
Abstract
Human milk is the optimal source of nutrition for infants, especially those born preterm or requiring neonatal intensive care unit care, offering physiologic and psychological benefits for both infants and lactating parents. Despite its importance, access to high-quality electric breast pumps remains a barrier, particularly for underserved populations. To address this, the Lactation Group (LG) at Henry Ford Hospital, a large urban hospital in Detroit, established a Pump Program providing electric pumps to parents facing financial, insurance, or logistical challenges. In the United States, access to durable medical equipment such as breast pumps often depends on insurance coverage, eligibility, and administrative processes, causing delays for many families. The program offers personal-use pumps for long-term needs and hospital-grade loaner pumps for neonatal intensive care unit families or those with lactation difficulties. Lactation consultants assess eligibility, coordinate with insurers or community programs, and provide hands-on education and emotional support. Since 2015, the Pump Program has served more than 1,400 families, maintaining high demand and positive feedback. It integrates through postpartum and intensive care workflows, ensuring continuity of lactation support during medical complications. By providing the necessary tools and addressing structural inequities, the program enhances access to human milk and promotes equitable infant nutrition. Its success highlights the vital role of hospital-based lactation support and offers a model for other urban hospitals aiming to improve health outcomes for families and infants.
Introduction
A high-quality, effective electric breast pump is an essential medical device for lactating individuals when caring for an infant in the neonatal intensive care unit (NICU). Human milk is the optimal form of nutrition and is associated with numerous health benefits, including a reduced risk of asthma, obesity, type 1 diabetes, and sudden infant death syndrome. Infants who receive breastmilk are also less likely to experience ear infections and gastrointestinal illnesses, including necrotizing enterocolitis (Ip et al., 2007). Benefits also extend to psychological well-being for both mothers and infants (Chantry et al., 2015; Meek & Noble, 2022). These benefits include a reduced risk of postpartum depression (Henshaw et al., 2015) and enhanced maternal well-being and emotional stability through stress reduction and promotion of relaxation (Whitley et al., 2020). Additionally, oxytocin strengthens the maternal–infant bond, fostering affectionate behaviors and a deeper emotional connection. These effects also help mothers experience a sense of purpose and control, reducing feelings of helplessness (Tucker & O’Malley, 2022). Furthermore, human milk nutrients are tailored to the infant’s developmental stages (Perrella et al., 2021), making it the ideal food at the right gestational age and supporting the development of a strong immune system (Cacho & Lawrence, 2017; Parker et al., 2021). Notably, infants born preterm and those admitted to the NICU may lack the physiologic capacity to breastfeed due to prematurity or medical complications. Without a breast pump, they would miss out on the benefits of human milk; therefore, an electric breast pump becomes a critical device that enables lactating individuals to provide essential nutrients to their infants through expressed human milk.
Despite clear evidence of the numerous benefits of human milk, significant socioeconomic inequities persist for lactating individuals (Alghamdi et al., 2017; Beauregard et al., 2019; Boundy et al., 2017). Many of our patients, ~69% of whom are enrolled in Medicaid, experience limited access to comprehensive maternity care, lactation support, and postpartum services. Economic pressures often force them to return to work as early as 6 weeks postpartum, often to jobs that lack paid family leave, workplace lactation accommodations, or schedule flexibility (Hallowell et al., 2016; Modak et al., 2023; Parker et al., 2021). These structural barriers disproportionately affect low-income families and contribute to disparities in breastfeeding initiation and continuation rates. The known disparities in human milk provision may stem from this early return to work within the first 6 months of an infant’s life, a critical period when human milk is most vital. This underscores the essential role a breast pump plays in ensuring infants receive this critical nourishment (Chamberlain et al., 2016; Nardella, 2024; Patel et al., 2019). By providing access to high-quality electric breast pumps, healthcare providers can help reduce inequities in human milk provision and improve lactation outcomes.
Obtaining a high-quality electric breast pump can be challenging for lactating individuals with limited resources (i.e., lack of insurance or limited income). For many parents in low-resource settings, purchasing or renting an electric breast pump is cost prohibitive. Personal-use double electric breast pumps range from $150 to $300, with premium brands costing as much as $400 to $800. Single electric pumps, while more affordable (e.g., $60 to $150), are suitable for those who pump occasionally or temporarily and have an established milk supply. Furthermore, those with preterm or sick infants in the NICU need to pump often and frequently to establish and maintain milk production, making a double electric breast pump essential (Palmquist et al., 2019; Parker et al., 2021). For infants born very preterm (i.e., <32 weeks gestation), a hospital-grade pump is recommended due to its consistent suction power and durability (Meier et al., 2011), but these pumps cost between $1,200 and $1,800 or can be rented for $70 to $80 per month.
Many insurance companies provide access to an electric breast pump, but there are often administrative burdens, such as complicated reimbursement requirements, or sparce information about the benefits of using an electric pump. Few community resources are available that provide access to an electric breast pump. The Women, Infants, and Children (WIC) program offers pumps on loan, but the demand far exceeds the supply, operating hours are limited, awareness of the program is lacking, and often transportation constraints hinder access to the service. Lactating individuals who have Medicaid insurance are limited to one pump every 5 years regardless of the condition of the pump or number of children born in that timeframe. The benefit is also not available to those with emergency services Medicaid. Further complicating the provision of these pumps is the complicated paperwork and lack of education on how to access the benefit, and for those who speak English as a second language, often information and guidance are not available in their primary language.
Key Messages
Access to high-quality, electric breast pumps is a vital resource for birthing individuals who wish to provide human milk to their infant hospitalized in the Neonatal Intensive Care Unit (NICU) or when a high-quality pump is not accessible by other means (e.g., insurance, WIC, self-pay).
The breast pump program at a large, urban safety net hospital improved equitable access to high-quality, electric breast pumps to more than 1400 birthing persons.
As the first program of its kind in a large urban hospital, this initiative reflects a deep commitment to prioritizing the health and wellbeing of lactating individuals and their infants.
Lastly, there is a significant lack of understanding within the postpartum community about the quality and differences between breast pumps. Many parents are confused about what kind of pump is most appropriate and often purchase one prenatally that does not suit their situation, particularly if they did not anticipate a preterm birth. A lactating individual’s response may differ by pump type and quality; thus, individualized assessment and support are essential components to understanding what pump type is recommended. Insurance providers may issue a lower-quality pump regardless of known ratings. Cheaper models often break or function poorly, and even if warranties cover the faulty pump, a lactating individual could be left without a working device during the replacement process, further compromising their milk supply. Using the right pump for specific circumstances is critical to helping lactating individuals establish and maintain a healthy milk supply, especially when separated from an infant admitted to the NICU.
Clinical Innovation
The Lactation Group (LG) at Henry Ford Hospital provides lactation support to families whose infant was delivered at or was transferred to this hospital. The team includes international board-certified lactation consultants (LCs), offering assessment, intervention, education, and recommendations to support families in their breastfeeding journey. The LG develops and implements staff training and quality-improvement projects related to supporting, protecting, and promoting breastfeeding and the provision of human milk. The Pump Program was established in response to a growing need for high-quality electric breast pumps that lactating individuals were unable to access. The program was first launched in 2015 with grant funding from a private foundation to purchase several breast pumps. As the program grew, provision of the pumps became more limited due to pump attrition and challenges associated with the COVID-19 pandemic, including reduced staffing and loss of funding. In 2023, new funding was secured to replenish lost and broken pumps through an internal pediatric hospital fund. Systematic data collection was implemented after the program was restarted in 2023; therefore, data from the earliest years of the program are not available for analysis.
Two types of pumps are offered through the Pump Program: (a) a personal-use pump and (b) a loaner-use pump. Prior to allocating either pump to an individual, LCs work with families to obtain a pump through known programs (e.g., personal insurance, WIC, etc.). If an appropriate pump cannot be obtained through these programs, then the family becomes eligible to receive a pump through the hospital program, ensuring that lactating parents in need have access to a high-quality electric breast pump.
1. Personal-use pump. Through this mechanism, lactating parents are provided with a double electric personal-use pump with all the necessary parts for pumping. Those who are experiencing difficulties with breastfeeding, facing challenges with milk supply, who have infants with an identified medical need for supplementation, or who are separated from their infant due to a NICU admission (e.g., >32 weeks) are eligible. The LC identifies eligible parents through their daily rounding and consults with providers. Eligibility for receipt of this personal-use pump may include, but are not limited to, the following reasons:
a. A lactating parent with no insurance who is not WIC eligible b. A lactating parent who is eligible for WIC, but a WIC pump is not accessible due to long weekend/holiday or availability c. A lactating parent who has insurance but does not qualify for a pump due to a time restriction (e.g., one pump every 5 years) and the previous pump is either lost or broken
2. Loaner-use pump. Through this mechanism, lactating parents are loaned a hospital-grade double electric pump free of charge to use for 1 month or until their infant is discharged from the hospital. Parents are also provided with a washable pump kit and replacement parts as needed, sterilizer bags, and an unlimited supply of sterile bottles to collect milk for the entire duration of pump use. During this loaner month, an LC will work with the parent to establish and maintain the milk supply and assist with the transition to a personal-use breast pump. On receipt of this loaner pump, the parent agrees not to share the pump with anyone else, assumes responsibility for loss or theft of the pump, and returns the pump to the NICU or LG when it is no longer needed (e.g., milk supply is well established, baby has been discharged, 1 month has passed, or they have received an equivalent pump from WIC). The LC also will help secure a personal-use breast pump to use at home. If a pump is not available through insurance or another program, the parent then would qualify to receive a personal-use pump through the hospital’s Pump Program. The LG identifies eligible parents through daily rounding and consults with providers and considers the following criteria:
a. A lactating parent delivered an early preterm infant (i.e., <32 weeks gestation) who was admitted to the NICU. b. A lactating parent has an infant in the NICU and is using a personal-use breast pump but is experiencing challenges with establishing a milk supply.
On return, pumps are inspected, cleaned, and tested for proper operation. They are returned in a lockable case, which ensures protection from damage; both the case and the pump are thoroughly cleaned. Parents sign on return of the pump, and the LG updates the Pump Program records by moving the parent from the “borrowed” list to the “returned” list. Additionally, documentation is added to the parent’s chart confirming the pump return. All records are maintained in a file for future review. Pumps are stored securely within the unit and sent for repair and maintenance as needed.
The rationale for offering two different types of pumps is that hospital-grade pumps are recommended for use when a prolonged pumping period is anticipated, such as infants born very preterm (Meier et al., 2011). Hospital-grade double electric breast pumps are designed to initiate, build, and maintain an adequate milk supply when pumping is the primary method of breast stimulation and milk removal. These pumps use a closed system that provides a barrier between the milk-collection kit and the pump mechanism, preventing contact with milk and allowing the pump to be used among multiple users without risk of contamination (U.S. Food and Drug Administration, 2021). Hospital-grade multiuse pumps are more powerful, effective, and reliable than most personal-use pumps and thus are more efficient in establishing and maintaining milk supply (Yuan et al., 2025). They are also more durable than personal-use pumps and intended to be used by more than one individual. The disadvantage of these hospital-grade pumps is the high cost, which is often a substantial barrier for the patient population. Lastly, not every lactating parent requires a hospital-grade breast pump when a personal-use pump would be more than sufficient to establish and maintain a milk supply for infants born at term or without medical complications.
Clinical Insights
Since formal data collection began in 2024, the Pump Program has provided ~100 pumps per year. In 2024, the LG had a total of four full-time employees who completed 4,795 lactation visits; of these, the Pump Program serviced 91 lactating parents at the time of data collection (59 parents received a personal-use pump and 32 parents received a loaner-use pump). Table 1 provides an overview of demographics for parents who could be identified from a chart review. The Pump Program serves parents across all care settings, including in-patient, outpatient, postpartum, and most notably, the NICU, which represents the most critical population of service. Currently, 10 loaner hospital-grade pumps are available, with demand exceeding supply, necessitating temporary use of personal-use pumps until a loaner pump becomes available. Personal communications between the LCs and parents consistently reported high satisfaction, and parents frequently express sincere gratitude for the resource so that they can establish and maintain a milk supply.
Demographic Characteristics of Lactating Individuals Served by the Pump Programs.
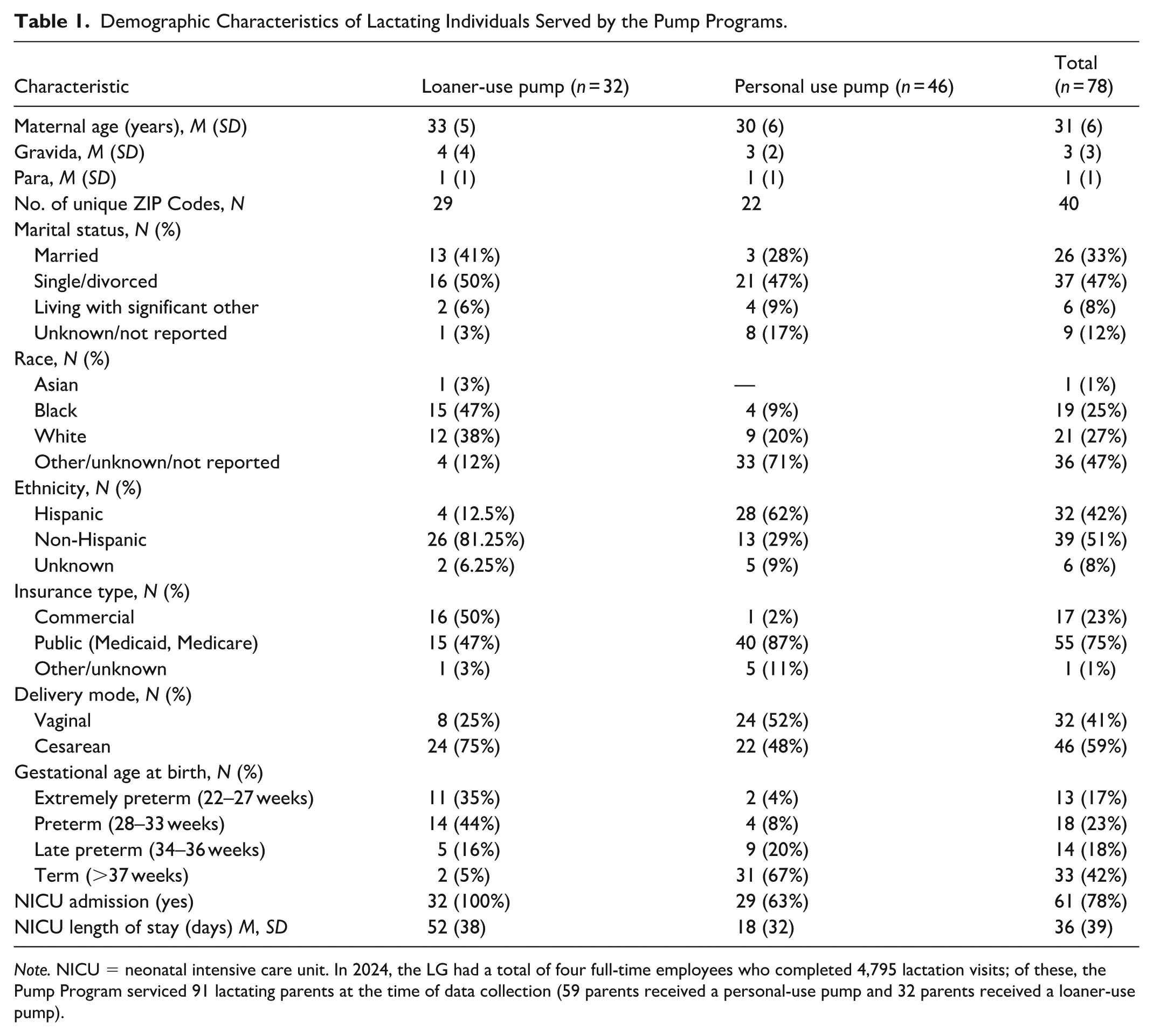
Note. NICU = neonatal intensive care unit. In 2024, the LG had a total of four full-time employees who completed 4,795 lactation visits; of these, the Pump Program serviced 91 lactating parents at the time of data collection (59 parents received a personal-use pump and 32 parents received a loaner-use pump).
Integrating the loaner-use program into the hospital’s clinical infrastructure required significant cross-departmental collaboration and strategic problem solving. Unlike the personal-use pump pathway, which primarily involved direct provision to families with minimal follow-up, the loaner-use program necessitated the creation of a robust operational workflow involving lactation services, nursing staff, obstetrics, and neonatology. Early implementation challenges included securing sustainable funding and establishing procedures to prevent and manage equipment attrition. Although the program was first funded through an external grant, that funding was no longer available when the program was restored after the pandemic. While trying to identify appropriate funding mechanisms, we discovered that internal hospital funding was available with minimal administrative hurdles, making it the most efficient source of funding. Internal hospital funds from the CATCH Pediatric Needs Fund support low-income, uninsured, or underinsured pediatric patients by covering personal devices and services not covered by insurance. The application process for these funds was straightforward, and in retrospect, much time could have been saved if we had explored internal funding options first because community funding applications were complex and limited in scope.
Another important issue we addressed with restoration of the program after COVID-19 was in response to previous issues with pump attrition. We implemented a detailed tracking and accountability system to address past issues with pump loss, logging every pump’s distribution, purpose, and return. Each pump is tagged and tracked, with families signing written agreements outlining proper use, maintenance, and return expectations (i.e., pump retrieval coordinated at time of NICU discharge or transfer). As a result of these provisions, we have successfully maintained our current inventory of 10 loaner-use pumps, the original devices purchased with the hospital’s internal CATCH funds, thus vital to sustaining the program’s success. These policy changes, supported by interdisciplinary buy-in, facilitated smoother integration into hospital workflows and strengthened long-term sustainability. Importantly, the program’s success reflects a systems-level approach to equitable lactation support—embedding the initiative within existing hospital operations rather than treating it as a siloed or ancillary service. Lastly, formal programmatic data were not systematically collected during the earliest years of the Pump Program because the initial focus was to address an urgent unmet need among families with infants in the NICU. At that time, dedicated personnel and infrastructure to support data collection and program evaluation were not available, and some early records were subsequently lost due to operational disruptions related to the COVID-19 pandemic, including staffing transitions, among a small clinical department with limited resources.
Clinical Workflow
In addition to the clinical innovation and insights, we want to highlight how the LG incorporates the Pump Program into its clinical workflow. In this section we offer case examples of how LCs interact with lactating parents in various settings across the hospital.
Postpartum
After birth, some lactating parents may experience feeding challenges with their infant, such as infant sleepiness, jaundice, weight loss, or latching difficulties, which might include anatomic conditions. In these situations, the LC plays a vital role in providing support and solutions. The LC evaluates both infant feeding behaviors and maternal factors (e.g., health conditions and medical and/or surgical history) that might impact milk production. In many cases, pumping is initiated to ensure consistent milk removal and to protect or establish the mother’s milk supply. Hospital-grade pumps are available in each room to support this process. The LC provides hands-on education for proper pump use, including assembly, cleaning, and creating an effective pumping schedule. If the infant cannot feed efficiently, expressed milk or supplementation is introduced as part of a tailored feeding plan.
Recognizing that access to a breast pump at home can be a barrier for some families, the LC has access to the Pump Program as a vital resource when insurance coverage is unavailable. By integrating the Pump Program into their care, the LC empowers families to overcome feeding challenges while ensuring that infants receive the nutrition they need. This comprehensive approach allows lactating parents to navigate early breastfeeding difficulties with confidence with the tools necessary for success. The Pump Program is a critical lifeline that provides mothers with the tools and confidence needed to meet their goals and support their infant’s health.
NICU
When an infant is admitted to the NICU, the LC becomes a key member of the care team, offering both practical and emotional support to the family. Their involvement begins with a thorough assessment of the lactating individual’s health history and birth experience, noting factors such as preterm delivery or cesarean birth that may influence milk production. In their initial meeting with the family, the LC will assess feeding goals and concerns and offer education on the importance of early, frequent milk expression. Hands-on instruction is often provided for using and cleaning a breast pump as well as for hand expression and collecting colostrum, which is especially valuable for NICU infants. To help the lactating individual establish and maintain supply, the LC helps to establish a pumping schedule of eight–10 sessions per day starting in hospital, offers tracking tools for home monitoring, and sets realistic expectations around milk volume in the early days.
Recognizing that access to equipment can be a barrier, the LC works to ensure that every family has what they need to succeed once discharged from hospital. If insurance coverage for a personal-use pump is available, the LC assists with verification and ordering; if not, they use the hospital Pump Program to secure a device for the individual. All options are explained clearly, with usage and allocations carefully documented. Beyond logistics, the LC offers ongoing emotional support, acknowledging the stress and uncertainty that often accompany a NICU stay. They remain available to answer questions, troubleshoot supply issues, and help the family prepare for transitions, such as moving from pumping to direct breastfeeding. Working closely with the NICU team, the LC ensures that feeding plans align with the baby’s medical needs. Through compassionate care and comprehensive support, they empower families to nourish their infants with human milk—no matter the challenges they face.
Intensive Care
In some cases, mothers’ birthing experience results in an admission to the intensive care unit, and the infant may or may not be admitted to the NICU. The LC plays a vital role in bridging the physical and emotional separation for the dyad. The LC will review the individual’s chart to confirm feeding intentions, followed by compassionate conversations with family members to discuss initiating pumping on the mother’s behalf. If supported, the LC collaborates with the intensive care unit nurse to educate the family on pump use, establish a regular pumping schedule, and ensure proper milk handling and storage. Medication safety is assessed in coordination with the medical team, and guidance is provided on when milk is safe to use. Throughout the hospitalization, the LC offers ongoing support, resources, and hospital-grade equipment with the goal to establish and maintain the individual’s milk supply until she can resume active participation. This collaborative, family-centered approach not only preserves the infant’s access to human milk but also offers the mother a sense of purpose, connection, and emotional healing during a profoundly difficult time.
Conclusion
In this article we present information about a breast pump program serving lactating individuals who have limited access to a high-quality electric breast pump or an infant admitted to the NICU. Financial constraints, lack of availability, language barriers, and complicated policies all have contributed to the limited use of electric breast pumps and are likely to contribute to disparities in the use or provision of human milk. This critical access program removes barriers, empowering lactating parents who wish to provide human milk for their infants to do so with confidence and support. From anecdotal comments and clinical insights, this program has provided a vital piece of equipment to parents who otherwise would not have obtained a pump within the critical time window needed to effectively establish a milk supply.
Since the inception of the program in 2015, this program has been at the forefront of supporting maternal and infant health and empowering hundreds of individuals to provide the lifesaving benefits of their own milk to their infants. This vital Pump Program established at a large, urban hospital has significantly improved access to human milk for infants and further exemplifies the health system’s commitment to eliminating systemic inequities in the provision of human milk. This innovative and essential program sets a powerful precedent in the provision of equitable care and improving access to human milk at other large urban hospitals.
Footnotes
Acknowledgements
We want to give a special thanks to the Lactation Group at Henry Ford Hospital for their unwavering commitment to birthing parents and their families in supporting the use of human milk. We also acknowledge the support and collaboration of Henry Ford Health and Michigan State University Health Sciences through the Initiative for Nursing Support of Publications and Innovations in Research and Education (INSPIRE) Program. This initiative is committed to advancing the dissemination of research and practice-improvement projects in the clinical setting through mentorship and the development of essential knowledge and skills for scholarship.
Ethical Considerations
This work reports on a hospital program, and thus, no ethical review was required.
Author Contributions
Funding
The Pump Program is sustained by funds from the Department of Pediatrics CATCH Pediatric Needs Fund, an internal fund program to assist low-income, uninsured, or underinsured children and adolescent patients who use Henry Ford Health services. The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are not publicly available. Contact authors for further information.