
Abstract
Objectives:
1. To determine if Self-Rated Health (SRH) predicts dementia over a five period in cognitively intact older adults, and in older adults with Cognitive Impairment, No Dementia (CIND); and 2. To determine if different methods of eliciting SRH (age-referenced (AR) versus unreferenced) yield similar results.
Design:
Prospective cohort.
Population:
1468 cognitively intact adults and 94 older adults with CIND aged 65+ living in the community, followed over five years.
Measures:
Age, gender, education, subjective memory loss, depressive symptoms, functional status, cognition, SRH and AR-SRH were all measured; dementia was diagnosed on clinical examination. Those with abnormal cognition not meeting criteria for dementia were diagnosed with CIND.
Results:
In those who were cognitively intact at time 1, and had good SRH: 69.4% were intact; 6.0% had CIND; 6.9% had dementia, and 17.7% had died at time 2, while in those with poor SRH: 44.9% were intact, 11.1% had CIND, 9.1% had dementia, and 34.8% had died (p<0.001, chi-square test). In multinomial regression models SRH predicted dementia and death. In those with CIND at time 1 and good SRH: 2.3% were intact: 18.6% had CIND; 34.9% had dementia and 44.2% had died at time 2, while in those with poor SRH: 4.8% were intact, 31.0% had CIND, 19.0% had dementia, and 43.6% had died (p=0.30, chi-square test). In multinomial regression models, this was not significant. AR-SRH analyses were similar.
Conclusions:
In cognitively intact older adults SRH predicts dementia. In older adults with CIND, SRH does not predict dementia.
Keywords
Self-rated health (SRH) can be assessed with a simple, reliable question 1 that may be useful in clinical practice, research, and general health surveys. The subjective assessment of one’s own health is associated with biomedical markers of disease, objective measures of health, 2 the number of comorbid conditions, 3 and activities of daily living (ADLs). 4 Moreover, SRH may be more than simply a reflection on one’s health, but may also reflect an individual’s efforts to achieve health-related goals, 5 health beliefs and behaviors, 6 and sociocultural influences.7-9 SRH may also contain information that is not entirely reflected in underlying medical conditions and risk factors. 10 Since first reported, the association between SRH and mortality 11 has been replicated in many studies in many countries and in many settings. Idler and Benyamini have reviewed the literature and reported that SRH is predictive of most causes of death, 12 except those most strongly associated with depression: suicide, homicide, and accidents. DeSalvo et al 13 have also systematically reviewed this association and found a strong, graded effect on mortality even after accounting for potential confounding factors such as age, gender, and functional status. SRH also predicts other adverse outcomes such as depression, 8 institutionalization,14,15 and functional decline. 16 There is some discussion about what SRH actually measures,17-19 and why it predicts adverse outcomes, but there is little doubt that poor SRH predicts a wide range of adverse outcomes.
Because it is easily measured and is so strongly associated with adverse outcomes, some have advocated incorporating broad general assessments of health, such as SRH, into clinical encounters. 20 Simply asking people how they feel may be a good barometer of their health as well as the opening to a more thorough history and physical. This approach reinforces the importance of talking to patients rather than simply conducting batteries of tests and questionnaires.
Another reason to elicit SRH may be to predict adverse cognitive outcomes. The association between general health and cognition has long been noted. 21 More recently, interest in the link between general health and dementia has been revisited. The Cache County study found that cognitive impairment, no dementia (CIND) and dementia were strongly correlated with measures of physical health. 22 Song et al 23 report that a higher number of cumulative health problems predicts dementia over a 5-year interval. There has also been some interest in the relationship between SRH and cognition. Walker et al 24 have reported on the accuracy of SRH in those with cognitive impairment. In those with mild and moderate impairment, SRH predicts death, while the association is less clear in those with severe cognitive impairment. Self-rated health may also predict cognitive loss. In a clinical sample of cognitively intact adults aged 60 to 64, subjective health was a predictor of developing mild cognitive decline over a 4-year period. 25 In the Bronx Longitudinal Aging Study, SRH was a very strong predictor of developing all types of dementia, even after accounting for other possible confounding factors. 26 Yip et al 27 found that poor SRH was a very strong predictor of developing dementia in nested case–control analyses of a population-based cohort study after adjusting for a number of potential possible confounding factors. They found a graded risk across the responses, from poor to excellent. More recently, the Three Cities (3C) study found that SRH is a strong predictor of incident dementia over 6 to 7 years. 28 This association was stronger in those with subjective cognitive complaints. We have also found that SRH is a strong predictor of dementia. 29 However, in these analyses, SRH was considered as a potential confounding factor in these analyses, and we did not consider it fully as a variable of interest.
To our knowledge, no studies have examined SRH as a predictor of dementia in those with mild cognitive impairment (MCI) or CIND. Clinicians may be particularly interested in predicting dementia in these groups of high-risk individuals. As well, the previous studies have not examined the effect of different SRH questions. SRH can be unreferenced (ie, as a simple question only), referenced against age (ie, for your age, how would you rate your health?),30,31 or referenced against time (ie, compared to 1 year ago, how would you rate your health?). Different wording and different reference points may result in different predictive ability. To validate some of the previous observations and to expand further on the current state of knowledge on the association between SRH and dementia, we have conducted a secondary analysis of an existing data set.
Specifically, the objectives are to (1) determine whether SRH predicts dementia in cognitively intact community-dwelling older adults over a 5-year period; (2) determine whether SRH predicts dementia in older adults with CIND; and (3) determine whether both age-referenced (AR)- and nonage-referenced SRH questions predict dementia.
Methods
Setting and Sample
Manitoba is a province in the prairie region of Canada. It has a stable population of 1 091 940 (in 1991) with 13.4% elderly individuals. 32 Data used in this study are from the Manitoba Study of Health and Aging (MSHA), a prospective cohort study of aging and cognition conducted in conjunction with the Canadian Study of Health and Aging (CSHA). 33 The primary objectives were to estimate the prevalence and incidence of dementia in Manitoba and to examine issues related to informal caregiving. The MSHA received ethical approval from the research ethics committee of the University of Manitoba and adhered to the Helsinki Declaration. Informed consent was obtained from the participants or from the appropriate proxy.
People older than the age of 65 and living in the community were randomly selected according to health region and age group from a list provided by Manitoba Health. Since health care is universal in Manitoba, this is one of the most complete listings of residents available. There was an oversampling of the oldest old (>85 years), in order to increase the likelihood of obtaining adequate numbers of individuals with cognitive impairment. All health regions were represented, including rural areas. Initially 2890 persons were selected, 1751 persons agreed to participate. The flow of participants is shown in Table 1. The sample was split into 2 subgroups, those with CIND and those who were cognitively intact (intact). Those who had missing variables at time 1, cognitive impairment on screening instrument, but did not undergo a clinical examination, or whose time 2 status was unknown were excluded from these analyses. Those with dementia at time 1 were also excluded from these analyses.
Baseline Characteristics of the Sample and Subgroups.
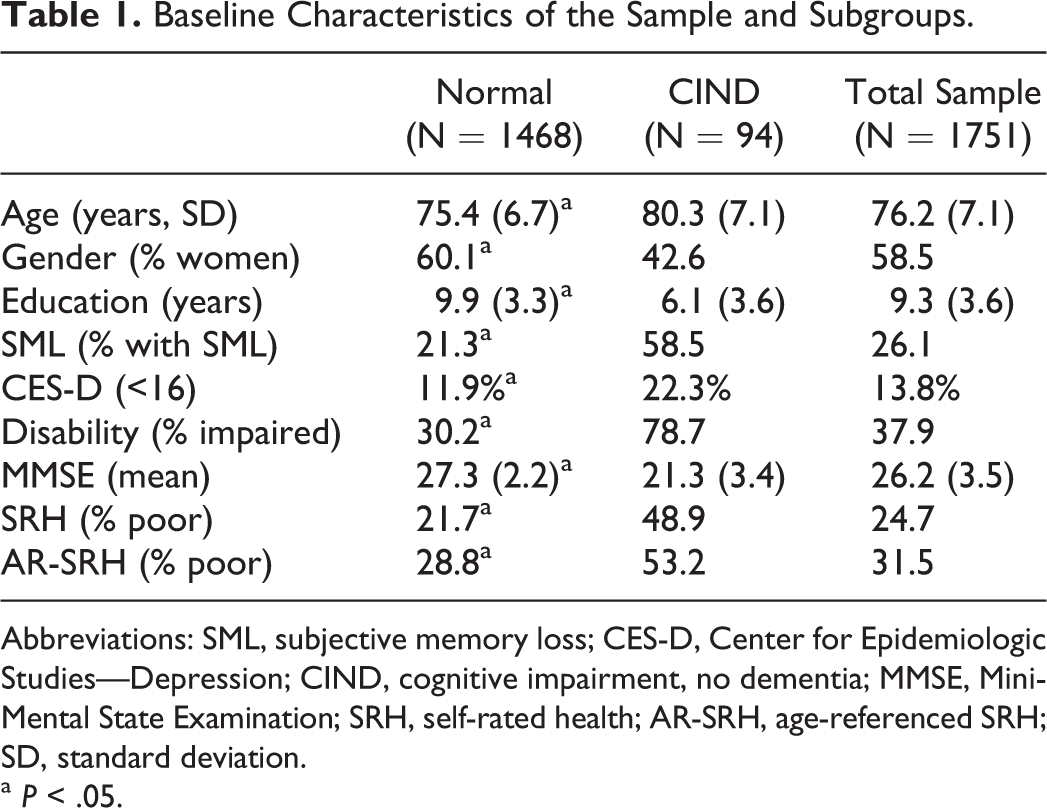
Abbreviations: SML, subjective memory loss; CES-D, Center for Epidemiologic Studies—Depression; CIND, cognitive impairment, no dementia; MMSE, Mini-Mental State Examination; SRH, self-rated health; AR-SRH, age-referenced SRH; SD, standard deviation.
a P < .05.
Measures
Predictor Variables
All participants underwent a screening questionnaire at both time 1 and time 2. Measurements included age, gender, and education that were self-reported. Subjective memory loss (SML) was assessed using a simple question “Have you noticed memory loss? Yes/no.” Functional status was based on self-report assessed using the 7-item ADL and the 7-item instrumental ADL scales from the Older American Resources Utilization Survey. 34 We considered the original scoring and categorized impairment as none/mild versus any other impairment. Depressive symptoms were assessed using the Center for Epidemiological Studies—Depression. 35 This is a valid, reliable measure of depressive symptoms. We considered a score greater than 15 to indicate the presence of depressive symptoms.
SRH was assessed using 2 questions “How would you say your health is these days? Would you say your health is very good, pretty good, not too good, poor, or very poor,” and “For your age, would you say in general your health is excellent, good for your age, fair for you age, poor for your age, or bad for your age?” For bivariate analyses, we considered SRH as a categorical variable, considering all 5 responses. In stratified analyses and in logistic regression models, we considered SRH and AR-SRH as dichomotous responses. For these analyses, we combined the responses into good versus not good. This was done because the number of observations in some cells was very small.
Cognitive Measurements
Cognition was assessed using the Modified Mini-Mental State Examination (3MS). 36 This is a modification of the Mini-Mental State Examination (MMSE)37,38 with expanded scoring and added items. Those who scored below 78 on the 3MS underwent a clinical examination to determine the presence of dementia using Diagnostic and Statistical Manual of Mental Disorders (Third Edition Revised) criteria for dementia. Since the MMSE is most widely used than the 3MS, we present analyses using the MMSE score.
For these analyses, we categorized cognition as intact (normal 3MS or 3MS below 78 but a normal clinical examination), CIND39-41 (3MS < 78, but clinical examination not consistent with dementia), or dementia (3MS < 78 and a clinical examination consistent with dementia).
Outcome Variable
Since SRH is a very strong predictor of death, we wanted to account for the effect of differential mortality. We therefore considered 4 outcomes at time 2, death, dementia, CIND, and intact. For these analyses, we included those who (1) had complete data on SRH, and cognitive status at time 1; (2) had an accurate time 2 outcome status (ie, no missing clinical data); (3) had normal cognition at time 1 or CIND at time 1 (ie, we excluded those with dementia at time 1). This left 2 samples those with normal cognition at time 1 and those with CIND at time 1.
Analyses
We considered SRH and AR-SRH as categorical independent variables for bivariate analyses between SRH and the outcomes, using chi-square tests. SRH was not normally distributed, and was scored on a 5-point scale. As well, in logistic regression models, and in multinomial logistic regression models, the number of observations in some cells was very small. We therefore dichotomized SRH and SRH into good versus not good for all stratified and regression analyses.
We constructed multinomial logistic regression models for 4 time 2 outcomes. The reference outcome was intact. Independent variables entered into the model were age (continuous), gender (categorical), education (continuous), depressive symptoms (dichotomous), functional status (no impairment vs impairment), SML (categorical), and the MMSE score (continuous). Since the MMSE and educational attainment were very closely correlated, we also constructed models without the MMSE. This did not alter the associations between SRH and time 2 outcomes, so we present the full models. We performed separate analyses for those with normal cognition and for those with CIND at time 1.
We also conducted analyses only on survivors. Here, we conducted bivariate analyses, and then constructed logistic regression models for those who survived (intact sample, N = 1016; CIND sample, N = 47). We considered the outcome as dementia at time 2 versus CIND/intact. These results were similar to the results of multinomial logistic regression models.
Standard regression diagnostics (eg, multicollinearity, influential outliers) were conducted. Bivariate analyses and graphs were conducted in SPSS version 10 (SPSS, Chicago), and statistical models were constructed using Stata version 11 (Statacorp, College Station, Texas). We also sought interactions in this effect. To do this, we constructed logistic regression models with dementia at time 2 as the outcome. We considered interactions between time 1 SRH and all other time 1 factors by entering the main effects and an interaction term into logistic regression models. We also considered interaction terms in the multinomial logistic regression. This gave similar results, but the results are more difficult to interpret, so we present the results from the logistic regression models. As well, we stratified the analyses on time 1 factors and performed analyses similar to those of Montlahuc et al. 28
Results
The baseline characteristics are shown in Table 1. Those who were cognitively intact at time 1 were younger, had better SRH, and were more likely to have higher education levels, less disability, fewer depressive symptoms, and less SML than those with CIND.
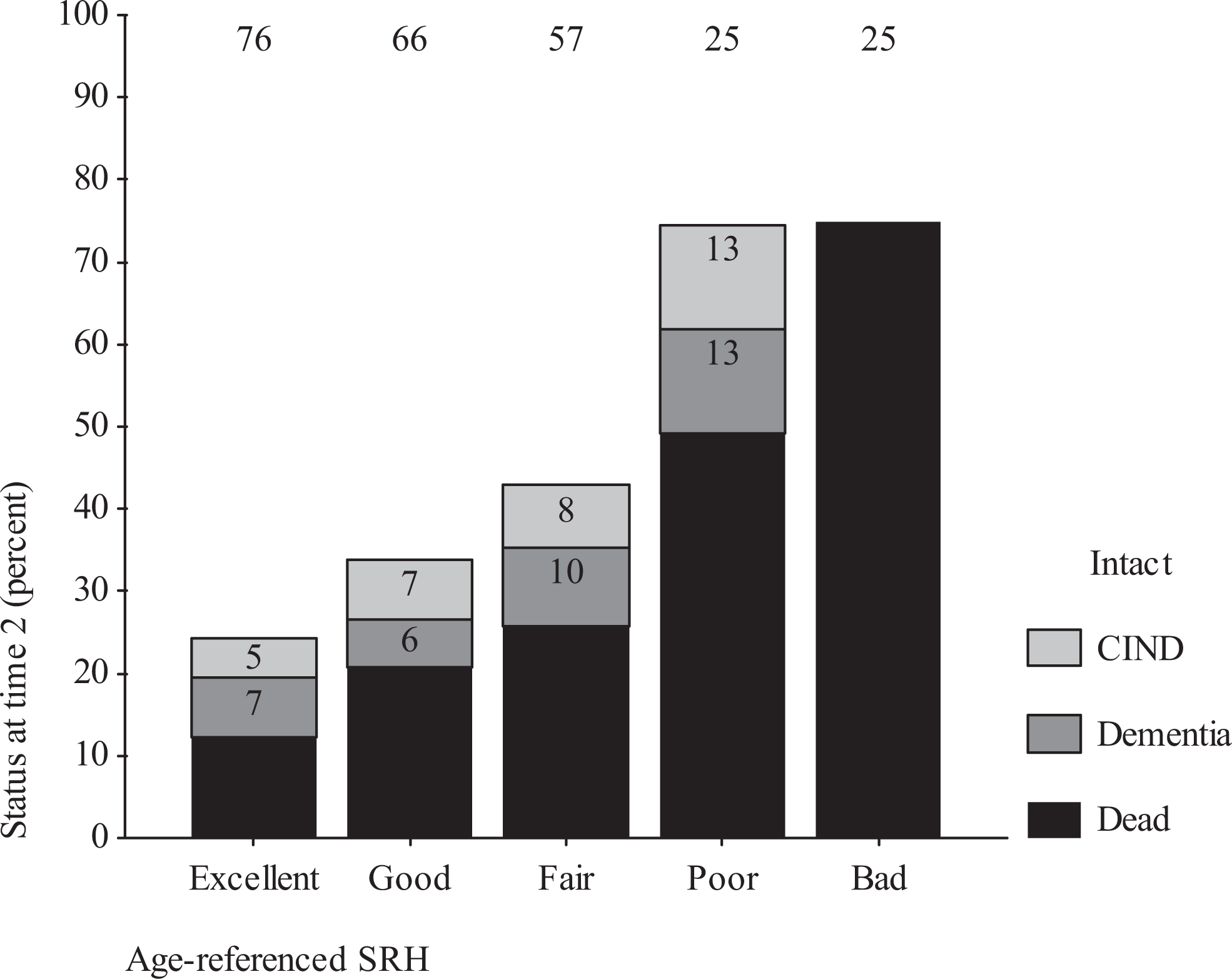
Among those who were cognitively intact at time 1, SRH was a strong predictor of having dementia and CIND 5 years later. In those who were cognitively intact at time 1 and had good SRH, 69.4% were intact, 6.0% had CIND, 6.9% had dementia, and 17.7% had died, while in those with poor SRH 44.9% were intact, 11.1% had CIND, 9.1% had dementia, and 34.8% had died (P < .001, chi-square test). There appeared to be a strong gradient in the risk of dementia, CIND, and death over a 5-year period (Figure 2). The effect of SRH on these outcomes was very impressive, with only a quarter of those with poor SRH remaining alive and cognitively intact at time 2, compared to three-fourth of those with very good SRH. It should be noted that the risk of death was much higher than the risk of dementia or CIND.
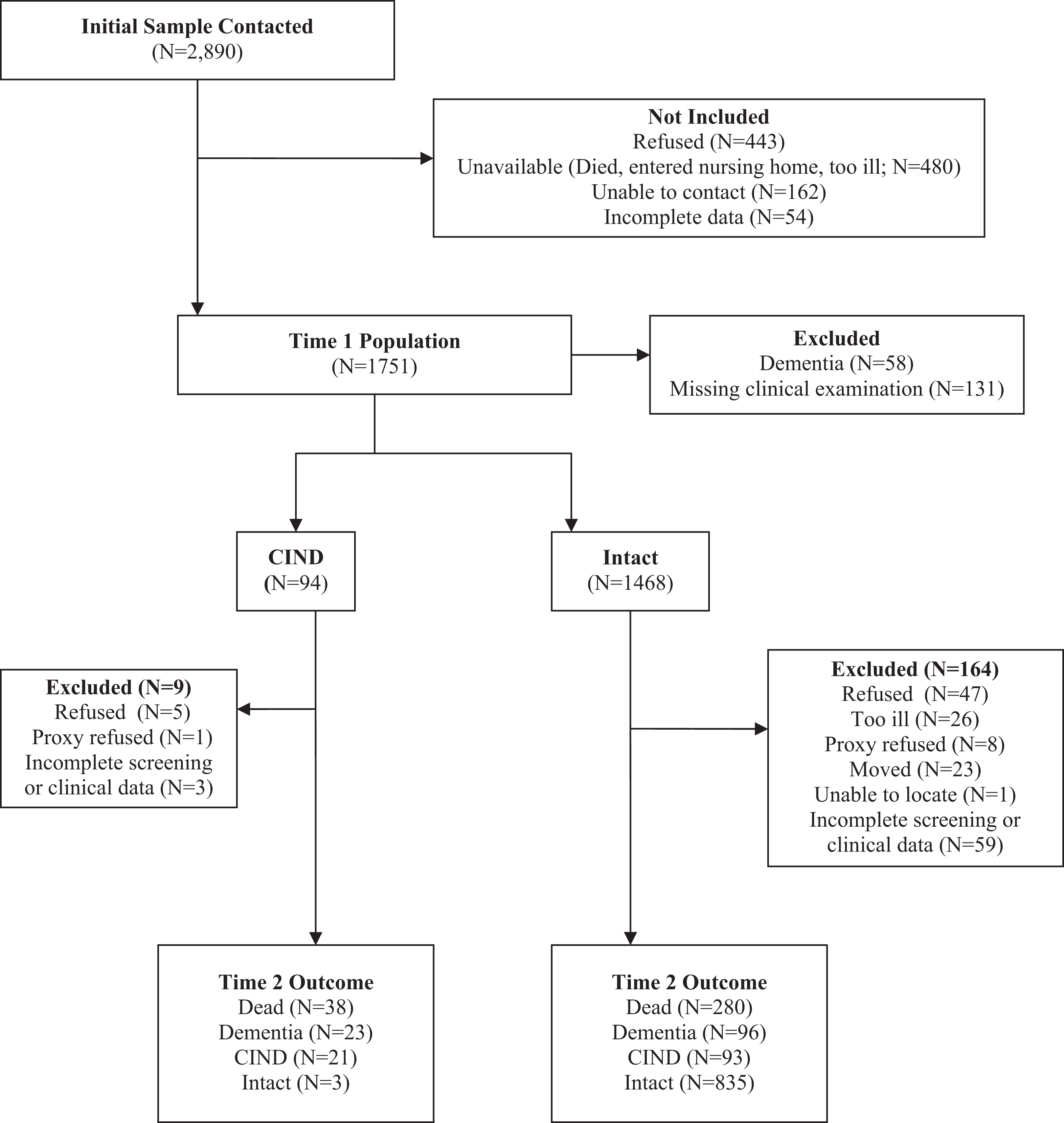
Flow of participants in the M anitoba Study of Health and Aging.
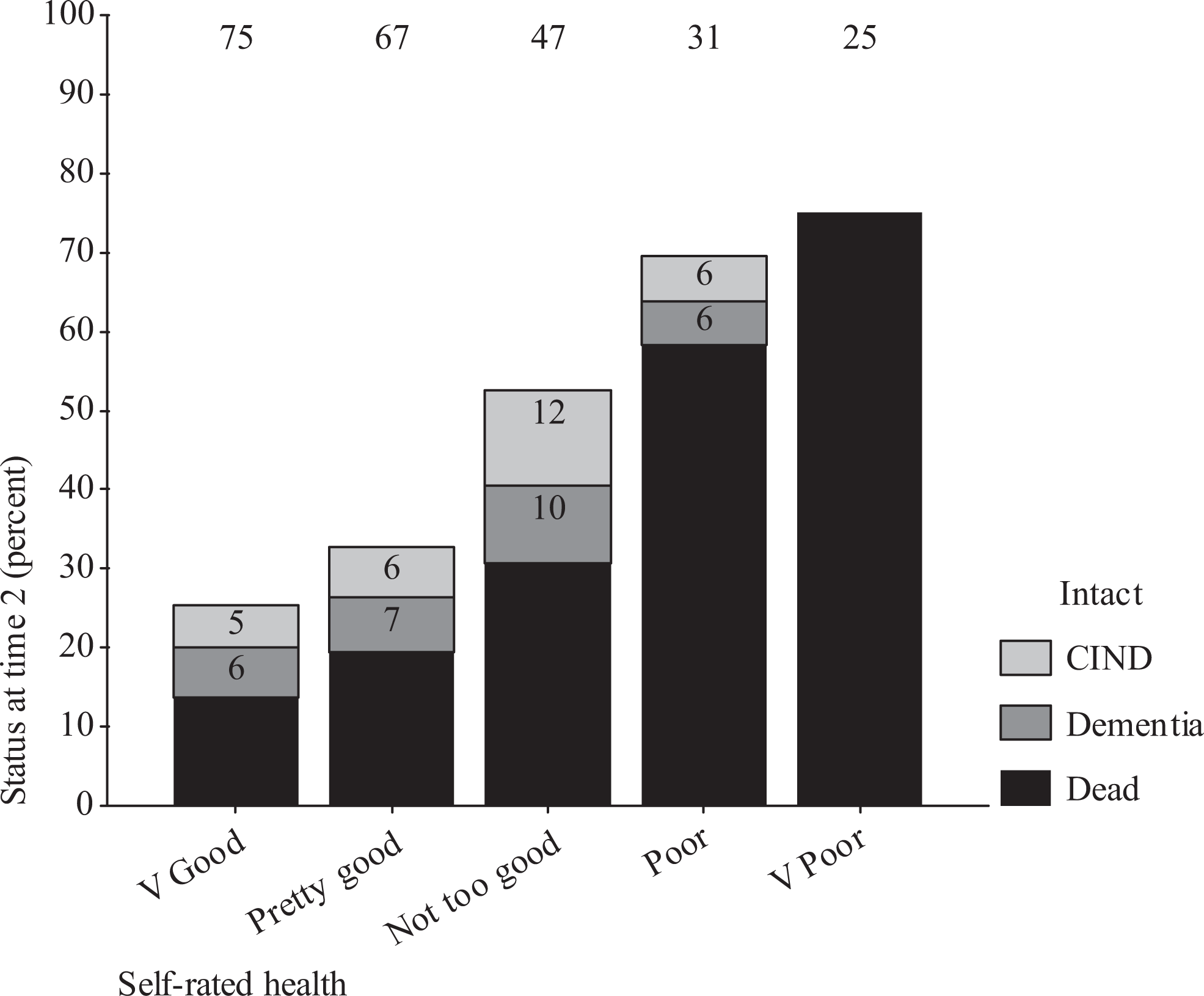
Self-rated health predicts dementia 5 years later in those with normal cognition. Self-rated health also predicts death and cognitive impairment, no dementia (CIND).
We constructed multinomial logistic regression models for time 2 outcomes. In these models, SRH remained a strong predictor of dementia 5 years later (Table 2). SRH was also a strong predictor of CIND and death at time 2. As well, age, depressive symptoms, and the MMSE predicted death. Age, SML, and the MMSE all predicted dementia at time 2.
Results of Multinomial Logistic Regression for Unreferenced SRH at Time 1 as a Predictor of Time 2 Cognitive Status, in Those With Normal Cognition at Time 1.a
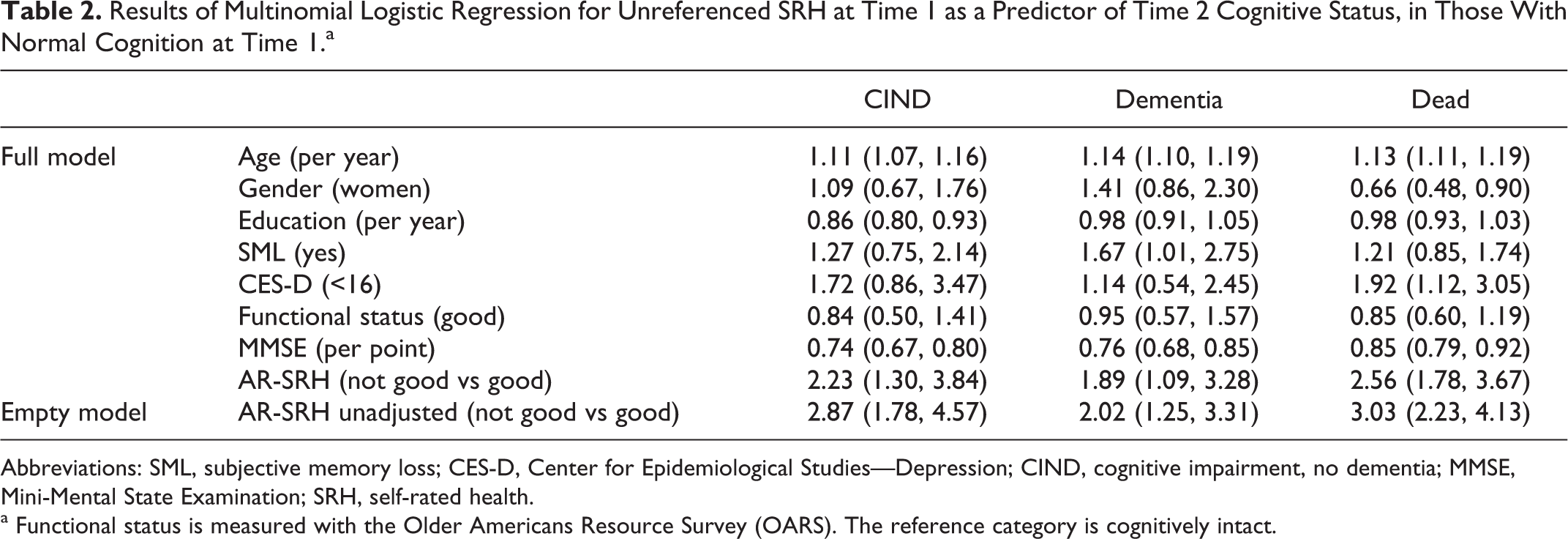
Abbreviations: SML, subjective memory loss; CES-D, Center for Epidemiological Studies—Depression; CIND, cognitive impairment, no dementia; MMSE, Mini-Mental State Examination; SRH, self-rated health.
a Functional status is measured with the Older Americans Resource Survey (OARS). The reference category is cognitively intact.
AR-SRH was also a strong predictor of death, dementia, and CIND in those with normal cognition. In those who were cognitively intact at time 1 and had good AR-SRH, 68.9% were intact, 6.6% had CIND, 6.2% had dementia, and 18.2% had died, while in those with poor AR-SRH 52.1% were intact, 8.3% had CIND, 9.9% had dementia, and 29.7% had died (P < .001, chi-square test). There was also an apparent gradient in this association (Figure 3). This association persisted after accounting for potential confounding factors (Table 3).
Age-referenced self-rated health predicts dementia 5 years later in those with normal cognition. Age-reference self-rated health also predicts death and cognitive impairment, no dementia (CIND).
Results of Multinomial Logistic Regression for Age-Referenced SRH at Time 1 as a Predictor of Time 2 Cognitive Status, in Those With Normal Cognition at Time 1.a
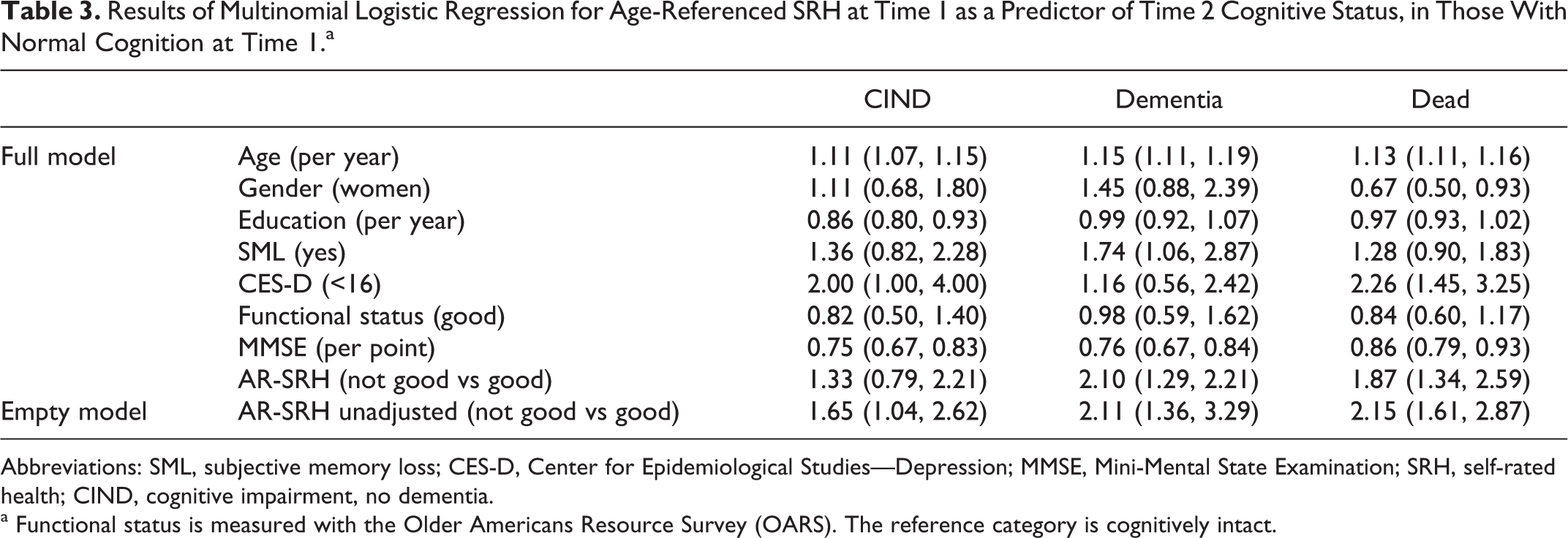
Abbreviations: SML, subjective memory loss; CES-D, Center for Epidemiological Studies—Depression; MMSE, Mini-Mental State Examination; SRH, self-rated health; CIND, cognitive impairment, no dementia.
a Functional status is measured with the Older Americans Resource Survey (OARS). The reference category is cognitively intact.
However, in those with CIND at time 1, SRH did not predict dementia (Figure 4). In those with good SRH at time 1, 2.3% were intact, 18.6% had CIND, 34.9% had dementia, and 44.2% had died, while in those with poor SRH 4.8% were intact, 31.0% had CIND, 19.0% had dementia, and 43.6% had died (P = .30, chi-square test). As previously reported, CIND has a high mortality risk and a high risk of progressing to dementia. Multinomial logistic regression models are shown in Table 4. There was no association between SRH and any adverse time 2 outcome in either bivariate analyses or regression models. The results of analyses with AR-SRH were very similar; in those with CIND, AR-SRH did not predict adverse outcomes (Figure 5). In those with good AR-SRH at time 1, 5.1% were intact, 17.9% had CIND, 33.3% had dementia, and 43.6% had died, while in those with poor AR-SRH, 2.2% were intact, 30.4% had CIND, 21.7% had dementia, and 45.7% had died (P = .40, chi-square test). There was no association noted in regression models (Table 5).
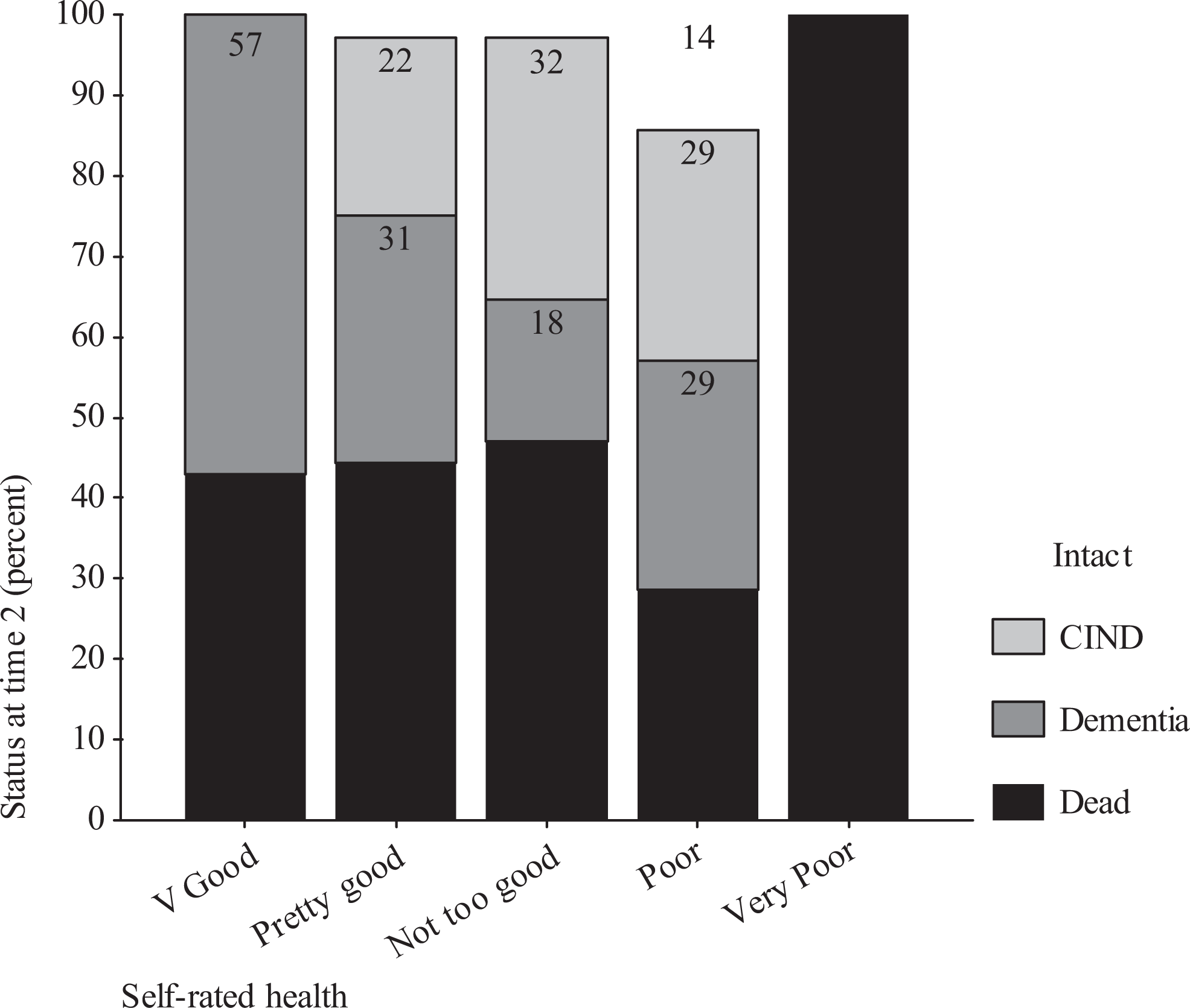
Sef-rated health is not associated with dementia 5 years later in those with cognitive impairment, no dementia. Self-rated health does not predict death or cognitive impairment, no dementia (CIND) at time 2.
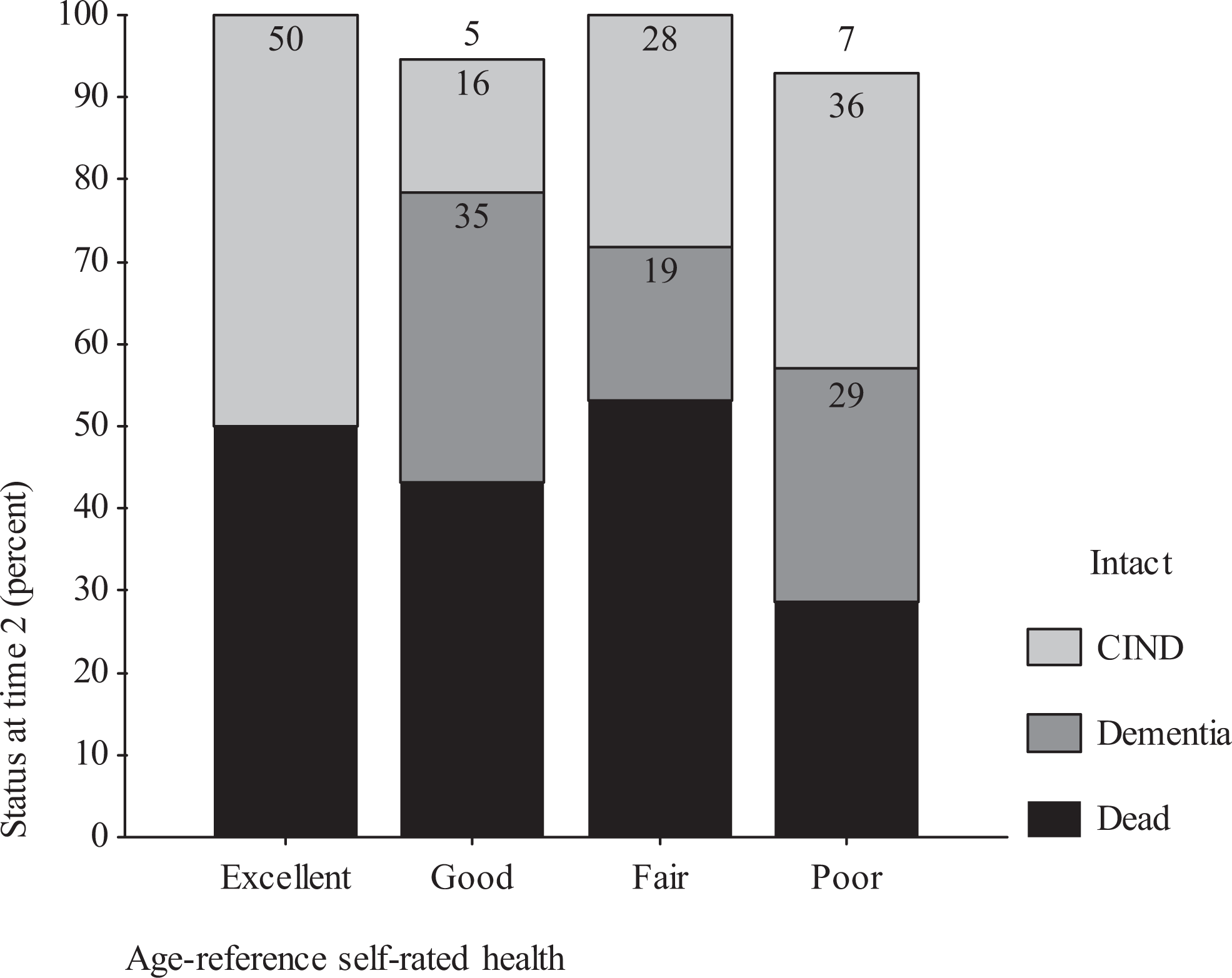
Age-referenced self-rated health is not associated with dementia 5 years later in those with cognitive impairment, no dementia. Age-referenced self-rated health does not predict death or cognitive impairment, no dementia (CIND) at time 2.
Results of Multinomial Logistic Regression for Unreferenced SRH at Time 1 as a Predictor of Time 2 Cognitive Status, in Those With Cognitive Impairment, No Dementia at Time 1.
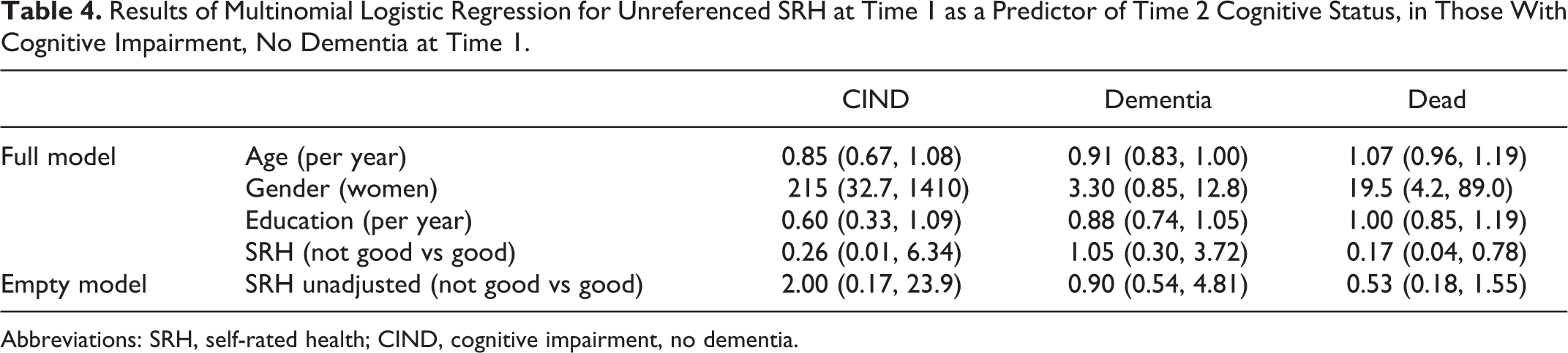
Abbreviations: SRH, self-rated health; CIND, cognitive impairment, no dementia.
Results of Multinomial Logistic Regression for Age-Referenced SRH at Time 1 as a Predictor of Time 2 Cognitive Status, in Those With Cognitive Impairment, No Dementia at Time 1.
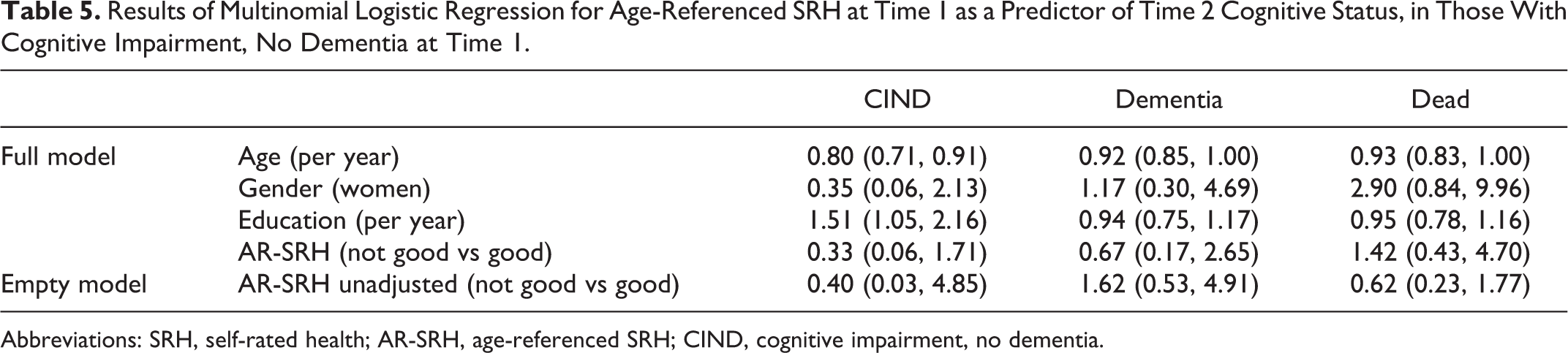
Abbreviations: SRH, self-rated health; AR-SRH, age-referenced SRH; CIND, cognitive impairment, no dementia.
As a sensitivity analyses, we considered analysis only on survivors. Here, we considered the outcome of dementia versus no dementia at time 2. While doing this, we had similar results; among those who were cognitively intact at time 1, SRH was a strong predictor of dementia and CIND 5 years later. In those with good initial SRH, 84.3% were cognitively intact, 7.3% had CIND, and 8.4% had dementia at time 2. For those with poor initial SRH, 69.0% were cognitively intact, 17.1% had CIND, and 13.9% had dementia at time 2 (P < .01, chi-square test). In those with good AR-SRH, 84.3% were cognitively intact at time 2, 8.1% had CIND, and 7.6% had dementia. In those with poor AR-SRH, 74.1% were cognitively intact, 11.8% had CIND, and 14.1% had dementia (P < .001, chi-square test). However, in those with CIND at time 1, SRH did not predict dementia; 62.5% of those with good SRH had dementia at time 2 versus 34.8% of those with poor SRH (P = .06) Indeed, in logistic regression models, SRH appears to lessen the risk of dementia: The adjusted odds ratio was 0.17 (95% confidence interval: 0.03-0.85) adjusting for age, gender, and education.
When we examined for interactions (Figure 6), we found that the effect of SRH was stronger in those with higher education than those with lower education levels. We also found a stronger effect in those with intact function than in those with functional impairment, similar to Montlahuc et al. 28 However, it is not clear whether these interactions are clinically meaningful. As well, searching for interactions is problematic in subgroups with very high mortality rates (eg, those with disability and poor SRH). Therefore, the results of these interactions should be interpreted with caution.
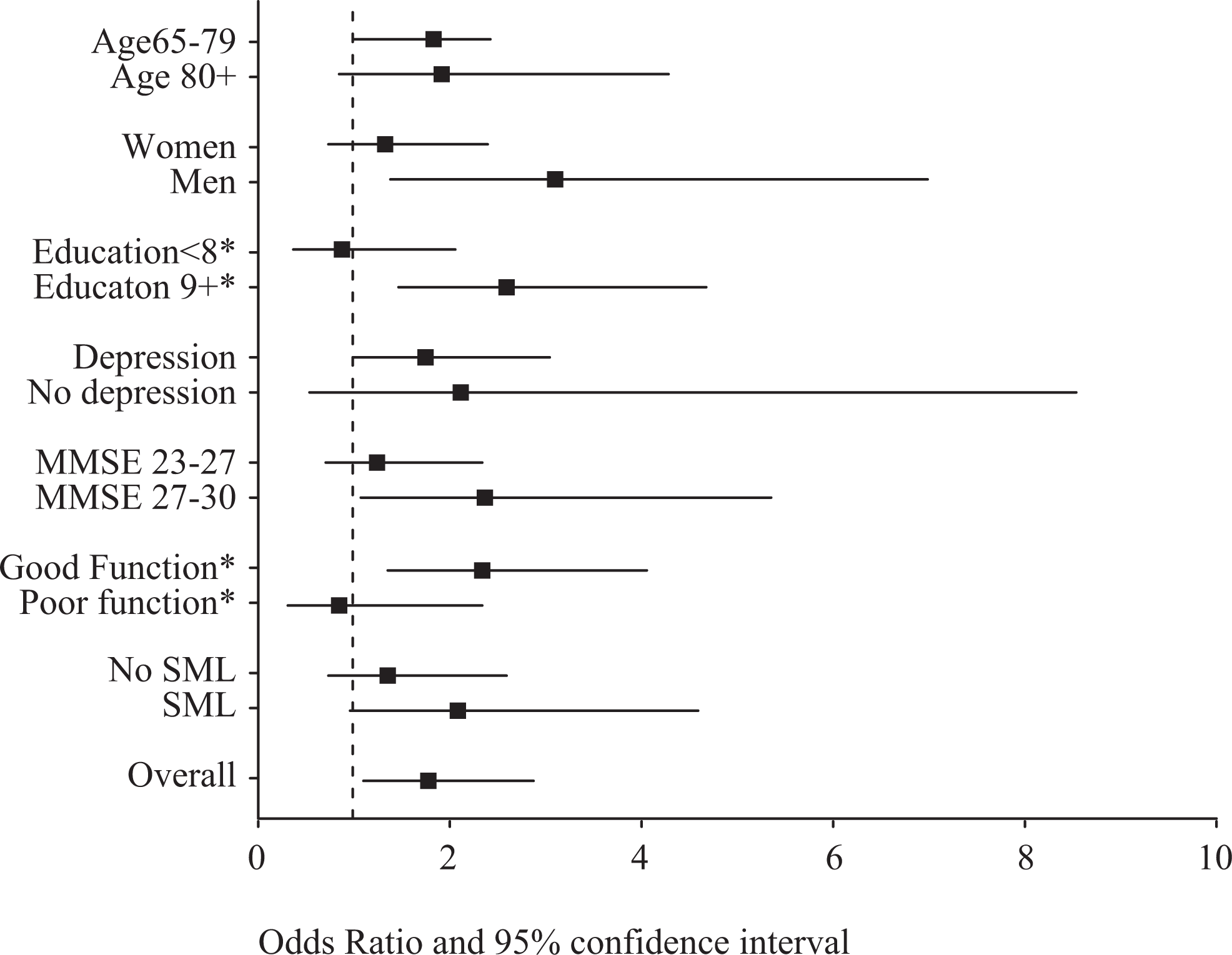
Interactions in the effect of SRH on dementia. Here, the unadjusted odds ratio and 95% confidence interval are presented. The effect of interactions in logistic regression models is statistically significant for education and functional status. *Denotes P < .05 for the interaction term in logistic regression models.
Discussion
Regardless of the question, SRH appears to predict dementia in those with normal cognition. This effect is strong and is not simply due to differential mortality. The association between SRH and death has been widely reported, and SRH also predicts institutionalization, health care utilization, and functional loss. There are fewer studies examining whether SRH predicts dementia. The 3C study 28 in France reported that SRH predicted incident dementia over an 8-year period, after controlling for potential confounding factors. The hazard ratio for incident dementia was 2.49, which is quite similar to the risk we observed. They also noted the interactions between SRH and depression, SRH and disability, and SRH and SML. We noted only the interaction between SRH and disability, but the power of our study is much lower. As well, it may be difficult to interpret interactions in the effect of SRH on dementia when the baseline mortality in some subgroups is exceptionally high.
The Medical Research Council Cognitive Function and Ageing Study also reported an increased risk of dementia among those with poor SRH. 27 This effect was quite strong and seen over a long follow-up time frame. The Bronx longitudinal study on aging also reported a markedly higher risk of dementia in those with poor SRH compared to those with good SRH after accounting for a wide range of potential confounding factors. 26 All these studies reported a graded association, which we also observed in bivariate analyses. However, we could not consider a graded effect in logistic regression models, since the number of observations in some cells became quite small. In our bivariate analyses, however, we observed a graded effect.
In those with CIND, however, it is less clear whether SRH predicts dementia. In our sample, CIND carried a high risk of death and dementia, which was also seen in the CSHA. 42 SRH did not predict dementia in bivariate analyses or after controlling for potential confounding factors. To our knowledge, there are no reports of SRH as a predictor of dementia in those with MCI or CIND. The lack of effect we observed may be for several reasons. First, CIND is a strong predictor of adverse outcomes, and SRH may not add to the prognostic value of cognitive loss; very few people with CIND were alive and cognitively intact 5 years later, regardless of their self-ratings of health. Second, CIND is a heterogeneous group of disorders affecting cognition. Many of those with poor SRH may be having low grade or persistent delirium or other medical conditions that affect cognition and carry a high mortality. Other diagnostic criteria for defining those with cognitive loss, such as MCI, may not be so heterogeneous. Using other categorizations may yield considerably different findings. As well, study in other populations such as memory clinic samples may also yield different results. Fourth, the subjective experience and/or reporting of poor health may be different in those with CIND than in those with normal cognition. Walker et al report that the association between SRH and mortality is less strong in those with dementia. Moreover, the effect of SRH on adverse outcomes is also less strong in those who are frail compared to those who are fit. 43 Therefore, SRH may not predict adverse outcomes in those with CIND.
The causal mechanism of the effect of SRH on dementia is not clear. Cognition may have multiple influences, some of which are health related. Those with poor health may have more morbid conditions and deficits that in turn predict dementia. 23 SRH may be an accurate reflection of this multimorbid state. SRH may also reflect health beliefs and behaviors,5,6 which may also be risk factors for cognitive decline. As well, SRH may be associated with frontal and subcortical dysfunction, which are often observed in parkisonism, depressive syndromes, and in those with vascular risk factors. Frontal and subcortical dysfunction may mediate some of the effect of social vulnerability on cognitive decline 44 and SRH may be in this causal pathway. Further research is needed into how SRH predicts cognitive decline.
We also note the strong effect of SRH on mortality, which has been widely reported previously. In fact, this risk may be much more clinically relevant than the risk of dementia. At all levels of SRH, the risk of death is markedly higher than the risk of dementia. SRH may thus be a less useful predictor of dementia in clinical practice. We also corroborate and elucidate the risk factors for dementia that have been previously noted in this data set. We have previously reported that SML predicts dementia, but in multivariable models including the MMSE, it is not predictive. Here, when accounting for mortality and CIND risk, we found that SML remained a predictor of dementia. In this data set, depressive symptoms predict death 45 and dementia. 46 However, when SRH and the MMSE are included in regression models, depressive symptoms do not predict dementia. It is possible that SRH, general health, and cognition confound the association between depressive symptoms and dementia. It is also possible that we lack the power to detect an effect of depressive symptoms in these current analyses, since there were few individuals with depressive symptoms who reported good SRH. Finally, the lack of effect of education which we note should be considered with caution since the MMSE and education are highly correlated and the model is difficult to interpret. It is also possible that the effect of education on dementia is mediated through cognitive test scores.
There are both strengths and limitations in our analyses. First, this is a population-based study. The results are therefore more generalizable to a general population. On the other hand, the results may not apply to specific populations of interest to clinicians. In particular, those attending memory clinics may be a much different population and may be much more homogenous in the etiology of their cognitive loss. Thus, the predictive usefulness of SRH in these groups may be very different. Second, we used 2 questions to elicit SRH—an age-referenced item and an unreferenced item. The results are very similar indeed. We asked the nonreferenced first, and there may be some ordering bias in the response to the age-referenced question, which do limit the inferences one can draw. Third, standardized, reliable measures were gathered by trained interviewers. Furthermore, the diagnosis of dementia was made by clinical assessment using standard criteria. This minimizes the misclassification of outcomes and risk factors. Fourth, there was some loss to follow-up. Some of this loss was due to nonparticipation, but most was due to medical illness, hospitalization, and death. We attempted to account for this by constructing multinomial models, to account for death, but this may be incomplete. Fifth, we did not have a large sample of participants with CIND. This may have limited the power to detect the effect of SRH in this sample. However, we observed no trend in the risk of dementia among those with poor SRH versus good SRH. Indeed, in some sensitivity analyses, the trend was toward protection. Sixth, we did not have a measure of MCI. Rather, we considered the diagnosis of CIND that is less specific and more heterogeneous in nature. Future studies into the effect of SRH on dementia should investigate the association between SRH and dementia in populations with MCI. Finally, we lacked the power to seek a gradient effect in logistic regression models. We observed a strong effect in bivariate models and others noted a graded effect.
Our findings are important for several reasons. First, it again raises the important association between general health and cognition. This was reported decades ago but may sometimes be overshadowed by the search for biomarkers and neuroimaging predictors of dementia. Attention to more global medical status of individuals and populations may be an important adjunct to more technical approaches to predicting and preventing dementia. This may be particularly relevant in the oldest old, where the causes of cognitive loss may be very complex and multifactorial.
Our findings may also be of interest to clinicians. Early detection of dementia has not been shown to improve outcomes, and screening for dementia is not recommended. If interventions are developed, prediction tools may become more prevalent. As the prediction tools are developed, it may be useful to consider simple measures such as self-reports of general health in addition to other measures. The high risk of other outcomes (such as death) also highlights the importance of competing risks in populations of older adults. Indeed, identifying those at risk for dementia may not as relevant as identifying the risk of death.
Finally, we found that SRH did not predict dementia in those with CIND. Those with CIND are at a higher risk of developing dementia, and the current focus is on preventing progression on to overt dementia in these groups. Targeting these individuals for close monitoring and follow-up may be advocated. However, SRH may not be a useful predictor of going on to dementia in these high risk groups. Further analyses of those with more distinct diagnostic entities (such as MCI) and in clinical populations are needed.
Footnotes
Authors’ Note
Dr Montgomery was involved in the initial study concept and design, acquisition of participants and/or data of the MSHA. He was involved in the concept of these analyses and interpretation of data, and reviewing the manuscript. Dr St John was involved in the acquisition of data of the second wave of MSHA, and was involved in the concept of these analyses and interpretation of data, and wrote the manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: specifically, neither Dr St John nor Dr Montgomery serve on the scientific advisory boards, serve on editorial boards, receive royalties, hold stock options, received research support from industry, receive travel funding from industry, serve on Boards of Directors, receive revenue from patents, receive license fee payments, or have given expert testimony in regard to medication use.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Manitoba Study of Health and Aging (MSHA) was funded primarily by Manitoba Health, with additional funding provided through the Canadian Study of Health and Aging by the Seniors Independence Research Program of the National Health Research and Development Program of Health Canada. The second wave of the MSHA was funded primarily by Manitoba Health's Healthy Communities Development Fund with additional funding provided through the Canadian Study of Health and Aging by the Seniors Independence Research Program of the National Health Research and Development Program of Health Canada (Project No. 6606-3954-MC[S]).). The results and conclusions are those of the authors and no official endorsement The sponsors had no role in the design, methods, participant recruitment, data collections, analysis, and preparation of article.