
Abstract
Background:
Dysphoric milk ejection reflex (D-MER) is a physiologic condition in which some women experience brief but intense negative emotions immediately before or during milk release. Awareness and understanding of D-MER remain limited among both mothers and healthcare providers, and qualitative evidence on women’s experiences of dysphoric D-MER remains limited.
Research Aim:
The aim of this study was to explore the experiences and coping strategies and support the needs of women with D-MER during breastfeeding and/or expressing milk.
Methods:
A qualitative descriptive design was employed. Six women in Türkiye who reported at least two D-MER symptoms were recruited using convenience sampling. Data were collected through in-depth online interviews between February and June of 2024 and analyzed using inductive thematic analysis.
Results:
Four main themes emerged: (a) valuing breastfeeding despite emotional discomfort—breastfeeding was generally valued yet negatively affected by D-MER; (b) onset, duration, and nature of D-MER symptoms—symptoms such as restlessness, unhappiness, irritability, chest tightness, and longing occurred within the first few minutes of milk flow and resolved quickly; (c) coping through distraction and social support—distraction techniques and social support were most frequently used; and (d) desire for recognition and nonjudgmental support—women desired greater understanding, nonjudgmental support, and recognition of D-MER in healthcare settings.
Conclusion:
D-MER can undermine the emotional experience of breastfeeding despite women’s desire to continue. Healthcare providers should be able to recognize D-MER, differentiate it from postpartum depression, and provide individualized education, reassurance, and practical coping guidance.
Introduction
Lactation is a natural process for many mothers, serving as a physiologic response of the body to meet the nutritional needs of the infant. The literature has examined the medical and physical difficulties that may predict early breastfeeding cessation, but little attention has been paid to the emotional experiences that may influence breastfeeding outcomes (Cox, 2010; Deif et al., 2021; Heise & Wiessinger, 2011; Ureño et al., 2018). During milk ejection, mothers may experience discomfort characterized by distressing feelings. This condition is referred to in the literature as dysphoric milk ejection reflex (D-MER). D-MER is characterized by discomfort that can begin within seconds of starting to breastfeed and typically diminishes after 5–10 minutes (Cox, 2010; Heise & Wiessinger, 2011; Uvnas-Moberg & Kendall-Tackett, 2018). This condition often causes women to experience emotional feelings such as unhappiness, sadness, irritability, guilt, hopelessness, and a desire to stop breastfeeding (Heise & Wiessinger, 2011). Symptoms typically begin within seconds of milk ejection and resolve within 5–10 minutes. In some women, symptoms may decrease in intensity after approximately 3 months, whereas in others, symptoms may persist throughout the breastfeeding period (Cox, 2010; Deif et al., 2021). Although D-MER is characterized by distressing emotional symptoms, these experiences are closely linked to the timing of milk ejection and occur within seconds of milk release, resolving shortly thereafter. This consistent temporal pattern suggests that D-MER symptoms are associated with underlying physiologic processes involved in the milk ejection reflex rather than reflecting a primary psychological condition (Ureño et al., 2018). Current understanding of the physiologic mechanisms underlying D-MER remains limited and largely hypothetical. Although neuroendocrine processes involved in the milk ejection reflex have been proposed as potential contributors, there is insufficient biologic evidence to confirm dopamine or oxytocin as definitive mediators of D-MER. The dopamine-related explanation, initially proposed by Heise and Wiessinger (2011), is primarily supported by behavioral and observational findings rather than direct physiologic measurement (Deif et al., 2021; Liu et al., 2023; Moriyama et al., 2024; Ureño et al., 2018). Similarly, hypotheses involving oxytocin remain theoretical, highlighting the need for further biologic research to clarify the mechanisms underlying D-MER.
It has been reported that mothers experiencing D-MER may have a negative breastfeeding experience due to distressing feelings, leading some to stop breastfeeding or to continue with difficulty (Lynn Herr et al., 2024). Recognizing and understanding this phenomenon, although rare, are important for all healthcare professionals. They should be able to offer solutions to manage these difficulties effectively.
Despite growing recognition of D-MER in the literature, current knowledge remains largely based on case reports, surveys, and theoretical discussions, with limited qualitative evidence capturing women’s lived experiences. As a result, healthcare professionals may struggle to recognize D-MER, differentiate it from postpartum mood disorders, and respond appropriately to women’s distress. Qualitative research is needed to explore how women perceive, interpret, and cope with D-MER symptoms in their daily breastfeeding and milk expression practices. Such insight may inform more empathetic, individualized lactation support and help women feel understood, validated, and better supported during the breastfeeding process.
This study focuses on the breastfeeding experiences of women with D-MER, a condition about which we still have limited information, and aims to contribute to the literature on this topic.
Methods
Design
This study employed a qualitative descriptive design to explore the experiences of women with D-MER, a methodology appropriate for obtaining straightforward descriptions of phenomena about which limited prior research exists (Kim et al., 2017). A qualitative descriptive approach was selected to provide a comprehensive summary of participants’ experiences in their own words without imposing an interpretive theoretical framework. The study was reported in accordance with the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines to enhance transparency and methodologic integrity (Baltacı, 2019; Tekindal & Uğuz Arsu, 2020).
Setting and Relevant Context
This study was conducted in Türkiye, where breastfeeding initiation rates are high; however, exclusive breastfeeding rates decline within the first 6 months postpartum (Hacettepe University Institute of Population Studies, 2019). Breastfeeding is socially and culturally supported, and women may experience expectations regarding continuation.
Participants were recruited through social media platforms, which are commonly used by women of reproductive age in Türkiye. Awareness and formal recognition of D-MER within routine maternal and lactation care remain limited in the literature (Ureño et al., 2018). Consequently, women experiencing D-MER symptoms may seek information and support through informal networks or online communities.
Participants and Recruitment
Participants were recruited using convenience sampling through invitation posts shared on the researchers’ personal social media accounts (i.e., Instagram and Facebook). The posts briefly described the study purpose and eligibility criteria. The invitation was further disseminated by midwives with large professional followings, expanding the reach of recruitment.
Women who expressed interest contacted the first author via direct message. All interested women were invited to participate in a brief online screening interview conducted via Zoom or telephone by the first author. During this screening, eligibility criteria were assessed based on participants’ self-reported symptoms and their temporal relationship with milk ejection.
Eligibility criteria included (a) age 18 years or older, (b) ability to communicate in Turkish, (c) self-report of at least two characteristic D-MER symptoms (e.g., sudden sadness, irritability, anxiety, restlessness, tearfulness, or a sense of inner overwhelm occurring within seconds of milk ejection and resolving spontaneously within minutes), and (d) willingness to participate in an in-depth interview.
Eligible participants then were provided with detailed study information and a written informed consent form via email. Written informed consent was obtained prior to scheduling the full in-depth interview. Women who did not meet eligibility criteria were thanked for their interest and not included in further stages of the study.
Fifteen women initially expressed interest. After screening, six women met inclusion criteria and were included in the study. Nine women were excluded because their reported symptoms did not occur in temporal association with milk ejection and therefore did not meet the operational criteria for D-MER.
Data Collection
Data were collected between February and June of 2024 through individual, semi-structured interviews conducted via Zoom or Google Meet. All interviews were conducted in Turkish by the first author (AIG). No third parties were present. Interviews lasted between 30 and 60 minutes and were audio recorded with participants’ permission. Field notes were taken during and immediately after each interview. All interviews were transcribed verbatim in Turkish on the same day. Transcripts were reviewed for accuracy by the second author (NKO).
Data-Collection Tools
Information Form
Sociodemographic and breastfeeding-related information was collected through a brief self-report form completed by participants prior to the interview.
Semi-structured Interview Form
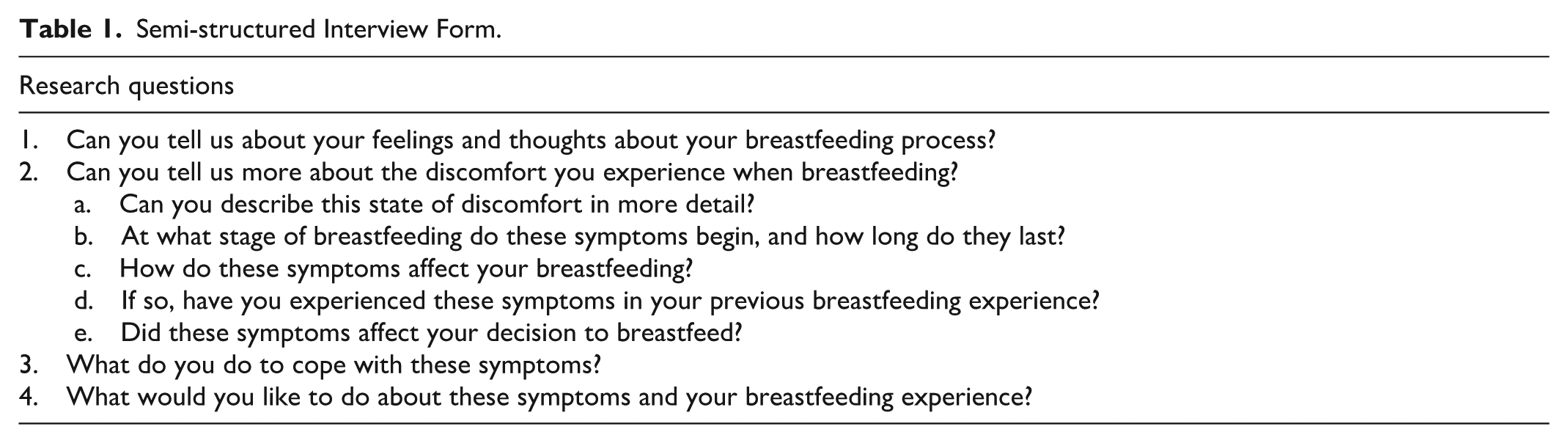
The study used a semi-structured interview form consisting of four main questions and five subquestions developed based on the relevant literature (Table 1). A pilot interview was conducted with two women who met the study’s inclusion criteria to evaluate the clarity and relevance of the interview guide. Minor revisions were made for clarity. Data obtained from the pilot interviews were not included in the final analysis.
Semi-structured Interview Form.
Data Analysis
Data were analyzed using inductive thematic analysis. Analysis began with line-by-line coding of each transcript to identify meaning units relevant to the research aim. Both researchers independently coded the first two transcripts to develop an initial coding framework. Codes were generated inductively without predefined categories and were documented in Microsoft Word and Excel tables to organize and compare coding across transcripts. A codebook was developed and refined iteratively as new codes emerged.
Subsequently, codes were compared within and across transcripts to identify similarities, differences, and patterns. Related codes were grouped into subthemes and then abstracted into overarching themes through iterative discussion and consensus meetings. Coding discrepancies were discussed until agreement was reached.
Field notes were reviewed alongside transcripts during analysis to provide contextual understanding and support interpretation of participants’ narratives. An audit trail was maintained throughout the process to document coding decisions, theme development, and analytic reflections.
No qualitative data-analysis software was used; coding and data management were conducted manually using secure digital documents. Data collection and analysis occurred concurrently. Recruitment ceased when no new codes or themes emerged, indicating data saturation.
Researcher Positionality
The first author (AIG) is an assistant professor of midwifery with 3 years of clinical experience in maternal and breastfeeding care and 2 years of academic experience in qualitative research. The second author (NKO) has academic experience in qualitative research methodology and maternal health. Both researchers have professional backgrounds in midwifery and maternal care, which may influence their perspectives on breastfeeding and maternal health experiences.
The researchers had no prior relationship with the participants. During recruitment and interviews, participants were informed about the purpose of the study, the researchers’ professional backgrounds, and the voluntary nature of participation. To minimize potential bias, the researchers engaged in reflexive discussions throughout data collection and analysis, acknowledging their professional assumptions regarding breastfeeding and striving to remain open to participants’ diverse experiences.
Methodologic Integrity
Trustworthiness was established using the criteria of credibility, dependability, confirmability, and transferability. Credibility was enhanced through prolonged engagement with the data, independent coding by the two researchers, and regular consensus meetings to discuss emerging codes and themes. An external researcher with expertise in breastfeeding research reviewed the developed themes to provide peer debriefing. In addition, one participant reviewed the preliminary findings to confirm that the themes accurately reflected her experience (i.e., member checking).
Dependability was supported by maintaining a detailed audit trail documenting analytic decisions, code development, theme refinement, and discussions between researchers throughout the analysis process. Confirmability was strengthened through reflexive dialogue between the researchers regarding their professional backgrounds in maternal health and potential assumptions related to breastfeeding experiences. Coding disagreements were resolved through discussion until consensus was reached.
Transferability was supported by providing detailed descriptions of participant characteristics, recruitment context, data-collection procedures, and illustrative quotations to enable readers to assess the applicability of findings to other settings.
Ethical Considerations
The study was approved by the Istanbul University–Cerrahpaşa Social and Humanitarian Studies Ethics Committee. In addition, the study was designed in accordance with the Declaration of Helsinki.
To maintain confidentiality, participants were assigned identification codes (e.g., Moms 1–6), and no identifying information was included in transcripts or reports. Digital recordings and transcripts were stored on a password-protected computer accessible only to the research team. Any potentially identifying details were removed during transcription. Participants did not receive financial or material compensation for participation.
Results
Participant sociodemographic and breastfeeding characteristics were as follows: the mean age was 28.5 years (SD = 2.36), and the mean age of infants was 7.0 months (SD = 3.31). Three participants were university graduates, four had one child, and four had male infants. Four participants breastfed exclusively, and three initiated breastfeeding immediately after birth.
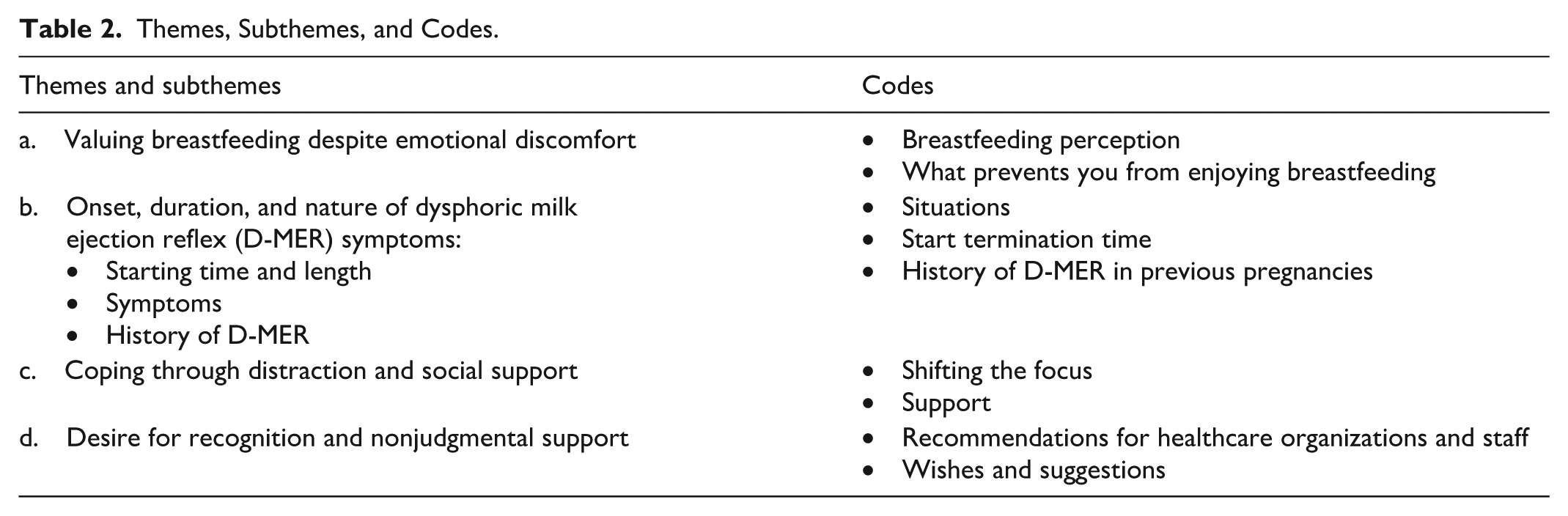
Four themes and four subthemes were identified based on participants’ D-MER experiences. The main themes were (a) valuing breastfeeding despite emotional discomfort, (b) onset, duration, and nature of D-MER symptoms, (c) coping through distraction and social support, and (d) desire for recognition and nonjudgmental support. The main themes, subthemes, and codes created are shown in Table 2.
Themes, Subthemes, and Codes.
Theme 1: Valuing Breastfeeding Despite Emotional Discomfort
This theme includes expressions about participants’ breastfeeding processes and D-MER experiences. Although participants described breastfeeding as a positive experience, they also reported that D-MER symptoms negatively affected this process.
I feel some emotions when I start breastfeeding, but I cannot say that breastfeeding is bad for me because of that. Because it goes away after a while. (Mom 1) Breastfeeding is good, my son has a little difficulty sucking, but I try to breastfeed because I know that breast milk is very important. It’s nice, but it’s hard to breastfeed everywhere. Or it’s hard to breastfeed at night. I’m so overwhelmed. (Mom 3) How good it feels to breastfeed. I actually breastfed my other daughter, I breastfed my other daughter until she was 1 year old, but breastfeeding with this daughter is a bit difficult for me. It is difficult [because] after my daughter grabs the breast, I feel a bit restless and nervous. I want to stop breastfeeding as soon as possible. (Mom 5)
Theme 2: Onset, Duration, and Nature of D-MER Symptoms
This theme included statements about how participants defined their D-MER experience, when it started, and how long it lasted. These statements were grouped into three subthemes: (a) starting time and length of D-MER symptoms, (b) symptoms, and (c) history of D-MER.
Subtheme 1: Starting Time and Length
This subtheme includes participants’ reports of when D-MER symptoms began and ended and how long they lasted. Participants reported that the discomfort they experienced occurred in the first few minutes of breastfeeding or expressing milk and disappeared in the later stages of breastfeeding/expressing milk.
When he first starts to suckle, that is when the first milk starts to flow, but after a few minutes, it passes when the flow of milk increases. For example, I had to express my milk a few times. I can explain more clearly when I think about that time. At first the milk flows slowly, then I feel uncomfortable and overwhelmed. Then the amount of milk increases or the flow speeds up, [and] then it passes. (Mom 1) It starts when I start breastfeeding. I think it lasts 5 minutes. It starts when my son starts to suckle [and] it is the same when I express milk. I have the same crying feeling when I express for the first time. (Mom 4) At first, after my son has latched on and expressed milk 4 or 5 times, it usually gets easier. It seems to happen when the space holds the breast completely and the milk starts to flow; that is, when there is an order. I think for 3 or 4 minutes and then it does not happen again, but I feel it at the beginning of each feeding. (Mom 6)
Subtheme 2: Symptoms
This subtheme includes participants’ statements about the D-MER symptoms they experienced during breastfeeding/milking experience. It is seen that the most prominent symptoms are restlessness, distress, and overwhelm.
For example, it happens at the time of birth, you know, when the midwives come to examine you. At that time there is a feeling of escaping from there, you want it to end as soon as possible, like restlessness, reluctance. I feel unhappy, panicky, and restless when my baby clings to the breast in the first few minutes of breastfeeding. (Mom 2) The pump is in massage mode at first, the milk begins to flow slowly, it starts at this stage. In fact, I suddenly feel tight inside. I want to cry. (Mom 3) I’m experiencing an intense feeling of crying. Suddenly I felt like I wanted to cry. Or I felt like snapping at everyone. I wanted to say get out of here, go away. I want to be alone; for example, I’m angry. I thought of my mom when I wasn’t thinking at all. I missed my mom and my home. (Mom 5)
Some participants reported experiencing D-MER symptoms not only while breastfeeding but also while expressing milk.
Yes, I have the same sensations when breastfeeding and expressing milk. (Mom 3) It starts when my son starts to suckle or it is the same when I express milk. I have the same crying feeling when I express milk for the first time. (Mom 4) I feel the same anxiety and restlessness just after my period. I’m experiencing the same inner overwhelm. It really looks like it. I didn’t want to stop breastfeeding, but once or twice I thought I should express and bottle feed. But I experienced the same things when I was breastfeeding, so nothing changed. (Mom 6)
Subtheme 3: History of D-MER
This subtheme included statements about participants’ experiences of D-MER symptoms in their previous pregnancies.
I never had anything like this with my daughter. It was 4 or 5 years ago. I could breastfeed my other child very little, but I did not feel anything like this during that time. (Mom 3) My complaints were only with this daughter. (Mom 5)
Theme 3: Coping Through Distraction and Social Support
This theme includes participants’ statements about their methods of coping with D-MER symptoms. Participants reported difficulties in continuing breastfeeding and using distraction methods and that social support was effective in managing these symptoms.
When I first feel it, yes, I want to stop, but I hold myself back. (Mom 1) I thought about using a silicone tip [nipple shield], thinking it might make me feel better. But it didn’t work very well. (Mom 2) I tried to stay calm, take deep breaths, and get through it with the support of the people who were with me. If someone is with me, I talk to them. If there was no one, I would answer the phone. (Mom 3) I play on the phone or watch TV while breastfeeding, or I try to close my eyes and rest for a while. (Mom 4)
Theme 4: Desire for Recognition and Nonjudgmental Support
Under this main theme, there are statements about participants’ recommendations, wishes, and suggestions for D-MER. It was emphasized that women need to be understood and that breastfeeding should not be a means of putting pressure on women.
I would like the breastfeeding centers of the hospitals to be more active and to provide services at home because it is difficult for new mothers to go to these centers with their babies. (Mom 2) I wish there were special therapy centers for breastfeeding, or not wanting to breastfeed, not being able to breastfeed, etc. For example, everyone is prejudiced in this regard, and breastfeeding counselors act as if we must always love breastfeeding and be happy while breastfeeding. In our society, it is always a bad mother who cannot breastfeed, and if you have these feelings, you are even worse. (Mom 3) I want to be understood. I don’t know exactly why I feel this way, but it would be nice to find out. (Mom 4) I would like people’s perceptions to change. Not everyone has to like breastfeeding. I would like it to be recognized, and efforts should be made to make it popular or to find out what the problem is. Otherwise, we want to breastfeed, but we cannot get help for these difficulties or we do not even know if it is a disease. (Mom 6)
Discussion
The findings of this study highlight several key aspects of women’s experiences with D-MER. Although participants valued breastfeeding and wished to continue, the sudden and intense negative emotions associated with milk ejection created significant emotional discomfort. Symptoms were reported to occur within the first minutes of breastfeeding or milk expression and resolved quickly thereafter. Participants commonly used distraction strategies and relied on social support to cope with these experiences. Participants also expressed a strong desire for greater recognition and understanding of D-MER within healthcare settings.
The milk ejection reflex is an important part of milk production. It is a neuroendocrine reflex evoked by stimulation of the nipple and areola. When milk release is accompanied by symptoms of dysphoria, it is called D-MER (Ahmed et al., 2024; Skowrońska et al., 2022). Women with D-MER only experience dysphoria during milk release. In most women, dysphoria only occurs in the presence of the milk ejection reflex and may occur even when there is no contact with the breast or areola (Heise & Wiessinger, 2011; Uvnas-Moberg & Kendall-Tackett, 2018). One case report indicated that direct sucking stimulation of the nipples was not necessary for the onset of D-MER-related sensations (Heise & Wiessinger, 2011). In the studies on D-MER in the literature, only the symptoms in breastfeeding women were investigated, and milk expression was not questioned. In this study, as a contribution to the literature, it was reported that women both breastfeeding and expressing milk experienced D-MER symptoms in similar ways.
It has been observed in the literature that many women experiencing D-MER share similar emotions, often experiencing anxiety, sadness, irritability, restlessness, tearfulness, anger, longing, and inner overwhelm (Deif et al., 2021; Frawley & McGuinness, 2023; Stacey, 2020; Uvnas-Moberg & Kendall-Tackett, 2018). Kacır et al. (2024) reported that women often experienced nausea in addition to feelings of tension, exhaustion, intolerance, and restlessness. In this study, similar to the literature, it was observed that women often felt overwhelmed and experienced shortness of breath, restlessness, unhappiness, irritability, chest tightness, tension, and longing; however, no gastrointestinal symptoms such as nausea were reported. These symptoms often occur with the onset of the milk ejection reflex and last less than 5 minutes (Heise & Wiessinger, 2011; Skowrońska et al., 2022). Symptoms may decrease 3 months after birth or persist during breastfeeding (Deif et al., 2021). Similar to the literature, it was observed that the symptoms of the women in the study occurred in the first few minutes and disappeared after about 5 minutes. Because the women in this study were actively breastfeeding, no conclusion could be drawn as to the time of resolution of D-MER symptoms.
D-MER is a condition associated with a range of negative emotions of varying intensity, including feelings such as longing, sadness, irritability, and anger (Deif, 2024; Heise & Wiessinger, 2011; Moriyama et al., 2024). Some participants in this study reported that they had not experienced D-MER during previous breastfeeding experiences. Similar observations have been reported in earlier studies, where women described D-MER symptoms occurring in one lactation period but not in another (Heise & Wiessinger, 2011; Liu et al., 2023; Uvnas-Moberg & Kendall-Tackett, 2018). These findings suggest that the occurrence of D-MER may vary between pregnancies. Potential explanations for this variability may include differences in hormonal regulation, infant sucking patterns, maternal physiologic responses, or contextual factors such as stress and environmental conditions (Deif et al., 2021; Tong et al., 2007). However, some studies also have reported recurrent cases of D-MER across multiple lactation periods, suggesting that individual physiologic differences may influence symptom persistence (Deif et al., 2021).
This variability also has potential clinical implications. Women who have experienced D-MER during one breastfeeding period may be encouraged to attempt breastfeeding in subsequent pregnancies because the condition may not necessarily recur.
There are not enough studies with high evidence value in the literature on the methods that can be used to alleviate the symptoms of D-MER and allow mothers to cope with the process (Deif, 2024; Ureño et al., 2018). Some studies have stated that lifestyle changes (e.g., nutrition, adequate water consumption, adequate sleep, etc.), distraction methods (watching TV, listening to music, chatting, being interested in the phone, etc.), and social support are effective (Kacır et al., 2024; Skowrońska et al., 2022; Ureño et al., 2018). Similar to the literature, this study found that women often resorted to reading books, using the phone, chatting, breathing exercises, and spousal support.
Although there are different methods to facilitate the process, the lack of knowledge of women and health professionals about D-MER makes it difficult to manage the process. It is known that women stop breastfeeding or try to continue the process as a duty due to the emotional difficulties they experience during breastfeeding (Ahmed et al., 2024; Kacır et al., 2024; Lynn Herr et al., 2024; Moriyama et al., 2024; Skowrońska et al., 2022). In this study, it was observed that women believed that breast milk was the most beneficial food for their babies and therefore continued breastfeeding despite symptoms.
It is vital that healthcare professionals involved in perinatal and breastfeeding care are able to recognize and define D-MER. It is important for women to know the cause of the difficulties they are experiencing and to receive support and counseling to help them cope. Women who do not know that the condition they are experiencing is a physiologic disorder see themselves as inadequate and bad (Heise & Wiessinger, 2011; Skowrońska et al., 2022). In this case, their stress levels increase, and their processes become more difficult (Deif et al., 2021; Heise & Wiessinger, 2011; Ureño et al., 2018). Moriyama et al. (2024) found in their study that women experiencing D-MER do not know what this condition is, why it occurs, and what to do. They found that after receiving information about the phenomenon, these women found it easier to cope with the symptoms and preferred to continue breastfeeding rather than stop. These women also reported feeling more understood and supported by those around them after recognizing D-MER. In this study, women suggested that they wanted D-MER to be recognized and to receive support from healthcare professionals. They also said that they wanted their experiences to be understood and supported by those around them.
Our findings highlight the need for routine screening for D-MER symptoms during lactation counseling sessions. Healthcare providers, especially midwives and lactation consultants, should be trained to recognize the physiologic nature of D-MER and differentiate it from postpartum depression. Incorporating practical coping techniques such as guided breathing, engaging in conversation, or using media for distraction into breastfeeding support can help mitigate the emotional burden. Establishing peer support networks and ensuring nonjudgmental communication may further enhance maternal well-being and breastfeeding continuation.
Conclusion
This study was conducted to explore the experiences of women with D-MER, how they define the symptoms of D-MER, when and how those symptoms occur, and the severity and duration of those symptoms. It also explored women’s coping strategies, social support mechanisms, and health service needs. The findings draw attention to the experiences and needs of women experiencing this condition. Due to the lack of awareness and evidence-based literature on D-MER and the similarity of symptoms, D-MER may be confused with postpartum depression or go undiagnosed. It is therefore important to educate the public, healthcare professionals involved in maternal and infant health, and breastfeeding counselors about D-MER. Effective studies with high levels of evidence are needed to prevent and relieve the symptoms of D-MER.
Strengths and Limitations of the Study
This study contributes qualitative evidence from Türkiye regarding the experiences and support needs of women with D-MER using a qualitative descriptive design. The inclusion of women who experienced D-MER during both breastfeeding and milk expression provides additional insight into the phenomenon across different lactation contexts. The use of rich, participant-derived quotations enhances transparency and supports the credibility of findings. Several limitations should be considered when interpreting the results. First, as a qualitative descriptive study with a small sample size, the findings are not intended to be generalizable but rather to provide in-depth insight into participants’ experiences. The use of convenience sampling through social media may have introduced self-selection bias because women who were more distressed or more motivated to share their experiences may have been more likely to participate. Second, data were collected through online interviews, which may have influenced the depth of interaction compared with face-to-face interviews. Although participants joined from private settings, variations in internet connectivity or environmental factors may have affected the interview process.
Third, D-MER experiences were identified based on participants’ self-reports and screening interviews rather than clinical diagnosis or standardized measurement tools. Currently, there is no validated diagnostic instrument for D-MER, and the absence of objective physiologic measures may limit the precision of classification. In addition, psychological or psychiatric history was not formally assessed, which limits our ability to fully differentiate D-MER symptoms from other mood-related conditions.
Finally, data were collected at a single time point, and changes in symptom intensity across different stages of lactation were not examined. Future research using longitudinal designs, larger and more diverse samples, and biologic or standardized assessment tools may provide a more comprehensive understanding of D-MER.
Footnotes
Acknowledgements
We thank the mothers who shared their experiences.
Ethical Considerations
This study was approved by the Social and Human Sciences Research Ethics Committee of Istanbul University–Cerrahpaşa Faculty of Health Sciences (Approval date: February 17, 2025; Protocol No. E-74555795-050.04-1229623). The study was conducted in accordance with ethical principles for research involving human participants.
Consent to Participate
All participants were informed about the purpose, methods, and procedures of the study before participation. Written and verbal informed consent was obtained from all participants prior to data collection. Participation was voluntary, and participants were informed of their right to withdraw from the study at any time without penalty or adverse consequences.
Consent for Publication
The participants were informed that the results of the study would be published in a scientific journal. They provided consent for the anonymous publication of their responses. No identifying personal information is disclosed in the publication.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are not publicly available due to ethical considerations and privacy restrictions related to participant confidentiality. Data are available from the corresponding author on reasonable request and with approval from the institutional ethics committee.