bryanton et al., 2020)—including lower frequency of direct C/BF in this cohort—oxytocin use does not appear to be disruptive in our cohort when controlling for covariates. Oxytocin dose in labor can impact perinatal outcomes; thus, our findings may have been different if oxytocin use was measured as a continuous variable, rather than binomial.
As observed in the results, NICU admission is associated with later timing of the first feed after birth, and, subsequently, increased formula feeding frequency and decreased direct C/BF frequency. Failure to support early and exclusive breastfeeding among those infants hospitalized in the NICU after birth contributes to an increased likelihood of lactation cessation earlier than planned by the birth/lactating parent (Parker et al., 2020). Dyad separation, stress, use of artificial nipples, preterm birth, and dependence on the use of pumps to express milk (i.e., pump dependence) have all been implicated in decreased lactation goal attainment and continuation. Lactation support interventions that are NICU-specific have demonstrated resolute success in promoting and achieving optimal lactation outcomes following NICU hospitalization for preterm and medically vulnerable infants (Froh et al., 2017).
Infant Formula Use and Direct Chest/Breastfeeding
A longer second stage of labor duration was not associated with infant formula feeding during the birth hospitalization or direct C/BF frequency in the 24 hours before discharge. Although we do not have data regarding length of pushing versus passive descent or “laboring down” during the second stage, a plausible explanation for these findings is that allowing a laboring person to labor down during the second stage of labor does not impair achievement of lactation goals. Importantly, interventions to expedite the second stage of labor by pushing (vs. allowing a birthing person to “labor down”) have been linked with adverse birth outcomes (Zipori et al., 2019) and may also increase the likelihood of infant formula supplementation during birth hospitalization and delayed initiation of direct C/BF.
Notably, 49% of participants in this cohort used infant formula at some point during birth hospitalization despite prenatal intention to exclusively or near-exclusively breastfeed. Indeed, feeding small volumes of infant formula may be consistent with the goals of those who intend to near-exclusively breastfeed. However, infant formula supplementation during birth hospitalization, even in small volumes, has been consistently linked to ongoing infant formula use beyond the immediate postpartum period, interferes with lactation success, and is associated with weaning earlier than the parent intended (Whipps et al., 2021). Further, infant formula feeding frequency was higher in BIPOC and/or Hispanic participants compared to White, non-Hispanic participants. Further, greater direct C/BF frequency was significantly associated with a higher education level. These results reflect the experiences of birth cohorts at other centers and reinforce existing evidence on how structural barriers and postnatal care practices limit an individual’s ability to attain their breastfeeding goals (Chantry et al., 2014; Kair et al., 2019; Morrow et al., 2021).
Our findings offer supporting evidence that use of synthetic oxytocin during labor and anesthesia is associated with decreased breastfeeding exclusivity during the immediate postpartum period, whereas avoidance of inductive agents and unmedicated births are associated with early breastfeeding exclusivity (Bryanton et al., 2020). Both synthetic oxytocin and anesthesia are associated with a cascade of interventions, including Cesarean birth and increased use of fluid boluses to mitigate irregular contractions, uterine hypertonia, and hypotension (Fan et al., 2020; Gomes et al., 2018). The cumulative effects of these labor interventions have been identified as barriers to breastfeeding, including infant formula supplementation in the immediate postpartum period.
An overarching hypothesis has been that initiation of breastfeeding within the first hour after birth promotes early and ongoing exclusivity and attainment of the lactating parent’s own goals (Bryanton et al., 2020; Fan et al., 2020). Surprisingly, in these analyses, the age of the first feed greater than 1 hour after birth was not a significant predictor of our other lactation outcome measures. This finding is consistent with the evidence generated by Parker et al. (2020). In their randomized clinical trial, initiation of milk removal during the first hour after birth was not associated with greater milk volumes among mothers who gave birth to premature infants (Parker et al., 2020). Rather, frequency of milk expression in the immediate postpartum period, versus milk removal initiation timing, may be more predictive of lactation success (Parker et al., 2020).
Delayed Onset of Lactogenesis
Onset of Lactogenesis II, also referred to as secretory activation, depends on hormonal shifts after the placenta detaches from the uterus, and can be interrupted by labor and birth interventions (Peng et al., 2024). Infrequent milk expression and infant formula supplementation can exacerbate challenges related to establishing and maintaining milk supply that arise from delayed onset of lactogenesis (Fan et al., 2020; Peng et al., 2024). Onset of Lactogenesis II can occur any time in the first 7 days after birth, but onset after 3 days (72 hr) postpartum has been linked with later adverse lactation outcomes, including decreased breastfeeding duration and exclusivity in the first year of life (Peng et al., 2024). A model including second stage of labor duration and other covariates was not associated with delayed Lactogenesis II in this cohort. The most plausible explanation for our findings is that we did not have sufficient variability within this cohort in delayed onset of Lactogenesis II, with only 22 (14%) experiencing this, compared to an incidence rate of 23%–44% in the United States.
Limitations
First, the duration of the second stage of labor for most participants was less than 3 hours in this cohort. This may have impacted our ability to detect a significant effect on direct C/BF outcomes among those who experience clinically prolonged second stage of labor. Participants of the MILK Trial had all expressed a prenatal intention to exclusively or nearly exclusively breastfeed, which may explain the results of these analyses, as parents who intend to breastfeed have a tendency to seek out lactation resources to overcome any challenges, which in turn are associated with postnatal lactation preparedness, self-efficacy, and confidence (Demirci et al., 2020). Reason for formula use was not documented, thus a comprehensive understanding of formula supplementation in this cohort could not be described. Oxytocin and anesthesia use in labor were both measured as nominal variables; thus, we were not able to account for dose or duration of use in our analyses, which may have impacted our results. Additionally, we were not able to discern active second stage of labor versus passive or “laboring down.” This distinction should be made in future research. Self-reporting of the onset of Lactogenesis II is an additional limitation, as it was measured with one question instead of other associated sensations asked retrospectively at 1 week postpartum. Furthermore, this was the variable with the largest amount of missing data (17% missing). Lastly, we did not have information on many other factors surrounding the labor experience, including clinicians and support persons attending the birth, which collectively and individually can play significant roles in chest/breastfeeding experiences and practices following birth.
Conclusion
A longer second stage of labor duration was not associated with any lactation outcome measures in the immediate postpartum period. Our findings suggest that interventions to reduce the length of second stage of labor duration may not be essential in the attainment of breastfeeding and lactation goals in the immediate postpartum period. Of note, nearly half of all participants used infant formula despite plans to exclusively breastfeed, indicating that there remain persistent barriers to early breastfeeding exclusivity during birth hospitalization.
Footnotes
Acknowledgements
The authors would like to thank each of the participants for their involvement with this project.
Ethical Considerations
Ethical approval was received from the University of Pittsburgh Human Research Protection Office (study #19050021) and informed consent was obtained before implementation of study procedures. The primary study was registered at ClinicalTrials.gov (NCT02724969).
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The primary study was funded by the National Institutes of Health (NIH), National Institute of Nursing Research (NINR), grant R00 NR015106, “Preventing Perceived Insufficient Milk: Development of a Text Message-Based Intervention,” PI: Demirci. Dr. Jessica Davis was co-sponsored by the Rockefeller University Heilbrunn Family Center for Research Nursing through the generosity of the Heilbrunn Family and the National Center for Advancing Translational Sciences, NIH, through Rockefeller University (Grant # UL1 TR001866); the NIH NINR training grant entitled “Targeted Research and Academic Training Program for Nurses in Genomics Award” (PI: Yvette Conley; Grant # T32NR009759) and the HRSA NRSA T32 training grant entitled “Primary Care Research” (Grant # T32HP22240); Rosemary Berkel Crisp Research Award (Sigma International); and the Margaret E. Wilkes Scholarship (University of Pittsburgh School of Nursing).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.