
Abstract
Introduction:
Our institution provides a lactation–medication consultation service for assessing drug transfer into breast milk and determining the appropriateness of breastfeeding. Information for lactating women in Japanese package inserts is often limited, especially for drugs used only in Japan. Carperitide is not approved for use outside Japan, and less is known about its transfer into breast milk or its safety when administered in infants. We report two cases in which atrial natriuretic peptide (ANP) concentrations during carperitide therapy in breast milk and maternal blood were measured.
Case presentation:
We measured ANP concentrations in breast milk and maternal plasma in two postpartum women with peripartum cardiomyopathy to evaluate the transfer of carperitide into breast milk. The breast milk concentration was 0.308 ng/ml in Case 1, and the mean concentration in Case 2 was 1.680 ± 0.055 ng/ml; the relative infant dose was 0.24% and 0.19%–0.53% for Cases 1 and 2, respectively. As the assay cannot distinguish between endogenous ANP and exogenous carperitide, the measured values represent the total ANP levels. During carperitide administration, breast milk ANP concentrations did not exceed the corresponding maternal plasma concentrations or the baseline breast milk levels when carperitide was not administered, suggesting that they remained within the range of endogenous ANP levels.
Conclusion:
The amount of carperitide transferred in these cases was low, potentially mitigating the risk of clinical effects on the infant.
Introduction
Decisions regarding drug use in lactating patients are crucial for ensuring appropriate maternal treatment while minimizing drug exposure risks to the infant. To conduct evidence-based assessments of drug transfer into breast milk and evaluate safety, we primarily reference literature (Hale & Krutsch, 2025) and databases (U.S. National Library of Medicine, n.d.) at our hospital’s Breast Milk and Medication Consultation Clinic, thereby determining the feasibility of breastfeeding.
However, drugs frequently used domestically have been used less (or not at all) overseas, resulting in a substantial lack of information on their transfer into breast milk (Anderson, 2018).
Carperitide, a recombinant human atrial natriuretic peptide (hANP), is broadly used in Japan as a crucial therapeutic agent for severe heart failure and pulmonary edema—conditions where sustaining maternal life and improving hemodynamics are critical (Daiichi Sankyo Company, Limited, 1995). Carperitide is typically administered during the acute phase when the maternal condition is unstable, and breastfeeding is often interrupted owing to the severity of illness. However, as the maternal condition improves and discharge is possible, breastfeeding may be resumed.
The manufacturer’s interview form indicates that no data are available regarding the transfer of carperitide into human breast milk (Daiichi Sankyo Company Limited, 1995). This lack of objective evidence represents a major clinical challenge when considering breastfeeding during therapy (Daiichi Sankyo Company, Limited, 1995).
According to Japanese labeling requirements, package inserts for lactating women must include “information deemed necessary based on pharmacokinetics, pharmacodynamics, and clinical experience” (Sera et al., 2024). Nonetheless, despite these regulatory requirements, there are very few drugs for which actual measurement data, such as breast milk concentrations and infant safety data after breastfeeding, based on clinical evidence are available: “When administering this drug to lactating women, weigh the therapeutic benefits against the advantages of breastfeeding. In animal studies (rats), transfer into milk has been reported” (Daiichi Sankyo Company, Limited, 1995).
As carperitide administration is not approved in Europe or the United States, and little is known about its transfer into human breast milk or its safety when given to infants, breastfeeding is often discontinued because of concerns about potential risks to the breastfed infant.
Key Messages
There is a scarcity of information regarding the transfer of carperitide into human breast milk, making it difficult to assess the safety of breastfeeding during maternal treatment.
Atrial natriuretic peptide (ANP) concentrations were measured in maternal plasma and breast milk, revealing extremely low carperitide levels in breast milk.
These findings suggest that infant exposure to carperitide through breastfeeding is minimal.
This study provides new clinical evidence to support informed decision-making about breastfeeding in mothers receiving carperitide therapy.
Given the lack of human data on ANP concentrations in breast milk during carperitide therapy, evidence-based guidance for breastfeeding during carperitide therapy remains limited. Therefore, we report two cases in which ANP concentrations were measured in maternal plasma and breast milk during carperitide therapy to help address this clinical knowledge gap.
History and Observational Assessments
Case 1
Patient demographics, history, and main symptoms:
An Asian female in her 30s (height 168 cm, weight 75 kg); primigravida (G1P0).
No remarkable past medical history
Clinical Findings
The patient was admitted to emergency care owing to pregnancy-induced hypertension. On hospital Day 1, she developed eclampsia and underwent an emergency cesarean section at 33 weeks and 1 day of gestation, delivering an infant weighing 1,772 g. Postoperatively, she was intubated and managed in the intensive care unit. On hospital Day 2, she developed pulmonary edema (cardiothoracic ratio, 61%; elevated B-type natriuretic peptide [BNP] level), and intravenous furosemide was initiated. On hospital Day 4, pulmonary embolism with pulmonary edema was diagnosed, and continuous intravenous infusion of carperitide (0.025 µg/kg/min) was initiated; it was discontinued on hospital Day 5. ANP concentrations in breast milk were obtained on hospital Days 4 and 13, and plasma ANP concentration measurements were obtained on hospital Day 13 (Figure 1).
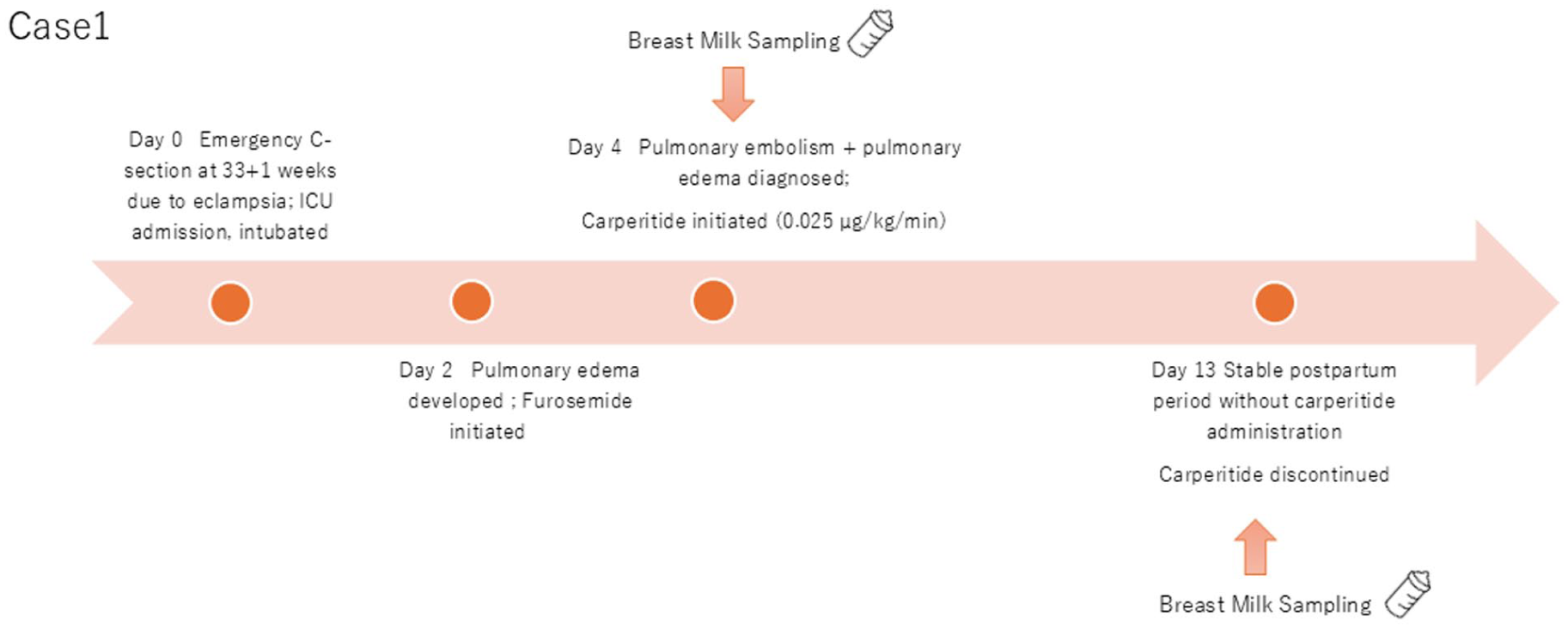
Clinical course of Case 1.
Case 2
Patient demographics, history, and main symptoms:
An Asian female in her 30s (height 162 cm, weight 60 kg); multipara (G2P2).
Past history: gestational hypertension
Clinical Findings
The patient had delivered an infant weighing 3,290 g at 38 weeks and 3 days via vaginal delivery at another hospital. Six days postpartum, she developed dyspnea and palpitations, followed by chest pain. She was diagnosed with acute heart failure and admitted to our hospital. Treatment included intravenous furosemide 20 mg twice daily, a continuous intravenous infusion of carperitide (0.05 µg/kg/min), and landiolol (5 µg/kg/min). On admission, the BNP level was 1,323.9 pg/ml. ANP concentrations in breast milk measurements were obtained on hospital Days 2, 3, 4, 5, and 8, and post-discharge; plasma ANP concentration measurements were obtained post-discharge (Figure 2).
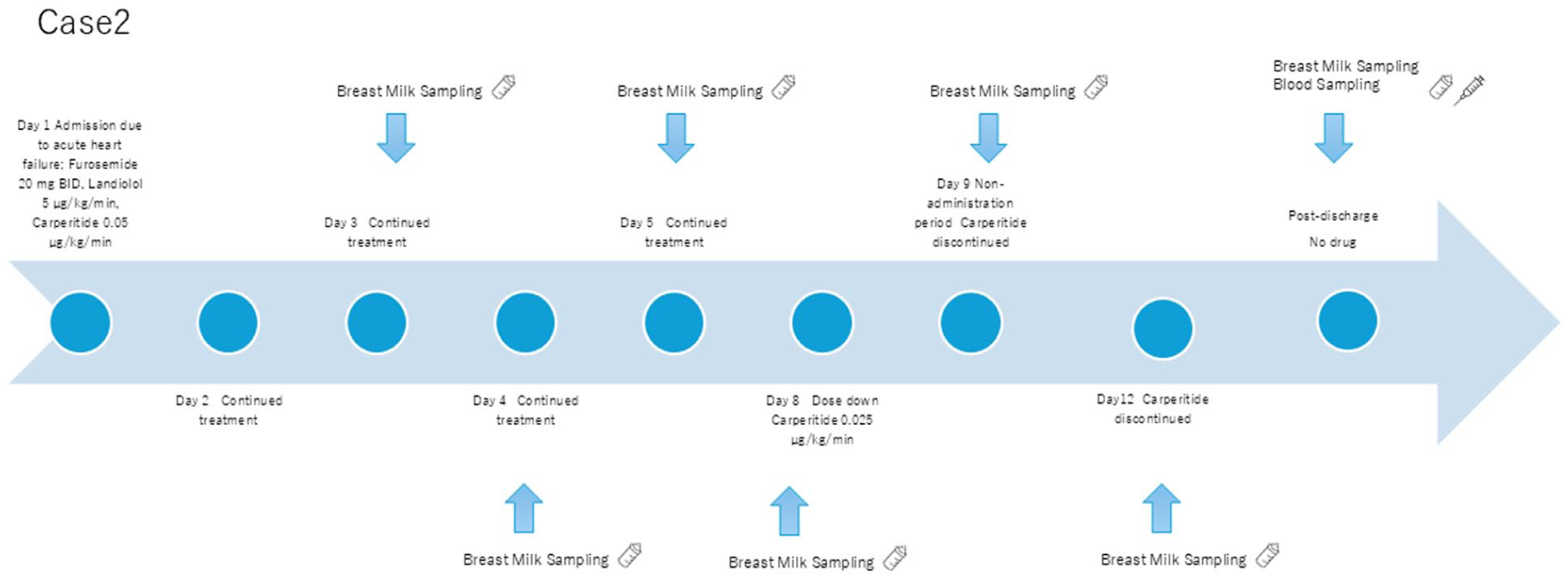
Clinical course of Case 2.
Sample Collection and Analysis
ANP concentrations were measured using the Arbor Assays DetectX® ANP EIA Kit (Cat. No. K071‑H1/K071‑H5; Arbor Assays, Ann Arbor, MI, USA), employing a competitive ELISA method.
A 100-µl sample of breast milk was centrifuged at 1,000 g for 15 min at 2°C–8°C. The aqueous layer was collected, and this process was repeated three times.
Samples were plated with primary antibody, incubated with enzyme-labeled ANP for competition, and developed with the 3,3’,5,5’-tetramethylbenzidine substrate. Absorbance was measured at 450 nm. Absorbance measurements were performed using a Thermo Scientific microplate reader (Varioskan Flash 2.4; Thermo Fisher Scientific, Waltham, MA, USA).
A calibration curve was prepared using pretreated human milk without carperitide, with standards ranging within 0.7–180 ng/ml (correlation coefficient 0.99; relative standard deviation of < 20% at all concentrations). Total breast milk ANP concentrations were calculated using this curve. The detection and quantitation limits of the assay were determined by comparing the optical density (OD) of 20 wells of the zero standard. The detection limit was 0.26 ng/ml, defined as two standard deviations from B0 along the standard curve. Similarly, the lower limit of quantitation (LOQ) was defined as 10 standard deviations from the breast milk blank, yielding an LOQ of 0.48 ng/ml.
This study was approved by the Ethics Committee of Showa University School of Medicine (approval number: 2572). Additionally, written informed consent was obtained from the patients for breast milk sample collection and publication of this case report in a scientific journal.
Sample Collection and Analysis
Both cases were evaluated to determine the extent of carperitide transfer into breast milk. The timing of breast milk and plasma sample collection was selected based on stabilization of maternal hemodynamics (see Figures 1 and 2 for clinical timelines). Clinical constraints prevented the simultaneous measurement of plasma and breast milk concentrations during hospitalization.
Case 1
Following an emergency Cesarean section, the patient required intubation and intensive care management, resulting in delayed initiation of breastfeeding. After starting carperitide therapy and achieving hemodynamic stability, breastfeeding counseling was provided. Breast milk samples were collected on hospital Days 4 and 13. The measured ANP concentration in Case 1 was below the lower LOQ (0.7 ng/ml) but above the limit of detection.
Case 2
The patient had initially been discharged postpartum and was breastfeeding at home. She was later readmitted with worsening symptoms, and doses of carperitide, furosemide, and landiolol were adjusted according to her cardiac status. Breast milk expression continued throughout hospitalization, with samples collected on hospital Days 2, 3, 4, 5, and 8. After discharge, additional breast milk and plasma samples were obtained.
In both cases, breastfeeding was resumed after the mothers’ conditions stabilized. No adverse effects were observed in either infant following the reinitiation of breastfeeding.
Outcomes
The results for Case 1 are presented in Table 1. In Case 1, the breast milk ANP concentration on Day 4 of hospitalization was 0.308 ng/ml. On Day 13 (the non-administration period), the breast milk and blood concentrations were 0.758 ng/ml and 1.423 ng/ml, respectively.
Breast Milk and Maternal Plasma Levels of ANP in Case 1.
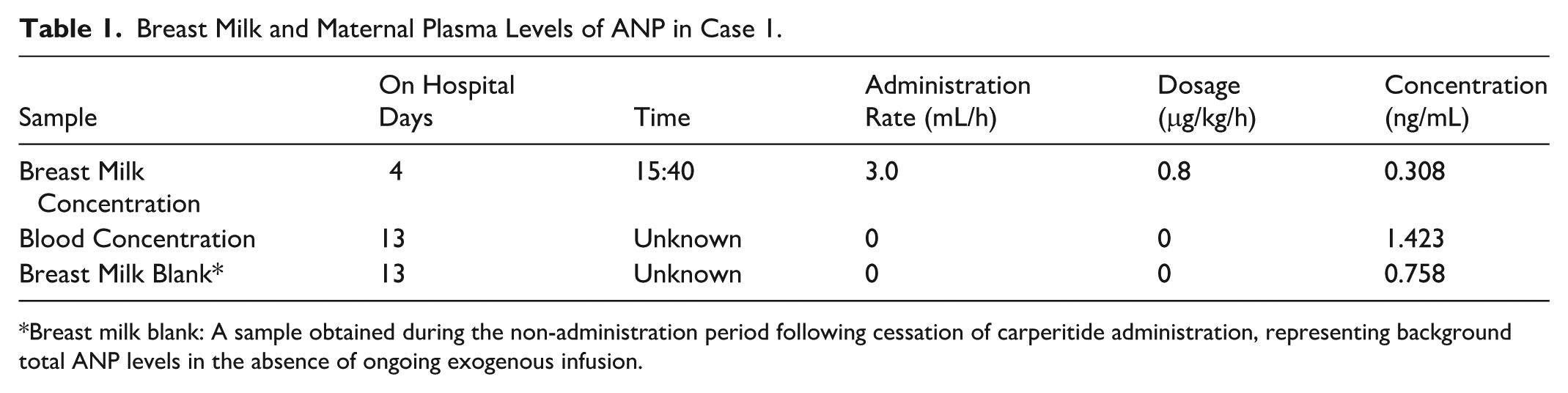
Breast milk blank: A sample obtained during the non-administration period following cessation of carperitide administration, representing background total ANP levels in the absence of ongoing exogenous infusion.
The results for Case 2 are presented in Table 2. In Case 2, the breast milk concentration on Day 8 was 1.267 ng/ml, with a mean concentration of 1.680 ± 0.055 ng/ml during the administration period. During the non-administration period (Days 9, 12, and post-discharge), the mean ANP concentration was 1.560 ± 0.039 ng/ml, and the post-discharge blood concentration was 2.760 ng/ml.
Breast Milk Concentration and Maternal Plasma Levels of ANP in Case 2.
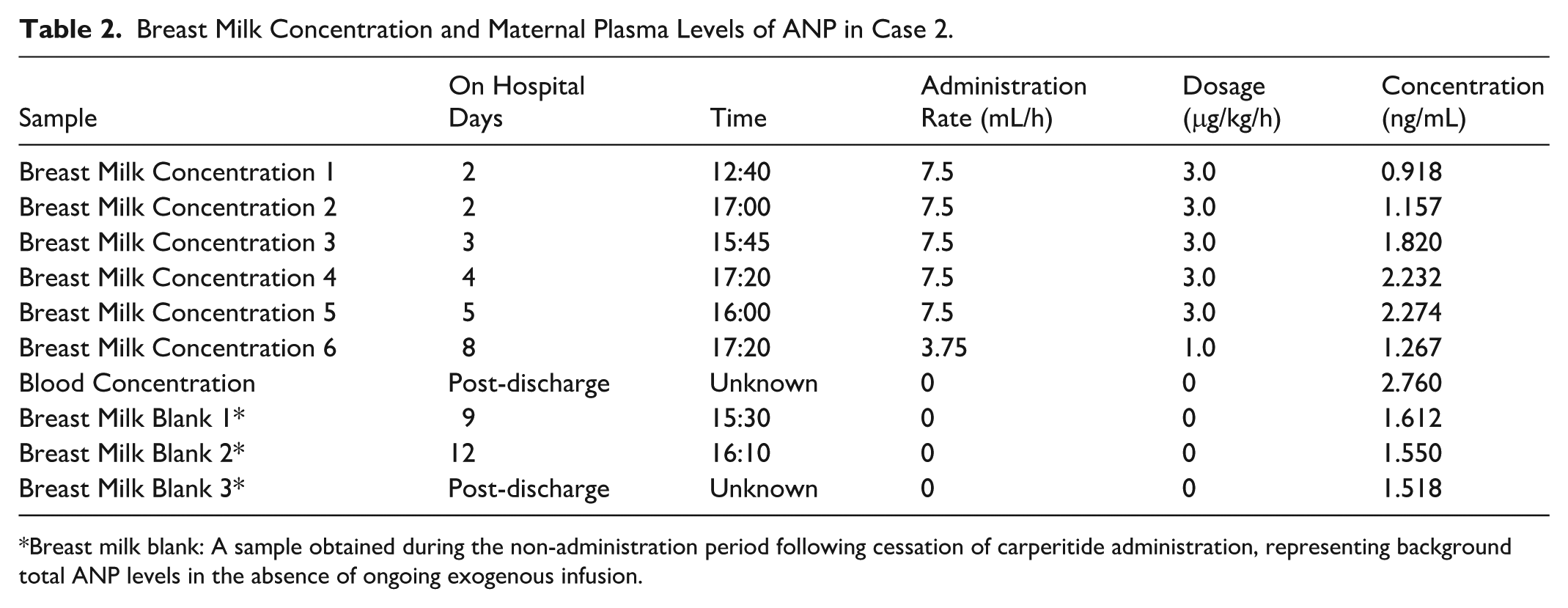
Breast milk blank: A sample obtained during the non-administration period following cessation of carperitide administration, representing background total ANP levels in the absence of ongoing exogenous infusion.
Assuming a breast milk intake of 150 ml/kg/day, the relative infant dose (RID) was estimated at 0.24% and 0.19%–0.53% for Cases 1 and 2, respectively.
Patient Perspective
The patients expressed a desire to breastfeed once their condition stabilized and agreed to our counseling and suggestions.
Discussion
This study measured carperitide concentrations in breast milk and plasma from two lactating women in the puerperium receiving carperitide therapy. To the best of our knowledge, this is the first report to investigate the transfer of natriuretic peptides (ANP and BNP) into human breast milk (National Library of Medicine (US), n.d.).
The competitive ELISA kit used detects both endogenous ANP and exogenous carperitide (hANP). Therefore, the concentrations reported here represent total ANP levels. Normal plasma ANP levels in healthy adults measured by this kit average 1.4 ng/ml (range: 0.8–3.0). In both cases, the measured ANP concentrations during carperitide administration were lower than or comparable to blood concentrations and did not exceed those observed during the non-administration period. These findings suggest that the transfer of carperitide into breast milk is minimal.
The calculated RID (0.19%–0.53%) was far below the generally accepted safety threshold of 10%. A RID of approximately 5%–10% is often used as an indicative threshold when assessing drug safety during lactation (Spigset, 2025). Of note, these RID values were calculated based on total ANP concentrations; if the measured values consisted entirely of exogenous carperitide (a worst-case scenario), infant exposure would remain clinically negligible. Considering the high molecular weight (3,080.44 Da) and hydrophilic nature of carperitide, low transfer into breast milk is pharmacologically expected (Daiichi Sankyo Company, Limited, 1995). The present results support this assumption.
However, because the assay cannot differentiate between endogenous ANP and exogenous ANP, the measured concentrations likely represent the total ANP levels (Nagai-Okatani et al., 2016). The consistent detection of ANP during non-administration periods reflects endogenous secretion (Ationu, 1998; Melo et al., 2000). As the assay does not differentiate endogenous ANP from exogenous carperitide and baseline ANP levels were not measured, the reported concentrations represent total ANP. Notably, measurable ANP concentrations were also observed after discontinuation of carperitide. Given that breast milk concentrations during infusion were not higher than those measured after cessation, the contribution of exogenous carperitide appears to have been limited. However, the precise proportion attributable to exogenous administration cannot be determined. Since both ANP and BNP are markers of heart failure, the condition itself may lead to increased endogenous ANP levels. The fact that breast milk concentrations did not increase during carperitide therapy further supports the interpretation that carperitide transfer is negligible.
Limitations
This study’s limitations include the inability to measure maternal plasma concentrations during infusion or the infant’s actual milk intake, which prevented calculation of the milk-to-plasma (M/P) ratio. Although the RID was estimated based on an assumed milk intake of 150 ml/kg/day, the absolute transferred dose remains extremely low.
Furthermore, the lack of baseline ANP measurements prior to the initiation of carperitide limits our ability to quantify the exact amount of drug transfer. However, the low RID values calculated from total ANP levels offer a conservative and reassuring estimate of infant safety.
Future studies should incorporate simultaneous measurement of maternal plasma levels during administration, actual milk intake, and differentiation between endogenous and exogenous peptides. Such data will allow more accurate calculation of M/P ratios and RIDs, enabling a more precise quantitative risk assessment for infants.
Comprehensive breastfeeding information, including milk volume and feeding frequency, was not available in these cases, restricting precise estimation of infant exposure. However, no adverse events were observed in either infant during follow-up.
Conclusion
Despite the above-mentioned limitations, this study suggests that ANP concentrations in breast milk during carperitide therapy are minimal from the perspective of milk transfer, providing a scientific basis for considering the safe resumption of breastfeeding once the maternal condition stabilizes. Given the absence of data in resources such as LactMed®, these findings offer valuable evidence to support clinical decision-making in lactating patients receiving carperitide.
Footnotes
Acknowledgements
The authors thank all participants for their cooperation in this study and acknowledge the support of the clinical and laboratory staff involved in data and sample collection.
Ethical Considerations
This study was approved by the institutional review board (
Consent to Participate
Written informed consent was obtained from all participants before participation in the study.
Author Contributions
Yasuha Ogawa: Conceptualization; Data curation; Formal analysis; Project administration; Supervision; Writing – original draft. Taro Kamiya: Conceptualization; Data curation; Investigation; Methodology; Supervision. Nao Tagawa: Data curation; Investigation. Satoru Aoki: Conceptualization; Investigation; Methodology. Mami Kobayashi: Methodology. Yoko Sato: Data curation. Sachiko Tanaka: Data curation; Investigation. Hitomi Wakabayashi: Conceptualization; Investigation; Validation. Katsumi Mizuno: Conceptualization; Investigation; Supervision; Validation.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data that support the findings of this study are available from the corresponding author upon reasonable request.*