
Abstract
Background:
Community pharmacists have the potential to provide adherence-support interventions, address adverse effects, and optimize health outcomes in vulnerable patient populations such as breastfeeding women who need rational antimicrobial therapy.
Research Aim:
The primary aim of this study was to investigate the influence of community pharmacists’ adherence support interventions on outcomes of antimicrobial therapy use and breastfeeding continuation in breastfeeding women.
Methods:
A prospective interventional before–after study was conducted in community pharmacies in Serbia (May–October 2022) within the Mama Friendly Pharmacy project. Breastfeeding women (N = 182) receiving antimicrobial therapy completed validated questionnaires and received pharmacist-led counseling, including risk assessment using specialized databases. A follow-up assessment included evaluated adherence, breastfeeding continuation, infant safety, and factors associated with intervention outcomes. Data were analyzed using SPSS (Version 24).
Results:
The results indicate that 84.71% of participants who believed that medications should be avoided during breastfeeding—regardless of clinical indication—expressed concerns about using the prescribed antimicrobial agent. Likewise, 58.76% of participants who generally held a positive attitude toward medication use during breastfeeding also reported uncertainty regarding antimicrobial therapy. Overall, 95.2% of participants accepted the recommended therapy and monitoring advice. Follow-up was completed by 80.8%, with positive outcomes and only 14 minor infant adverse effects reported, none requiring medical intervention. Logistic regression identified maternal age as the only significant predictor of follow-up participation.
Conclusion:
By improving both therapy acceptance and duration and supporting informed decision-making regarding breastfeeding, community pharmacists play a critical role in resolving uncertainties, preventing interruption of breastfeeding, and helping address antimicrobial resistance.
This is a visual representation of the abstract.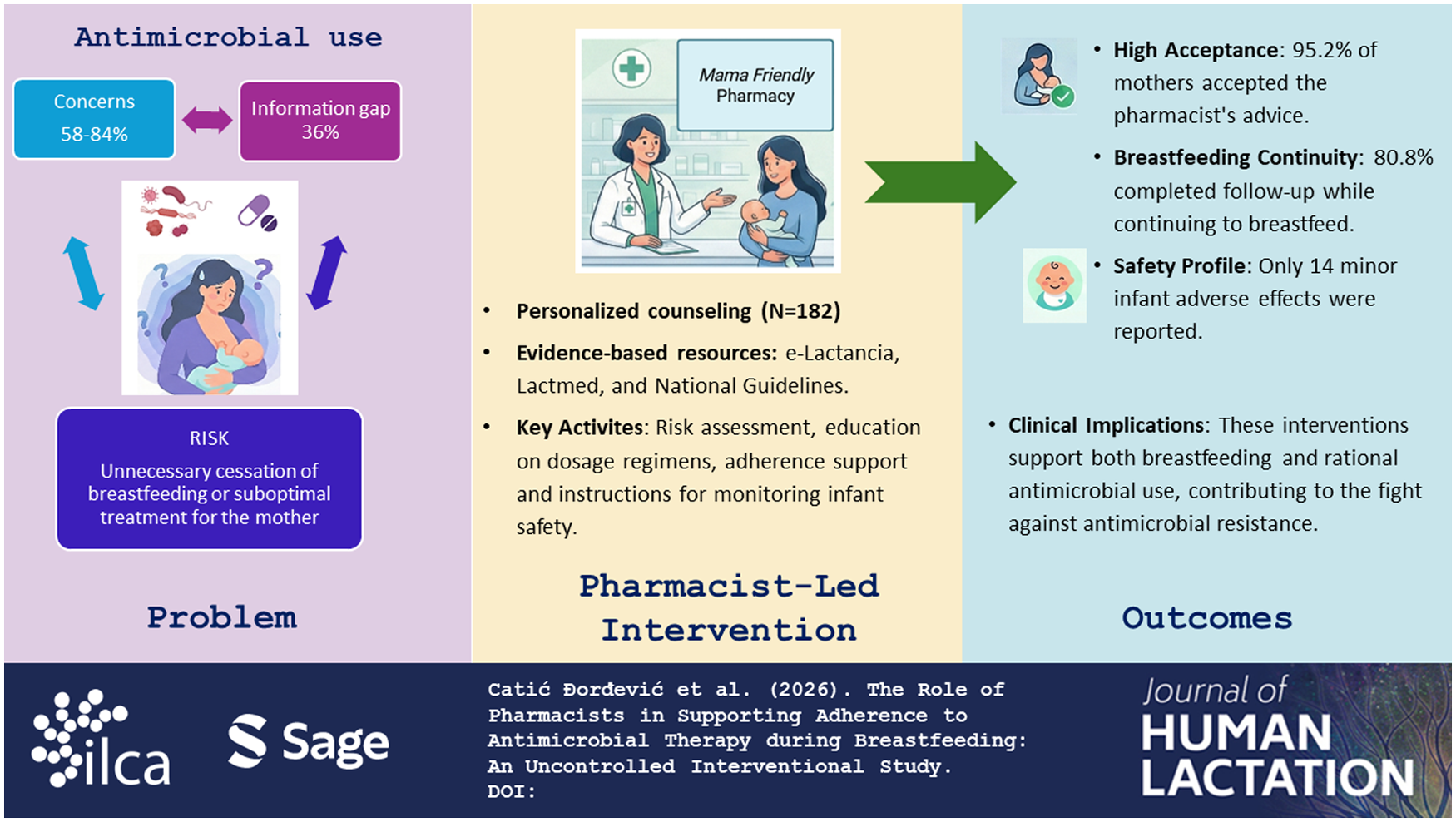
Background
The rational use of antimicrobial (AM) therapy is critical in combating antimicrobial drug resistance. It relies on establishing and maintaining the appropriate treatment duration. Incomplete adherence or administration of shorter, sub-therapeutic courses can lead to treatment failure and a significant increase in resistance patterns. Therefore, strict antimicrobial stewardship measures, along with pharmacist-led strategies to enhance adherence, are essential for maintaining optimal treatment outcomes and preserving the long-term effectiveness of anti-infective medications. Community pharmacists play a key role in ensuring adherence support interventions, addressing adverse effects, and optimizing health outcomes (Al-Shami et al., 2023).
In vulnerable patient populations, such as breastfeeding women, the rational AM therapy is an even more important goal (de Sá Del Fiol et al., 2016). While AM therapy is not routinely required in breastfeeding women, it becomes essential in specific clinical situations, such as acute infections requiring prompt treatment. As the most accessible healthcare professionals in primary care, community pharmacists are consistently available to breastfeeding women, offering support related to lactation and the management of various health concerns (Ronai et al., 2009). Given the well-documented, invaluable benefits of breast milk for the growth and development of infants, pharmacists aim to provide essential support to nursing mothers. This support includes counseling on breastfeeding, addressing minor health issues, and ensuring infant safety during necessary pharmacotherapy.
However, in many cases, breastfeeding duration does not align with World Health Organization (WHO) recommendations. Among the diverse reasons for early cessation, one common cause is the need for acute medication use, which often raises concerns among mothers about potential risks to their infants (McClatchey et al., 2018). Previous investigation showed that despite reassuring advice, one in five women either did not initiate therapy or did not continue breastfeeding (Ito et al., 1993).
Key Messages
Adherence to antimicrobial therapy in breastfeeding mothers is often suboptimal due to concerns about potential adverse effects on the infant, which may compromise treatment effectiveness and contribute to antimicrobial resistance.
Our findings further confirm the importance of counseling on medication use and safe breastfeeding practices for maintaining high adherence during antimicrobial therapy.
The 95.15% acceptance rate of adherence-support interventions in our study, together with 80.77% availability for follow-up, confirms the effectiveness of adherence-support strategies implemented in community pharmacy settings.
In addition, the study highlights the need for a patient-centered approach that is adjusted primarily according to age rather than educational level.
Rational AM therapy depends not only on appropriate prescribing practices but also on adherence to recommended dosing regimens. Adherence itself is a key determinant of treatment success (Adams & Stolpe, 2016). When a patient collects a prescribed antibiotic, the pharmacist can contribute to rational therapy implementation—first, by promoting primary adherence support (timely initiation of treatment), and, later, by supporting total adherence (completion of the entire prescribed course), while managing potential side effects as needed. Following Kelly et al. (2023), pooled results showed a statistically significant increase in the odds of medication adherence with the pharmacist counseling.
The modern role of pharmacists in therapy management is increasingly characterized by a structured and tailored approach, providing individualized care that aligns with each patient’s specific needs, ultimately leading to more effective outcomes (Sim et al., 2017). The positive impact of the structured pharmaceutical service on the continuation of breastfeeding in situations where it is necessary to administer medication to breastfeeding woman has been recognized (Kovačević et al., 2025). According to competences, the role of the pharmacist is not to promote AM use, but to support its safe and evidence-based use when clinically indicated. Incomplete adherence or administration of shorter, sub-therapeutic courses can lead to treatment failure and a significant increase in resistance patterns. Stringent antibiotic stewardship and pharmacist-led interventions to support total adherence are essential to preserve the long-term therapeutic efficacy of AM agents.
Barriers to the implementation of rational AM therapy often stem from the prescriber’s concerns of potential harm to the infant during breastfeeding, and the mother’s fear for her child’s safety during treatment (Ito et al., 1993). These challenges are not related to the indication for AM therapy itself, but rather to uncertainty regarding its safe use during lactation. Every therapy requires a careful assessment of benefit and safety for the patient. Poor quality of information about drug safety during lactation can contribute to confusion in giving recommendations. This confusion can result in early cessation of breastfeeding or insufficient health care for the breastfeeding woman (McClatchey et al., 2018). Therefore, the adherence support intervention must also include a safety evaluation for the infant, while ensuring the mother receives necessary treatment.
The primary aim of this study was to investigate the influence of community pharmacists’ interventions on adherence support and the safety outcomes of AM therapy in breastfeeding women. More accurately, we evaluated the acceptance of adherence support interventions and factors associated with continued follow-up, and estimated concerns toward AM use during breastfeeding.
Methods
A prospective interventional, uncontrolled before-and-after study was conducted between May and October 2022 in community pharmacies across the Republic of Serbia. This study was part of the Mama Friendly Pharmacy project (in Serbian: Mama Friendly Apoteka – za bezbednu primenu lekova u toku dojenja – Vaš farmaceut). During the provision of routine pharmaceutical care, pharmacists offered breastfeeding women additional support and pharmaceutical care services tailored to their specific needs.
All participating breastfeeding women voluntarily visited pharmacies marked with the Mama Friendly Pharmacy sign (labelled to provide structured pharmaceutical services for breastfeeding women) and provided written informed consent prior to enrollment and receipt of the standardized pharmaceutical service. Ethical approval for the study was obtained from the Ethics Committee of the Pharmaceutical Chamber of Serbia (Approval No. 316/5.3, issued on November 29, 2022).
In total, 1,243 structured pharmaceutical care services were provided throughout the duration of the project, and in 182 of all breastfeeding mothers, a prescribed AM therapy was noted. The inclusion criteria for this study required the prescription of antimicrobial medication.
Data were collected using a structured questionnaire developed by the research team specifically for the purposes of collecting breastfeeding women’s data. Prior to the start of the research, the questionnaire was pilot-tested and validated through voluntary participation of eight breastfeeding women to ensure clarity, relevance, and comprehensibility of the questions.
The questionnaire consisted of three sections. The first section collected demographic data related to the mother and infant (age, postpartum period, and infant age). The second section included information on the mother’s health status, the infant’s health condition, and pharmacotherapy used during pregnancy and after delivery. The third section explored mothers’ attitudes toward medication use during breastfeeding, including their willingness to use prescribed medications during lactation and concerns regarding potential risks to the infant.
Additional questions addressed whether the prescribing physician had provided counseling regarding the safety of the prescribed medication during breastfeeding and its potential impact on lactation or infant health. After data collection and therapy assessment, pharmacists provided personalized counseling to ensure rational antimicrobial use while supporting continued breastfeeding and infant safety through recommended monitoring. Pharmacist interventions and follow-up evaluations were documented using a dedicated questionnaire. This questionnaire collected information on the course and completion of antimicrobial therapy, breastfeeding continuation, pharmacist interventions, adherence to therapy, and any reported adverse effects in infants. Mothers were informed in advance about possible signs and symptoms to monitor in their infants. For each prescribed medication, pharmacists performed an individual risk assessment based on available scientific evidence and specialized databases for medication safety during breastfeeding. Specifically, resources such as the e-Lactancia database, National Guidelines for Safe Pharmacotherapy During Breastfeeding, Lactmed, Drugs.com, and Summary of Product Characteristics (SPC) were consulted to assess drug compatibility with breastfeeding, and to identify risks or safer alternatives. The counseling focused on ensuring the rational use of antimicrobial therapy, maintaining breastfeeding whenever possible, and safeguarding infant health through appropriate monitoring recommendations.
A follow-up visit was scheduled depending on the characteristics and duration of the prescribed therapy, in order to evaluate the outcome of the pharmacist-led intervention. In some cases, follow-up was conducted through telephone contact when an in-person visit was not feasible.
Each response was scored according to predefined criteria. The pharmacist-led intervention was considered successful if it resulted in appropriate use of the prescribed antimicrobial therapy, continuation of breastfeeding, and appropriate monitoring of the infant with recording of eventual adverse reactions in the infant.
Sample Size
The sample size was estimated to be approximately 320 breastfeeding mothers (80% power of study, Type I error 0.05, number of newborns in Serbia annually approximately 60,000, the proportion of breastfeeding about 50%, expected proportion of antimicrobial use in the population of breastfeeding mothers 30%, dropout rate 20%). In our study, out of a total of 1,243 breastfeeding women participating in the project, 746 mothers (60.0%) had been prescribed a medication during breastfeeding, whereas the proportion of anti-infectives was lower than expected (182 mothers, 15.1%) .
Statistical Analysis
Continuous data were presented as mean and standard deviation and/or median and interquartile range. Categorical variables were presented as absolute numbers and percentages. Continuous variables were analyzed using Student’s t-test and the Mann–Whitney U test, while categorical variables were analyzed using the chi-square test. Student’s t-test was used to compare normally distributed parameters, whereas the Mann–Whitney U test was applied when the assumption of normality was not met. Additionally, logistic regression was conducted to evaluate the factors affecting breastfeeding mothers’ willingness to undergo evaluation of the proposed intervention. Statistical analyses were performed using SPSS (Version 24), with a significance level set at p < 0.05.
Results
Of 1,243 breastfeeding women participating in the project, a total of 746 mothers (60.0%) had been prescribed a medication while breastfeeding. In the total sample, the most commonly used medications were anti-infectives (15.1%) and medications for the respiratory system (10.9%). Considering the total number of services provided during the project, 182 breastfeeding women had an indication and prescription for AM therapy. The main goal of the standardized pharmaceutical service was to ensure rational AM treatment while maintaining the safety of the infant. To achieve this, four key activities were undertaken:
Assessment of the justification for the prescribed therapy, drug selection, and dosage regimen;
Collection of demographic data and breastfeeding-related information;
Education and counseling aimed at achieving high primary adherence—start of AM therapy and total adherence—as well as timely and adequate dosing regimen and therapy duration;
Evaluation of the effectiveness of antimicrobial therapy and the pharmacist-led intervention provided.
Demographic and Clinical Characteristics
A total of 182 breastfeeding mothers with AM prescription entered the analysis. The mean age of the mothers was 30.8 years, while the median infant age was 5 months. Most participants had higher or university education and lived in urban areas. Detailed characteristics are presented in Table 1.
Demographic Characteristics of the Participants With Prescribed Antimicrobial Therapy (N = 182).
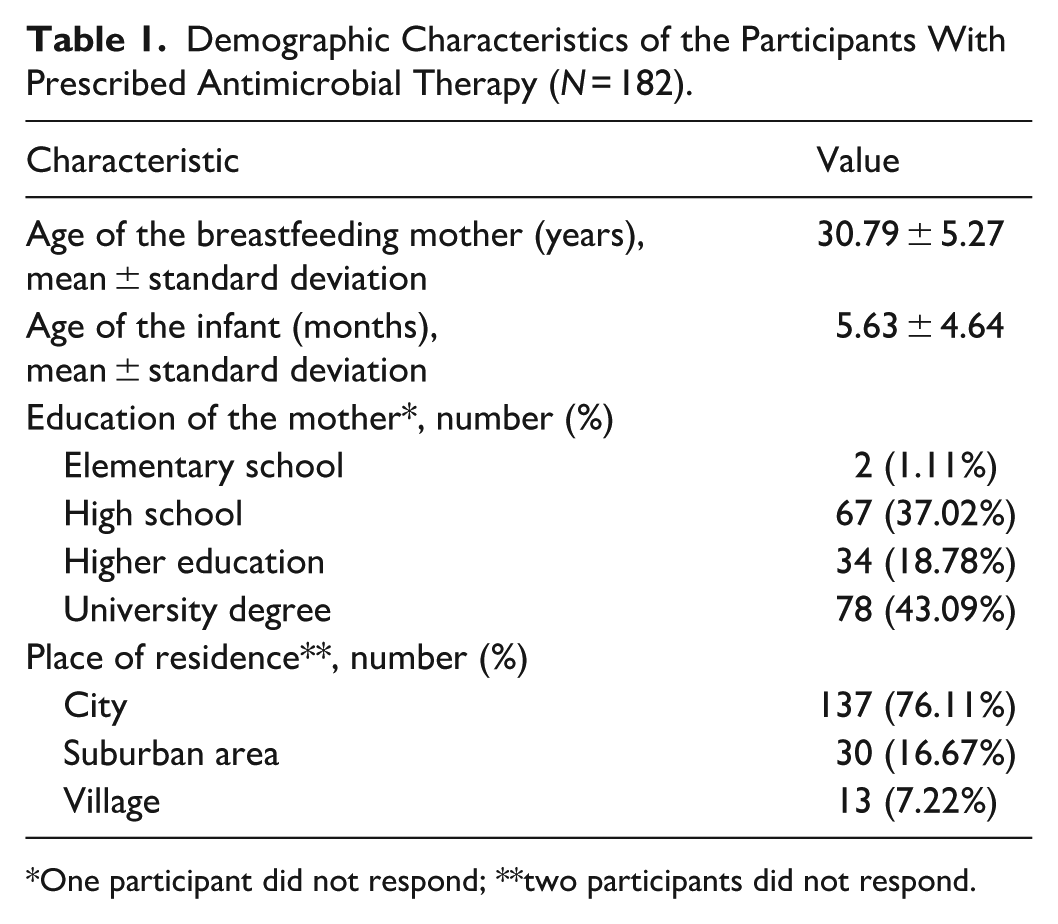
One participant did not respond; **two participants did not respond.
As the first step, prescriptions were checked for indications and contraindications of the prescribed drugs, potential allergies, dosage regimens, and treatment duration. All participants had a valid physician’s report and/or an electronic medical prescription for the prescribed drug. Seven breastfeeding women required the concomitant administration of two AM agents. Table 2 shows the highest prevalence of penicillin antibiotics, accounting for 37% of all prescribed drugs, followed by cephalosporin antibiotics with 32%. All prescribed AM drugs and dosage regimens were found to be compatible with breastfeeding, using the e-Lactancia database, National Guidelines for Safe Pharmacotherapy During Breastfeeding, Lactmed, Drugs.com, or SPC.
Prescribed Antimicrobial Medications Among Breastfeeding Mothers.
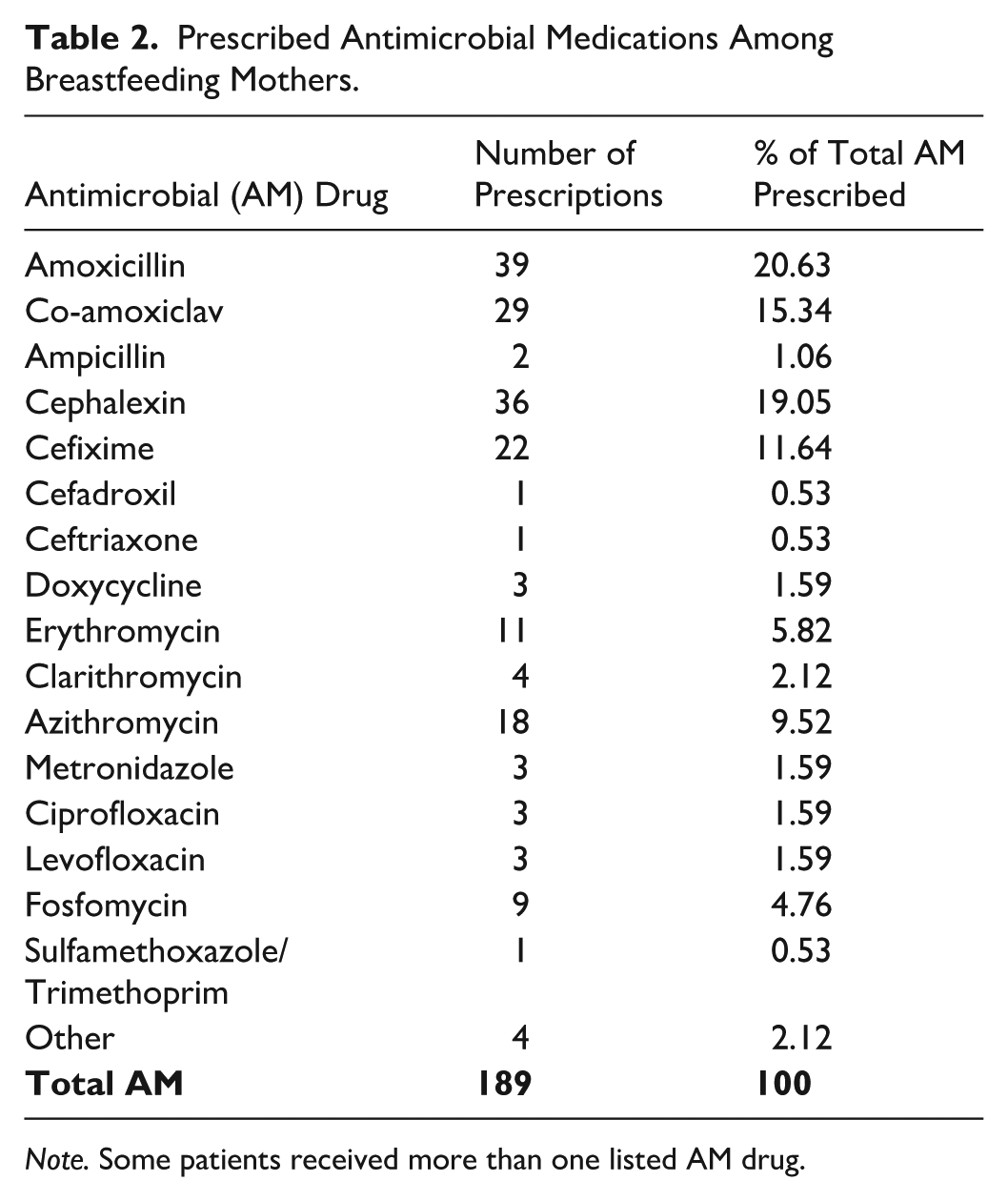
Note. Some patients received more than one listed AM drug.
As shown in Table 3, respiratory and urinary tract infections were the most common indications for AM therapy (25.82% each), followed by mastitis and dental infections.
Medical Indications for Antimicrobial Prescriptions.
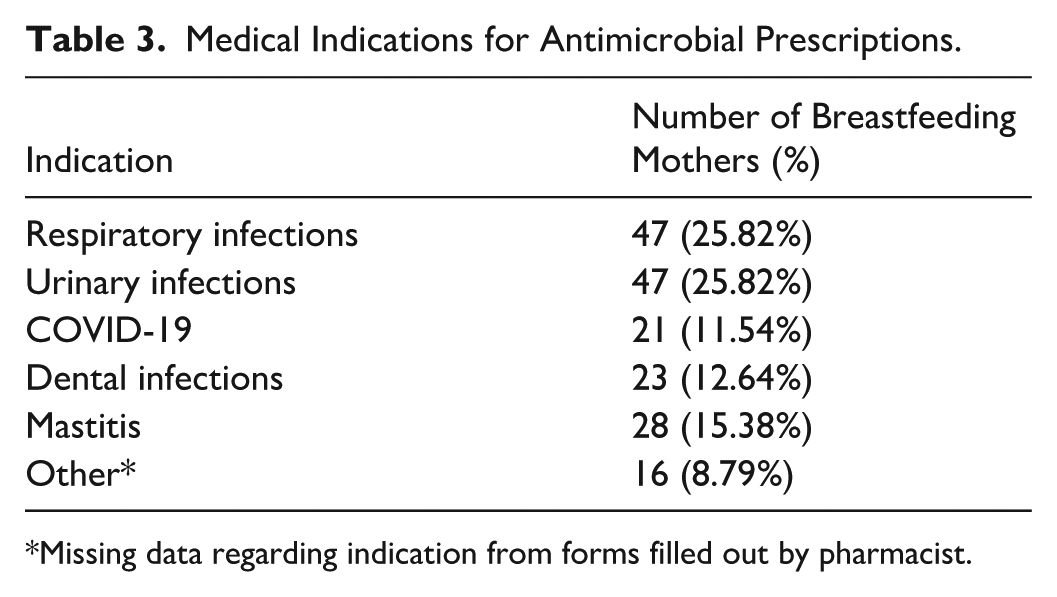
Missing data regarding indication from forms filled out by pharmacist.
Attitudes and Concerns About Antimicrobial Medication Use
The results indicate that 84.71% of participants who believed that medications should be avoided during breastfeeding—regardless of clinical indication—expressed concerns about using the prescribed AM. Likewise, 58.76% of participants who generally held a positive attitude toward medication use during breastfeeding also reported uncertainty regarding AM therapy. These findings are illustrated in Figure 1, which presents the attitudes of breastfeeding women regarding concerns about breastfeeding during therapy.
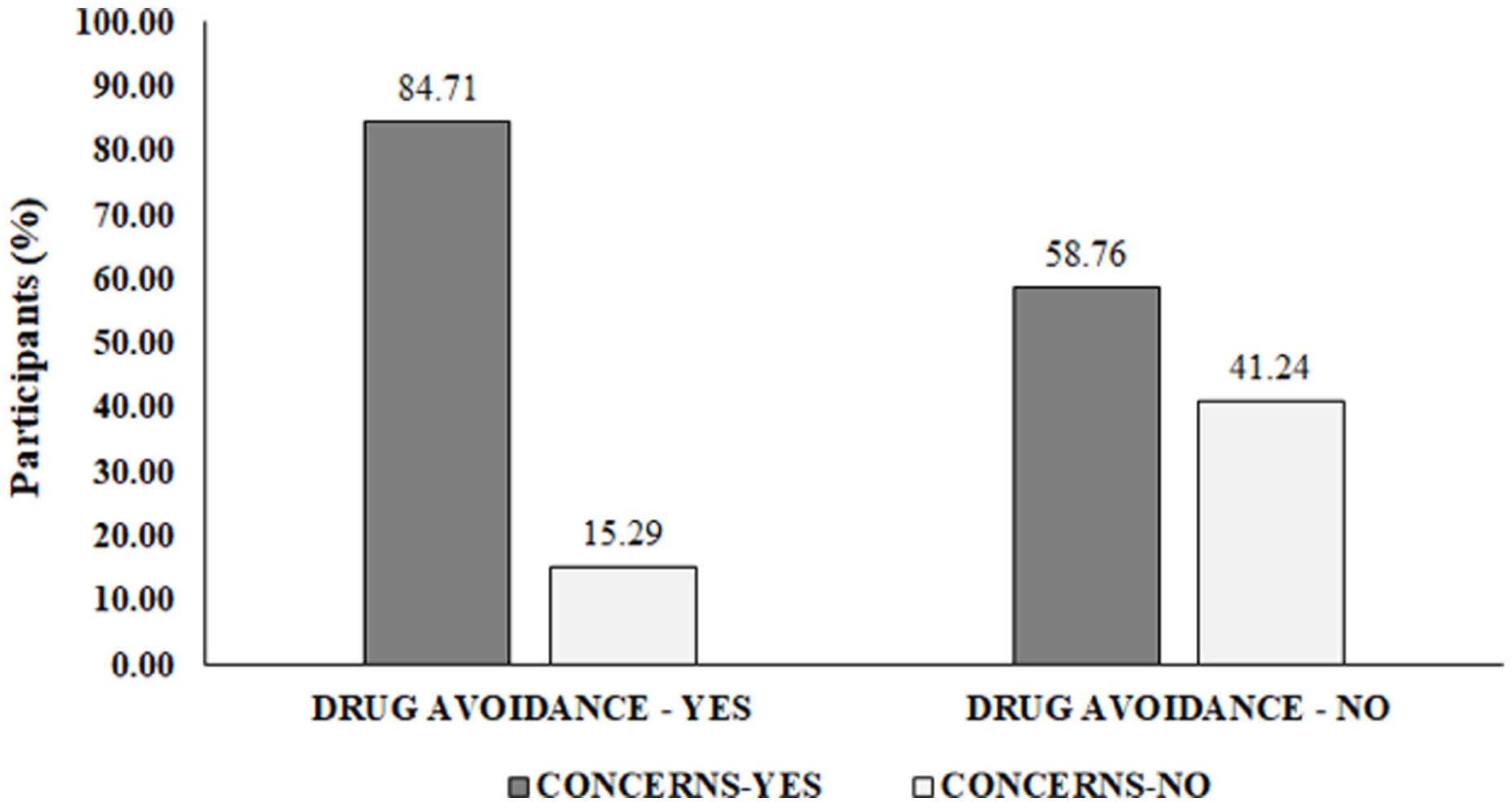
The attitudes of breastfeeding women regarding concerns about pharmacotherapy during breastfeeding.
To explore the background of negative attitudes toward AM or medication use in general, breastfeeding mothers were asked to report previously given information, that is, physician’s advice regarding continuation of breastfeeding during AM therapy. As shown in Figure 2, 4.95% of breastfeeding mothers were advised to discontinue breastfeeding during AM therapy, which is not consistent with current literature recommendations for prescribed medicines.
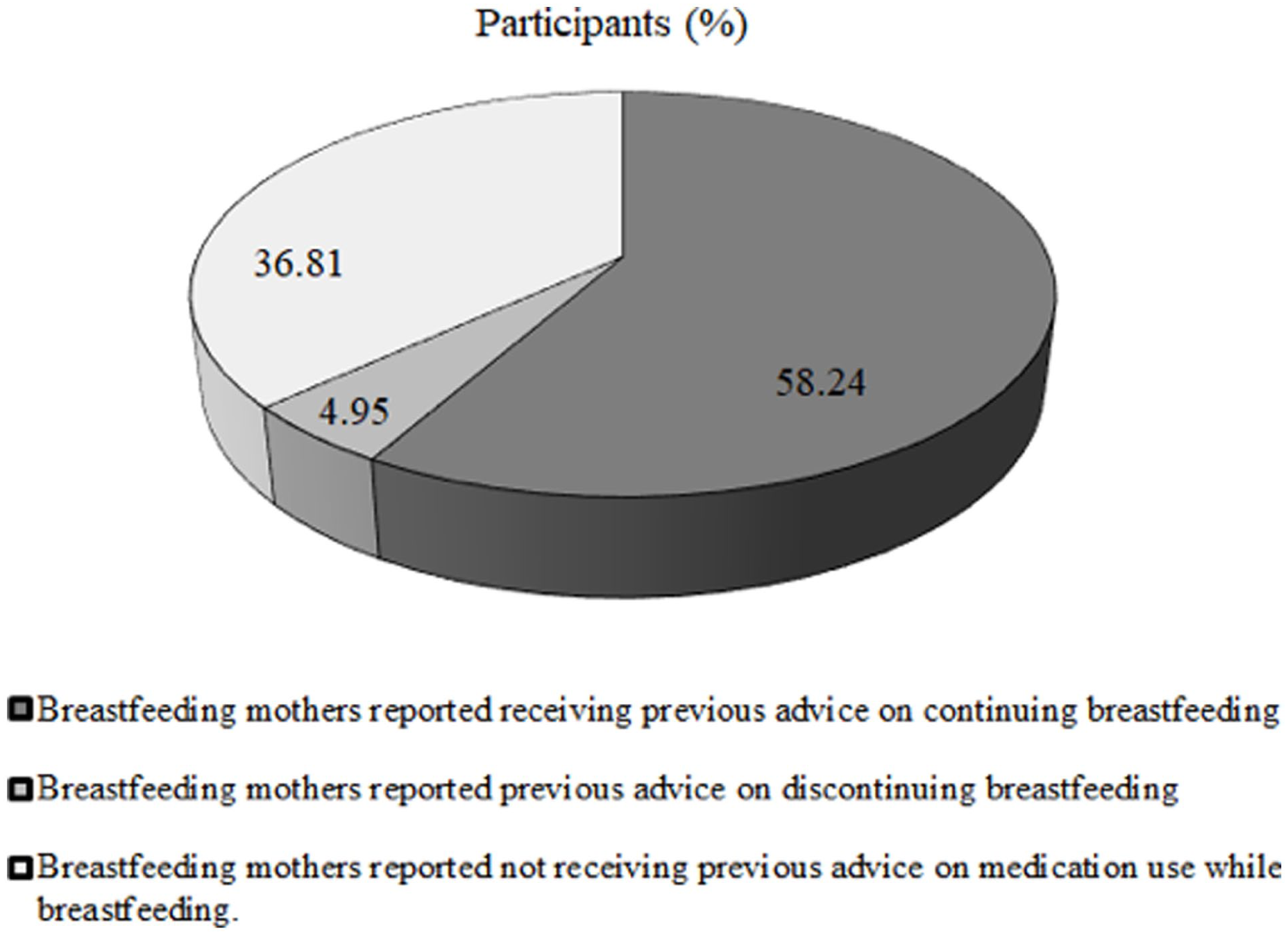
Breastfeeding mothers’ reports on antimicrobial treatment recommendations received before visiting the community pharmacy.
Pharmacist-Led Interventions
During pharmaceutical counseling, pharmacists used reliable literature sources to assess the safety of AM and subsequently provided appropriate and tailored pharmacist-led interventions to promote adherence, safety, and the efficacy of AM therapy. Table 4 summarizes the literature sources consulted by pharmacists and the resulting recommendations. National guidelines and the e-lactancia database were the most frequently used information sources. Pharmacists most commonly recommended monitoring for diarrhea, allergic reactions, and rash in breastfed infants. In 13.74% of breastfeeding mothers receiving antimicrobial therapy, no monitoring for potential adverse effects in the infant was considered necessary.
Pharmacist-Led Recommendations and Literature Sources Used.
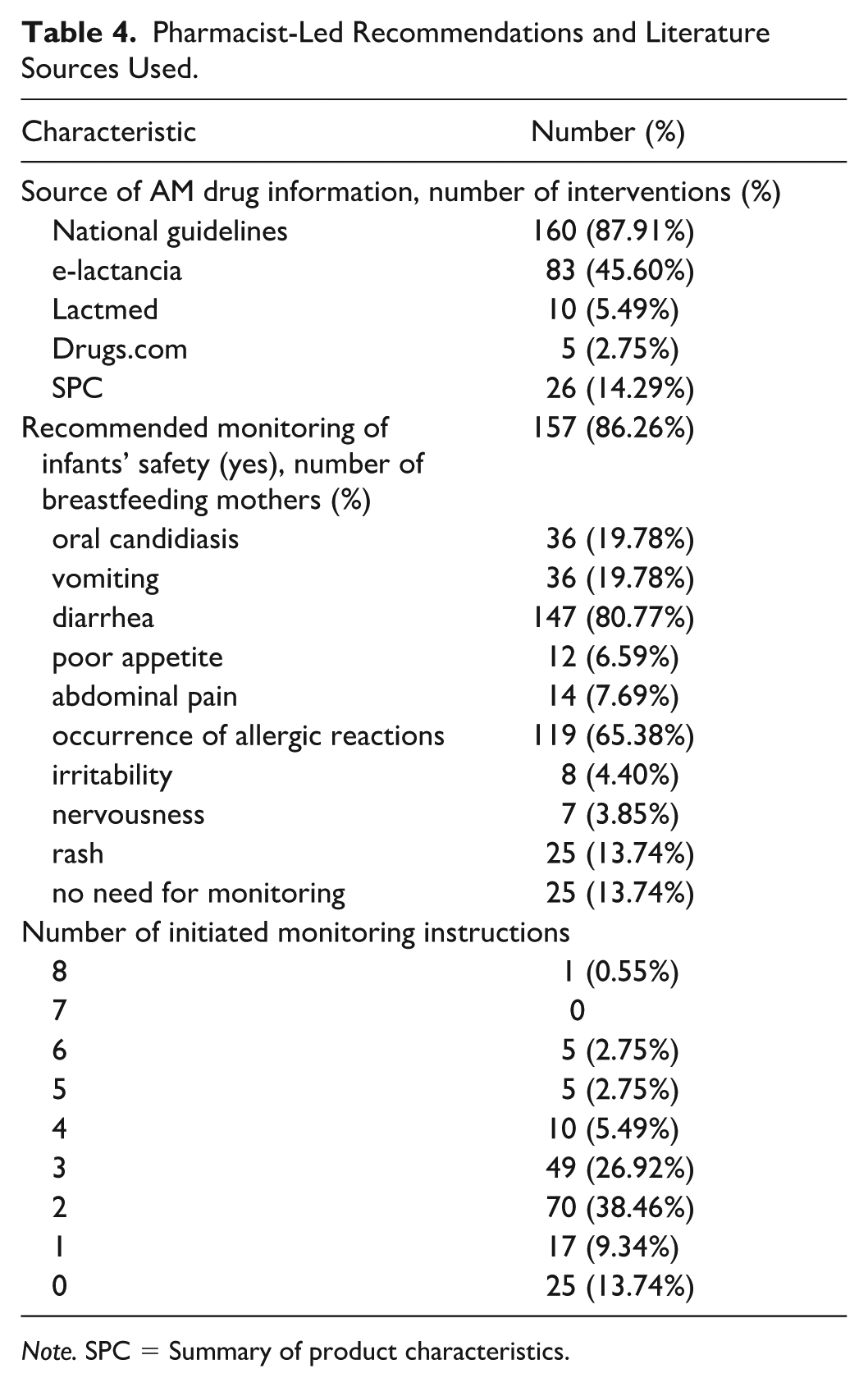
Note. SPC = Summary of product characteristics.
During counseling, breastfeeding mothers expressed willingness to follow the pharmacist-led recommendations on AM use and breastfeeding: 175 of them (95.15%) reported accepting both the instructions for regular AM use and the advice related to breastfeeding and child monitoring.
The evaluation of the achieved level of adherence and health outcomes in breastfeeding women was conducted in person or via a telephone call (Figure 3).
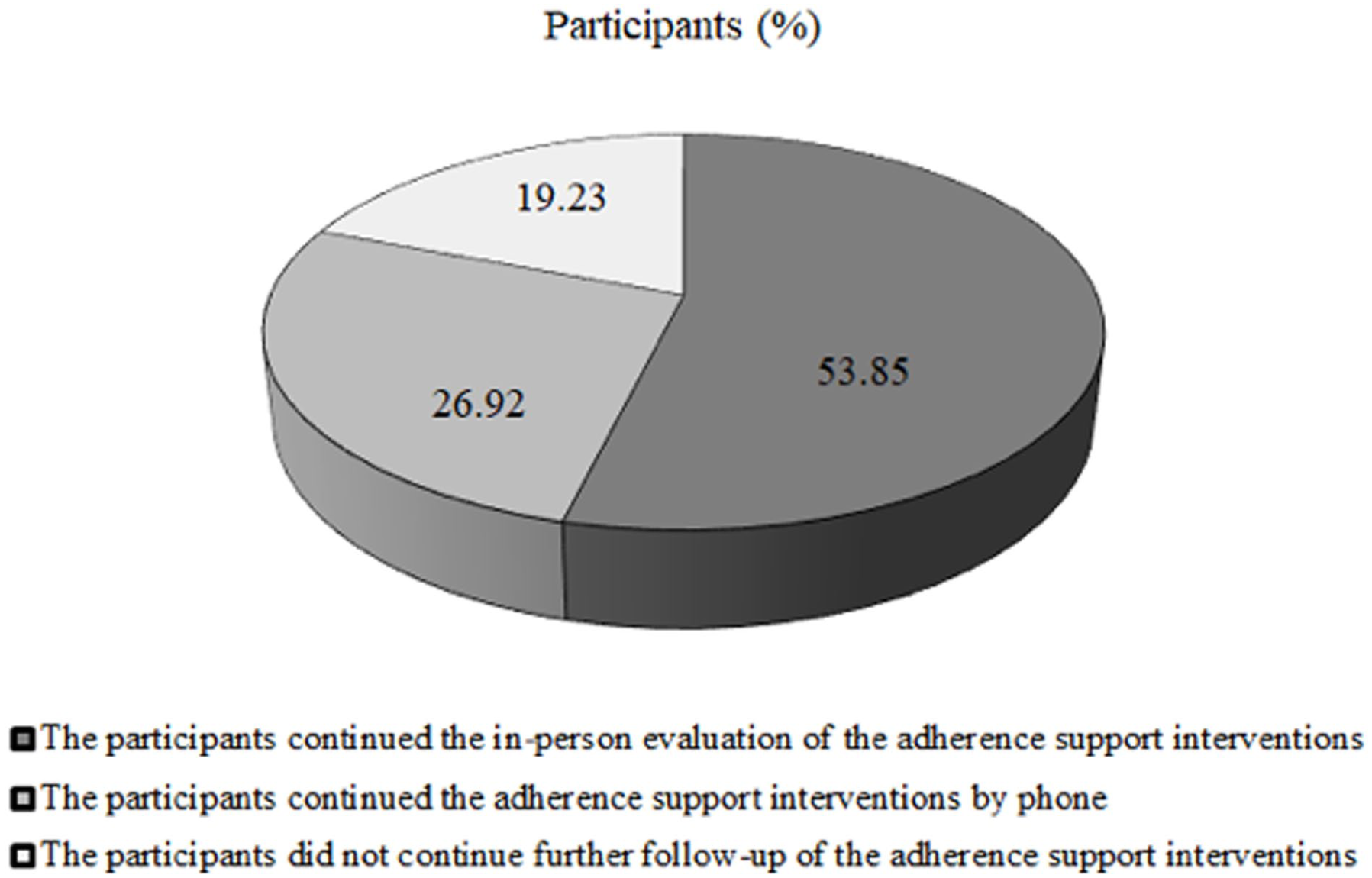
Breastfeeding mothers’ follow-up methods.
A total of 80.77% of participants completed the follow-up evaluation, with most reporting positive health outcomes. Over half of the mothers expressed a preference for in-person follow-up at the pharmacy. A total of 14 minor adverse effects were observed in infants, but none required medical intervention.
Table 5 shows regression analyses of factors influencing willingness to evaluate adherence support intervention with the pharmacist. When examining factors influencing participation in follow-up, maternal age was the only significant covariate (OR = 1.099; 95% CI [1.014, 1.192]; p = 0.022). Neither maternal education level nor infant age showed a significant association with willingness to participate in the outcomes evaluation.
Regression Analysis of Factors Influencing Willingness to Participate in Continuous Follow-Up by the Pharmacist.
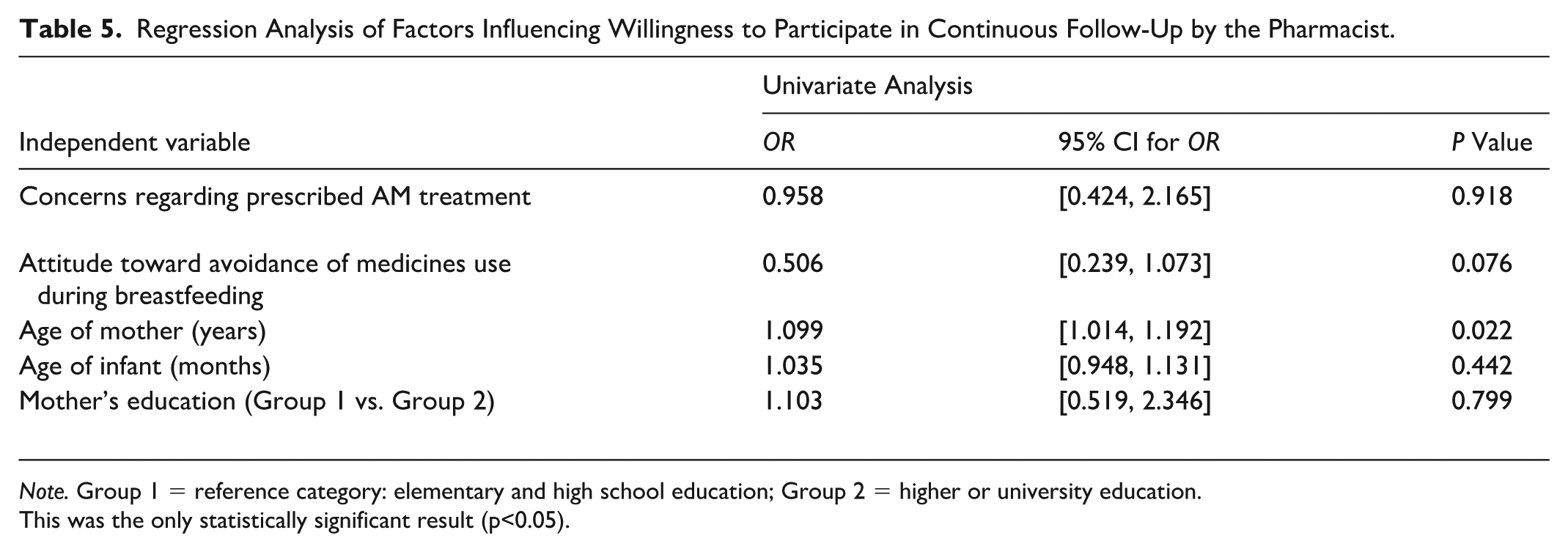
Note. Group 1 = reference category: elementary and high school education; Group 2 = higher or university education.
This was the only statistically significant result (p<0.05).
Discussion
This study aimed to investigate the influence of community pharmacist interventions on therapy adherence and outcomes of AM use in breastfeeding women. Moreover, an acceptance of pharmacist-led adherence support interventions was evaluated. Study results indicate the important role of pharmacist-led interventions on adherence to AM treatment with safe breastfeeding continuation.
The modern pharmaceutical practice includes standardization of pharmaceutical services, additional postgraduate education of pharmacists, and the personal efforts of community pharmacists in improving adherence. The need for tailored pharmacist-led interventions is highlighted by results of this study, as well as other findings; or particular importance are interventions that are included in standardized health care service (Albassam & Awad, 2018). Breastfeeding represents a valuable source of nutrients and plays a foundational role in a child’s physical and psychological development, as well as in the long-term health of the individual. In addition to family support, breastfeeding women often require assistance and guidance from healthcare professionals. When AM therapy is clinically indicated, breastfeeding women often face barriers such as safety concerns, fear of infant exposure, and inconsistent information, which were confirmed in our research. A pharmacist-structured approach and support through evidence-based counseling fight against delayed initiation, breastfeeding interruption, or early discontinuation of AM therapy. Pharmacist-led interventions, according to our results, resulted in improved treatment completion and maintained breastfeeding, and also contributed to AM stewardship. As identified in our study, between 58%–84% of breastfeeding mothers expressed concerns regarding prescribed AM use, regardless of their previous attitude towards medication use in breastfeeding, in general. These findings strongly indicate the importance of structured and system-wide education and support to breastfeeding mothers requiring postpartum therapy. Previous research showed that one-third of Dutch women who required pharmacotherapy chose not to initiate breastfeeding due to medication use, and, in approximately 30% of these cases, the decision was inappropriate (de Waard et al., 2019). It is essential that mothers trust the safety of the prescribed therapy for their breastfed infant, particular antimicrobial therapies, as this confidence facilitates treatment acceptance and supports the continuation of breastfeeding (Lurie et al., 2021). On the other hand, just over half of the breastfeeding mothers (58.24%) were given appropriate supportive information on AM safety by a prescriber during the prescription process. Our study revealed a wide information gap in more than one-third of mothers (36.81%), which may result in profound concerns such as uninformed decision-making on either therapy or breastfeeding discontinuation, resulting in suboptimal health outcomes for both the mother and the baby.
It has been demonstrated that the involvement of healthcare professionals and the provision of education to breastfeeding mothers can increase breastfeeding rates and extend breastfeeding duration (Renfrew et al., 2009). Conversely, the lack of formal and continuing education on medication use during lactation among health professionals often leads to unnecessary recommendations to discontinue breastfeeding when pharmacotherapy is required (Byerley et al., 2022). The Mama Friendly Pharmacy project, launched in 2021/2022, aimed to support breastfeeding and establish a structured pharmaceutical service for breastfeeding women in Serbia. The project’s main findings demonstrate the significant contribution of structured pharmaceutical care to safe pharmacotherapy during lactation (Kovačević et al., 2025). In addition, the service supported longer breastfeeding duration, providing health benefits for the infant and cost savings for the family (Catić Đorđević et al., 2025).
The fight against AM resistance continues to be one of the major global public health tasks of our century, and it requires a multidisciplinary approach, highly integrated across all levels of the healthcare system and environmental sectors (Holmes et al., 2016). Given the limited number of new AM agents entering the market, the fight against resistance relies heavily on high adherence—both at initiation and throughout the course of therapy—which requires correct dosing and appropriate treatment duration (Tang et al., 2023). Pharmacists are part of a multidisciplinary approach that, by monitoring prescribed medications and providing counseling and adherence support interventions, can contribute to achieving the best possible health outcomes. Still, evidence supporting collaborative models of pharmacists and physicians in primary care, focusing on prescription rationalization—optimal dosage regimen and treatment duration—remains limited (Saha et al., 2021). In the vulnerable population of breastfeeding mothers, there exists a pressing need for enhanced education to support adherence as an important factor in rational antimicrobial pharmacotherapy. From a therapeutic-outcome perspective, it is of paramount importance to initiate timely and optimal treatment of maternal conditions for the requisite duration, while concurrently informing patients about the potential effects of prescribed medications on the breastfed infant, and providing robust support to continue breastfeeding. Indeed, although most medications are not absolutely contraindicated during lactation, inadequate counseling or overly cautious practice may lead to the unnecessary interruption of breastfeeding, or suboptimal maternal therapy (Pilgrim et al., 2025).
Previous findings affirmed the benefit of professional lactation support to increase breastfeeding intensity and duration (Bonuck et al., 2014). For this reason, pharmacist-led interventions are aimed at supporting safe breastfeeding during pharmacotherapy, particular during short-term AM therapy. According to our results the most common infections among breastfeeding mothers were respiratory and urinary tract infections, and penicillin followed by cephalosporin were the most frequently prescribed medications. The findings indicate that 84.71% of respondents who believed that medications should be avoided during breastfeeding—regardless of clinical necessity—reported concerns about using the prescribed medicine. Likewise, among participants who generally held a positive attitude toward medication use during lactation, 58.76% still expressed uncertainty regarding antimicrobial therapy. The vast majority of participants (96.15%) indicated that they would adhere to the prescribed dosing regimen and comply with the recommended monitoring protocols for potential adverse effects in the breastfed child. This confirmed the high influence of pharmaceutical counseling on primary adherence. However, 80.77% of participants during the follow-up visit/call and evaluation of the adherence support intervention confirmed a high level of adherence in the sense of accepting the treatment (primary adherence) and adhered to the dosage regimen and treatment duration (total adherence).
The literature reports inconsistent advice regarding medication safety during lactation, which represents a significant barrier to continued breastfeeding (McClatchey et al., 2018). Poor-quality or contradictory information can create confusion among healthcare providers and patients, potentially leading to premature breastfeeding cessation or suboptimal therapy. Our findings further confirm the importance of counseling appropriate literature on medication use and safe breastfeeding practices for maintaining high adherence during antimicrobial therapy. The availability of national guidelines for medication use during the breastfeeding period enabled pharmacists to more easily access valid and relevant information in order to implement the adherence and breastfeeding support intervention (88% of pharmacists accessed the online version of the guidelines during the study). Also, it is crucial that pharmacists are properly educated in the use of evidence-based scientific sources that provide the greatest quantity of safe-rated drugs among all lactation resources (Gökçay et al., 2025).
Assessment of outcomes is necessary, as participation in a single training program, or access to informational resources, without subsequent evaluation, is inadequate to guarantee the consistent provision of evidence-informed care for breastfeeding women (Bohn et al., 2023). In this context, community pharmacists play a pivotal role in the continuous education of breastfeeding mothers regarding safe medication use. By promoting adherence to prescribed antimicrobial regimens and evaluating associated health outcomes, pharmacists can make a substantial contribution to combating antimicrobial resistance while simultaneously enhancing the safety and effectiveness of therapy within the breastfeeding dyad (Pilgrim et al., 2025; Saha et al., 2021).
In contrast to studies that utilized telephone communication as the primary method for assessing health outcomes (Lurie et al., 2021), our findings demonstrate that personal contact was the preferred modality for follow-up evaluation. Notably, younger mothers (aged < 30 years) were less likely to express a willingness to participate in continued follow-up, highlighting the importance of tailoring pharmaceutical counseling to the individual needs and preferences of postpartum women. Other studies reported a positive association between maternal educational level and participation in the medication use process (Al-Sawalha et al., 2016; Tigka et al., 2022). In contrast, we reported a lack of association between maternal educational level and willingness to enter counseling follow-up. These findings could actually confirm the high necessity of this vulnerable patient group for healthcare professional-guided education and support on medication use, regardless of socioeconomic factors. The discrepancies between our findings and literature data could also be explained by study design and setting, as well as the selection process, since other studies were observational by design, and conducted via questionnaires in hospitals and maternal and child care centers (Al-Sawalha et al., 2016; Tigka et al., 2022).
Further, follow-up assessments revealed a very low incidence of adverse effects in breastfed infants. Specifically, in 14 cases, mothers reported only minor symptoms, none of which necessitated intervention by a pediatrician or pharmacist. Importantly, no mother discontinued breastfeeding, confirming the effectiveness of brief pharmacist-provided education aimed at supporting safe antimicrobial use during lactation.
Pharmacists play a critical role in improving the initiation of AM therapy by addressing the significant information gap, and maternal fears regarding infant safety, that often lead women to avoid necessary treatment. By utilizing evidence-based specialized databases such as e-Lactancia, LactMed, and national guidelines, pharmacists provide personalized risk assessments that resolve therapeutic uncertainties and reassure mothers that prescribed medications are compatible with breastfeeding. To support the continuation of therapy (total adherence), pharmacists emphasize the importance of completing the full course and maintaining the correct dosage regimen, which is essential for both maternal recovery and the global fight against antimicrobial resistance. Counseling also improves adherence by instructing mothers on infant safety monitoring, providing the support needed to continue breastfeeding even when pharmacotherapy is required. Structured pharmaceutical services and follow-up evaluations, conducted either in person or via telephone, ensure that any minor adverse effects in the infant are identified early, preventing premature or unnecessary cessation of breastfeeding.
Limitations of the Study
First, antimicrobial therapy was considered rational whenever the patient possessed a valid prescription, as antibiogram confirmation was not required to verify appropriateness. Second, 19.27% of participants could not be reached for follow-up evaluation of the pharmacist-led intervention and total adherence. Finally, the study sample consisted exclusively of breastfeeding women who voluntarily agreed to participate in a structured pharmaceutical care service, potentially limiting the generalizability of the findings to the broader population of breastfeeding women (selection bias).
Conclusion
The results of our study confirm the effectiveness of adherence support interventions implemented within community pharmacy settings. In situations where antimicrobial therapy is clinically indicated in breastfeeding women, these interventions play a critical role in resolving therapeutic uncertainties, preventing unnecessary interruption of breastfeeding, and providing education on medication safety and infant care. By improving both therapy acceptance and the duration of therapy, and supporting informed decision-making regarding breastfeeding, such interventions may also contribute to more traditional AM use and help address AM resistance. Further research is warranted to validate the significance of adherence support interventions in a larger population of breastfeeding women.
Footnotes
Acknowledgements
Authors want to thank Ljiljana Stanković, the late Branko Petrović and all participants of the Mama Friendly Pharmacy Project.
Ethical Considerations
Ethical approval for the study was obtained from the Ethics Committee of the Pharmaceutical Chamber of Serbia (Approval No. 316/5.3, issued on 29.11.2022).
Consent to Participate
All participants signed an informed consent to participate.
Consent for Publication
All participants were informed of the authors’ intention to publish the results.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Ministry of Science, Technological Development, and Innovation of the Republic of Serbia through two grant agreements with the University of Belgrade – Faculty of Pharmacy (Nos. 451-03-33/2026-03/200161 and 451-03-34/2026-03/200161) and University of Niš –Faculty of Medicine (No. 451-03-34/2026-03/200113).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.